
Monitoring Patients Reported Outcomes after Valve Replacement Using Wearable Devices: Insights on Feasibility and Capability Study: Feasibility Results

 , ,
, ,  , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
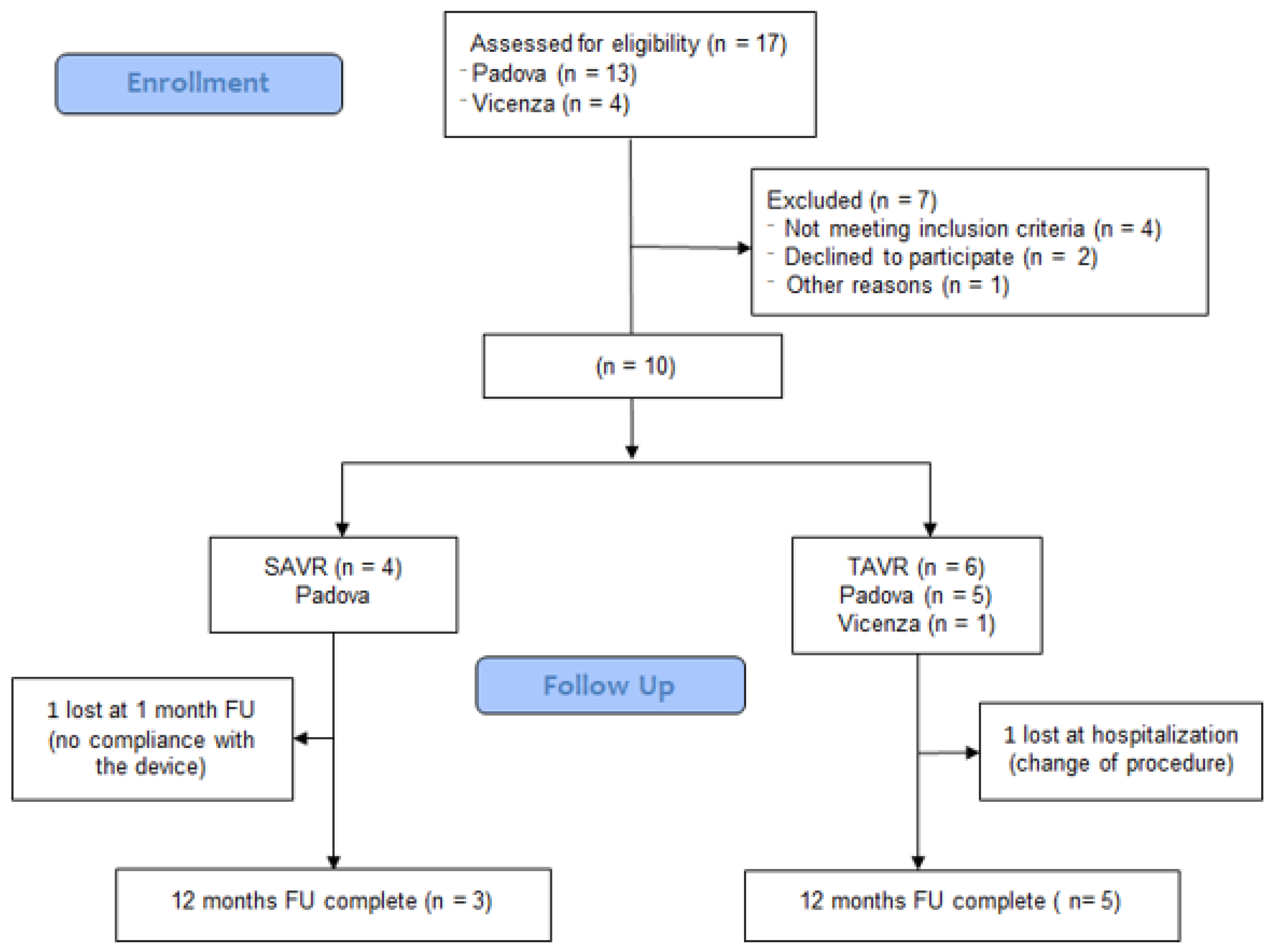
2.1. Study Design and Inclusion Criteria
2.2. Data Collection and Procedures
2.3. Ethical Considerations
2.4. Device
2.5. Device Setup and Usage
2.6. Measurements
2.7. Acceptance of the Technology
2.8. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Score Trend
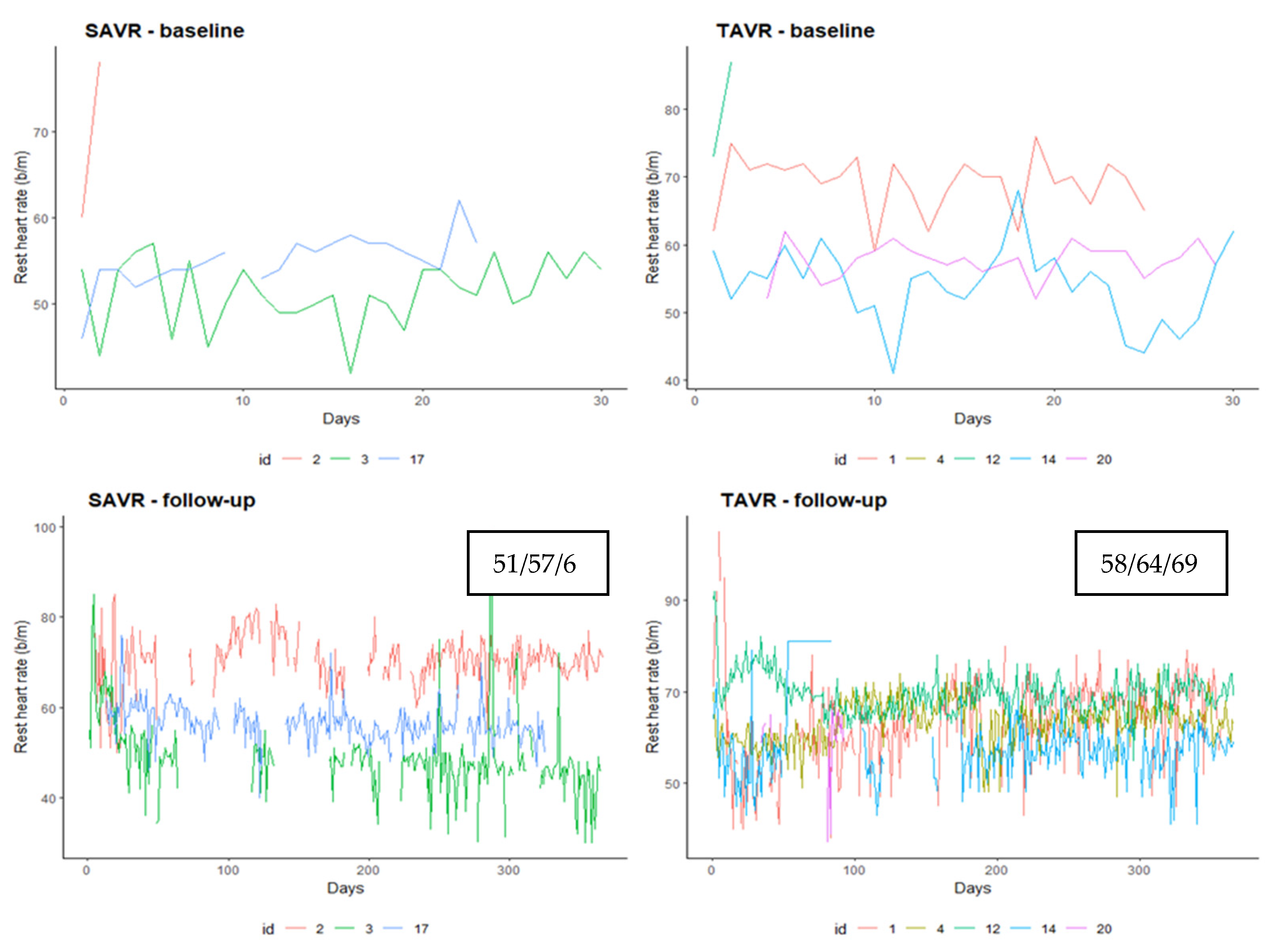
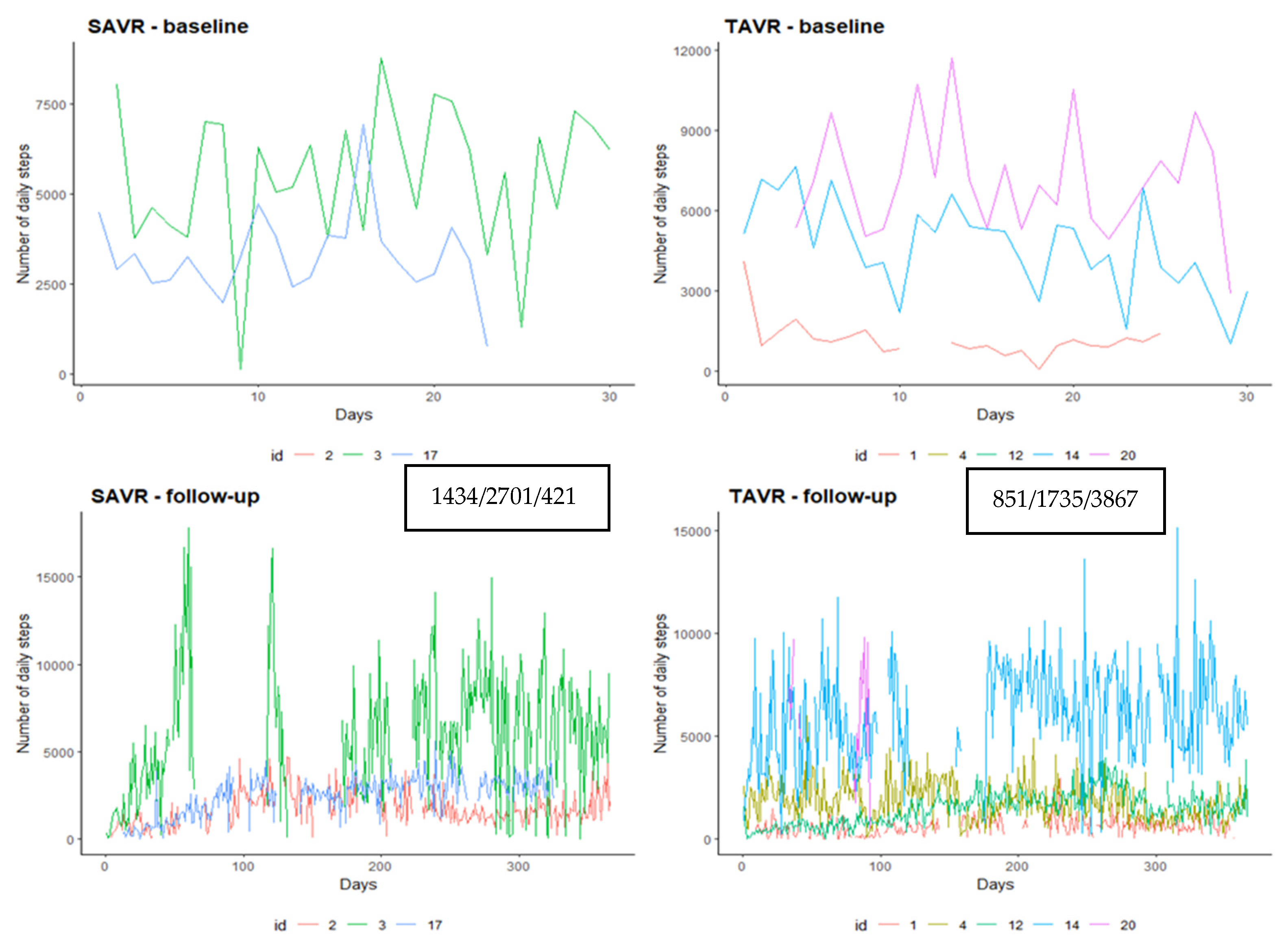
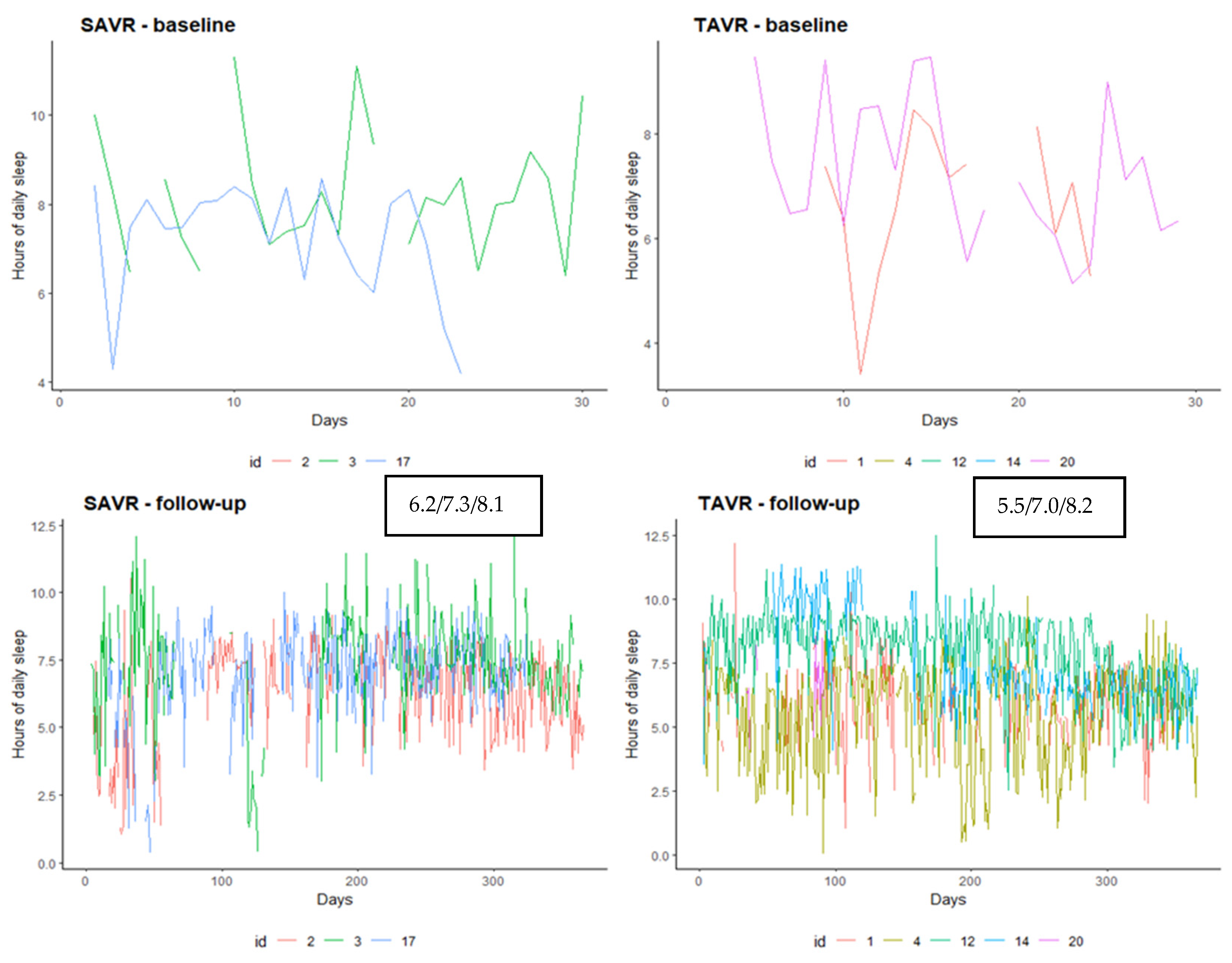
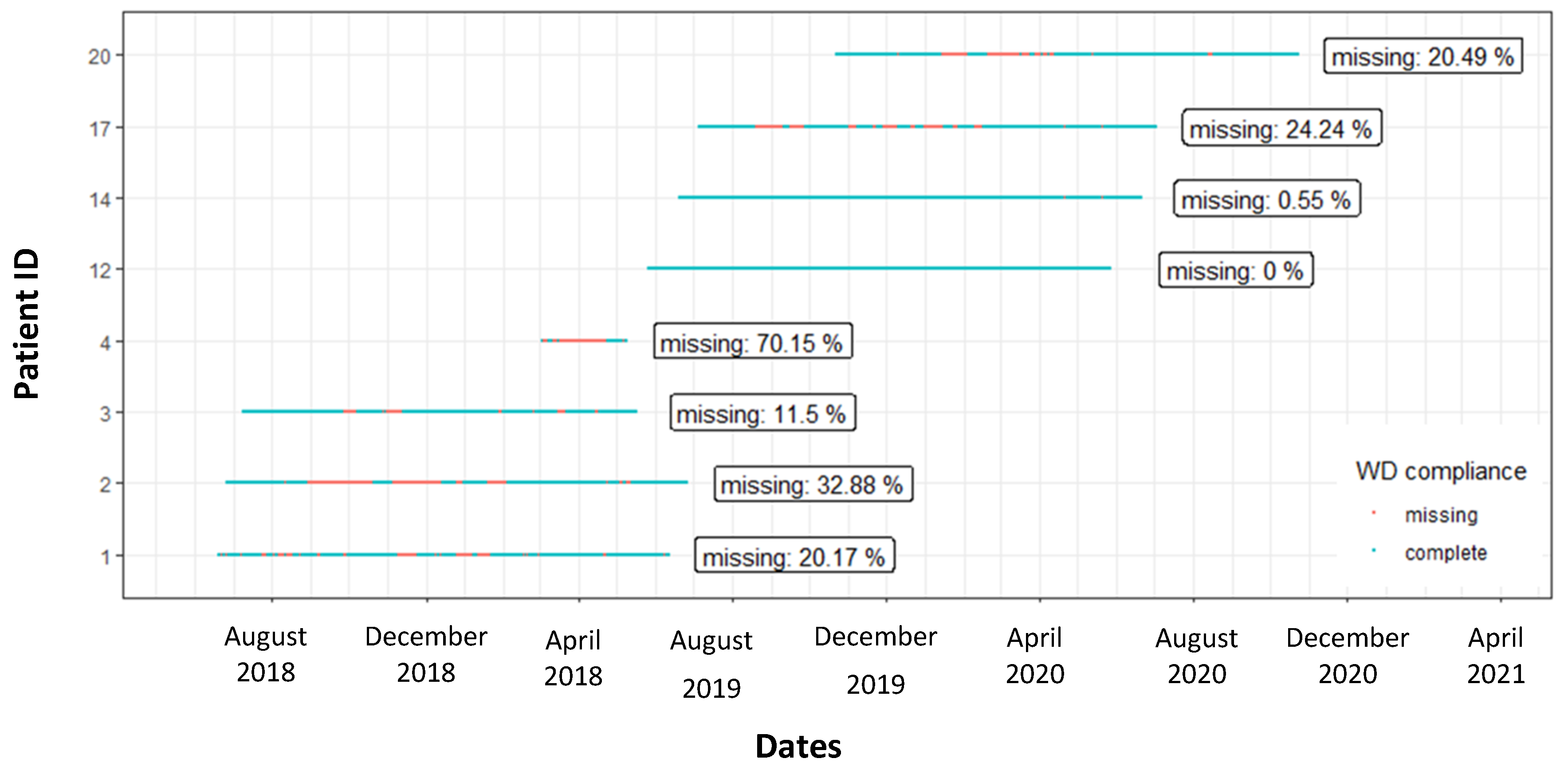
3.3. Device’s Data
3.4. Compliance and Acceptance of the Technology
3.5. Technology Acceptance Questionnaire
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fuller, D.; Colwell, E.; Low, J.; Orychock, K.; Tobin, M.A.; Simango, B.; Buote, R.; Van Heerden, D.; Luan, H.; Cullen, K.; et al. Reliability and Validity of Commercially Available Wearable Devices for Measuring Steps, Energy Expenditure, and Heart Rate: Systematic Review. JMIR mHealth uHealth 2020, 8, e18694. [Google Scholar] [CrossRef] [PubMed]
- Shipments of Wearable Devices Leap to 125 Million Units, Up 35.1% in the Third Quarter, According to IDC [Internet. IDC Prem Glob Mark Intell Co. Available online: https://www.idc.com/getdoc.jsp?containerId=prUS47067820 (accessed on 13 December 2020).
- Byrom, B.; Watson, C.; Doll, H.; Coons, S.J.; Eremenco, S.; Ballinger, R.; Mc Carthy, M.; Crescioni, M.; O’Donohoe, P.; Howry, C. Selection of and Evidentiary Considerations for Wearable Devices and Their Measurements for Use in Regulatory Decision Making: Recommendations from the ePRO Consortium. Value Health 2018, 21, 631–639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chandrasekaran, R.; Katthula, V.; Moustakas, E. Patterns of Use and Key Predictors for the Use of Wearable Health Care Devices by US Adults: Insights from a National Survey. J. Med. Internet Res. 2020, 22, e22443. [Google Scholar] [CrossRef] [PubMed]
- Kekade, S.; Hseieh, C.-H.; Islam, M.d.M.; Atique, S.; Mohammed Khalfan, A.; Li, Y.-C.; Abdul, S.S. The usefulness and actual use of wearable devices among the elderly population. Comput. Methods Programs Biomed. 2018, 153, 137–159. [Google Scholar] [CrossRef] [PubMed]
- Straiton, N.; Alharbi, M.; Bauman, A.; Neubeck, L.; Gullick, J.; Bhindi, R.; Gallagher, R. The validity and reliability of consumer-grade activity trackers in older, community-dwelling adults: A systematic review. Maturitas 2018, 112, 85–93. [Google Scholar] [CrossRef] [Green Version]
- Cadmus-Bertram, L.A.; Marcus, B.H.; Patterson, R.E.; Parker, B.A.; Morey, B.L. Randomized Trial of a Fitbit-Based Physical Activity Intervention for Women. Am. J. Prev. Med. 2015, 49, 414–418. [Google Scholar] [CrossRef] [Green Version]
- Barton, J.; O’Flynn, B.; Tedesco, S. A review of physical activity monitoring and activity trackers for older adults. Stud. Health Technol. Inform. 2017, 242, 748–754. [Google Scholar]
- Puri, A.; Kim, B.; Nguyen, O.; Stolee, P.; Tung, J.; Lee, J. User Acceptance of Wrist-Worn Activity Trackers Among Community-Dwelling Older Adults: Mixed Method Study. JMIR mHealth uHealth 2017, 5, e173. [Google Scholar] [CrossRef] [Green Version]
- Anker, S.D.; Agewall, S.; Borggrefe, M.; Calvert, M.; Jaime Caro, J.; Cowie, M.R.; Ford, I.; Paty, J.A.; Riley, J.P.; Swedberg, K.; et al. The importance of patient-reported outcomes: A call for their comprehensive integration in cardiovascular clinical trials. Eur. Heart J. 2014, 35, 2001–2009. [Google Scholar] [CrossRef] [Green Version]
- Deutsch, M.-A.; Bleiziffer, S.; Elhmidi, Y.; Piazza, N.; Voss, B.; Lange, R.; Krane, M. Beyond adding years to life: Health-related quality-of-life and functional outcomes in patients with severe aortic valve stenosis at high surgical risk undergoing transcatheter aortic valve replacement. Curr. Cardiol. Rev. 2013, 9, 281–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, D.H.; Afilalo, J.; Shi, S.M.; Popma, J.J.; Khabbaz, K.R.; Laham, R.J.; Grodstein, F.; Guibone, K.; Lux, E.; Lipsitz, L.A. Evaluation of Changes in Functional Status in the Year After Aortic Valve Replacement. JAMA Intern. Med. 2019, 179, 383–391. [Google Scholar] [CrossRef]
- Baig, M.M.; GholamHosseini, H.; Moqeem, A.A.; Mirza, F.; Lindén, M. A Systematic Review of Wearable Patient Monitoring Systems—Current Challenges and Opportunities for Clinical Adoption. J. Med. Syst. 2017, 41, 115. [Google Scholar] [CrossRef] [PubMed]
- Izmailova, E.S.; Wagner, J.A.; Perakslis, E.D. Wearable Devices in Clinical Trials: Hype and Hypothesis. Clin. Pharm. 2018, 104, 42–52. [Google Scholar] [CrossRef] [PubMed]
- Russo, N.; Compostella, L.; Tarantini, G.; Setzu, T.; Napodano, M.; Bottio, T.; D’Onofrio, A.; Isabella, G.; Gerosa, G.; Iliceto, S. Cardiac rehabilitation after transcatheter versus surgical prosthetic valve implantation for aortic stenosis in the elderly. Eur. J. Prev. Cardiol. 2014, 21, 1341–1348. [Google Scholar] [CrossRef] [PubMed]
- Lorenzoni, G.; Azzolina, D.; Lanera, C.; Brianti, G.; Gregori, D.; Vanuzzo, D.; Baldi, I. Time trends in first hospitalization for heart failure in a community-based population. Int. J. Cardiol. 2018, 271, 195–199. [Google Scholar] [CrossRef]
- Liu, Z.; Kidney, E.; Bem, D.; Bramley, G.; Bayliss, S.; de Belder, M.A.; Cummins, C.; Duarte, R. Transcatheter aortic valve implantation for aortic stenosis in high surgical risk patients: A systematic review and meta-analysis. PLoS ONE 2018, 13, e0196877. [Google Scholar] [CrossRef]
- Schymik, G.; Heimeshoff, M.; Bramlage, P.; Herbinger, T.; Würth, A.; Pilz, L.; Schymik, J.S.; Wondraschek, R.; Süselbeck, T.; Gerhardus, J.; et al. A comparison of transcatheter aortic valve implantation and surgical aortic valve replacement in 1,141 patients with severe symptomatic aortic stenosis and less than high risk. Catheter. Cardiovasc. Interv. 2015, 86, 738–744. [Google Scholar] [CrossRef] [PubMed]
- Levett, J.Y.; Windle, S.B.; Filion, K.B.; Brunetti, V.C.; Eisenberg, M.J. Meta-Analysis of Transcatheter Versus Surgical Aortic Valve Replacement in Low Surgical Risk Patients. Am. J. Cardiol. 2020, 125, 1230–1238. [Google Scholar] [CrossRef] [PubMed]
- Olsson, K.; Nilsson, J.; Hörnsten, Å.; Näslund, U. Patients’ self-reported function, symptoms and health-related quality of life before and 6 months after transcatheter aortic valve implantation and surgical aortic valve replacement. Eur. J. Cardiovasc. Nurs. 2017, 16, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Straiton, N.; Jin, K.; Bhindi, R.; Gallagher, R. Functional capacity and health-related quality of life outcomes post transcatheter aortic valve replacement: A systematic review and meta-analysis. Age Ageing 2018, 47, 478–482. [Google Scholar] [CrossRef] [Green Version]
- Lorenzoni, G.; Azzolina, D.; Fraccaro, C.; Di Liberti, A.; D’Onofrio, A.; Cavalli, C.; Fabris, T.; D’Amico, G.; Cibin, G.; Nai Fovino, L.; et al. Using Wearable Devices to Monitor Physical Activity in Patients Undergoing Aortic Valve Replacement: Protocol for a Prospective Observational Study. JMIR Res. Protoc. 2020, 9, e20072. [Google Scholar] [CrossRef]
- Tedesco, S.; Sica, M.; Ancillao, A.; Timmons, S.; Barton, J.; O’Flynn, B. Validity Evaluation of the Fitbit Charge2 and the Garmin vivosmart HR+ in Free-Living Environments in an Older Adult Cohort. JMIR mHealth uHealth 2019, 7, e13084. [Google Scholar] [CrossRef]
- Hlatky, M.A.; Boineau, R.E.; Higginbotham, M.B.; Lee, K.L.; Mark, D.B.; Califf, R.M.; Cobb, F.R.; Pryor, D.B. A brief self-administered questionnaire to determine functional capacity (the Duke Activity Status Index). Am. J. Cardiol. 1989, 64, 651–654. [Google Scholar] [CrossRef]
- Mok, M.; Nombela-Franco, L.; Dumont, E.; Urena, M.; DeLarochellière, R.; Doyle, D.; Villeneuve, J.; Côté, M.; Ribeiro, H.B.; Allende, R.; et al. Chronic obstructive pulmonary disease in patients undergoing transcatheter aortic valve implantation: Insights on clinical outcomes, prognostic markers, and functional status changes. JACC Cardiovasc. Interv. 2013, 6, 1072–1084. [Google Scholar] [CrossRef] [Green Version]
- Mahoney, F.I.; Barthel, D.W. Functional evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar] [PubMed]
- Ribeiro, G.S.; Melo, R.D.; Deresz, L.F.; Dal Lago, P.; Pontes, M.R.; Karsten, M. Cardiac rehabilitation programme after transcatheter aortic valve implantation versus surgical aortic valve replacement: Systematic review and meta-analysis. Eur. J. Prev. Cardiol. 2017, 24, 688–697. [Google Scholar] [CrossRef] [PubMed]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Johns, M.W. A new method for measuring daytime sleepiness: The Epworth sleepiness scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- About the ESS—Epworth Sleepiness Scale. Available online: https://epworthsleepinessscale.com/about-the-ess/ (accessed on 1 December 2020).
- Team, RC. R: A Language and Environment for Statistical Computing. Vienna, Austria. 2020. Available online: https://www.R-project.org/ (accessed on 1 December 2020).
- Alharbi, M.; Straiton, N.; Smith, S.; Neubeck, L.; Gallagher, R. Data management and wearables in older adults: A systematic review. Maturitas 2019, 124, 100–110. [Google Scholar] [CrossRef] [PubMed]
- Finley, D.J.; Fay, K.A.; Batsis, J.A.; Stevens, C.J.; Sacks, O.A.; Darabos, C.; Cook, S.B.; Lyons, K.D. A feasibility study of an unsupervised, pre-operative exercise program for adults with lung cancer. Eur. J. Cancer Care (Engl.) 2020, 29, e13254. [Google Scholar] [CrossRef]
- Mercer, K.; Giangregorio, L.; Schneider, E.; Chilana, P.; Li, M.; Grindrod, K. Acceptance of Commercially Available Wearable Activity Trackers Among Adults Aged Over 50 and With Chronic Illness: A Mixed-Methods Evaluation. JMIR mHealth uHealth 2016, 4, e7. [Google Scholar] [CrossRef] [PubMed]
- Henriksen, A.; Sand, A.-S.; Deraas, T.; Grimsgaard, S.; Hartvigsen, G.; Hopstock, L. Succeeding with prolonged usage of consumer-based activity trackers in clinical studies: A mixed methods approach. BMC Public Health 2020, 20, 1300. [Google Scholar] [CrossRef] [PubMed]
- Tedesco, S.; Barton, J.; O’Flynn, B. A Review of Activity Trackers for Senior Citizens: Research Perspectives, Commercial Landscape and the Role of the Insurance Industry. Sensors 2017, 17, 1277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hermsen, S.; Moons, J.; Kerkhof, P.; Wiekens, C.; De Groot, M. Determinants for Sustained Use of an Activity Tracker: Observational Study. JMIR mHealth uHealth 2017, 5, e164. [Google Scholar] [CrossRef] [Green Version]
- Baig, M.M.; Afifi, S.; GholamHosseini, H.; Mirza, F. A Systematic Review of Wearable Sensors and IoT-Based Monitoring Applications for Older Adults—A Focus on Ageing Population and Independent Living. J. Med. Syst. 2019, 43, 233. [Google Scholar] [CrossRef]
- Preusse, K.C.; Mitzner, T.L.; Fausset, C.B.; Rogers, W.A. Older Adults’ Acceptance of Activity Trackers. J. Appl. Gerontol. 2017, 36, 127. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.; Choudhury, A. Comparison of Older and Younger Adults’ Attitudes Toward the Adoption and Use of Activity Trackers. JMIR mHealth uHealth 2020, 8, e18312. [Google Scholar] [CrossRef]
- Batsis, J.A.; Naslund, J.A.; Zagaria, A.B.; Kotz, D.; Dokko, R.; Bartels, S.J.; Carpenter-Song, E. Technology for Behavioral Change in Rural Older Adults with Obesity. J. Nutr. Gerontol. Geriatr. 2019, 38, 130–148. [Google Scholar] [CrossRef] [PubMed]
- Martinato, M.; Lorenzoni, G.; Zanchi, T.; Bergamin, A.; Buratin, A.; Azzolina, D.; Gregori, D. Assessment of Physical Activity in the Elderly Population: Usability and Accuracy of a Smartwatch. JMIR mHealth uHealth 2021, 9, e20966. [Google Scholar] [CrossRef]
- Kristoffersson, A.; Lindén, M. A Systematic Review on the Use of Wearable Body Sensors for Health Monitoring: A Qualitative Synthesis. Sensors 2020, 20, 1502. [Google Scholar] [CrossRef] [Green Version]
- Kononova, A.; Li, L.; Kamp, K.; Bowen, M.; Rikard, R.V.; Cotten, S.; Peng, W. The Use of Wearable Activity Trackers Among Older Adults: Focus Group Study of Tracker Perceptions, Motivators, and Barriers in the Maintenance Stage of Behavior Change. JMIR mHealth uHealth 2019, 7, e9832. [Google Scholar] [CrossRef] [PubMed]
- Brickwood, K.-J.; Watson, G.; O’Brien, J.; Williams, A.D. Consumer-Based Wearable Activity Trackers Increase Physical Activity Participation: Systematic Review and Meta-Analysis. JMIR mHealth uHealth 2019, 7, e11819. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N | SAVR (N = 5) | TAVR (N = 12) | Overall (N = 17) | p Value | ||
|---|---|---|---|---|---|---|
| Center | Padova | 17 | 100% (5) | 67% (8) | 76% (13) | 0.14 |
| Vicenza | 0% (0) | 33% (4) | 24% (4) | |||
| Drop out | Yes | 17 | 40% (2) | 50% (6) | 47% (8) | 0.71 |
| Gender | Female | 17 | 40% (2) | 67% (8) | 59% (10) | 0.31 |
| Male | 60% (3) | 33% (4) | 41% (7) | |||
| Age | 17 | 76/78/79 | 79/82/85 | 78/79/83 | 0.046 | |
| Marital status | Married cohabitant | 17 | 80% (4) | 67% (8) | 71% (12) | 0.58 |
| Widowed unmarried | 20% (1) | 33% (4) | 29% (5) | |||
| Educational level | Primary | 16 | 40% (2) | 64% (7) | 56% (9) | 0.38 |
| Secondary | 60% (3) | 36% (4) | 44% (7) | |||
| Risk factors | Diabetes | 17 | 0% (0) | 8% (1) | 6% (1) | 0.47 |
| Hypertension | 100% (5) | 75% (9) | 82% (14) | |||
| Smoker | 0% (0) | 17% (2) | 12% (2) | |||
| Status | Elective | 16 | 100% (5) | 82% (9) | 88% (14) | 0.31 |
| Urgent | 0% (0) | 18% (2) | 12% (2) | |||
| Clinical frailty scale | Well | 17 | 40% (2) | 8% (1) | 18% (3) | 0.25 |
| Managing well | 40% (2) | 17% (2) | 24% (4) | |||
| Vulnerable | 0% (0) | 33% (4) | 24% (4) | |||
| Mildly Frail | 20% (1) | 25% (3) | 24% (4) | |||
| Moderate Frail | 0% (0) | 17% (2) | 12% (2) | |||
| NYHA class | 1 | 16 | 20% (1) | 9% (1) | 12% (2) | 0.82 |
| 2 | 60% (3) | 64% (7) | 62% (10) | |||
| 3 | 20% (1) | 27% (3) | 25% (4) | |||
| COPD | 17 | 0% (0) | 8% (1) | 6% (1) | 0.78 | |
| Ejection fraction | 15 | 57/60/62 | 50/58/61 | 54/58/62 | 0.49 |
| Baseline | 1 Month | 3 Months | 6 Months | 12 Months | ||
|---|---|---|---|---|---|---|
| Barthel Index | SAVR | 88/95/98 | 92/95/98 | 95/100/100 | 72/95/98 | 80/100/100 |
| TAVR | 90/90/100 | 70/70/85 | 80/85/90 | 90/95/95 | 85/85/100 | |
| DASI score | SAVR | 21.6/30.4/31.9 | 8.2/16.4/20.8 | 14.5/16.2/19.8 | 12.6/23.4/25.2 | 12.2/19.9/22.6 |
| TAVR | 10.7/14.4/20.4 | 7.2/7.2/14.4 | 12.7/16.4/32.5 | 10.7/15.4/26.9 | 7.2/12.8/24.4 | |
| IADL score | SAVR | 4.5/6.0/6.5 | 2.5/5.0/6.0 | 2.5/3.0/4.0 | 1.5/3.0/3.5 | 3.5/5.0/5.5 |
| TAVR | 5/6/6 | 2/4/4 | 2/4/6 | 2/3/6 | 3/5/8 | |
| ESS score | SAVR | 1.0/2.0/6.0 | 2.5/4.0/5.0 | 2.5/3.0/4.5 | 3.0/4.0/6.0 | 3.0/3.0/5.5 |
| TAVR | 3/3/3 | 3/3/4 | 3/5/5 | 4/4/5 | 5/5/5 |
| Period. | SAVR (N = 3) | TAVR (N = 5) | Combined (N = 8) | p Value |
|---|---|---|---|---|
| Overall | 76/82/96 84+/13 | 39/83/100 71+/34 | 73/82/100 76+/28 | 0.92 |
| Pre | 89/100/100 93+/12 | 25/86/100 67+/39 | 65/93/100 77+/33 | 0.47 |
| Post | 71.1/75.1/80.1 75.8+/0.091 | 79.5/79.8/99.5 75.9+/32.4 | 73.1/79.6/88.8 75.9+/25.0 | 0.5 |
| N | SAVR (N = 3) | TAVR (N = 5) | Combined (N = 8) | p Value | |
|---|---|---|---|---|---|
| Perceived usefulness (30) | 7 | 16/16/16 | 17/17/17 | 17/17/17 | 0.16 |
| Perceived ease of use (35) | 7 | 29/30/31 | 32/32/32 | 30/32/32 | 0.57 |
| Equipment characteristics (10) | 7 | 30/31/32 | 30/31/32 | 30/31/32 | 0.73 |
| Privacy concern (15) | 7 | 7.0/8.0/9.0 | 9.0/9.0/9.0 | 8.0/9.0/9.5 | 0.72 |
| Perceived risk (15) | 7 | 10/10/10 | 5/5/5 | 5/5/8 | 0.009 |
| Facilitating conditions (10) | 7 | 5.8/6.5/7.2 | 7.0/7.0/7.0 | 6.5/7.0/7.5 | 0.86 |
| Subjective norm (15) | 7 | 9.5/10.0/10.5 | 8.0/9.0/10.0 | 8.5/9.0/10.5 | 0.48 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ocagli, H.; Lorenzoni, G.; Lanera, C.; Schiavo, A.; D’Angelo, L.; Liberti, A.D.; Besola, L.; Cibin, G.; Martinato, M.; Azzolina, D.; et al. Monitoring Patients Reported Outcomes after Valve Replacement Using Wearable Devices: Insights on Feasibility and Capability Study: Feasibility Results. Int. J. Environ. Res. Public Health 2021, 18, 7171. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137171
Ocagli H, Lorenzoni G, Lanera C, Schiavo A, D’Angelo L, Liberti AD, Besola L, Cibin G, Martinato M, Azzolina D, et al. Monitoring Patients Reported Outcomes after Valve Replacement Using Wearable Devices: Insights on Feasibility and Capability Study: Feasibility Results. International Journal of Environmental Research and Public Health. 2021; 18(13):7171. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137171
Chicago/Turabian StyleOcagli, Honoria, Giulia Lorenzoni, Corrado Lanera, Alessandro Schiavo, Livio D’Angelo, Alessandro Di Liberti, Laura Besola, Giorgia Cibin, Matteo Martinato, Danila Azzolina, and et al. 2021. "Monitoring Patients Reported Outcomes after Valve Replacement Using Wearable Devices: Insights on Feasibility and Capability Study: Feasibility Results" International Journal of Environmental Research and Public Health 18, no. 13: 7171. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137171