
Differences in the Protection Motivation Theory Constructs between People with Various Latent Classes of Motivation for Vaccination and Preventive Behaviors against COVID-19 in Taiwan

 , ,
, ,
Abstract
:1. Introduction
1.1. Vaccination and Preventive Behaviors against Coronavirus Disease 2019
1.2. Motivation to Get Vaccinated and to Adopt Preventive Behaviors against COVID-19
1.3. Applying Protection Motivation Theory to Evaluate the Motivation to Get Vaccinated and to Adopt Preventive Behaviors
1.4. Study Aims and Hypotheses
2. Methods
2.1. Participants
2.2. Measures
2.2.1. Motivation to Get Vaccinated for COVID-19
2.2.2. Motivation to Adopt Preventive Behaviors
2.2.3. Constructs of the Extended PMT
2.2.4. Sociodemographic Characteristics
2.3. Statistical Analysis
3. Results
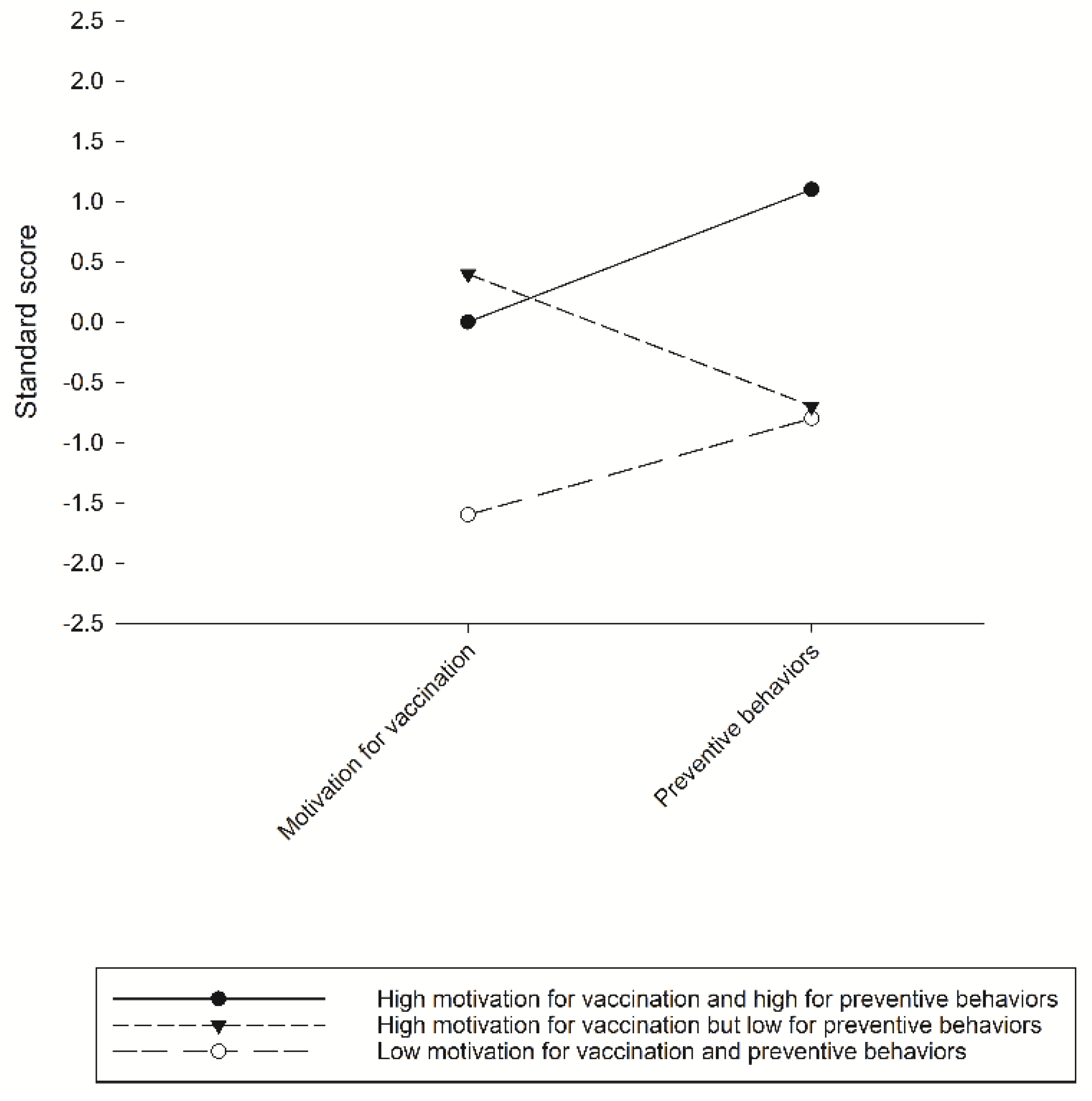
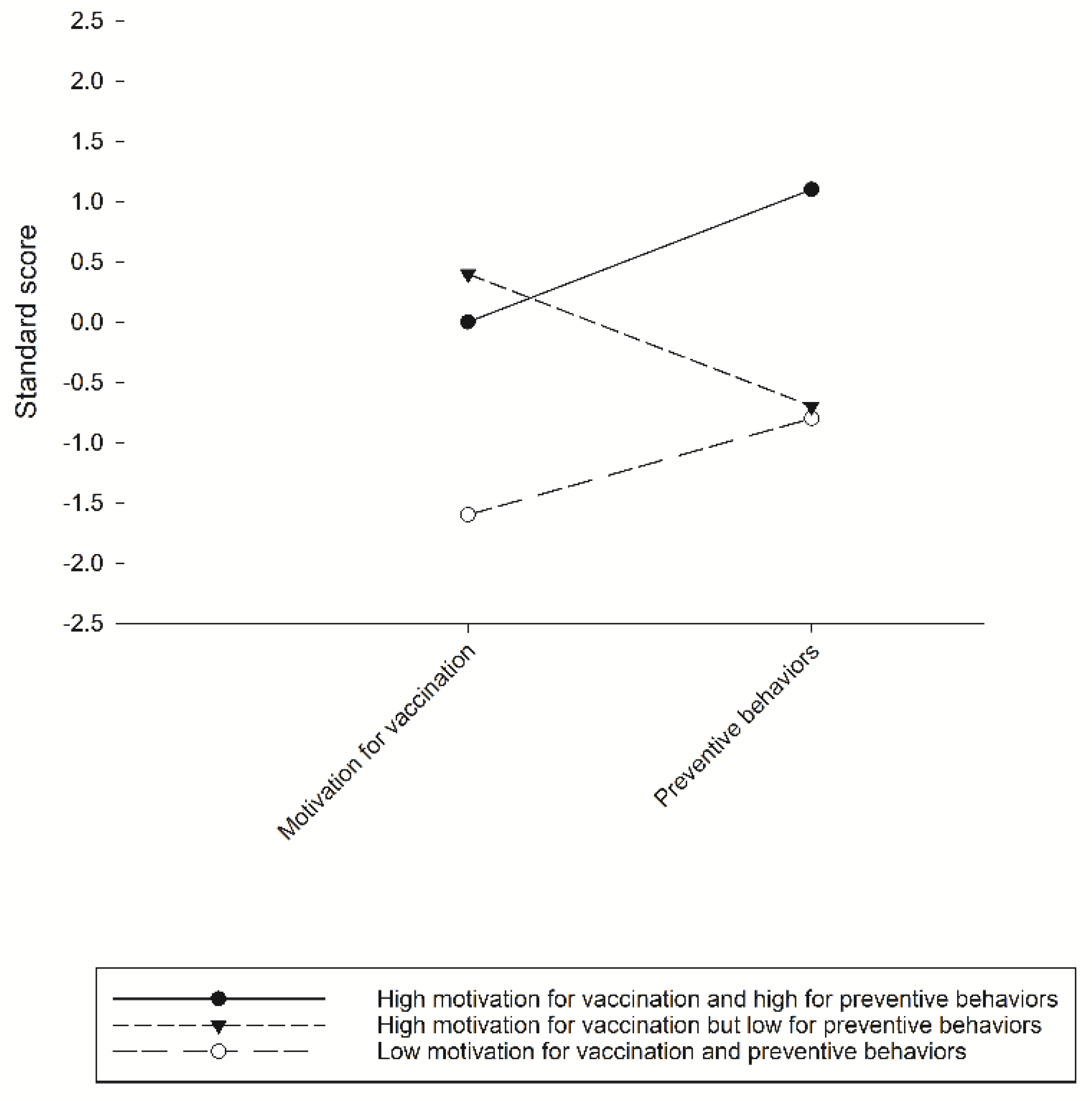
3.1. Results of LPA
3.2. PMT Constructs Predicting the Latent Classes
4. Discussion
4.1. Low Motivation for Getting Vaccinated and Adopting Preventive Behaviors and Related PMT Constructs
4.2. High Motivation for Getting Vaccination but Low Motivation for Adopting Preventive Behaviors and Related PMT Constructs
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Science and Engineering at Johns Hopkins. Modeling 2019-nCoV. Available online: https://0-systems-jhu-edu.brum.beds.ac.uk/research/public-health/ncov-model/ (accessed on 28 May 2021).
- Torales, J.; O’Higgins, M.; Castaldelli-Maia, J.M.; Ventriglio, A. The outbreak of COVID-19 coronavirus and its impact on global mental health. Int. J. Soc. Psychiatry 2020, 66, 317–320. [Google Scholar] [CrossRef] [Green Version]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef]
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef]
- Rundle, A.G.; Park, Y.; Herbstman, J.B.; Kinsey, E.W.; Wang, Y.C. COVID-19–Related School Closings and Risk of Weight Gain Among Children. Obesity 2020, 28, 1008–1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Ma, Z.F. Impact of the COVID-19 Pandemic on Mental Health and Quality of Life among Local Residents in Liaoning Province, China: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 2381. [Google Scholar] [CrossRef] [Green Version]
- Crayne, M.P. The traumatic impact of job loss and job search in the aftermath of COVID-19. Psychol. Trauma Theory Res. Pract. Policy 2020, 12, S180–S182. [Google Scholar] [CrossRef]
- Oksanen, A.; Kaakinen, M.; Latikka, R.; Savolainen, I.; Savela, N.; Koivula, A. Regulation and Trust: 3-Month Follow-up Study on COVID-19 Mortality in 25 European Countries. JMIR Public Health Surveill. 2020, 6, e19218. [Google Scholar] [CrossRef]
- Gavi, the Vaccine Alliance. The Gavi COVAX Advance Market Commitment: An Investment Opportunity. Available online: https://www.gavi.org/investment-opportunity-gavi-covax-amc (accessed on 24 June 2021).
- Honein, M.A.; Christie, A.; Rose, D.A.; Brooks, J.T.; Meaney-Delman, D.; Cohn, A.; Sauber-Schatz, E.K.; Walker, A.; McDonald, L.C.; Liburd, L.C.; et al. Summary of Guidance for Public Health Strategies to Address High Levels of Community Transmission of SARS-CoV-2 and Related Deaths, December. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1860–1867. [Google Scholar] [CrossRef]
- World Health Organization (WHO). WHO SAGE Roadmap for Prioritizing Uses of Covid-19 Vaccines in the Context of Limited Supply. Version 1. Geneva, 13 November. Available online: https://cdn.who.int/media/docs/default-source/immunization/sage/covid/sage-prioritization-roadmap-covid19-vaccines_31a59ccd-1fbf-4a36-a12f-73344134e49d.pdf?sfvrsn=bf227443_36&download=true (accessed on 16 April 2021).
- Coronavirus Disease (COVID-19): Vaccines. Available online: https://www.who.int/news-room/q-a-detail/coronavirus-disease-(covid-19)-vaccines (accessed on 25 May 2021).
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Sadoff, J.; Gray, G.; Vandebosch, A.; Cárdenas, V.; Shukarev, G.; Grinsztejn, B.; Goepfert, P.A.; Truyers, C.; Fennema, H.; Spiessens, B.; et al. Safety and Efficacy of Single-Dose Ad26.COV2.S Vaccine against Covid-19. N. Engl. J. Med. 2021, 384, 2187–2201. [Google Scholar] [CrossRef]
- Xia, S.; Zhang, Y.; Wang, Y.; Wang, H.; Yang, Y.; Gao, G.F.; Tan, W.; Wu, G.; Xu, M.; Lou, Z.; et al. Safety and immunogenicity of an inactivated SARS-CoV-2 vaccine, BBIBP-CorV: A randomised, double-blind, placebo-controlled, phase 1/2 trial. Lancet Infect. Dis. 2021, 21, 39–51. [Google Scholar] [CrossRef]
- Conti, P.; Caraffa, A.; Gallenga, C.E.; Kritas, S.K.; Frydas, I.; Younes, A.; Di Emidio, P.; Tetè, G.; Pregliasco, F.; Ronconi, G. The British variant of the new coronavirus-19 (Sars-Cov-2) should not create a vaccine problem. J. Biol. Regul. Homeost. Agents 2021, 35, 1–4. [Google Scholar]
- Binagwaho, A.; Mathewos, K.; Davis, S. Equitable and Effective Distribution of the COVID-19 Vaccines—A Scientific and Moral Obligation. Int. J. Health Policy Manag. 2021. [Google Scholar] [CrossRef]
- Forni, G.; Mantovani, A. COVID-19 vaccines: Where we stand and challenges ahead. Cell Death Differ. 2021, 28, 626–639. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Novel Coronavirus (2019-Ncov) Advice for the Public. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public (accessed on 1 October 2020).
- Cowling, B.J.; Ali, S.T.; Ng, T.W.Y.; Tsang, T.K.; Li, J.C.M.; Fong, M.W.; Liao, Q.; Kwan, M.Y.W.; Lee, S.L.; Chiu, S.S.; et al. Impact assessment of non-pharmaceutical interventions against coronavirus disease 2019 and influenza in Hong Kong: An observational study. Lancet Public Health 2020, 5, e279–e288. [Google Scholar] [CrossRef]
- Prem, K.; Liu, Y.; Russell, T.W.; Kucharski, A.J.; Eggo, R.M.; Davies, N.; Jit, M.; Klepac, P.; Flasche, S.; Clifford, S.; et al. The effect of control strategies to reduce social mixing on outcomes of the COVID-19 epidemic in Wuhan, China: A modelling study. Lancet Public Health 2020, 5, e261–e270. [Google Scholar] [CrossRef] [Green Version]
- Coroiu, A.; Moran, C.; Campbell, T.; Geller, A.C. Barriers and facilitators of adherence to social distancing recommendations during COVID-19 among a large international sample of adults. PLoS ONE 2020, 15, e0239795. [Google Scholar] [CrossRef]
- Haischer, M.H.; Beilfuss, R.; Hart, M.R.; Opielinski, L.; Wrucke, D.; Zirgaitis, G.; Uhrich, T.D.; Hunter, S.K. Who is wearing a mask? Gender-, age-, and location-related differences during the COVID-19 pandemic. PLoS ONE 2020, 15, e0240785. [Google Scholar] [CrossRef]
- Islam, J.Y.; Vidot, D.C.; Camacho-Rivera, M. Determinants of COVID-19 preventive behaviours among adults with chronic diseases in the USA: An analysis of the nationally representative COVID-19 impact survey. BMJ Open 2021, 11, e044600. [Google Scholar] [CrossRef]
- Lin, Y.; Hu, Z.; Zhao, Q.; Alias, H.; Danaee, M.; Wong, L.P. Understanding COVID-19 vaccine demand and hesitancy: A nationwide online survey in China. PLoS Negl. Trop. Dis. 2020, 14, e0008961. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, J.B.; Bell, R.A. Predictors of intention to vaccinate against COVID-19: Results of a nationwide survey. Vaccine 2021, 39, 1080–1086. [Google Scholar] [CrossRef]
- Sherman, S.M.; Smith, L.E.; Sim, J.; Amlôt, R.; Cutts, M.; Dasch, H.; Rubin, G.J.; Sevdalis, N. COVID-19 vaccination intention in the UK: Results from the COVID-19 vaccination acceptability study (CoVAccS), a nationally representative cross-sectional survey. Hum. Vaccines Immunother. 2021, 17, 1612–1621. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.C.; Fang, Y.; Cao, H.; Chen, H.; Hu, T.; Chen, Y.; Zhou, X.; Wang, Z. Behavioral Intention to Receive a COVID-19 Vaccination among Chinese Factory Workers: Cross-sectional Online Survey. J. Med. Internet Res. 2021, 23, e24673. [Google Scholar] [CrossRef]
- Salmon, D.A.; Dudley, M.Z.; Brewer, J.; Kan, L.; Gerber, J.E.; Budigan, H.; Proveaux, T.M.; Bernier, R.; Rimal, R.; Schwartz, B. COVID-19 vaccination attitudes, values and intentions among United States adults prior to emergency use authorization. Vaccine 2021, 39, 2698–2711. [Google Scholar] [CrossRef] [PubMed]
- Schmid, P.; Rauber, D.; Betsch, C.; Lidolt, G.; Denker, M.-L. Barriers of Influenza Vaccination Intention and Behavior—A Systematic Review of Influenza Vaccine Hesitancy, 2005. PLoS ONE 2017, 12, e0170550. [Google Scholar] [CrossRef]
- Ling, M.; Kothe, E.J.; Mullan, B.A. Predicting intention to receive a seasonal influenza vaccination using Protection Motivation Theory. Soc. Sci. Med. 2019, 233, 87–92. [Google Scholar] [CrossRef] [Green Version]
- Rogers, R.W. A Protection Motivation Theory of Fear Appeals and Attitude Change. J. Psychol. 1975, 91, 93–114. [Google Scholar] [CrossRef]
- Bish, A.; Yardley, L.; Nicoll, A.; Michie, S. Factors associated with uptake of vaccination against pandemic influenza: A systematic review. Vaccine 2011, 29, 6472–6484. [Google Scholar] [CrossRef]
- Camerini, A.-L.; Diviani, N.; Fadda, M.; Schulz, P.J. Using protection motivation theory to predict intention to adhere to official MMR vaccination recommendations in Switzerland. SSM Popul. Health 2019, 7, 100321. [Google Scholar] [CrossRef]
- Schulz, P.J.; Hartung, U. Unsusceptible to Social Communication? The Fixture of the Factors Predicting Decisions on Different Vaccinations. Health Commun. 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Floyd, D.L.; Prentice-Dunn, S.; Rogers, R.W. A Meta-Analysis of Research on Protection Motivation Theory. J. Appl. Soc. Psychol. 2000, 30, 407–429. [Google Scholar] [CrossRef]
- Weston, D.; Ip, A.; Amlôt, R. Examining the application of behaviour change theories in the context of infectious disease outbreaks and emergency response: A review of reviews. BMC Public Health 2020, 20, 1–19. [Google Scholar] [CrossRef]
- Vetter, V.; Denizer, G.; Friedland, L.R.; Krishnan, J.; Shapiro, M. Understanding modern-day vaccines: What you need to know. Ann. Med. 2018, 50, 110–120. [Google Scholar] [CrossRef] [PubMed]
- Prasetyo, Y.T.; Castillo, A.M.; Salonga, L.J.; Sia, J.A.; Seneta, J.A. Factors affecting perceived effectiveness of COVID-19 prevention measures among Filipinos during Enhanced Community Quarantine in Luzon, Philippines: Integrating Protection Motivation Theory and extended Theory of Planned Behavior. Int. J. Infect. Dis. 2020, 99, 312–323. [Google Scholar] [CrossRef] [PubMed]
- Okuhara, T.; Okada, H.; Kiuchi, T. Predictors of Staying at Home during the COVID-19 Pandemic and Social Lockdown based on Protection Motivation Theory: A Cross-sectional Study in Japan. Health 2020, 8, 475. [Google Scholar] [CrossRef]
- Farooq, A.; Laato, S.; Islam, A.K.M.N. Impact of Online Information on Self-Isolation Intention During the COVID-19 Pandemic: Cross-Sectional Study. J. Med. Internet Res. 2020, 22, e19128. [Google Scholar] [CrossRef]
- Hromatko, I.; Tonković, M.; Vranic, A. Trust in Science, Perceived Vulnerability to Disease, and Adherence to Pharmacological and Non-pharmacological COVID-19 Recommendations. Front. Psychol. 2021, 12, 664554. [Google Scholar] [CrossRef]
- Rad, R.E.; Mohseni, S.; Takhti, H.K.; Azad, M.H.; Shahabi, N.; Aghamolaei, T.; Norozian, F. Application of the protection motivation theory for predicting COVID-19 preventive behaviors in Hormozgan, Iran: A cross-sectional study. BMC Public Health 2021, 21, 1–11. [Google Scholar] [CrossRef]
- Kowalski, R.M.; Black, K.J. Protection Motivation and the COVID-19 Virus. Health Commun. 2021, 36, 15–22. [Google Scholar] [CrossRef]
- Wang, P.-W.; Ahorsu, D.; Lin, C.-Y.; Chen, I.-H.; Yen, C.-F.; Kuo, Y.-J.; Griffiths, M.; Pakpour, A. Motivation to Have COVID-19 Vaccination Explained Using an Extended Protection Motivation Theory among University Students in China: The Role of Information Sources. Vaccines 2021, 9, 380. [Google Scholar] [CrossRef] [PubMed]
- Leng, A.; Maitland, E.; Wang, S.; Nicholas, S.; Liu, R.; Wang, J. Individual preferences for COVID-19 vaccination in China. Vaccine 2021, 39, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.-J.; Yen, C.-F.; Chang, Y.-P.; Wang, P.-W. Comparisons of Motivation to Receive COVID-19 Vaccination and Related Factors between Frontline Physicians and Nurses and the Public in Taiwan: Applying the Extended Protection Motivation Theory. Vaccines 2021, 9, 528. [Google Scholar] [CrossRef] [PubMed]
- National Center for High-Performance Computing. Taiwan Reports of the COVID-19 Pandemic. Available online: https://covid-19.nchc.org.tw/dt_005-covidTable_taiwan.php (accessed on 28 May 2021).
- Liao, Q.; Cowling, B.J.; Lam, W.W.T.; Ng, D.M.W.; Fielding, R. Anxiety, worry and cognitive risk estimate in relation to protective behaviors during the 2009 influenza A/H1N1 pandemic in Hong Kong: Ten cross-sectional surveys. BMC Infect. Dis. 2014, 14, 169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ko, N.-Y.; Lu, W.-H.; Chen, Y.-L.; Li, D.-J.; Chang, Y.-P.; Wang, P.-W.; Yen, C.-F. Cognitive, Affective, and Behavioral Constructs of COVID-19 Health Beliefs: A Comparison Between Sexual Minority and Heterosexual Individuals in Taiwan. Int. J. Environ. Res. Public Health 2020, 17, 4282. [Google Scholar] [CrossRef] [PubMed]
- Yeh, Y.-C.; Chen, I.-H.; Ahorsu, D.; Ko, N.-Y.; Chen, K.-L.; Li, P.-C.; Yen, C.-F.; Lin, C.-Y.; Griffiths, M.; Pakpour, A. Measurement Invariance of the Drivers of COVID-19 Vaccination Acceptance Scale: Comparison between Taiwanese and Mainland Chinese-Speaking Populations. Vaccines 2021, 9, 297. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, J.; Beymer, P.; Anderson, D.; Van Lissa, C.; Schmidt, J. tidyLPA: An R Package to Easily Carry Out Latent Profile Analysis (LPA) Using Open-Source or Commercial Software. J. Open Source Softw. 2018, 3, 978. [Google Scholar] [CrossRef] [Green Version]
- Celeux, G.; Soromenho, G. An entropy criterion for assessing the number of clusters in a mixture model. J. Classif. 1996, 13, 195–212. [Google Scholar] [CrossRef] [Green Version]
- Tein, J.-Y.; Coxe, S.; Cham, H. Statistical Power to Detect the Correct Number of Classes in Latent Profile Analysis. Struct. Equ. Model. Multidiscip. J. 2013, 20, 640–657. [Google Scholar] [CrossRef]
- Wu, A.M.; Lau, J.T.; Ma, Y.-L.; Cheng, K.-M.; Lau, M.M. A longitudinal study using parental cognitions based on the theory of planned behavior to predict childhood influenza vaccination. J. Infect. Public Health 2020, 13, 970–979. [Google Scholar] [CrossRef] [PubMed]
- Ng, T.W.; Cowling, B.J.; So, H.C.; Ip, D.K.; Liao, Q. Testing an integrative theory of health behavioural change for predicting seasonal influenza vaccination uptake among healthcare workers. Vaccine 2020, 38, 690–698. [Google Scholar] [CrossRef]
- Meyer, D.; Shearer, M.P.; Chih, Y.-C.; Hsu, Y.-C.; Lin, Y.-C.; Nuzzo, J.B. Taiwan’s Annual Seasonal Influenza Mass Vaccination Program—Lessons for Pandemic Planning. Am. J. Public Health 2018, 108, S188–S193. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.-Y.; Lee, S.-D.; Lo, K.-J. Legend of hepatitis B vaccination: The Taiwan experience. J. Gastroenterol. Hepatol. 2004, 19, 121–126. [Google Scholar] [CrossRef]
- Taiwan News. Taiwan Becoming Less Likely to Purchase COVID Vaccine from BioNTech. Available online: https://www.taiwannews.com.tw/en/news/4163283 (accessed on 28 May 2021).
- Taiwan Center for Disease Control. Central Epidemic Command Center Lists 10 Priority Groups, with First 3 to Receive Doses Immediately. Available online: https://www.cdc.gov.tw/En (accessed on 28 May 2021).
- Jordan, R.E.; Adab, P.; Cheng, K.K. COVID-19: Risk factors for severe disease and death. BMJ 2020, 368, m1198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daoust, J.-F. Elderly people and responses to COVID-19 in 27 Countries. PLoS ONE 2020, 15, e0235590. [Google Scholar] [CrossRef]
- Bobkowski, P.; Smith, J. Social media divide: Characteristics of emerging adults who do not use social network websites. Media Cult. Soc. 2013, 35, 771–781. [Google Scholar] [CrossRef]
- Alessi, E.J.; Martin, J.I. Conducting an Internet-based Survey: Benefits, Pitfalls, and Lessons Learned. Soc. Work Res. 2010, 34, 122–128. [Google Scholar] [CrossRef]
- Daoust, J.-F.; Nadeau, R.; Dassonneville, R.; Lachapelle, E.; Bélanger, É.; Savoie, J.; Van Der Linden, C. How to Survey Citizens’ Compliance with COVID-19 Public Health Measures: Evidene from Three Survey Experiments. J. Exp. Polit. Sci. 2020, 1–8. [Google Scholar] [CrossRef]
- Daoust, J.-F.; Bélanger, É.; Dassonneville, R.; Lachapelle, E.; Nadeau, R.; Becher, M.; Brouard, S.; Foucault, M.; Hönnige, C.; Stegmueller, D. A guilt-free strategy increases self-reported non-compliance with COVID-19 preventive measures: Experimental evidence from 12 countries. PLoS ONE 2021, 16, e0249914. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Measures | Items | Response Scale |
|---|---|---|
| Motivation to receive a COVID-19 vaccination | Please rate your current willingness to receive a COVID-19 vaccine: | 1 (very low) to 10 (very high) |
| Motivation to adopt protective behaviors | In the past week, did you (1) avoid going to crowded places, (2) wash your hands more often, and (3) wear a mask more often? | Each item was rated as 0 (no) or 1 (yes) and summed to obtain a total score |
| Constructs of PMT | ||
| Perceived severity | Item 1: Please rate the current level of your concern about COVID-19: | 1 (very mild) to 10 (very severe) |
| Item 2: How serious is COVID-19 relative to SARS? | 1 (much less serious) to 5 (much more serious) | |
| Perceived vulnerability | Item 1: How likely do you think you are to contract COVID-19 over the next month? | 1 (very unlikely) to 7 (very likely) |
| Item 2: If you were to develop flu-like symptoms tomorrow, would you be worried? | 1 (not at all worried) to 7 (extremely worried) | |
| Item 3: In the past week, how often have you worried about catching COVID-19? | 1 (never) to 5 (all the time) | |
| Item 4: What do you think your chances are of getting COVID-19 over the next month are compared with others outside your family? | 1 (no chance) to 7 (certain) | |
| Self-efficacy of COVID-19 vaccination | I can choose whether to receive a COVID-19 jab or not. | 1 (strongly disagree) to 7 (strongly agree) |
| Response efficacy of COVID-19 vaccination | Item 1: Vaccination is a very effective way to protect me against COVID-19. | 1 (strongly disagree) to 7 (strongly agree) |
| Item 2: It is important that I receive the COVID-19 vaccine. | ||
| Item 3: Vaccination greatly reduces my risk of catching COVID-19. | ||
| Item 4: The COVID-19 vaccine plays an important role in protecting my life and that of others. | ||
| Item 5: The COVID-19 shot will make an important contribution to my health and well-being. | ||
| Item 6: Receiving the COVID-19 shot has a positive influence on my health. | ||
| Response cost of COVID-19 vaccination | (1) Safety and possible side effects of vaccine, (2) cost of vaccine, and (3) time spent on vaccination will influence my willingness to get vaccinated for COVID-19. | 1 (strongly disagree) to 4 (strongly agree) |
| Knowledge about COVID-19 vaccination | Item 1: I understand how the COVID-19 shot helps my body fight the COVID-19 virus. | 1 (strongly disagree) to 7 (strongly agree) |
| Item 2: I understand how vaccination protects me from COVID-19. | ||
| Item 3: How the COVID-19 jab works to protect my health is a mystery to me. * | ||
| Previous vaccination for seasonal influenza | Did you receive an influenza vaccination in recent years? | 1 (never) to 4 (always) |
| No. of Classes | AIC | BIC | Entropy | BLRT (p-Value) |
|---|---|---|---|---|
| 1 | 5948.51 | 5968.33 | 1 | - |
| 2 | 5954.41 | 5989.09 | 0.21 | 0.48 |
| 3 | 5590.48 | 5640.02 | 0.74 | 0.01 |
| 4 | 5596.53 | 5660.93 | 0.6 | 0.67 |
| 5 | 5497.76 | 5577.02 | 0.78 | 0.01 |
| 6 | 5497.01 | 5591.13 | 0.73 | 0.02 |
| Variable | High Motivations for Vaccination and High for Preventive Behaviors (N = 417) | Low Motivations for Vaccination and Low for Preventive Behaviors (N = 123) | OR 1 c (95% CI) | High Motivations for Vaccination but Low for Preventive Behaviors (N = 507) | OR 2 c (95% CI) |
|---|---|---|---|---|---|
| Sociodemographics | |||||
| Gender a | |||||
| Female | 250 (60.0%) | 81 (65.9%) | 1.00 | 286 (56.4%) | 1.00 |
| Male | 167 (40.0%) | 42 (34.1%) | 0.78 (0.51–1.18) | 221 (43.6%) | 1.16 (0.89–1.50) |
| Age a | |||||
| <35 | 191 (45.8%) | 62 (50.4%) | 1.00 | 289 (57.0%) | 1.00 |
| 35–49 | 175 (42.0%) | 46 (37.4%) | 0.81 (0.53–1.25) | 187 (36.9%) | 0.71 (0.54–0.93) * |
| ≥50 | 51 (12.2%) | 15 (12.2%) | 0.91 (0.48–1. 72) | 31 (6.1%) | 0.40 (0.25–0.65) *** |
| Education levels a | |||||
| High school or below | 43 (10.3%) | 13 (10.6%) | 1.00 | 54 (10.7%) | 1.00 |
| Bachelor’s degree | 247 (59.2%) | 85 (69.1%) | 1.14 (0.58–2.22) | 335 (66.1%) | 1.08 (0.70–1.67) |
| Master’s degree and above | 127 (30.5%) | 25 (20.3%) | 0.65 (0.31–1.38) | 118 (23.3%) | 0.74 (0.46–1.19) |
| PMT constructsb | |||||
| Perceived vulnerability | 7.8 ± 3.3 | 5.6 ± 3.3 | 0.81 (0.76–0.87) *** | 6.4 ± 3.1 | 0.88 (0.84–0.92) ** |
| Perceived severity | 7.6 ± 3.0 | 5.6 ± 2.9 | 0.79 (0.73–0.85) *** | 6.3 ± 2.9 | 0.85 (0.81–0.89) ** |
| Self-efficacy to have vaccination | 5.0 ± 1.1 | 4.6 ± 1.8 | 0.75 (0.64–0.88) *** | 5.0 ± 1.0 | 0.96 (0.85–1.09) |
| Response efficacy of vaccination | 25.4 ± 6.8 | 15.7 ± 6.5 | 0.81 (0.78–0.84) *** | 25.7 ± 5.6 | 1.01 (0.98–1.03) |
| Response cost of vaccination | 5.6 ± 1.9 | 5.6 ± 2.0 | 0.96 (0.87–1.07) | 6.0 ± 1.8 | 1.11 (1.04–1.19) ** |
| Knowledge about vaccination | 11.3 ± 4.0 | 8.8 ± 4.0 | 0.85 (0.80–0.90) ** | 11.9 ± 3.7 | 1.03 (1.00–1.07) |
| Previous vaccination for seasonal influenza | 1.5 ± 1.3 | 1.0 ± 1.3 | 0.72 (0.61–0.85) *** | 1.5 ± 1.3 | 1.02 (0.92–1.13) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.-L.; Lin, Y.-J.; Chang, Y.-P.; Chou, W.-J.; Yen, C.-F. Differences in the Protection Motivation Theory Constructs between People with Various Latent Classes of Motivation for Vaccination and Preventive Behaviors against COVID-19 in Taiwan. Int. J. Environ. Res. Public Health 2021, 18, 7042. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137042
Chen Y-L, Lin Y-J, Chang Y-P, Chou W-J, Yen C-F. Differences in the Protection Motivation Theory Constructs between People with Various Latent Classes of Motivation for Vaccination and Preventive Behaviors against COVID-19 in Taiwan. International Journal of Environmental Research and Public Health. 2021; 18(13):7042. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137042
Chicago/Turabian StyleChen, Yi-Lung, Yen-Ju Lin, Yu-Ping Chang, Wen-Jiun Chou, and Cheng-Fang Yen. 2021. "Differences in the Protection Motivation Theory Constructs between People with Various Latent Classes of Motivation for Vaccination and Preventive Behaviors against COVID-19 in Taiwan" International Journal of Environmental Research and Public Health 18, no. 13: 7042. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137042