
Assessment of Referrals and Hospitalizations in the Hospital Transformed into COVID-19 Facility in Poland during the “Spring Wave” of the Epidemic in 2020—A Cross-Sectional Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. The Cross-Sectional Study
2.1.1. Patient and Setting Characteristics
2.1.2. Measurements
2.2. Hospitalisation Rates Analysis
2.3. Statistical Analysis
2.4. Ethics Approval
3. Results
3.1. COVID-Hospital Functioning Analysis—A Cross-Sectional Study
3.1.1. Study Cohort Characteristics
3.1.2. Main Symptoms That Could Suggest COVID-19
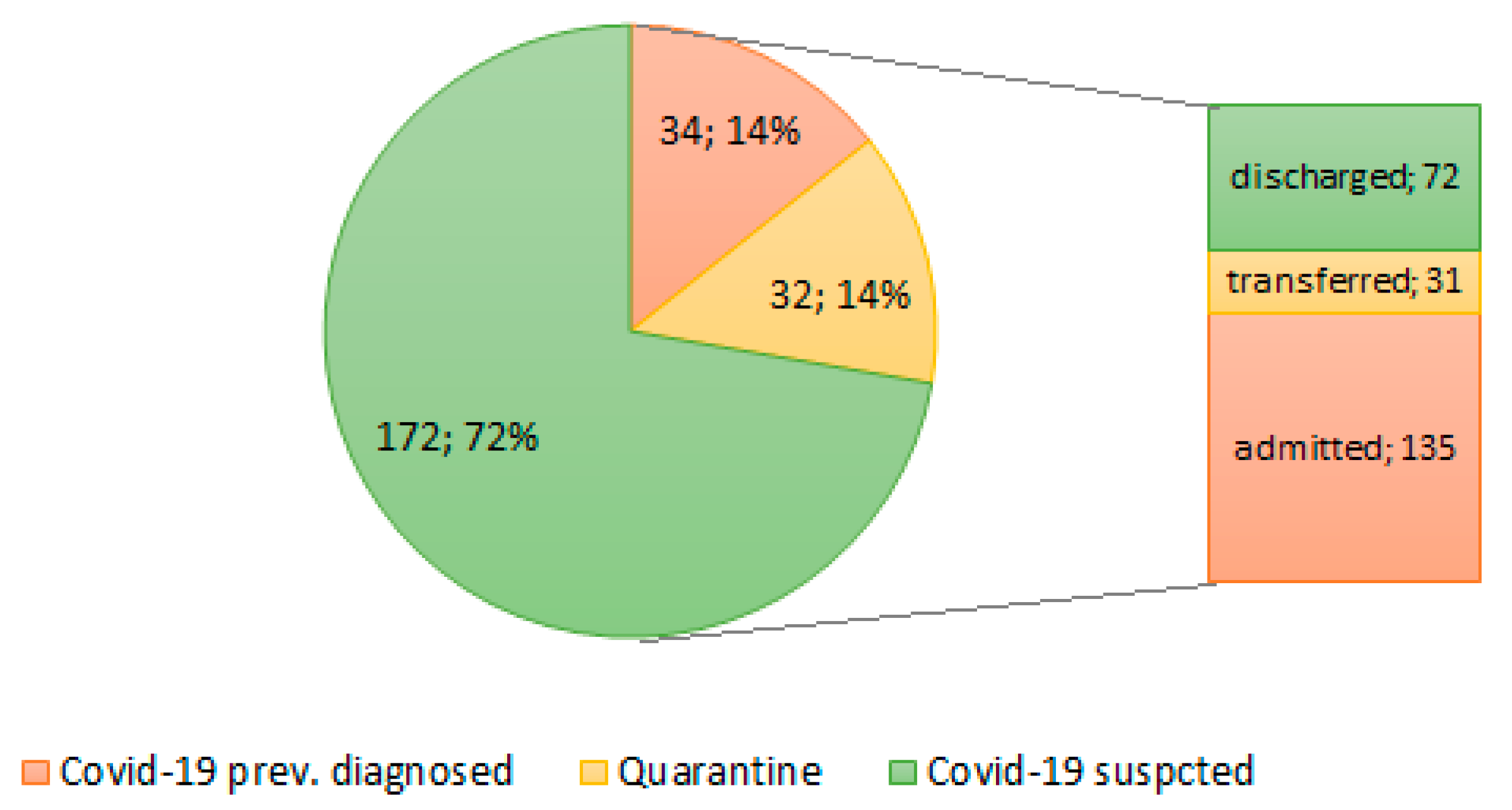
3.1.3. Patient Transfer from the ER
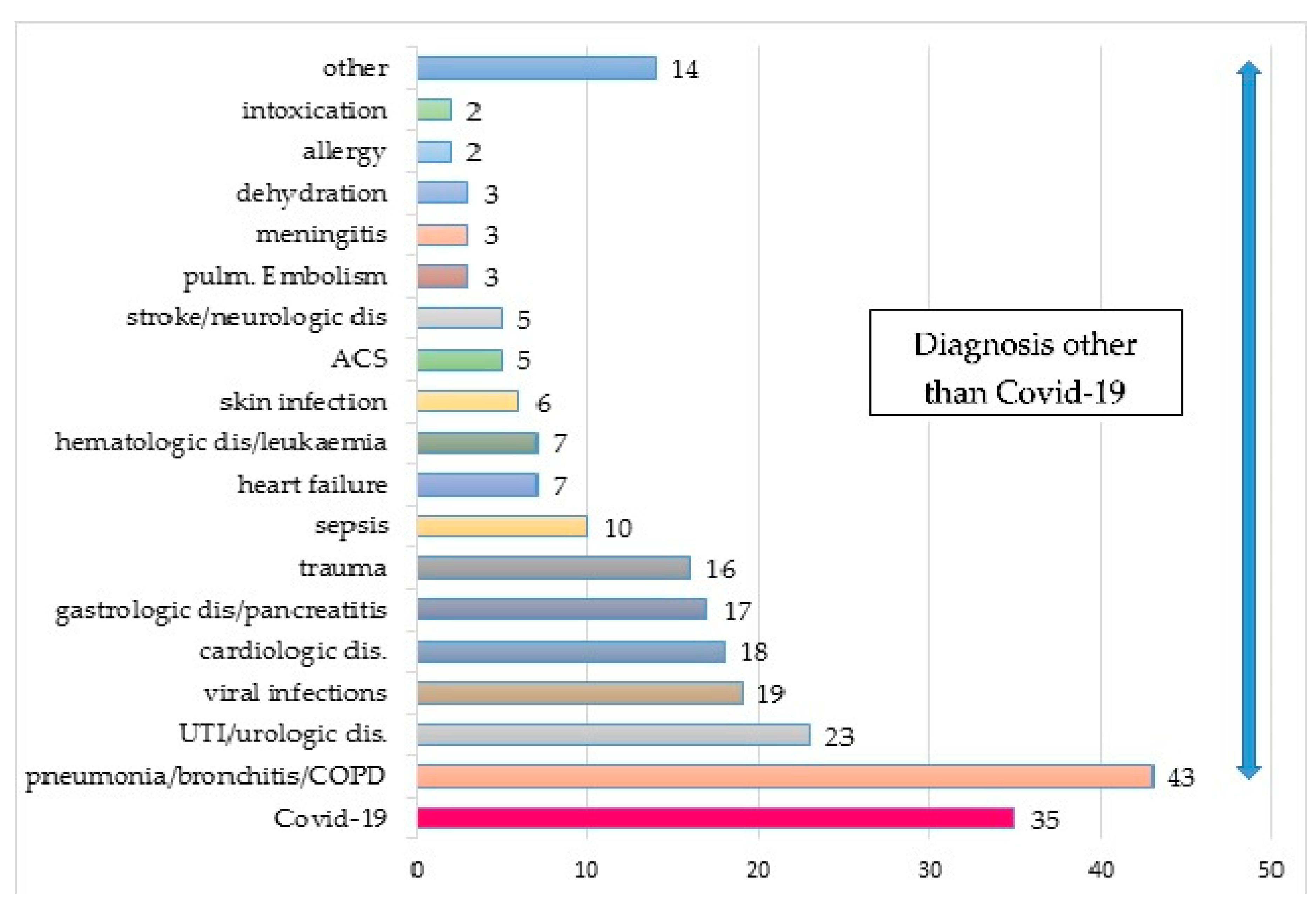
3.1.4. Characteristics of Hospitalized Patients
3.2. Changes in the Number of Hospitalizations in Poland and in Selected COVID- and Non-COVID Hospitals between 2019 and 2020—NHF Data Analysis
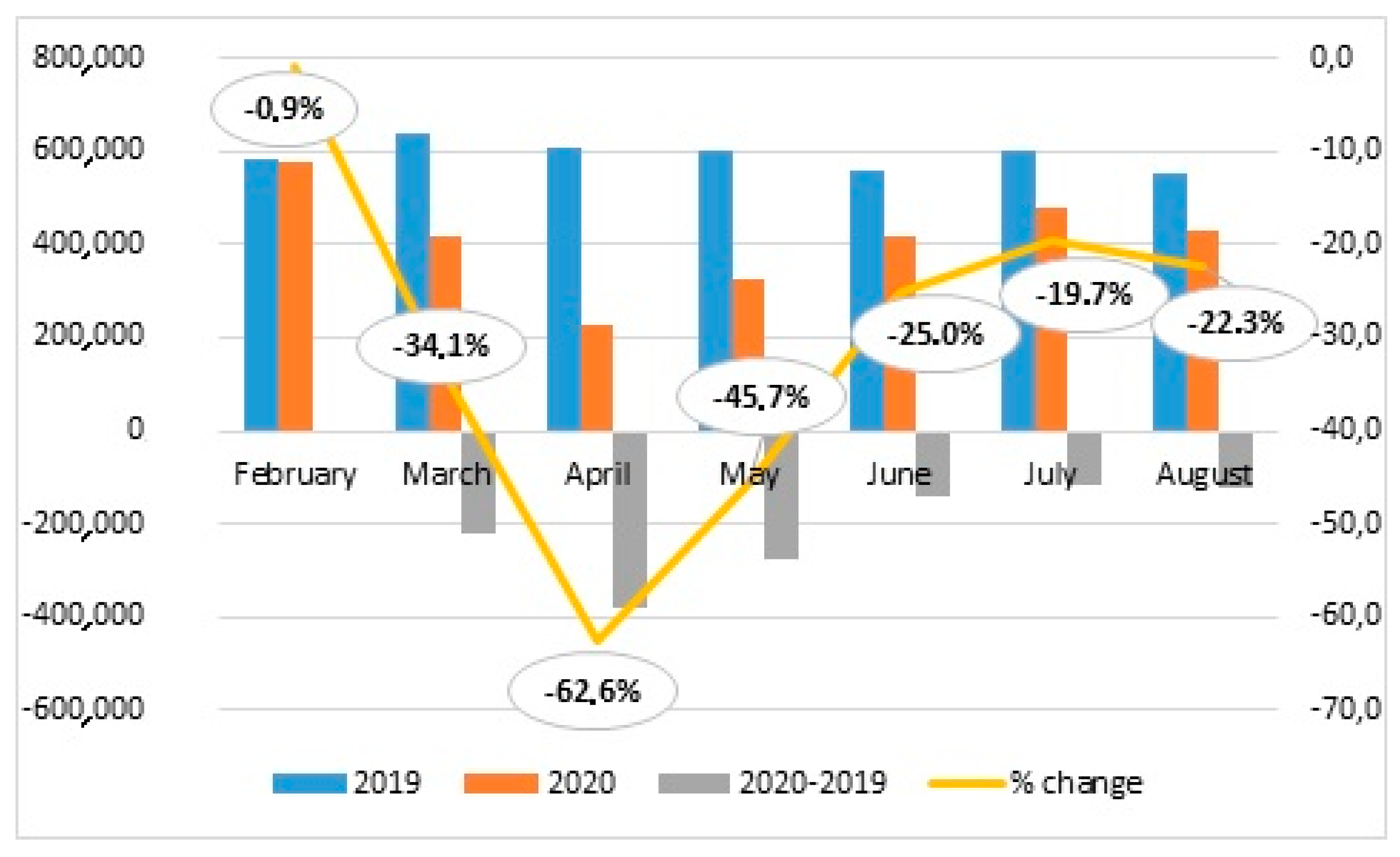
3.2.1. Comparison of Hospitalization Numbers in Poland in 2019 and 2020
3.2.2. Hospitalization Rates in COVID- and Non-COVID Hospitals
4. Discussion
5. Conclusions
Abbreviation
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization Regional Office for Europe: WHO Announces COVID-19 Outbreak a Pandemic. 2019. Available online: http://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-COVID19/news/news/2020/3/who-announces-COVID-19-outbreak-a-pandemic (accessed on 4 May 2021).
- Pinkas, J.; Jankowski, M.; Szumowski, Ł.; Lusawa, A.; Zgliczyński, W.S.; Raciborski, F.; Wierzba, W.; Gujski, M. Public health interventions to mitigate early spread of SARS-CoV-2 in Poland. Med. Sci. Monit. 2020, 26, e924730. [Google Scholar] [CrossRef] [PubMed]
- Ordinance of the Minister of Health of March 20, 2020 Regarding the Announcement of the State of the Epidemic in the Territory of the Republic of Poland. Available online: http://prawo.sejm.gov.pl/isap.nsf/DocDetails.xsp?id=WDU20200000491 (accessed on 4 May 2021). (In Polish)
- Act of March 2, 2020, on Special Arrangements for the Prevention and Combating of COVID-19, Other Infectious Diseases, and Crises Caused by Them. Available online: http://prawo.sejm.gov.pl/isap.nsf/download.xsp/WDU20200000374/T/D20200374L.pdf (accessed on 4 May 2021). (In Polish)
- Flisiak, R.; Horban, A.; Jaroszewicz, J.; Kozielewicz, D.; Pawłowska, M.; Parczewski, M.; Piekarska, A.; Tomasiewicz, K.; Zarębska-Michaluk, D. Recommendations of management in SARS-CoV-2 infection of the Polish Association of Epidemiologists and Infectiologists. Pol. Arch. Intern. Med. 2020, 130, 352–357. [Google Scholar] [CrossRef] [Green Version]
- Available online: https://www.rp.pl/COVID-19/305319943-W-Polsce-rusza-likwidacja-szpitali-dla-chorych-na-COVID-19.html (accessed on 4 May 2021).
- Stefura, T.; Rymarowicz, J.; Wysocki, M.; Szeliga, J.; Wallner, G.; Pędziwiatr, M.; Nowakowski, M.; Major, P. Surgical Care in Poland after COVID19 Outbreak: A National Survey. Available online: https://assets.researchsquare.com/files/rs-41119/v1/9d6e4d0e-c8cb-4563-8a7d-70eb03d18ba5.pdf (accessed on 4 May 2021).
- Maluchnik, M.; Podwójcic, K.; Więckowska, B. Decreasing access to cancer diagnosis and treatment during the COVID-19 pandemic in Poland. Acta Oncol. 2020, 60, 28–31. [Google Scholar] [CrossRef]
- Experts on One-Named Hospitals: This Solution Has no Future. Available online: https://www.rynekzdrowia.pl/Polityka-zdrowotna/Eksperci-o-szpitalach-jednoimiennych-takie-rozwiazanie-nie-ma-przyszlosci,209570,14,3.html (accessed on 4 May 2021). (In Polish).
- World Health Organization. Public Health Surveillance for COVID-19: Interim Guidance. Available online: https://www.who.int/publications/i/item/who-2019-nCoV-surveillanceguidance-2020.7 (accessed on 4 May 2021).
- World Health Organization. Laboratory Testing for 2019 Novel Coronavirus (2019-nCoV) in Suspected Human Cases. Available online: https://www.who.int/publications/i/item/10665-331501 (accessed on 4 May 2021).
- Available online: https://zdrowedane.nfz.gov.pl/local/nfz/reports.php (accessed on 4 May 2021).
- Available online: https://www.medonet.pl/koronawirus/koronawirus-w-polsce,prof--grodzicki--pacjenci-w-stanie-bezposredniego-zagrozenia-zycia-nie-odbija-sie-od-naszych-drzwi--szpital-uniwersytecki-nie-tylko-dla-pacjentow-z-COVID-19,artykul,66987717.html (accessed on 4 May 2021).
- Nowak, B.; Szymański, P.; Pańkowski, I.; Szarowska, A.; Życińska, K.; Rogowski, W.; Gil, R.; Furmanek, M.; Tatur, J.; Zaczyński, A.; et al. Clinical characteristics and short-term outcomes of patients with coronavirus disease 2019: A retrospective single-center experience of a designated hospital in Poland. Pol. Arch. Intern. Med. 2020, 130, 407–411. [Google Scholar]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Liu, J.; Ren, N.; He, R.; Li, M.; Dong, Q. Emergency management in fever clinic during the outbreak of COVID-19: An experience from Zhuhai. Epidemiol. Infect. 2020, 148, e174. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zong, L.; Zhang, J.; Sun, H.; Walline, J.H.; Sun, P.; Xu, S.; Li, Y.; Wang, C.; Liu, J.; et al. Identifying the effects of an upgraded ‘fever clinic’ on COVID-19 control and the workload of the emergency department: A retrospective study in a tertiary hospital in China. BMJ Open 2020, 10, e039177. [Google Scholar] [CrossRef] [PubMed]
- Candel, F.J.; Canora, J.; Zapatero, A.; Barba, R.; del Castillo, J.G.; García-Casasola, G.; Gil-Prieto, R.; Barreiro, P.; Fragiel, M.; Prados, F.; et al. Temporary hospitals in times of the COVID pandemic. An example and a practical view. Rev. Esp. Quimioter. 2021. [Google Scholar] [CrossRef] [PubMed]
- Romagnani, P.; Gnone, G.; Guzzi, F.; Negrini, S.; Guastalla, A.; Annunziato, F.; Romagnani, S.; de Palma, R. The COVID-19 infection: Lessons from the Italian experience. J. Public Health Policy 2020, 41, 238–244. [Google Scholar] [CrossRef] [PubMed]
- Legido-Quigley, H.; Mateos, J.T.; Campos, V.R.; Sánchez, M.G.; Muntaner, C.; McKee, M. The resilience of the Spanish health system against the COVID-19 pandemic. Lancet Public Health 2020, 5, e251–e252. [Google Scholar] [CrossRef] [Green Version]
- Gujski, M.; Raciborski, F.; Jankowski, M.; Nowicka, P.M.; Rakocy, K.; Pinkas, J. Epidemiological analysis of the first 1389 cases of COVID-19 in Poland: A preliminary report. Med. Sci. Monit. 2020, 26, e924702. [Google Scholar] [CrossRef] [PubMed]
- Ochal, M.; Romaszko, M.; Glińska-Lewczuk, K.; Gromadziński, L.; Romaszko, J. Assessment of the consultation rate with general practitioners in the initial phase of the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2020, 17, 7710. [Google Scholar] [CrossRef] [PubMed]
- Kokoszka-Bargieł, I.; Cyprys, P.; Rutkowska, K.; Madowicz, J.; Knapik, P. Intensive care unit admissions during the first 3 months of the COVID-19 pandemic in Poland: A single-center, cross-sectional study. Med. Sci. Monit. 2020, 26, e926974. [Google Scholar] [CrossRef] [PubMed]
- Miralles, O.; Sanchez-Rodriguez, D.; Marco, E.; Annweiler, C.; Baztan, A.; Betancor, É.; Cambra, A.; Cesari, M.; Fontecha, B.J.; Gąsowski, J.; et al. Unmet needs, health policies, and actions during the COVID-19 pandemic: A report from six European countries. Eur. Geriatr. Med. 2020, 15, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Polish Government COVID-19 Statistics. Available online: https://www.gov.pl/web/koronawirus/wykaz-zarazen-koronawirusem-sars-cov-2 (accessed on 29 June 2021). (In Polish)
- Feral-Pierssens, A.L.; Claret, P.G.; Chouihed, T. Collateral damage of the COVID-19 outbreak: Expression of concern. Eur. J. Emerg. Med. 2020, 27, 233–234. [Google Scholar] [CrossRef] [PubMed]
- Casalino, E.; Choquet, C.; Bouzid, D.; Peyrony, O.; Curac, S.; Fontaine, J.P.; Plaisance, P.; Chauvin, A.; Ghazali, D.A. Analysis of emergency department visits and hospital activity during influenza season, COVID-19 epidemic, and lockdown periods in view of managing a future disaster risk: A multicenter observational study. Int. J. Environ. Res. Public Health 2020, 17, 8302. [Google Scholar] [CrossRef] [PubMed]
- Bodilsen, J.; Nielsen, P.B.; Søgaard, M.; Dalager-Pedersen, M.; Speiser, L.O.Z.; Yndigegn, T.; Nielsen, H.; Larsen, T.B.; Skjøth, F. Hospital admission and mortality rates for non-COVID diseases in Denmark during COVID-19 pandemic: Nationwide population based cohort study. BMJ 2021, 373, n1135. [Google Scholar] [CrossRef] [PubMed]
- Minister of Health. Strategy 3.0. Available online: https://www.gov.pl/web/zdrowie/strategia-walki-z-pandemia-COVID19 (accessed on 4 May 2021). (In Polish)
- Raciborski, F.; Pinkas, J.; Jankowski, M.; Sierpiński, R.; Zgliczyński, W.S.; Szumowski, Ł.; Rakocy, K.; Wierzba, W.; Gujski, M. Dynamics of the coronavirus disease 2019 outbreak in Poland: An epidemiological analysis of the first 2 months of the epidemic. Pol. Arch. Intern. Med. 2020, 130, 615–621. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Total | <60 Years | ≥60 Years | P a | |
|---|---|---|---|---|
| Number of referrals | 238 (100.0) | 99 (41.6) | 139 (58.4) | |
| Age, years, Me (IQR) | 64.5 (44–78) | 41 (33;50) | 76 (67;84) | 0.001 b |
| Sex, men | 144 (60.5) | 67 (67.7) | 77 (55.4) | 0.06 |
| Cause of the referral | ||||
| Fever | 91 (38.2) | 31 (31.3) | 60 (43.2) | 0.06 |
| Dyspnoea | 21 (8.8) | 8 (8.1) | 13 (9.4) | 0.72 |
| Respiratory Insufficiency | 2 (0.8) | - | 2 (1.4) | 0.23 |
| COVID-19 | 32 (13.5) | 11 (11.1) | 21 (15.1) | 0.37 |
| Pneumonia | 21 (8.8) | 6 (6.1) | 15 (10.8) | 0.21 |
| Pulmonary disorders | 6 (2.5) | 2 (2) | 4 (2.9) | 0.66 |
| Cardiological disorders | 9 (3.8) | 2 (2) | 7 (5) | 0.23 |
| Acute coronary syndrome | 5 (2.1) | 2 (2) | 3 (2.2) | 0.92 |
| Stenocardy | 7 (2.9) | 6 (6.1) | 1 (0.7) | 0.015 |
| Trauma | 14 (5.9) | 12 (12.1) | 2 (1.4) | 0.005 |
| Gastrointestinal disorders | 17 (7.1) | 13 (13.1) | 4 (2.9) | 0.003 |
| Urological disorder | 5 (2.1) | 1 (1) | 4 (2.9) | 0.31 |
| Neurological disorder | 3 (1.3) | 2 (2) | 1 (0.7) | 0.37 |
| Hematological disorder | 1 (0.4) | 1 (1) | - | 0.23 |
| Intoxication | 1 (0.4) | 1 (1) | - | 0.23 |
| Dermatological disorder | 2 (0.2) | - | 2 (1.4) | 0.19 |
| Who referred | ||||
| Emergency medical Services | 95 (39.9) | 34 (34.3) | 61 (43.9) | 0.14 |
| Infectious disease department | 22 (9.2) | 6 (6.1) | 16 (11.5) | 0.16 |
| Hospital emergency ward | 11 (4.6) | 4 (4) | 7 (5) | 0.71 |
| Other hospital | 25 (10.5) | 10 (10.1) | 15 (10.8) | 0.86 |
| GP/ outpatient department | 27 (11.3) | 7 (7.1) | 20 (14.4) | 0.08 |
| Sanitary and epidemiological department | 13 (5.5) | 8 (8.1) | 5 (3.6) | 0.13 |
| Patients presented themselves | 45 (18.9) | 30 (30.3) | 15 (10.8) | 0.002 |
| Symptoms indicative of COVID-19 | ||||
| Fever | 151 (63.5) | 56 (56.6) | 95 (68.4) | 0.06 |
| Cough | 53 (22.3) | 18 (18.2) | 35 (25.2) | 0.2 |
| Dyspnoea | 75 (31.5) | 18 (18.2) | 57 (41) | <0.001 |
| Severe general health status | 26 (10.9) | 6 (6.1) | 20 (14.4) | 0.04 |
| Total | Total | <60 Years | ≥60 Years | P a |
|---|---|---|---|---|
| Admitted to the hospital | 135 (59.3) | 32 (32.3) | 103 (74.1) | <0.001 |
| Comorbidity: | ||||
| Hypertension | 95 (70) | 9 (28) | 86 (83) | <0.001 |
| CAD | 33 (24) | - | 33 (32) | <0.001 |
| Atrial fibrillation | 35 (26) | 2 (6) | 33 (32) | 0.003 |
| Heart failure | 67 (50) | 2 (6) | 65 (63) | <0.001 |
| Diabetes | 46 (34) | 5 (16) | 41 (40) | 0.01 |
| COPD | 20 (15) | 2 (6) | 18 (17) | 0.12 |
| Immunosuppressive therapy | 14 (10) | 2 (6) | 12 (12) | 0.38 |
| Neoplasm | 18 (13) | 2 (6) | 16 (16) | 0.36 |
| Dementia | 15 (11) | - | 15 (15) | 0.02 |
| IADL disability | 43 (33) | 4 (13) | 39 (39) | 0.01 |
| Delirium during hospitalization | 31 (23) | 7 (22) | 24 (23) | 0.87 |
| Transfer to Intensive care unit | 17 (13) | 3 (10) | 14 (14) | 0.55 |
| Death | 19 (14) | 4 (13) | 15 (15) | 0.86 |
| Final Diagnoses | Coexisting Symptom by Admission | |||
|---|---|---|---|---|
| Fever (n = 151) | Cough (n = 53) | Dyspnoe (n = 75) | Severe Health Status (n = 26) | |
| COVID-19 pneumonia | 18 (11.9) | 14 (26.4) | 19 (25.3) | 8 (30.8) |
| COVID-19 negative | ||||
| Pneumonia/bronchitis/COPD | 33 (21.6) | 27 (50.9) | 23 (30.7) | 3 (11.5) |
| Viral infections | 19 (12.6) | - | 1 (1.3) | - |
| Sepsis | 10 (6.6) | 1 (1.9) | 4 (5.3) | 4 (15.4) |
| UTI/urologic dis | 19 (12.6) | - | 2 (2.7) | - |
| Heart failure | 2 (1.3) | 1 (1.9) | 5 (6.7) | - |
| ACS | 1 (0.7) | - | 5 (6.7) | 2 (7.7) |
| Pulmonary embolism | 3 (2) | 2 (3.8) | 1 (1.3) | 1 (3.9) |
| Cardiologic dis | 5 (3.3) | 1 (1.9) | 2 (2.7) | 1 (3.9) |
| Trauma | 3 (2) | - | - | - |
| Gastrologic dis | 8 (5.3) | 1 (1.9) | 1 (1.3) | - |
| Hematologic dis/leukaemia | 4 (2.7) | 2 (3.8) | 2 (2.7) | - |
| Dehydration | 2 (1.3) | - | 2 (2.7) | 1 (3.9) |
| Skin infections | 5 (3.3) | 1 (1.9) | 1 (1.3) | - |
| Meningitis | 3 (2) | - | 1 (1.3) | 1 (3.9) |
| Neurologic dis/stroke | 4 (2.7) | 1 (1.9) | - | 1 (3.9) |
| Intoxication | 2 (1.3) | - | - | - |
| Allergy | 1 (0.7) | - | 1 (1.3) | - |
| other | 9 (5.9) | 2 (3.8) | 5 (6.7) | 4 (15.4) |
| Hospitalizations | Months | ||||||
|---|---|---|---|---|---|---|---|
| February | March | April | May | June | July | August | |
| COUNTY HOSPITALS | |||||||
| COVID: Hospital in Lomza | |||||||
| Number in 2019 | 1488 | 1537 | 1488 | 1512 | 1365 | 1474 | 1379 |
| Number in 2020 | 1494 | 689 | 69 | 38 | 247 | 601 | 580 |
| Change in number (2019–2020) | 6 | −848 | −584 | −1474 | −1118 | −873 | −799 |
| % change (2019–2020) | 0.4 | −55.2 | −94.8 | −97.5 | −81.9 | −59.2 | −57.9 |
| NON-COVID: Sniadecja Hospital in Bialystok | |||||||
| Number in 2019 | 1933 | 1922 | 1890 | 1959 | 1776 | 2001 | 1601 |
| Number in 2020 | 1810 | 1402 | 875 | 1395 | 1592 | 1747 | 1446 |
| Change in number (2019–2020) | −123 | −520 | −1015 | −564 | −184 | −254 | −155 |
| % change (2019–2020) | −6.4 | −27.1 | −53.7 | −28.8 | −10.4 | −12.7 | −9.7 |
| Pa | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| UNIVERSITY HOSPITALS | |||||||
| COVID: University Hospital in Cracow | |||||||
| Number in 2019 | 4998 | 5168 | 4828 | 5189 | 4541 | 5449 | 4340 |
| Number in 2020 | 4462 | 2982 | 1226 | 1887 | 2766 | 3636 | 1258 |
| Change in number (2019–2020) | −536 | −2186 | −3602 | −3302 | −1775 | −1813 | −3082 |
| % change (2019–2020) | −10.7 | −42.3 | −74.6 | −63.6 | −39.1 | −33.3 | −71.0 |
| NON-COVID: University Hospital in Bialystok | |||||||
| Number in 2019 | 3288 | 3713 | 3622 | 3468 | 3315 | 3520 | 2907 |
| Number in 2020 | 3399 | 2226 | 961 | 1572 | 2150 | 2537 | 1990 |
| Change in number (2019–2020) | 111 | −1487 | −2661 | −1896 | −1165 | −983 | −917 |
| % change (2019–2020) | 3.4 | −40.0 | −73.5 | −54.7 | −35.1 | −27.9 | −31.5 |
| Pb | <0.001 | 0.03 | 0.25 | <0.001 | <0.001 | <0.001 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kasiukiewicz, A.; Wojszel, Z.B. Assessment of Referrals and Hospitalizations in the Hospital Transformed into COVID-19 Facility in Poland during the “Spring Wave” of the Epidemic in 2020—A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 7143. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137143
Kasiukiewicz A, Wojszel ZB. Assessment of Referrals and Hospitalizations in the Hospital Transformed into COVID-19 Facility in Poland during the “Spring Wave” of the Epidemic in 2020—A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2021; 18(13):7143. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137143
Chicago/Turabian StyleKasiukiewicz, Agnieszka, and Zyta Beata Wojszel. 2021. "Assessment of Referrals and Hospitalizations in the Hospital Transformed into COVID-19 Facility in Poland during the “Spring Wave” of the Epidemic in 2020—A Cross-Sectional Study" International Journal of Environmental Research and Public Health 18, no. 13: 7143. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137143