
Effect of Physical Guidance on Learning a Tracking Task in Children with Cerebral Palsy

 ,
, 
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Sample Size
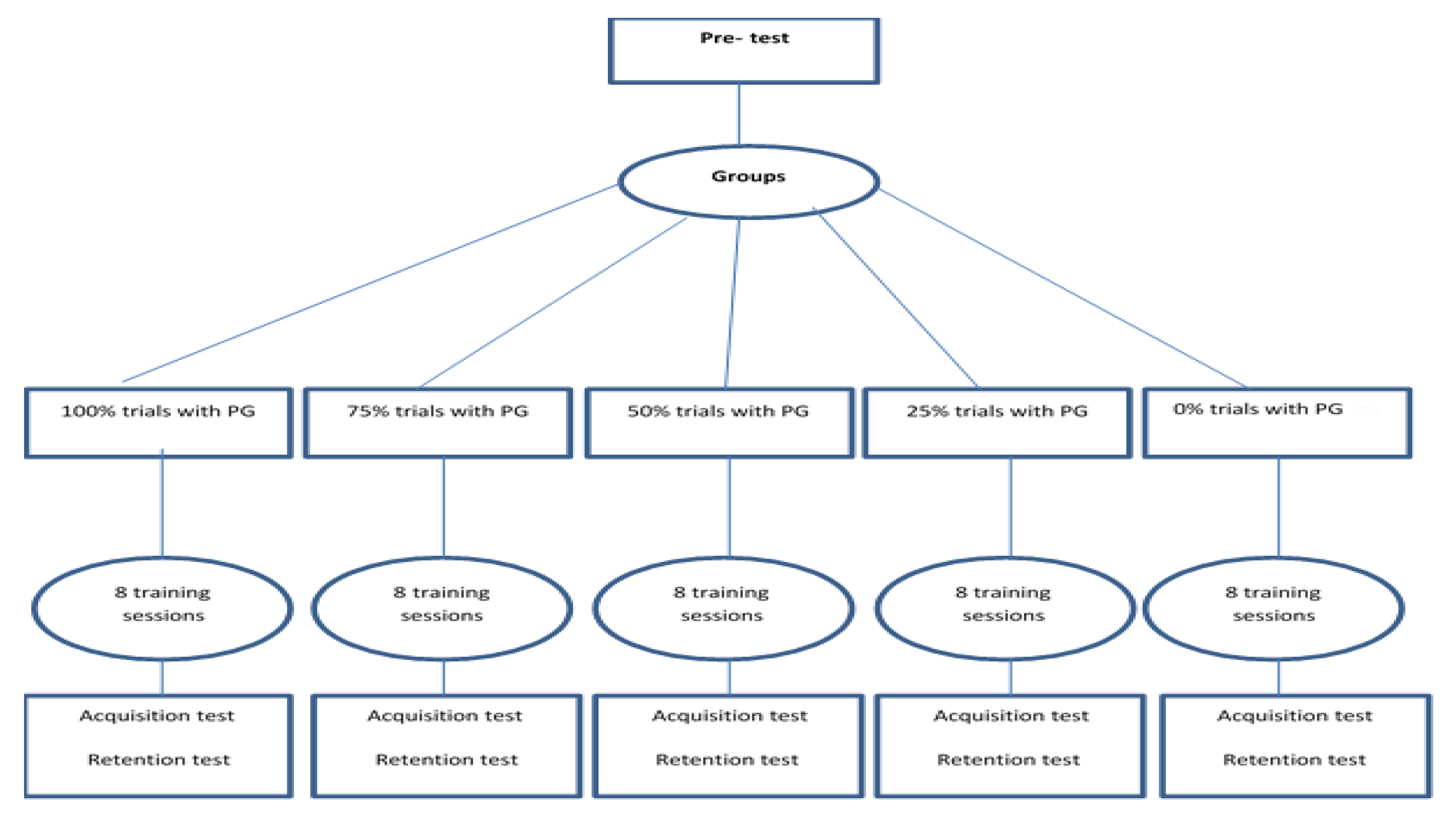
2.3. Procedure and Design
2.4. Statistical Analysis
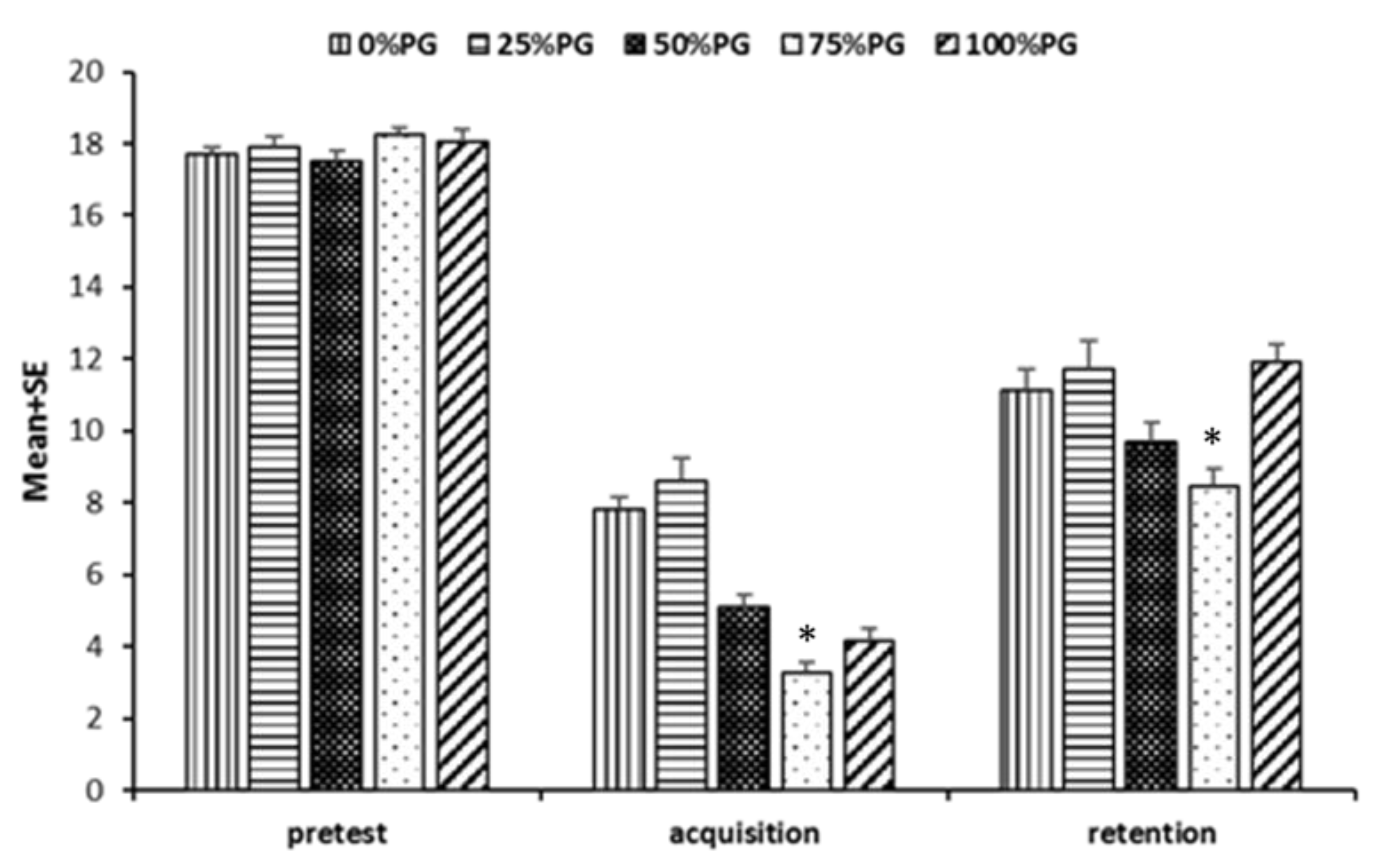
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lamb, D.R. Basic principles for improving sport performance. GSSI Sports Sci. Exch. 1995, 8, 1. [Google Scholar]
- Hemayattalab, R.; Rostami, L.R. Effects of frequency of feedback on the learning of motor skill in individuals with cerebral palsy. Res. Dev. Disabil. 2010, 31, 212–217. [Google Scholar] [CrossRef]
- Toovey, R.; Harvey, A.R.; McGinley, J.L.; Lee, K.J.; Shih, S.T.; Spittle, A.J. Bike skills training for children with cerebral palsy: Protocol for a randomised controlled trial. BMJ Open 2018, 8, e019898. [Google Scholar] [CrossRef]
- Schmidt, R.A.; Lee, T.D. Motor Learning and Control: A Behavioral Emphasis; Human Kinetics: Champaign, IL, USA, 2005. [Google Scholar]
- Carneiro, M.I.; Russo, C.; Masson, R.; Sebastiano, D.R.; Baranello, G.; Turati, C.; Bolognini, N. Motor learning in unilateral cerebral palsy and the influence of corticospinal tract reorganization. Eur. J. Paediatr. Neurol. 2020, 27, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Robert, M.T.; Sambasivan, K.; Levin, M.F. Extrinsic feedback and upper limb motor skill learning in typically-developing children and children with cerebral palsy. Restor. Neurol. Neurosci. 2017, 35, 171–184. [Google Scholar] [CrossRef]
- Sharif, M.R.; Hemayattalab, R.; Sayyah, M.; Hemayattalab, A.; Bazazan, S. Effects of physical and mental practice on motor learning in individuals with cerebral palsy. J. Dev. Phys. Disabil. 2015, 27, 479–487. [Google Scholar] [CrossRef]
- Burtner, P.A.; Leinwand, R.; Sullivan, K.J.; Goh, H.T.; Kantak, S.S. Motor learning in children with hemiplegic cerebral palsy: Feedback effects on skill acquisition. Dev. Med. Child Neurol. 2014, 56, 259–266. [Google Scholar] [CrossRef]
- Fathirezaie, Z.; Abbaspour, K.; Badicu, G.; Zamani Sani, S.H.; Nobari, H. The Effect of Environmental Contexts on Motor Proficiency and Social Maturity of Children: An Ecological Perspective. Children 2021, 8, 157. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, K.J.; Kantak, S.S.; Burtner, P.A. Motor learning in children: Feedback effects on skill acquisition. Phys. Ther. 2008, 88, 720–732. [Google Scholar] [CrossRef] [PubMed]
- van der Kamp, J.; Steenbergen, B.; Masters, R.S. Explicit and implicit motor learning in children with unilateral cerebral palsy. Disabil. Rehabil. 2018, 40, 2790–2797. [Google Scholar] [CrossRef] [PubMed]
- Wulf, G.; Shea, C.H.; Whitacre, C.A. Physical-guidance benefits in learning a complex motor skill. J. Mot. Behavior. 1998, 30, 367–380. [Google Scholar] [CrossRef] [PubMed]
- Bania, T.; Dodd, K.J.; Taylor, N. Habitual physical activity can be increased in people with cerebral palsy: A systematic review. Clin. Rehabil. 2011, 25, 303–315. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, R.A.; Wrisberg, C.A. Motor Learning and Performance: A Situation-Based Learning Approach; Human Kinetics: Champaign, IL, USA, 2008. [Google Scholar]
- Larson, C.A.; Surber-Berro, M.R. The effects of observational feedback and verbal cues on the motor learning of an aimed reach-and-point task. Pediatric Phys. Ther. 2006, 18, 214–225. [Google Scholar] [CrossRef] [PubMed]
- Gillespie, M. Summary versus every-trial knowledge of results for individuals with intellectual disabilities. Adapt. Phys. Act. Q. 2003, 20, 46–56. [Google Scholar] [CrossRef]
- Marschall, F.; Bund, A.; Wiemeyer, J. Does frequent augmented feedback really degrade learning? A meta-analysis. Beweg. Train. 2007, 1, 75–86. [Google Scholar]
- Schmidt, R.A. Motor Learning and Performance: From Principles to Practice; Human Kinetics: Champaign, IL, USA, 1991. [Google Scholar]
- Winstein, C.J.; Pohl, P.S.; Lewthwaite, R. Effects of physical guidance and knowledge of results on motor learning: Support for the guidance hypothesis. Res. Q. Exerc. Sport 1994, 65, 316–323. [Google Scholar] [CrossRef]
- Morgan, C.; Darrah, J.; Gordon, A.M.; Harbourne, R.; Spittle, A.; Johnson, R.; Fetters, L. Effectiveness of motor interventions in infants with cerebral palsy: A systematic review. Dev. Med. Child Neurol. 2016, 58, 900–909. [Google Scholar] [CrossRef] [Green Version]
- Robert, M.T.; Guberek, R.; Sveistrup, H.; Levin, M.F. Motor learning in children with hemiplegic cerebral palsy and the role of sensation in short-term motor training of goal-directed reaching. Dev. Med. Child Neurol. 2013, 55, 1121–1128. [Google Scholar] [CrossRef] [Green Version]
- Franz, F.; Edgar, E.; Albert-Georg, L.; Axel, B. G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar]
- Chen, D.D.; Kaufman, D.; Chung, M.-W. Emergent patterns of feedback strategies in performing a closed motor skill. Percept. Mot. Ski. 2001, 93, 197–204. [Google Scholar] [CrossRef]
- Sabari, J.S.; Kane, L.; Flanagan, S.R.; Steinberg, A. Constraint-induced motor relearning after stroke: A naturalistic case report. Arch. Phys. Med. Rehabil. 2001, 82, 524–528. [Google Scholar] [CrossRef] [PubMed]
- Onla-or, S.; Winstein, C.J. Determining the optimal challenge point for motor skill learning in adults with moderately severe Parkinson’s disease. Neurorehabilit. Neural Repair 2008, 22, 385–395. [Google Scholar] [CrossRef] [PubMed]
- Garvey, M.A.; Giannetti, M.L.; Alter, K.E.; Lum, P.S. Cerebral palsy: New approaches to therapy. Curr. Neurol. Neurosci. Rep. 2007, 7, 147–155. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Groups of PG | Totally (n = 5) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0% (n = 5) | 25% (n = 5) | 50% (n = 5) | 75% (n = 5) | 100% (n = 5) | ||||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| Age (years) | 11.00 | 1.581 | 11.00 | 2.55 | 11.20 | 2.95 | 11.20 | 2.95 | 11.00 | 2.236 | 11.08 | 2.29 |
| Height (cm) | 133.2 | 8.468 | 133.80 | 13.9 | 133.8 | 15.9 | 133.0 | 14.5 | 132.6 | 11.69 | 133.2 | 12.04 |
| Body mass (kg) | 32.00 | 5.24 | 32.40 | 8.64 | 33.00 | 9.82 | 33.60 | 9.91 | 32.60 | 6.65 | 32.72 | 7.564 |
| BMI (kg/m2) | 17.91 | 0.7313 | 17.75 | 1.10 | 18.01 | 1.21 | 18.61 | 2.08 | 18.34 | 0.6198 | 18.13 | 1.197 |
| Tests | Groups of PG | Totally (n = 5) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0% (n = 5) | 25% (n = 5) | 50% (n = 5) | 75% (n = 5) | 100% (n = 5) | ||||||||
| Mean | SD | Mean | SD | Mean | Sd | Mean | SD | Mean | SD | Mean | SD | |
| Pre-test | 17.68 | 0.54 | 17.88 | 0.71 | 17.51 | 0.65 | 18.26 | 0.45 | 18.03 | 0.85 | 17.87 | 0.65 |
| Acquisition | 7.80 | 0.76 | 8.61 | 1.38 | 5.10 | 0.71 | 3.27 | -0.73 | 4.18 | 0.76 | 5.79 | 2.27 |
| Retention | 11.11 | 1.38 | 11.71 | 1.79 | 9.71 | 1.16 | 8.45 | 1.12 | 11.93 | 1.05 | 10.58 | 1.81 |
| Group (I) | Comparative Group (J) | Pre-Test | Acquisition | Retention | |||
|---|---|---|---|---|---|---|---|
| MD (I–J) | p | MD (I–J) | p | MD (I–J) | p | ||
| 0% | 25% | −0.20 | 0.99 | −0.82 | 0.57 | −0.60 | 0.95 |
| 50% | 0.17 | 0.99 | 2.70 | ≤0.001 * | 1.40 | 0.48 | |
| 75% | −0.58 | 0.63 | 4.55 | ≤0.001 * | 2.67 | 0.03 * | |
| 100% | −0.35 | 0.91 | 3.62 | ≤0.001 * | −0.83 | 0.86 | |
| 25% | 50% | 0.37 | 0.90 | 3.52 | ≤0.001 * | 2.00 | 0.16 |
| 75% | −0.38 | 0.88 | 5.37 | ≤0.001 * | 3.27 | 0.007 * | |
| 100% | −0.15 | 0.99 | 4.34 | ≤0.001 * | −0.22 | <0.999 | |
| 50% | 75% | −0.75 | 0.39 | 1.85 | 0.03 * | 1.27 | 0.57 |
| 100% | −0.52 | 0.72 | 0.92 | 0.51 | −2.22 | <0.999 | |
| 75% | 100% | 0.23 | 0.98 | −0.93 | 0.50 | −3.48 | 0.004 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nobari, H.; Azimzadeh, E.; Hassanlouei, H.; Badicu, G.; Pérez-Gómez, J.; Ardigò, L.P. Effect of Physical Guidance on Learning a Tracking Task in Children with Cerebral Palsy. Int. J. Environ. Res. Public Health 2021, 18, 7136. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137136
Nobari H, Azimzadeh E, Hassanlouei H, Badicu G, Pérez-Gómez J, Ardigò LP. Effect of Physical Guidance on Learning a Tracking Task in Children with Cerebral Palsy. International Journal of Environmental Research and Public Health. 2021; 18(13):7136. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137136
Chicago/Turabian StyleNobari, Hadi, Elham Azimzadeh, Hamidollah Hassanlouei, Georgian Badicu, Jorge Pérez-Gómez, and Luca Paolo Ardigò. 2021. "Effect of Physical Guidance on Learning a Tracking Task in Children with Cerebral Palsy" International Journal of Environmental Research and Public Health 18, no. 13: 7136. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137136