
Neighborhood Characteristics and Cancer Survivorship: An Overview of the Current Literature on Neighborhood Landscapes and Cancer Care

Abstract
:1. Introduction
2. Materials and Methods
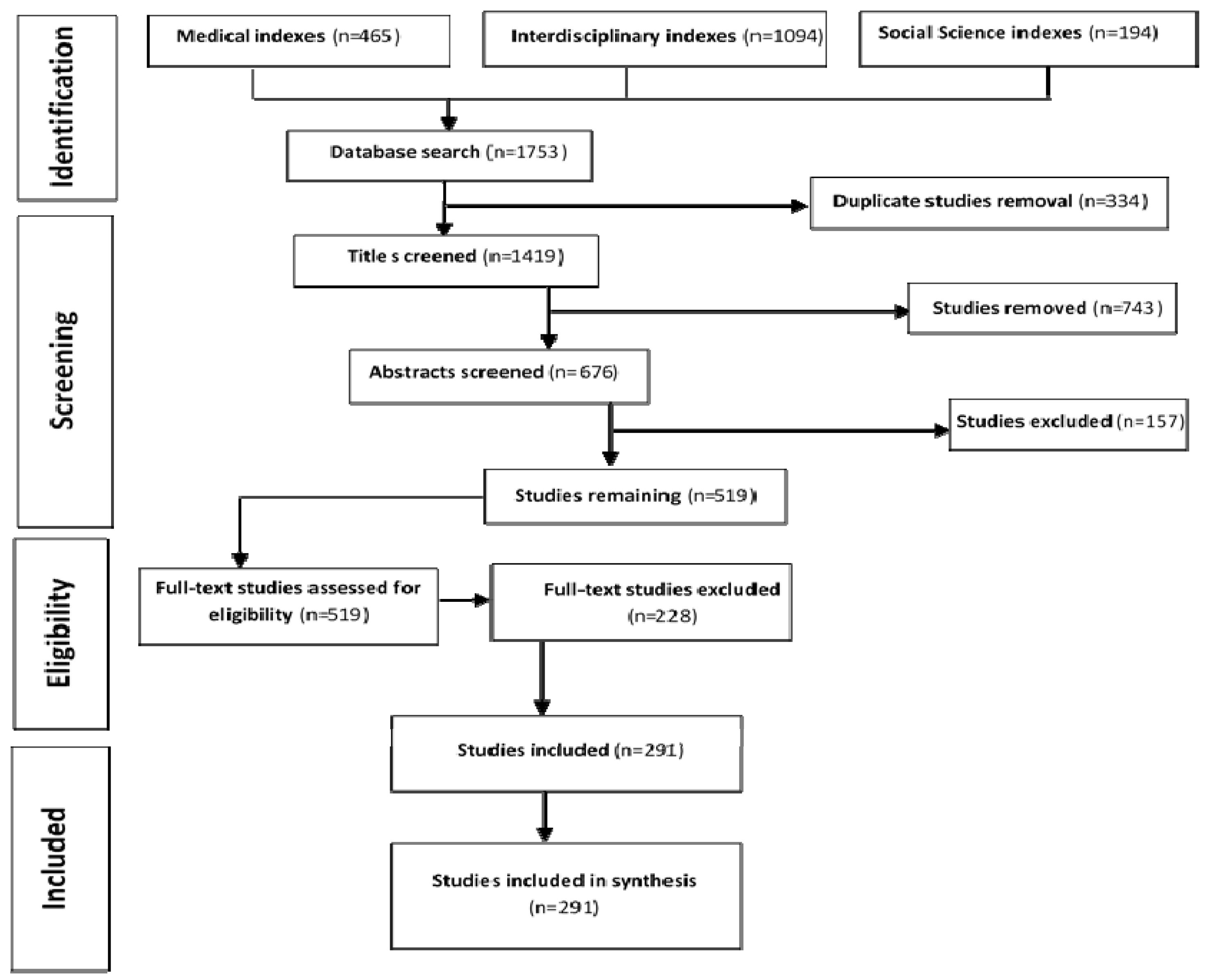
2.1. Search Strategy and Identification of Relevant Studies
2.2. Inclusion Criteria
2.3. Data Processing and Extraction from Included Studies
2.4. Collating, Summarizing and Reporting the Findings
2.5. Conceptualizing the Findings
3. Results
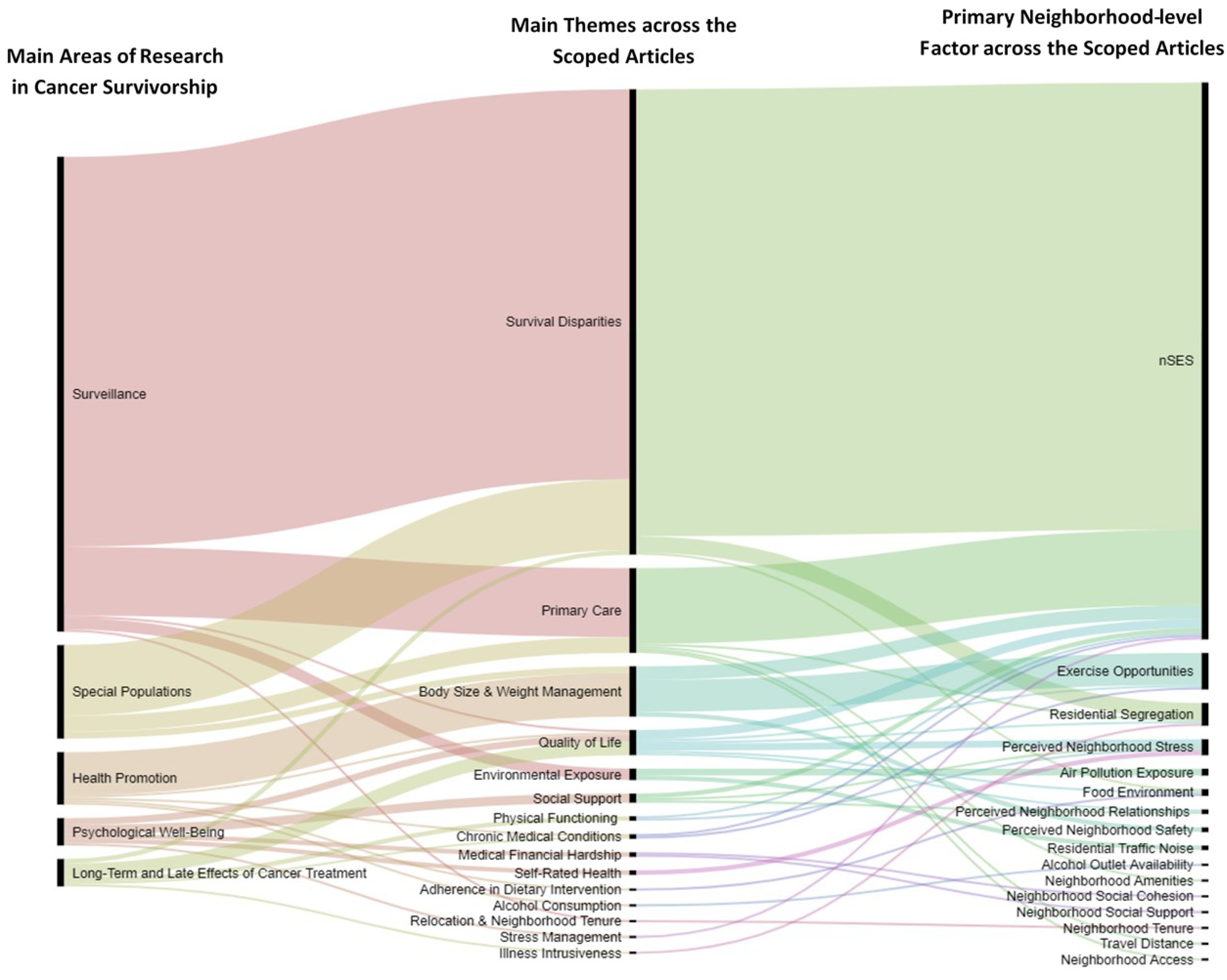
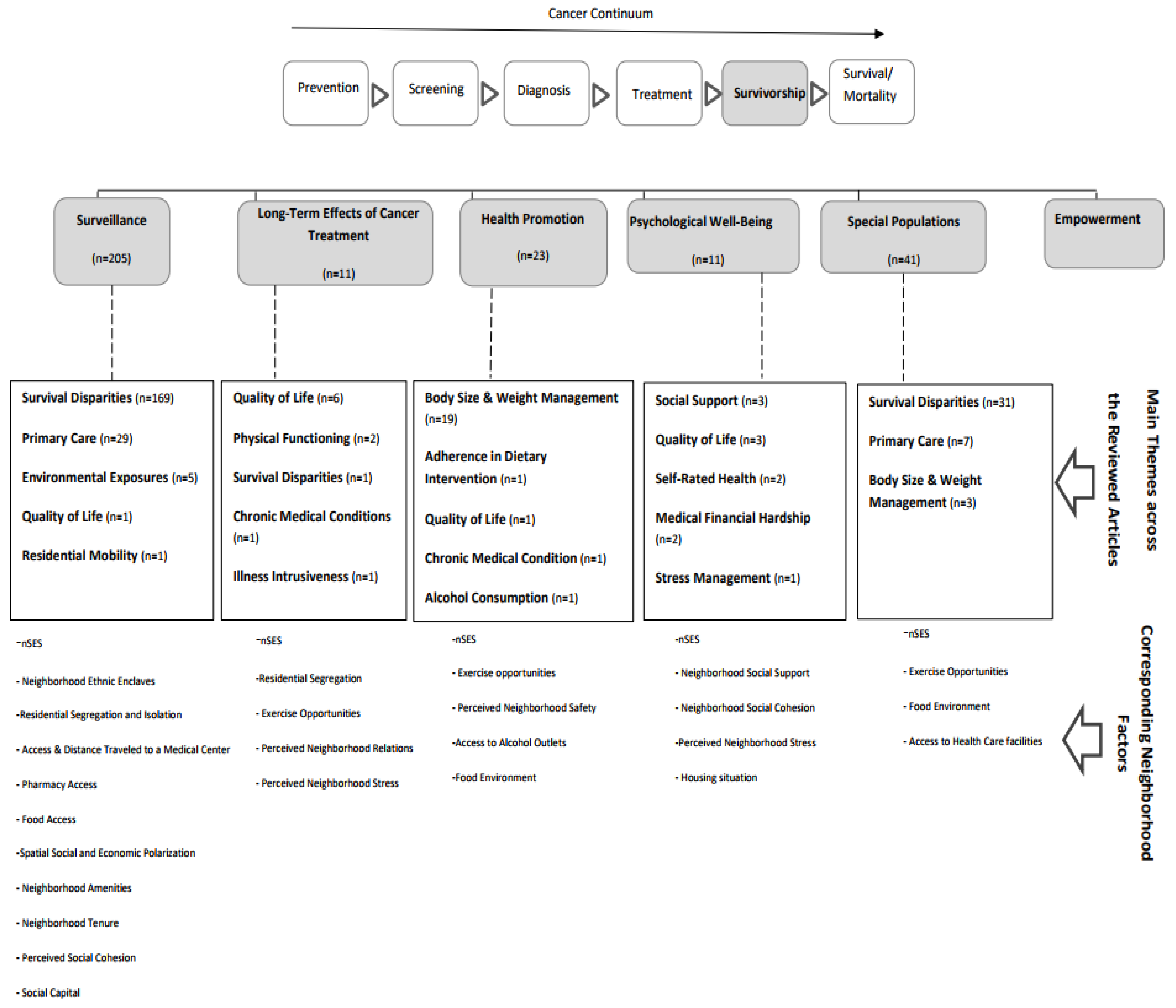
3.1. Main Areas of Cancer Survivorship Research and Utilized Neighborhood Metrics
3.1.1. Surveillance
3.1.2. Long-Term Effects of Cancer Treatment
3.1.3. Health Promotion
3.1.4. Psychological Well-Being
3.1.5. Special Populations
3.2. Overlaps between Neighborhood Metrics Utilized in the Scoped Articles and LEED-ND Metrics
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- World Health Organization Cancer. Available online: https://www.who.int/health-topics/cancer#tab=tab_1 (accessed on 13 July 2020).
- American Cancer Society. Cancer Treatment & Survivorship Facts & Figures 2019–2021; American Cancer Society: New York, NY, USA, 2019. [Google Scholar]
- The Cancer Atlas Cancer Survivorship. Available online: canceratlas.cancer.org (accessed on 13 July 2020).
- Miller, K.D.; Nogueira, L.; Mariotto, A.B.; Rowland, J.H.; Yabroff, K.R.; Alfano, C.M.; Jemal, A.; Kramer, J.L.; Siegel, R.L. Cancer treatment and survivorship statistics, 2019. CA. Cancer J. Clin. 2019, 69, 363–385. [Google Scholar] [CrossRef] [Green Version]
- Halpern, M.T.; McCabe, M.S.; Burg, M.A. The Cancer Survivorship Journey: Models of Care, Disparities, Barriers, and Future Directions. Am. Soc. Clin. Oncol. Educ. B 2016, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Husain, M.; Nolan, T.S.; Foy, K.; Reinbolt, R.; Grenade, C.; Lustberg, M. An overview of the unique challenges facing African-American breast cancer survivors. Support. Care Cancer 2019, 27, 729–743. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.A.; Andrews, K.S.; Brooks, D.; Fedewa, S.A.; Manassaram-Baptiste, D.; Saslow, D.; Brawley, O.W.; Wender, R.C. Cancer screening in the United States, 2017: A review of current American Cancer Society guidelines and current issues in cancer screening. CA. Cancer J. Clin. 2017, 67, 100–121. [Google Scholar] [CrossRef] [PubMed]
- Paice, J.A.; Portenoy, R.; Lacchetti, C.; Campbell, T.; Cheville, A.; Citron, M.; Constine, L.S.; Cooper, A.; Glare, P.; Keefe, F.; et al. Management of chronic pain in survivors of adult cancers: American Society of Clinical Oncology clinical practice guideline. J. Clin. Oncol. 2016, 34, 3325–3345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ligibel, J.A.; Alfano, C.M.; Courneya, K.S.; Demark-Wahnefried, W.; Burger, R.A.; Chlebowski, R.T.; Fabian, C.J.; Gucalp, A.; Hershman, D.L.; Hudson, M.M.; et al. American Society of Clinical Oncology Position Statement on Obesity and Cancer. Obstet. Gynecol. Surv. 2015, 70, 28–29. [Google Scholar] [CrossRef] [Green Version]
- Schwedhelm, C.; Boeing, H.; Hoffmann, G.; Aleksandrova, K.; Schwingshackl, L. Effect of diet on mortality and cancer recurrence among cancer survivors: A systematic review and meta-analysis of cohort studies - PubMed. Nutr. Rev. 2016, 74, 737–748. [Google Scholar] [CrossRef] [Green Version]
- Ramaswamy, A.T.; Toll, B.A.; Chagpar, A.B.; Judson, B.L. Smoking, cessation, and cessation counseling in patients with cancer: A population-based analysis. Cancer 2016, 122, 1247–1253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- LoConte, N.K.; Brewster, A.M.; Kaur, J.S.; Merrill, J.K.; Alberg, A.J. Alcohol and cancer: A statement of the American society of clinical oncology. J. Clin. Oncol. 2018, 36, 83–93. [Google Scholar] [CrossRef] [Green Version]
- Storey, L.; Fern, L.A.; Martins, A.; Wells, M.; Bennister, L.; Gerrand, C.; Onasanya, M.; Whelan, J.S.; Windsor, R.; Woodford, J.; et al. A Critical Review of the Impact of Sarcoma on Psychosocial Wellbeing. Sarcoma 2019, 2019. [Google Scholar] [CrossRef]
- Shapiro, C.L. Cancer Survivorship. N. Engl. J. Med. 2018, 379, 2438–2450. [Google Scholar] [CrossRef] [PubMed]
- Jørgensen, C.R.; Thomsen, T.G.; Ross, L.; Dietz, S.M.; Therkildsen, S.; Groenvold, M.; Rasmussen, C.L.; Johnsen, A.T. What Facilitates “Patient Empowerment” in Cancer Patients During Follow-Up: A Qualitative Systematic Review of the Literature. Qual. Health Res. 2018, 28, 292–304. [Google Scholar] [CrossRef]
- Wray, A.J.D.; Minaker, L.M. Is cancer prevention influenced by the built environment? A multidisciplinary scoping review. Cancer 2019, 125, 3299–3311. [Google Scholar] [CrossRef] [PubMed]
- Bates, J.E.; Howell, R.M.; Liu, Q.; Yasui, Y.; Mulrooney, D.A.; Dhakal, S.; Smith, S.A.; Leisenring, W.M.; Indelicato, D.J.; Gibson, T.M.; et al. Therapy-related cardiac risk in childhood cancer survivors: An analysis of the childhood cancer survivor study. J. Clin. Oncol. 2019, 37, 1090–1101. [Google Scholar] [CrossRef] [Green Version]
- Fong, A.J.; Lafaro, K.; Ituarte, P.H.G.; Fong, Y. Association of Living in Urban Food Deserts with Mortality from Breast and Colorectal Cancer. Ann. Surg. Oncol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Day, B.H. The Value of Greenspace Under Pandemic Lockdown. Environ. Resour. Econ. 2020, 1–25. [Google Scholar] [CrossRef]
- Plascak, J.J.; Llanos, A.A.M.; Qin, B.; Chavali, L.; Lin, Y.; Pawlish, K.S.; Goldman, N.; Hong, C.C.; Demissie, K.; Bandera, E.V. Visual cues of the built environment and perceived stress among a cohort of black breast cancer survivors. Health Place 2021, 67, 102498. [Google Scholar] [CrossRef]
- Vijayasiri, G.; Molina, Y.; Chukwudozie, I.; Tejeda, S.; Pauls, H.; Rauscher, G.; Campbell, R.; Warnecke, R. Racial Disparities in Breast Cancer Survival: The Mediating Effects of Macro-Social Context and Social Network Factors. J. Health Dispar. Res. Pract. 2018, 11, 6. [Google Scholar]
- O’Brien, K.M.; Timmons, A.; Butow, P.; Gooberman-Hill, R.; O’Sullivan, E.; Balfe, M.; Sharp, L. Associations between neighbourhood support and financial burden with unmet needs of head and neck cancer survivors. Oral Oncol. 2017, 65, 57–64. [Google Scholar] [CrossRef] [Green Version]
- Porcherie, M.; Linn, N.; Roué Le Gall, A.; Thomas, M.-F.; Faure, E.; Rican, S.; Simos, J.; Cantoreggi, N.; Vaillant, Z.; Cambon, L.; et al. Relationship between urban green spaces and cancer: A scoping review. Int. J. Environ. Res. Public Health 2021, 18, 1751. [Google Scholar] [CrossRef]
- Sucharew, H.; Macaluso, M. Methods for research evidence synthesis: The scoping review approach. J. Hosp. Med. 2019, 14, 416–418. [Google Scholar] [CrossRef] [Green Version]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- U.S. Green Building Council LEED for Neighborhood Development. Available online: http://leed.usgbc.org/nd.html (accessed on 18 October 2020).
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 1–7. [Google Scholar] [CrossRef]
- Thomas, A.; Lubarsky, S.; Durning, S.J.; Young, M.E. Knowledge Syntheses in Medical Education. Acad. Med. 2017, 92, 161–166. [Google Scholar] [CrossRef] [Green Version]
- Mayer, D.K.; Nasso, S.F.; Earp, J.A. Defining cancer survivors, their needs, and perspectives on survivorship health care in the USA. Lancet Oncol. 2017, 18, e11–e18. [Google Scholar] [CrossRef]
- Mendeley. 2018. Available online: https://www.mendeley.com/ (accessed on 5 July 2021).
- Microsoft Corporation. Microsoft Excel. 2016. Available online: https://www.microsoft.com/en-us/microsoft-365/33 (accessed on 5 July 2021).
- Mauri, M.; Elli, T.; Caviglia, G.; Uboldi, G.; Azzi, M. RAWGraphs: A Visualisation Platform to Create Open Outputs. In Proceedings of the 12th Biannual Conference on Italian SIGCHI Chapter, Cagliari, Italy, 18–20 September 2017; pp. 28:1–28:5. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, N.; Buliung, R.; Wilson, K. Disability and food access and insecurity: A scoping review of the literature. Health Place 2019, 57, 107–121. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. LEED-ND and Healthy Neighborhoods: An Expert Panel Review; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2008. [Google Scholar]
- Cooney, T.; Fisher, P.G.; Tao, L.; Clarke, C.A.; Partap, S. Pediatric neuro-oncology survival disparities in California. J. Neurooncol. 2018, 138, 83–97. [Google Scholar] [CrossRef]
- Johnson, A.M.; Johnson, A.; Hines, R.B.; Bayakly, R. The effects of residential segregation and neighborhood characteristics on surgery and survival in patients with early-stage non?small cell lung cancer. Cancer Epidemiol. Biomarkers Prev. 2016, 25, 750–758. [Google Scholar] [CrossRef] [Green Version]
- Lamont, E.B.; Hayreh, D.; Pickett, K.E.; Dignam, J.J.; List, M.A.; Stenson, K.M.; Haraf, D.J.; Brockstein, B.E.; Sellergren, S.A.; Vokes, E.E. Is patient travel distance associated with survival on phase II clinical trials in oncology? J. Natl. Cancer Inst. 2003, 95, 1370–1375. [Google Scholar] [CrossRef] [Green Version]
- Jefferson, K.; Quest, T.; Yeager, K.A. Factors Associated with Black Cancer Patients’ Ability to Obtain Their Opioid Prescriptions at the Pharmacy. J. Palliat. Med. 2019, 22, 1143–1148. [Google Scholar] [CrossRef] [PubMed]
- Boehmer, U.; Potter, J.; Clark, M.A.; Ozonoff, A.; Ceballos, R.M.; Winter, M.; Hartshorn, K.L. Neighborhood Characteristics and Colorectal Cancer Survivors’ Quality of Care. Health Equity 2019, 3, 619–627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, B.; Lee, F.F.; Boscoe, F. Residential mobility among adult cancer survivors in the United States. BMC Public Health 2020, 20, 1601. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Narcisse, M.; McElfish, P.A. Medical financial hardship reported by Native Hawaiian and Pacific Islander cancer survivors compared with non-Hispanic whites. Cancer 2020, 126, 2900–2914. [Google Scholar] [CrossRef]
- Richter, N.L.; Gorey, K.M.; Haji-Jama, S.; Luginaah, I.N. Care and Survival of Mexican American Women with Node Negative Breast Cancer: Historical Cohort Evidence of Health Insurance and Barrio Advantages. J. Immigr. Minor. Health 2015, 17, 652–659. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamont, E.B.; Zaslavsky, A.M.; Subramanian, S.V.; Meilleur, A.E.; He, Y.; Landrum, M.B. Elderly breast and colorectal cancer patients’ clinical course: Patient and contextual influences. Med. Care 2014, 52, 809–817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdel-Rahman, O. Treatment choices and outcomes of non-metastatic hepatocellular carcinoma patients in relationship to neighborhood socioeconomic status: A population-based study. Int. J. Clin. Oncol. 2020, 25, 861–866. [Google Scholar] [CrossRef] [PubMed]
- Shah, M.; Parmar, A.; Chan, K.K.W. Socioeconomic disparity trends in diagnostic imaging, treatments, and survival for non-small cell lung cancer 2007-2016. Cancer Med. 2020, 9, 3407–3416. [Google Scholar] [CrossRef] [Green Version]
- Bristow, R.E.; Chang, J.; Ziogas, A.; Randall, L.M.; Anton-Culver, H. High-volume ovarian cancer care: Survival impact and disparities in access for advanced-stage disease. Gynecol. Oncol. 2014, 132, 403–410. [Google Scholar] [CrossRef] [Green Version]
- Schupp, C.W.; Press, D.J.; Gomez, S.L. Immigration factors and prostate cancer survival among Hispanic men in California: Does neighborhood matter? Cancer 2014, 120, 1401–1408. [Google Scholar] [CrossRef] [Green Version]
- Russell, E.; Kramer, M.R.; Cooper, H.L.F.; Thompson, W.W.; Arriola, K.R.J. Residential racial composition, spatial access to care, and breast cancer mortality among women in Georgia. J. Urban Health 2011, 88, 1117–1129. [Google Scholar] [CrossRef] [Green Version]
- Collin, L.J.; Gaglioti, A.H.; Beyer, K.M.; Zhou, Y.; Moore, M.A.; Nash, R.; Switchenko, J.M.; Miller-Kleinhenz, J.M.; Ward, K.C.; McCullough, L.E. Neighborhood-level redlining and lending bias are associated with breast cancer mortality in a large and diverse metropolitan area. Cancer Epidemiol. Prev. Biomark. 2021, 30, 53–60. [Google Scholar] [CrossRef]
- Beyer, K.; Zhou, Y.; Matthews, K.; Bemanian, A.; Laud, P.; Bemanian, A.; Nattinger, A.B. New spatially continuous indices of redlining and racial bias in mortgage lending: Links to survival after breast cancer diagnosis and implications for health disparities research. Health Place 2016, 40, 34–43. [Google Scholar] [CrossRef]
- Leach, C.R.; Vereen, R.N.; Rao, A.V.; Ross, K.; Diefenbach, M.A. Impact of individual- and area-level race/ethnicity on illness intrusiveness among cancer survivors | Translational Behavioral Medicine | Oxford Academic. Transl. Behav. Med. 2019, 9, 1208–1215. [Google Scholar] [CrossRef]
- Schootman, M.; Perez, M.; Schootman, J.C.; Fu, Q.; McVay, A.; Margenthaler, J.; Colditz, G.A.; Kreuter, M.W.; Jeffe, D.B. Influence of built environment on quality of life changes in African-American patients with early-stage breast cancer. Health Place 2020, 63, 102333. [Google Scholar] [CrossRef] [PubMed]
- Yan, B.; Yang, L.M.; Hao, L.P.; Yang, C.; Quan, L.; Wang, L.H.; Wu, Z.; Li, X.P.; Gao, Y.T.; Sun, Q.; et al. Determinants of quality of life for breast cancer patients in Shanghai, China. PLoS ONE 2016, 11, 153714. [Google Scholar] [CrossRef] [Green Version]
- Ashing-Giwa, K.T.; Lim, J.W. Predicting physical quality of life among a multiethnic sample of breast cancer survivors. Qual. Life Res. 2010, 19, 789–802. [Google Scholar] [CrossRef] [PubMed]
- Kent, E.E.; Sender, L.S.; Morris, R.A.; Grigsby, T.J.; Montoya, M.J.; Ziogas, A.; Anton-Culver, H. Multilevel socioeconomic effects on quality of life in adolescent and young adult survivors of leukemia and lymphoma. Qual. Life Res. 2013, 22, 1339–1351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pruitt, S.L.; McQueen, A.; Deshpande, A.D.; Jeffe, D.B.; Schootman, M. Mediators of the effect of neighborhood poverty on physical functioning among breast cancer survivors: A longitudinal study. Cancer Causes Control 2012, 23, 1529–1540. [Google Scholar] [CrossRef]
- Stalsberg, R.; Eikemo, T.A.; Lundgren, S.; Reidunsdatter, R.J. Physical activity in long-term breast cancer survivors – A mixed-methods approach. Breast 2019, 46, 126–135. [Google Scholar] [CrossRef] [Green Version]
- Kwarteng, J.L.; Beyer, K.M.M.; Banerjee, A.; Stolley, M.R. Facilitators of behavior change and weight loss in an intervention for African American Breast Cancer Survivors. Cancer Causes Control 2020, 31, 737–747. [Google Scholar] [CrossRef]
- DeGuzman, P.B.; Chu, C.; Keim-Malpass, J. Built and Natural Environment Barriers and Facilitators to Physical Activity in Rural, Suburban, and Small Urban Neighborhoods. Oncol. Nurs. Forum 2019, 46, 545–555. [Google Scholar] [CrossRef]
- Trinh, L.; Larsen, K.; Faulkner, G.E.; Plotnikoff, R.C.; Rhodes, R.E.; North, S.; Courneya, K.S. Social-ecological correlates of physical activity in kidney cancer survivors. J. Cancer Surviv. 2016, 10, 164–175. [Google Scholar] [CrossRef] [PubMed]
- Lune, H.; Berg, B.L. Qualitative Resaearch Methods for the Social Sciences; Pearson: London, UK, 2017; ISBN 9780134202136. [Google Scholar]
- Hastert, T.A.; McDougall, J.A.; Strayhorn, S.M.; Nair, M.; Beebe-Dimmer, J.L.; Schwartz, A.G. Social needs and health-related quality of life among African American cancer survivors: Results from the Detroit Research on Cancer Survivors study. Cancer 2021, 127, 467–475. [Google Scholar] [CrossRef]
- Brunet, J.; Taran, S.; Burke, S.; Sabiston, C.M. A qualitative exploration of barriers and motivators to physical activity participation in women treated for breast cancer. Disabil. Rehabil. 2013, 35, 2038–2045. [Google Scholar] [CrossRef] [PubMed]
- Spector, D.; Battaglini, C.; Groff, D. Perceived exercise barriers and facilitators among ethnically diverse breast cancer survivors. Oncol. Nurs. Forum 2013, 40, 472–480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schootman, M.; Deshpande, A.D.; Lynskey, M.T.; Pruitt, S.L.; Lian, M.; Jeffe, D.B. Alcohol Outlet Availability and Excessive Alcohol Consumption in Breast Cancer Survivors. J. Prim. Care Community Heal. 2013, 4, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Lynch, B.M.; Owen, N.; Hawkes, A.L.; Aitken, J.F. Perceived barriers to physical activity for colorectal cancer survivors. Support. Care Cancer 2010, 18, 729–734. [Google Scholar] [CrossRef]
- McGowan, E.L.; Fuller, D.; Cutumisu, N.; North, S.; Courneya, K.S. The role of the built environment in a randomized controlled trial to increase physical activity among men with prostate cancer: The PROMOTE trial. Support. Care Cancer 2017, 25, 2993–2996. [Google Scholar] [CrossRef]
- Tejeda, S.; Stolley, M.R.; Vijayasiri, G.; Campbell, R.T.; Estwing Ferrans, C.; Warnecke, R.B.; Rauscher, G.H. Negative psychological consequences of breast cancer among recently diagnosed ethnically diverse women. Psychooncology. 2017, 26, 2245–2252. [Google Scholar] [CrossRef]
- Ashing-Giwa, K.T.; Lim, J.W. Examining the impact of socioeconomic status and socioecologic stress on physical and mental health quality of life among breast cancer survivors. Oncol. Nurs. Forum 2009, 36, 79–88. [Google Scholar] [CrossRef]
- Wu, C.; Ashing, K.T.; Jones, V.C.; Barcelo, L. The association of neighborhood context with health outcomes among ethnic minority breast cancer survivors. J. Behav. Med. 2018, 41, 52–61. [Google Scholar] [CrossRef] [PubMed]
- Schootman, M.; Deshpande, A.D.; Pruitt, S.L.; Jeffe, D.B. Neighborhood foreclosures and self-rated health among breast cancer survivors. Qual. Life Res. 2012, 21, 133–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Howell, C.R.; Wilson, C.L.; Yasui, Y.; Srivastava, D.K.; Lu, W.; Bjornard, K.L.; Ehrhardt, M.J.; Brinkman, T.M.; Chemaitilly, W.; Hodges, J.R.; et al. Neighborhood effect and obesity in adult survivors of pediatric cancer: A report from the St. Jude lifetime cohort study. Int. J. Cancer 2020, 147, 338–349. [Google Scholar] [CrossRef]
- Slater, M.E.; Kelly, A.S.; Sadak, K.T.; Ross, J.A. Active transportation in adult survivors of childhood cancer and neighborhood controls. J. Cancer Surviv. 2016, 10, 11–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schootman, M.; Jeffe, D.B.; Lian, M.; Deshpande, A.D.; Gillanders, W.E.; Aft, R.; Sumner, W. Area-Level Poverty Is Associated with Greater Risk of Ambulatory–Care–Sensitive Hospitalizations in Older Breast Cancer Survivors. J. Am. Geriatr. Soc. 2008, 56, 2180–2187. [Google Scholar] [CrossRef] [Green Version]
- Dawes, A.J.; Louie, R.; Nguyen, D.K.; Maggard-Gibbons, M.; Parikh, P.; Ettner, S.L.; Ko, C.Y.; Zingmond, D.S. The impact of continuous medicaid enrollment on diagnosis, treatment, and survival in six surgical cancers. Health Serv. Res. 2014, 49, 1787–1811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, I.; Shariff-Marco, S.; Koo, J.; Monroe, K.R.; Yang, J.; John, E.M.; Kurian, A.W.; Kwan, M.L.; Henderson, B.E.; Bernstein, L.; et al. Contribution of the neighborhood environment and obesity to breast cancer survival: The California breast cancer survivorship consortium. Cancer Epidemiol. Biomark. Prev. 2015, 24, 1282–1290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shariff-Marco, S.; Gomez, S.L.; Sangaramoorthy, M.; Yang, J.; Koo, J.; Hertz, A.; John, E.M.; Cheng, I.; Keegan, T.H.M. Impact of neighborhoods and body size on survival after breast cancer diagnosis. Health Place 2015, 36, 162–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tabaczynski, A.; Strom, D.A.; Wong, J.N.; McAuley, E.; Larsen, K.; Faulkner, G.E.; Courneya, K.S.; Trinh, L. Demographic, medical, social-cognitive, and environmental correlates of meeting independent and combined physical activity guidelines in kidney cancer survivors. Support. Care Cancer 2020, 28, 43–54. [Google Scholar] [CrossRef]
- Keegan, T.H.M.; Shariff-Marco, S.; Sangaramoorthy, M.; Koo, J.; Hertz, A.; Schupp, C.W.; Yang, J.; John, E.M.; Gomez, S.L. Neighborhood influences on recreational physical activity and survival after breast cancer. Cancer Causes Control 2014, 25, 1295–1308. [Google Scholar] [CrossRef] [Green Version]
- Granger, C.L.; Denehy, L.; McDonald, C.F.; Irving, L.; Clark, R.A. Physical activity measured using global positioning system tracking in non-small cell lung cancer: An observational study. Integr. Cancer Ther. 2014, 13, 482–492. [Google Scholar] [CrossRef]
- Jankowska, M.M.; Natarajan, L.; Godbole, S.; Meseck, K.; Sears, D.D.; Patterson, R.E.; Kerr, J. Research article kernel density estimation as a measure of environmental exposure related to insulin resistance in breast cancer survivors. Cancer Epidemiol. Biomark. Prev. 2017, 26, 1078–1084. [Google Scholar] [CrossRef] [Green Version]
- Feathers, A.; Aycinena, A.C.; Lovasi, G.S.; Rundle, A.; Gaffney, A.O.; Richardson, J.; Hershman, D.; Koch, P.; Contento, I.; Greenlee, H. Food environments are relevant to recruitment and adherence in dietary modification trials. Nutr. Res. 2014, 35, 480–488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nekhlyudov, L.; Mollica, M.A.; Jacobsen, P.B.; Mayer, D.K.; Shulman, L.N.; Geiger, A.M. Developing a Quality of Cancer Survivorship Care Framework: Implications for Clinical Care, Research, and Policy. J. Natl. Cancer Inst. 2019, 111, 1120–1130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, C.C.; Matthews, A.K.; Asthana, A.; Shah, R.C. The impact of neighborhood disadvantage on health-related quality of life among African American and White cancer survivors. Transl. Cancer Res. 2019, 8, S313–S322. [Google Scholar] [CrossRef] [PubMed]
- Aguiñaga, S.; Ehlers, D.K.; Cosman, J.; Severson, J.; Kramer, A.F.; McAuley, E. Effects of physical activity on psychological well-being outcomes in breast cancer survivors from prediagnosis to posttreatment survivorship. Psychooncology 2018, 27, 1987–1994. [Google Scholar] [CrossRef]
- Choe, E.Y.; Jorgensen, A.; Sheffield, D. Does a natural environment enhance the effectiveness of Mindfulness-Based Stress Reduction (MBSR)? Examining the mental health and wellbeing, and nature connectedness benefits. Landsc. Urban Plan. 2020, 202. [Google Scholar] [CrossRef]
- Rogers, L.Q.; Courneya, K.S.; Anton, P.M.; Verhulst, S.; Vicari, S.K.; Robbs, R.S.; McAuley, E. Effects of a multicomponent physical activity behavior change intervention on fatigue, anxiety, and depressive symptomatology in breast cancer survivors: Randomized trial. Psychooncology. 2017, 26, 1901–1906. [Google Scholar] [CrossRef]
- Pinquart, M.; Duberstein, P.R. Associations of social networks with cancer mortality: A meta-analysis. Crit. Rev. Oncol. Hematol. 2010, 75, 122–137. [Google Scholar] [CrossRef] [Green Version]
- Moen, P.; Chermack, K. The Relationship of Built Environment to Perceived Social Support and Psychological Distress in Hispanic Elders: The Role of “Eyes on the Street. ” J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2005, 60, 234–246. [Google Scholar] [CrossRef]
- Yancik, R. Population aging and cancer: A cross-national concern. Cancer J. 2005, 11, 437–441. [Google Scholar] [CrossRef] [PubMed]
- Keegan, T.H.M.; Kushi, L.H.; Li, Q.; Brunson, A.; Chawla, X.; Chew, H.K.; Malogolowkin, M.; Wun, T. Cardiovascular disease incidence in adolescent and young adult cancer survivors: A retrospective cohort study. J. Cancer Surviv. 2018, 12, 388–397. [Google Scholar] [CrossRef] [PubMed]
- Kaal, S.E.J.; Husson, O.; van Duivenboden, S.; Jansen, R.; Manten-Horst, E.; Servaes, P.; Prins, J.B.; van den Berg, S.W.; van der Graaf, W.T.A. Empowerment in adolescents and young adults with cancer: Relationship with health-related quality of life. Cancer 2017, 123, 4039–4047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuijpers, W.; Groen, W.G.; Aaronson, N.K.; Van Harten, W.H. A systematic review of web-based interventions for patient empowerment and physical activity in chronic diseases: Relevance for cancer survivors. J. Med. Internet Res. 2013, 15, e37. [Google Scholar] [CrossRef] [Green Version]
- Van Den Berg, S.W.; Van Amstel, F.K.P.; Ottevanger, P.B.; Gielissen, M.F.M.; Prins, J.B. The cancer empowerment questionnaire: Psychological empowerment in breast cancer survivors. J. Psychosoc. Oncol. 2013, 31, 565–583. [Google Scholar] [CrossRef] [PubMed]
- Gomez, S.L.; Glaser, S.L.; McClure, L.A.; Shema, S.J.; Kealey, M.; Keegan, T.H.M.; Satariano, W.A. The California Neighborhoods Data System: A new resource for examining the impact of neighborhood characteristics on cancer incidence and outcomes in populations. Cancer Causes Control 2011, 22, 631–647. [Google Scholar] [CrossRef] [Green Version]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Area | LEED-ND Metrics | Metrics in the Scoped Articles |
|---|---|---|
| SLL Smart Location and Linkages | Smart Location (access to public transportation and walkability).
| Smart Location
|
| NPD Neighborhood Pattern and Design | Compact Development (promote livability, transportation efficiency, and walkability).
| Compact Development
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Namin, S.; Zhou, Y.; Neuner, J.; Beyer, K. Neighborhood Characteristics and Cancer Survivorship: An Overview of the Current Literature on Neighborhood Landscapes and Cancer Care. Int. J. Environ. Res. Public Health 2021, 18, 7192. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137192
Namin S, Zhou Y, Neuner J, Beyer K. Neighborhood Characteristics and Cancer Survivorship: An Overview of the Current Literature on Neighborhood Landscapes and Cancer Care. International Journal of Environmental Research and Public Health. 2021; 18(13):7192. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137192
Chicago/Turabian StyleNamin, Sima, Yuhong Zhou, Joan Neuner, and Kirsten Beyer. 2021. "Neighborhood Characteristics and Cancer Survivorship: An Overview of the Current Literature on Neighborhood Landscapes and Cancer Care" International Journal of Environmental Research and Public Health 18, no. 13: 7192. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137192