
Haemoglobin Levels in Early Life among Infants with and without Retinopathy of Prematurity

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Blencowe, H.; Lawn, J.E.; Vazquez, T.; Fielder, A.; Gilbert, C. Preterm-associated visual impairment and estimates of retinopathy of prematurity at regional and global levels for 2010. Pediatr. Res. 2013, 74 (Suppl. S1), 35–49. [Google Scholar] [CrossRef] [Green Version]
- Gilbert, C.; Fielder, A.; Gordillo, L.; Quinn, G.; Semiglia, R.; Visintin, P.; Zin, A. Characteristics of Infants with Severe Retinopathy of Prematurity in Countries with Low, Moderate, and High Levels of Development: Implications for Screening Programs. Pediatrics 2005, 115, e518–e525. [Google Scholar] [CrossRef] [Green Version]
- William, V. Final results of the Early Treatment for Retinopathy of Prematurity (ETROP) randomized trial. Trans. Am. Ophthalmol. Soc. 2004, 102, 233–250. [Google Scholar]
- American Academy of Ophthalmology. Retinopathy of Prematurity. Available online: https://eyewiki.aao.org/Retinopathy_of_Prematurity#Pathophysiology (accessed on 19 January 2021).
- AlBalawi, H.B.; AlBalawi, N.S.; AlSuhaimi, N.A.; AlBalawi, A.A.; Alatawi, A.S.; Mirghani, H.O.; Al-Dhibi, H.A.; Alenezi, S.H. Incidence and risk factors for retinopathy of prematurity in Tabuk city, KSA. Middle East Afr. J. Ophthalmol. 2020, 27, 105–109. [Google Scholar] [CrossRef]
- Al-Qahtani, B.; Al-Otaibi, M.; Alabdulajabbar, K.; Selayem, N.B.; AlShehri, W.; Omair, A.; AlSaif, S. Retinopathy of Prematurity Incidence and Risk Factors in a Tertiary Hospital in Riyadh, Saudi Arabia. Middle East Afr. J. Ophthalmol. 2019, 26, 235–239. [Google Scholar] [CrossRef]
- Braimah, I.Z.; Enweronu-Laryea, C.; Sackey, A.H.; Kenu, E.; Agyabeng, K.; Ofori-Adjei, I.-O.D.-B.; Beyuo, V.; Oku, A.; Essuman, V.A. Incidence and risk factors of retinopathy of prematurity in Korle-Bu Teaching Hospital: A baseline prospective study. BMJ Open 2020, 10, e035341. [Google Scholar] [CrossRef]
- Huang, H.-B.; Chen, Y.-H.; Wu, J.; Hicks, M.; Yi, Y.-Z.; Zhang, Q.-S.; Chow, C.-B.; Cheung, P.-Y. Early Risk Factors for Retinopathy of Prematurity in Very and Extremely Preterm Chinese Neonates. Front. Pediatr. 2020, 8, 553519. [Google Scholar] [CrossRef]
- Siswanto, J.E.; Ronoatmodjo, S.; Adisasmita, A.; Soemantri, A.; Sitorus, R.S.; Sauer, P.J.J. Risk factors for the development and progression of retinopathy of prematurity in preterm infants in Indonesia. J. Neonatal Perinat. Med. 2020, 13, 253–260. [Google Scholar] [CrossRef]
- American Academy of Ophthalmology. New ROP Screening Criteria Validated. Available online: https://www.aao.org/eyenet/article/new-rop-screening-criteria-validated (accessed on 27 March 2021).
- Binenbaum, G.; Tomlinson, L.A.; de Alba Campomanes, A.G.; Bell, E.F.; Donohue, P.; Morrison, D.; Quinn, G.E.; Repka, M.X.; Rogers, D.; Yang, M.B.; et al. Validation of the Postnatal Growth and Retinopathy of Prematurity Screening Criteria. JAMA Ophthalmol. 2020, 138, 31–37. [Google Scholar] [CrossRef]
- Chong, C.; McGhee, C.N.J.; Dai, S.H. Causes of childhood low vision and blindness in New Zealand. Clin. Exp. Ophthalmol. 2019, 47, 165–170. [Google Scholar] [CrossRef]
- López Ulloa, J.A.L.; Burn, H.; Beauregard, A.M. Causes of Blindness and Visual Impairment in Early Childhood at a Low Vision Service in Mexico City: A 15-year Review. Ophthalmic Epidemiol. 2021, 10, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, J.; Asamoah, F.K.; Singhvi, D.; Kwan, A.W.; Morris, J.K.; Aladangady, N. Haemoglobin level at birth is associated with short term outcomes and mortality in preterm infants. BMC Med. 2015, 13, 16. [Google Scholar] [CrossRef] [Green Version]
- Englert, J.; Saunders, R.A.; Purohit, D.; Hulsey, T.C.; Ebeling, M. The effect of anemia on retinopathy of prematurity in extremely low birth weight infants. J. Perinatol. 2001, 21, 21–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gotru, S.; Ahlers-Schmidt, C.R.; Delmore, P.; Shaw, J.; Bloom, B.T. The absolute nucleated red blood cell (aNRBC) count at birth is not an indicator for retinopathy of prematurity (ROP). J. Perinatol. 2013, 33, 21–24. [Google Scholar] [CrossRef]
- Lundgren, P.; Athikarisamy, S.E.; Patole, S.; Lam, G.C.; Smith, L.E.; Simmer, K. Duration of anaemia during the first week of life is an independent risk factor for retinopathy of prematurity. Acta Paediatr. 2018, 107, 759–766. [Google Scholar] [CrossRef]
- Lundgren, P.; Hellgren, G.; Pivodic, A.; Savman, K.; Smith, L.E.H.; Hellstrom, A. Erythropoietin serum levels, versus anaemia as risk factors for severe retinopathy of prematurity. Pediatr. Res. 2019, 86, 276–282. [Google Scholar] [CrossRef]
- Stutchfield, C.J.; Jain, A.; Odd, D.; Williams, C.; Markham, R. Foetal haemoglobin, blood transfusion, and retinopathy of prematurity in very preterm infants: A pilot prospective cohort study. Eye 2017, 31, 1451–1455. [Google Scholar] [CrossRef]
- Zhu, Z.; Hua, X.; Yu, Y.; Zhu, P.; Hong, K.; Ke, Y. Effect of red blood cell transfusion on the development of retinopathy of prematurity: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0234266. [Google Scholar] [CrossRef]
- An International Classification of Retinopathy of Prematurity. The Committee for the Classification of Retinopathy of Prematurity. Arch. Ophthalmol. 1984, 102, 1130–1134. [Google Scholar] [CrossRef]
- International Committee for the Classification of Retinopathy of Prematurity. The international classification of retinopathy of prematurity revisited. Arch. Ophthalmol. 2005, 123, 991–999. [Google Scholar] [CrossRef]
- Early Treatment For Retinopathy of Prematurity Cooperative Group. Revised Indications for the Treatment of Retinopathy of Prematurity: Results of the early treatment for retinopathy of prematurity randomized trial. Arch. Ophthalmol. 2003, 121, 1684–1694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawn, J.E.; Davidge, R.; Paul, V.K.; Von Xylander, S.; de Graft Johnson, J.; Costello, A.; Kinney, M.V.; Segre, J.; Molyneux, L. Born Too Soon: Care for the preterm baby. Reprod. Health 2013, 10, S5. [Google Scholar] [CrossRef] [Green Version]
- Chawanpaiboon, S.; Vogel, J.P.; Moller, A.-B.; Lumbiganon, P.; Petzold, M.; Hogan, D.; Landoulsi, S.; Jampathong, N.; Kongwattanakul, K.; Laopaiboon, M.; et al. Global, regional, and national estimates of levels of preterm birth in 2014: A systematic review and modelling analysis. Lancet Glob. Health 2019, 7, e37–e46. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Stahl, A.; Hellstrom, A.; Smith, L.E. Current update on retinopathy of prematurity: Screening and treatment. Curr. Opin. Pediatr. 2011, 23, 173–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarpal, S.; Ashat, M.; Puri, S. Screening of retinopathy of prematurity: A neglected public health issue. Ann. Med Health Sci. Res. 2014, 4, S65–S66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashton, N. Oxygen and the retinal blood vessels. Trans. Ophthalmol. Soc. U. K. 1980, 100, 359–362. [Google Scholar] [PubMed]
- Patz, A. Oxygen Studies in Retrolental Fibroplasia. IV. Clinical and experimental observations. Am. J. Ophthalmol. 1954, 38, 291–308. [Google Scholar] [CrossRef]
- Bossi, E.; Koerner, F.; Flury, B.; Zulauf, M. Retinopathy of prematurity: A risk factor analysis with univariate and multivariate statistics. Helv. Paediatr. Acta 1984, 39, 307–317. [Google Scholar]
- Akyüz Ünsal, A.I.; Key, Ö.; Güler, D.; Kurt Omurlu, I.; Anık, A.; Demirci, B.; Dündar, S. Can Complete Blood Count Parameters Predict Retinopathy of Prematurity? Turk. J. Ophthalmol. 2020, 50, 87–93. [Google Scholar] [CrossRef]
- Brown, M.S.; Phibbs, R.H.; Garcia, J.F.; Dallman, P.R. Postnatal changes in erythropoietin levels in untransfused premature infants. J. Pediatr. 1983, 103, 612–617. [Google Scholar] [CrossRef]
- Widness, J.A. Pathophysiology of Anemia During the Neonatal Period, Including Anemia of Prematurity. NeoReviews 2008, 9, e520. [Google Scholar] [CrossRef] [Green Version]
- Muady, G.F.; Bitterman, H.; Laor, A.; Vardi, M.; Urin, V.; Ghanem-Zoubi, N. Hemoglobin levels and blood transfusion in patients with sepsis in Internal Medicine Departments. BMC Infect. Dis. 2016, 16, 569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kc, A.; Rana, N.; Målqvist, M.; Ranneberg, L.J.; Subedi, K.; Andersson, O. Effects of Delayed Umbilical Cord Clamping vs Early Clamping on Anemia in Infants at 8 and 12 Months: A randomized clinical trial. JAMA Pediatr. 2017, 171, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Datta, B.V.; Kumar, A.; Yadav, R. A Randomized Controlled Trial to Evaluate the Role of Brief Delay in Cord Clamping in Preterm Neonates (34–36 weeks) on Short-term Neurobehavioural Outcome. J. Trop. Pediatr. 2017, 63, 418–424. [Google Scholar] [CrossRef] [PubMed]
- Fenton, C.; McNinch, N.L.; Bieda, A.; Dowling, D.; Damato, E. Clinical Outcomes in Preterm Infants Following Institution of a Delayed Umbilical Cord Clamping Practice Change. Adv. Neonatal Care 2018, 18, 223–231. [Google Scholar] [CrossRef] [PubMed]
- Cibulskis, C.C.; Maheshwari, A.; Rao, R.; Mathur, A.M. Anemia of prematurity: How low is too low? J. Perinatol. 2021, 1–14. [Google Scholar] [CrossRef]
- Strauss, R.G.; Widness, J.A. Is There a Role for Autologous/Placental Red Blood Cell Transfusions in the Anemia of Prematurity? Transfus. Med. Rev. 2010, 24, 125–129. [Google Scholar] [CrossRef] [Green Version]
- Brooks, S.E.; Marcus, D.M.; Gillis, D.; Pirie, E.; Johnson, M.H.; Bhatia, J. The Effect of Blood Transfusion Protocol on Retinopathy of Prematurity: A Prospective, Randomized Study. Pediatrics 1999, 104, 514–518. [Google Scholar] [CrossRef]
- Lust, C.; Vesoulis, Z.; Jackups, R., Jr.; Liao, S.; Rao, R.; Mathur, A.M. Early red cell transfusion is associated with development of severe retinopathy of prematurity. J. Perinatol. 2019, 39, 393–400. [Google Scholar] [CrossRef]
- Dani, C.; Reali, M.F.; Bertini, G.; Martelli, E.; Pezzati, M.; Rubaltelli, F.F. The role of blood transfusions and iron intake on retinopathy of prematurity. Early Hum. Dev. 2001, 62, 57–63. [Google Scholar] [CrossRef]
- Ashton, N. Retinal angiogenesis in the human embryo. Br. Med Bull. 1970, 26, 103–106. [Google Scholar] [CrossRef] [PubMed]
- Patz, A. The role of oxygen in retrolental fibroplasia. Sinai Hosp. J. 1954, 3, 6–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michaelson, I.C. Retinal Circulation in Man and Animals. Br. J. Ophthalmol. 1954, 38, 441. [Google Scholar] [CrossRef] [Green Version]
- Owen, L.A.; Hartnett, M.E. Current Concepts of Oxygen Management in Retinopathy of Prematurity. J. Ophthalmic Vis. Res. 2014, 9, 94–100. [Google Scholar] [PubMed]
- Podraza, W. A new approach to neonatal medical management that could transform the prevention of retinopathy of prematurity: Theoretical considerations. Med. Hypotheses 2020, 137, 109541. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Tang, Y.; Zhu, T.; Li, Y.; Chun, H.; Qu, Y.; Mu, D. Cumulative evidence for association of sepsis and retinopathy of prematurity. Medicine 2019, 98, e17512. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Dammann, O. Perinatal infection, inflammation, and retinopathy of prematurity. Semin. Fetal Neonatal Med. 2012, 17, 26–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansen-Pupp, I.; Hellström-Westas, L.; Cilio, C.M.; Andersson, S.; Fellman, V.; Ley, D. Inflammation at birth and the insulin-like growth factor system in very preterm infants. Acta Paediatr. 2007, 96, 830–836. [Google Scholar] [CrossRef] [PubMed]
- Thissen, J.-P. How Proinflammatory Cytokines May Impair Growth and Cause Muscle Wasting. Horm. Res. Paediatr. 2007, 67 (Suppl. S1), 64–70. [Google Scholar] [CrossRef]
- Jacobo, S.M.P.; Kazlauskas, A. Insulin-like Growth Factor 1 (IGF-1) Stabilizes Nascent Blood Vessels. J. Biol. Chem. 2015, 290, 6349–6360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hellström, A.; Engström, E.; Hård, A.L.; Albertsson-Wikland, K.; Carlsson, B.; Niklasson, A.; Löfqvist, C.; Svensson, E.; Holm, S.; Ewald, U.; et al. Postnatal Serum Insulin-Like Growth Factor I Deficiency Is Associated With Retinopathy of Prematurity and Other Complications of Premature Birth. Pediatrics 2003, 112, 1016–1020. [Google Scholar] [CrossRef] [Green Version]
- Rogiers, P.; Zhang, H.; Leeman, M.; Nagler, J.; Neels, H.; Mélot, C.; Vincent, J.L. Erythropoietin response is blunted in critically ill patients. Intensiv. Care Med. 1997, 23, 159–162. [Google Scholar] [CrossRef] [PubMed]
- Hamad, A.E.; Moinuddin, O.; Blair, M.P.; Schechet, S.A.; Shapiro, M.J.; Quiram, P.A.; Mammo, D.A.; Berrocal, A.M.; Prakhunhungsit, S.; Cernichiaro-Espinosa, L.A.; et al. Late-Onset Retinal Findings and Complications in Untreated Retinopathy of Prematurity. Ophthalmol. Retin. 2020, 4, 602–612. [Google Scholar] [CrossRef] [PubMed]
- Vijayalakshmi, P. Ocular Morbidity Associated with Retinopathy of Prematurity in Treated and Untreated Eyes: A Review of the Literature and Data from a Tertiary Eye-care Center in Southern India. Indian Pediatr. 2016, 53 (Suppl. S2), S137–S142. [Google Scholar]
- Strauss, R.G. Anaemia of prematurity: Pathophysiology and treatment. Blood Rev. 2010, 24, 221–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Lim, Z.; Oo, K.T.; Tai, E.L.M.; Shatriah, I. Efficacy of WINROP as a Screening Tool for Retinopathy of Prematurity in the East Coast of Malaysia. Clin. Ophthalmol. 2020, 14, 1101–1106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, J.H.; Lofqvist, C.; Hellstrom, A.; Heo, H. Efficacy of the Screening Algorithm WINROP in a Korean Population of Preterm Infants. JAMA Ophthalmol. 2013, 131, 62–66. [Google Scholar] [CrossRef] [Green Version]
- Bai, Y.C.; Wu, R.; Chen, S.Z.; Wei, S.Y.; Chen, H.J.; Chen, Y.C.; Feng, S.F.; Lu, X.H. Efficacy of the WINROP algorithm for retinopathy of prematurity screening in Southern China. Int. J. Ophthalmol. 2021, 14, 127–132. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | ROP n= 31 | non-ROP n= 31 | p-Value |
|---|---|---|---|
| Birth weight in grams (mean ± SD) | 962.2 ± 167.9 | 960.6 ± 147.8 | 0.968 † |
| Gestational age in weeks (mean ± SD) | 27.5 ± 1.8 | 28.0 ± 1.4 | 0.443 † |
| Volume of blood transfusion in ml (mean ± SD) | 104.2 ± 62 | 53.9 ± 28 | <0.001 *† |
| Days of oxygen supplementation (mean ± SD) | 14.4 ± 17.1 | 3.1 ± 4.7 | 0.001 *† |
| Culture proven sepsis | 16 (51%) | 1 (3%) | <0.001 * |
| Intraventricular haemorrhage | 17 (54%) | 20 (64%) | 0.605 ‡ |
| Enterocolitis | 5 (16%) | 7 (22%) | 0.749 ‡ |
| Pneumonia | 10 (32%) | 8 (26%) | 0.780 ‡ |
| Congenital heart disease | 10 (32%) | 7 (22.5%) | 0.570 ‡ |
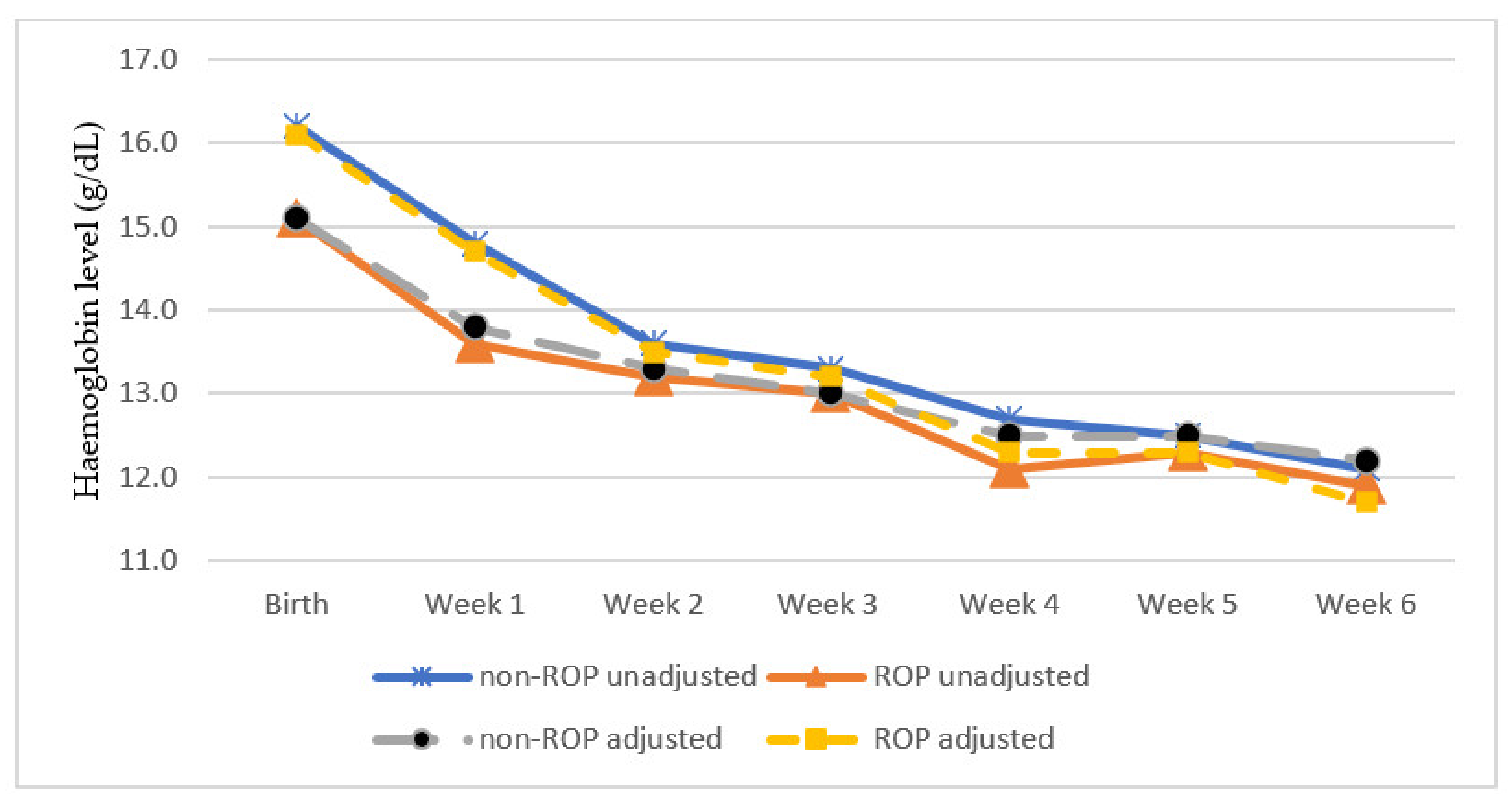
| Mean Haemoglobin (g/dL) | ||||
|---|---|---|---|---|
| Period | non-ROP n= 31 | ROP n= 31 | p Value 1 | p Value 2 |
| Birth | 16.2 ± 2.6 | 15.1 ± 1.7 | 0.057 | 0.158 |
| Week 1 | 14.8 ± 1.4 | 13.6 ± 1.4 | 0.002 * | 0.038 * |
| Week 2 | 13.6 ± 1.4 | 13.2 ± 1.2 | 0.259 | 0.496 |
| Week 3 | 13.3 ± 1.2 | 13.0 ± 1.3 | 0.430 | 0.490 |
| Week 4 | 12.7 ± 1.1 | 12.1 ± 0.9 | 0.036 * | 0.185 |
| Week 5 | 12.5 ± 0.9 | 12.3 ± 1.4 | 0.668 | 0.214 |
| Week 6 | 12.1 ± 1.0 | 11.9 ± 1.4 | 0.240 | 0.239 |
| Mean Haemoglobin (g/dL) | ||||
|---|---|---|---|---|
| Period | ROP not Requiring Treatment/no ROP n = 43 | ROP Requiring Treatment n = 19 | p-Value 1 | p-Value 2 |
| Birth | 16.0 ± 2.3 | 14.7 ± 1.9 | 0.033 * | 0.139 |
| Week 1 | 14.6 ± 1.4 | 13.3 ± 1.5 | 0.002 * | 0.219 |
| Week 2 | 13.5 ± 1.2 | 13.2 ± 1.1 | 0.311 | 0.120 |
| Week 3 | 13.4 ± 1.3 | 12.5 ± 0.8 | 0.012 * | 0.139 |
| Week 4 | 12.6 ± 1.0 | 11.9 ± 0.9 | 0.013 * | 0.458 |
| Week 5 | 12.4 ± 0.9 | 12.5 ± 1.6 | 0.790 | 0.771 |
| Week 6 | 12.1 ± 1.1 | 11.9 ± 1.6 | 0.378 | 0.091 |
| Name | Year | Sample Size | Country | Conclusions |
|---|---|---|---|---|
| Bossi et al. [30] | 1984 | 132 | Switzerland | Haemoglobin levels show no correlation with ROP. |
| Englert et al. [15] | 2001 | 107 | America | Anaemia is not an independent risk factor for severity of ROP. |
| Banerjee et al. [14] | 2015 | 920 | United Kingdom | Low haemoglobin at birth is associated with ROP in premature infants. Duration of anaemia during the first week of life is associated with an increased risk of developing ROP warranting treatment. |
| Lundgren et al. [17] | 2018 | 227 | Australia | Mean haemoglobin levels during the first week of life did not differ significantly between infants with ROP requiring treatment and controls after adjusting for confounders. |
| Lundgren et al. [18] | 2019 | 78 | Sweden | Anaemia during the first week of postnatal life is a significant risk factor for severe ROP. |
| Akyüz Ünsal et al. [31] | 2020 | 142 | Turkey | Haemoglobin levels in the first month of life are significantly lower in infants with ROP than those without ROP. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pheng, E.; Lim, Z.D.; Tai Li Min, E.; Rostenberghe, H.V.; Shatriah, I. Haemoglobin Levels in Early Life among Infants with and without Retinopathy of Prematurity. Int. J. Environ. Res. Public Health 2021, 18, 7054. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137054
Pheng E, Lim ZD, Tai Li Min E, Rostenberghe HV, Shatriah I. Haemoglobin Levels in Early Life among Infants with and without Retinopathy of Prematurity. International Journal of Environmental Research and Public Health. 2021; 18(13):7054. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137054
Chicago/Turabian StylePheng, Edwin, Zi Di Lim, Evelyn Tai Li Min, Hans Van Rostenberghe, and Ismail Shatriah. 2021. "Haemoglobin Levels in Early Life among Infants with and without Retinopathy of Prematurity" International Journal of Environmental Research and Public Health 18, no. 13: 7054. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137054