
Periodontal Conditions and Pathogens Associated with Pre-Eclampsia: A Scoping Review

 , and
, and 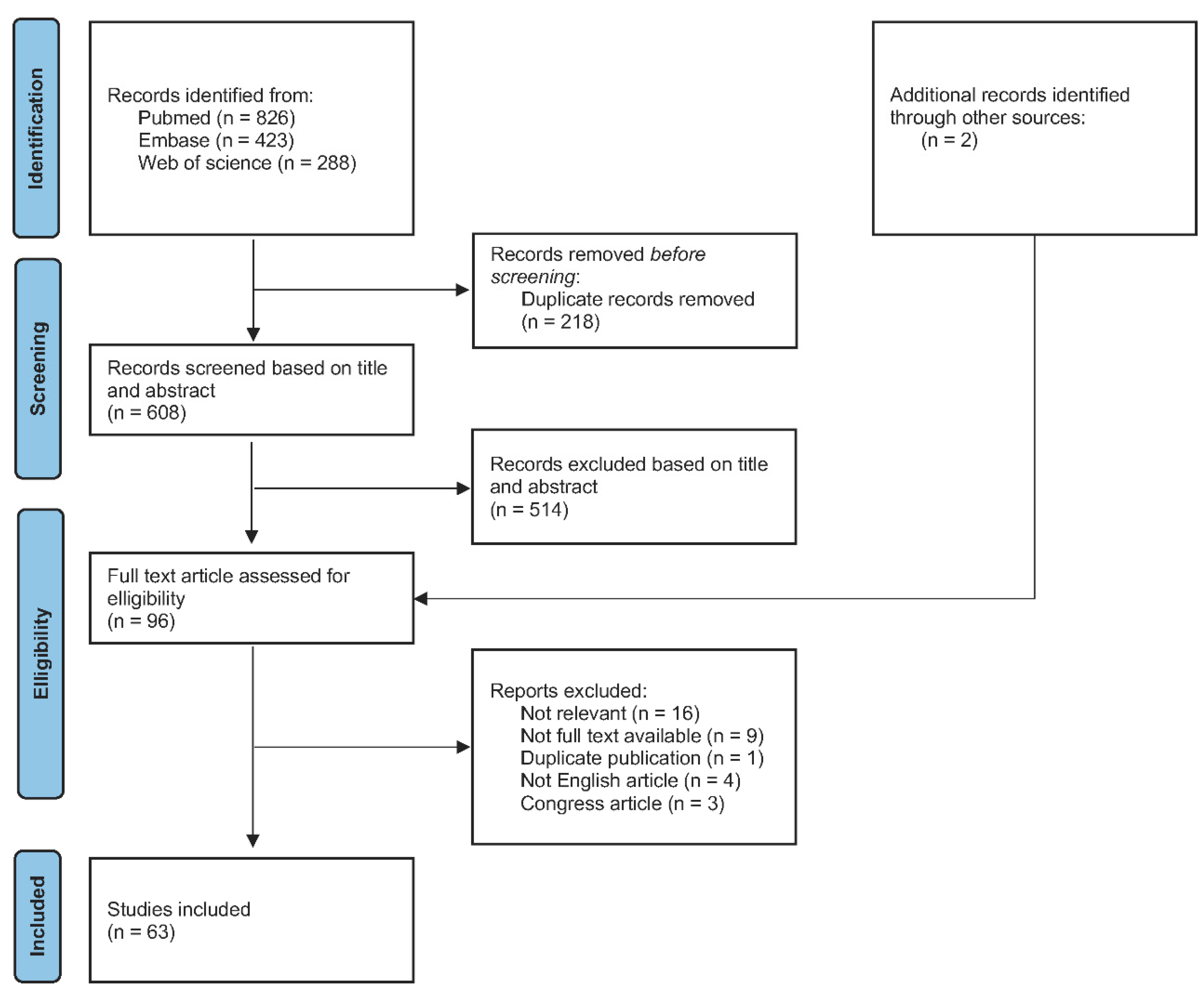{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Identification of Research Question
2.2. Selection of Publications
Screening and Eligibility of Publications
2.3. Determination of the Association between Periodontal Disease, Periodontal Pathogens and Pre-Eclampsia
2.3.1. Classification of Publications according to the Level of Evidence
2.3.2. Data Extraction from the Included Studies, GRADE Classification of Publications and Summary of Results
- -
- High: The real effect is similar to that of the estimated effect;
- -
- Moderate: The real effect is likely to be similar to the estimated effect, but it may be considerably different;
- -
- Low: The real effect may be considerably different from the estimated effect.;
- -
- Very low: The real effect is likely to be considerably different from the estimated effect.
3. Results
3.1. Selection of Publications Included
3.2. Included Publications Characteristics
3.3. Synthesis of the Results
4. Discussion
4.1. Periodontal Conditions during the Pregnancy
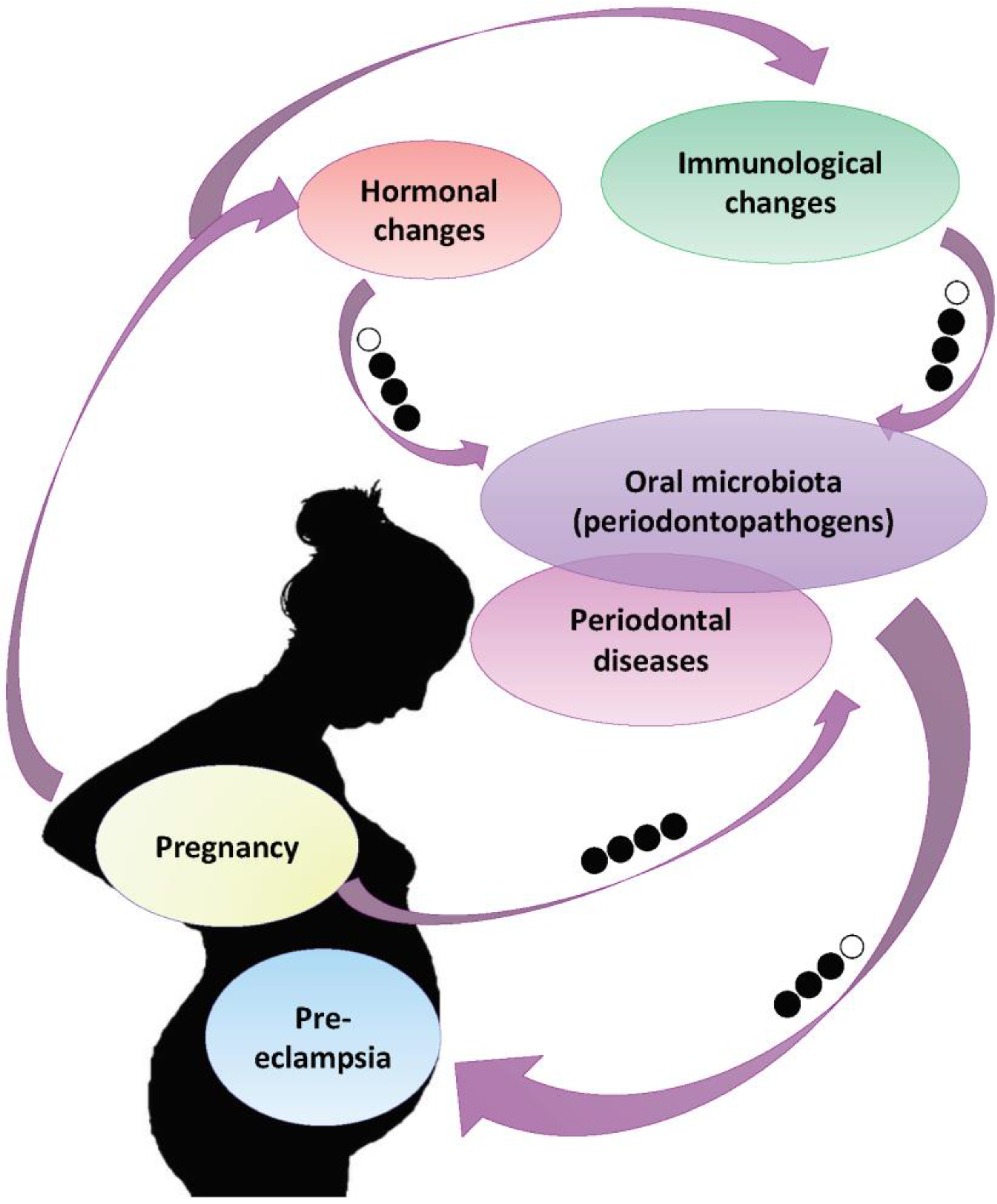
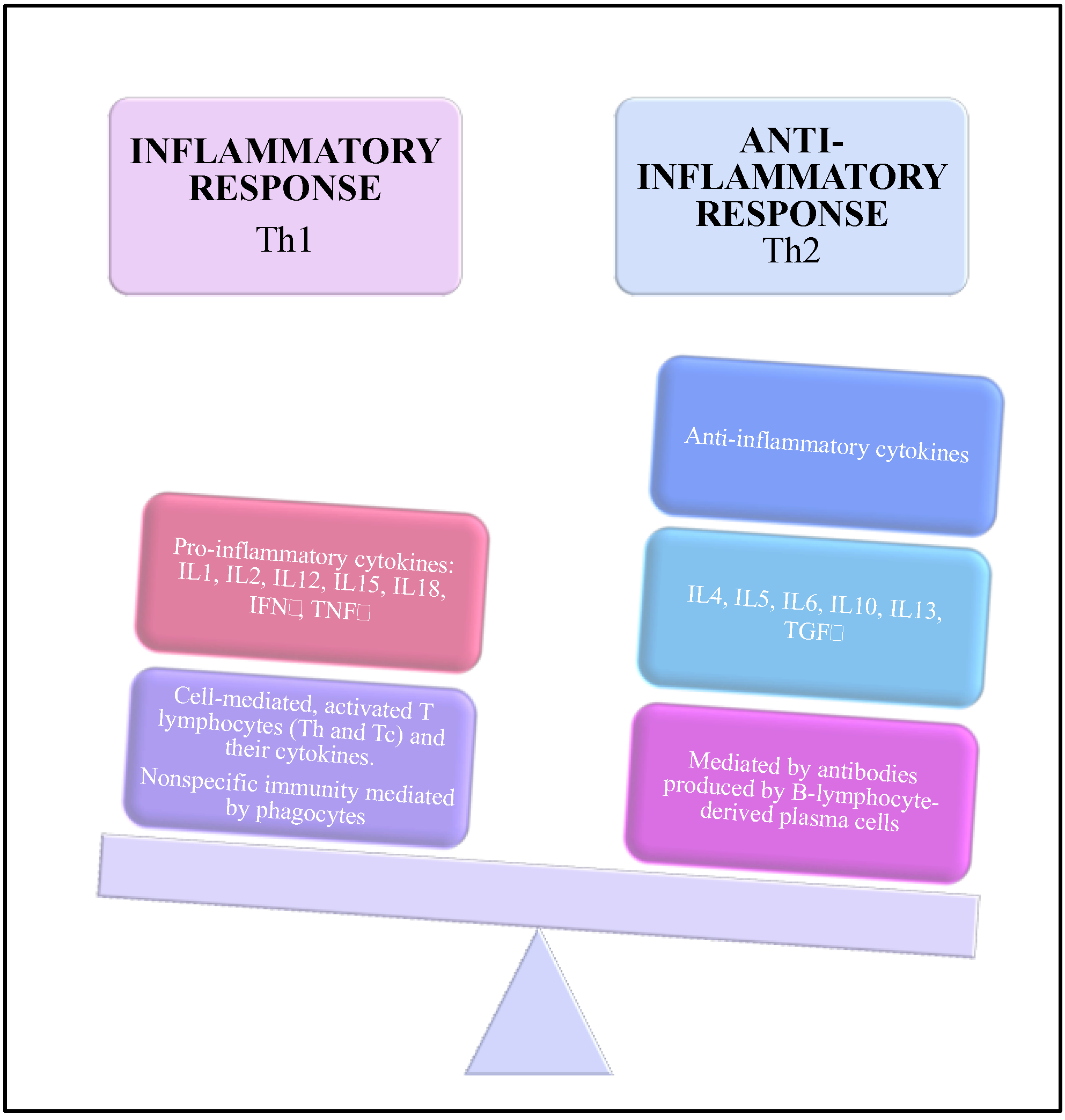
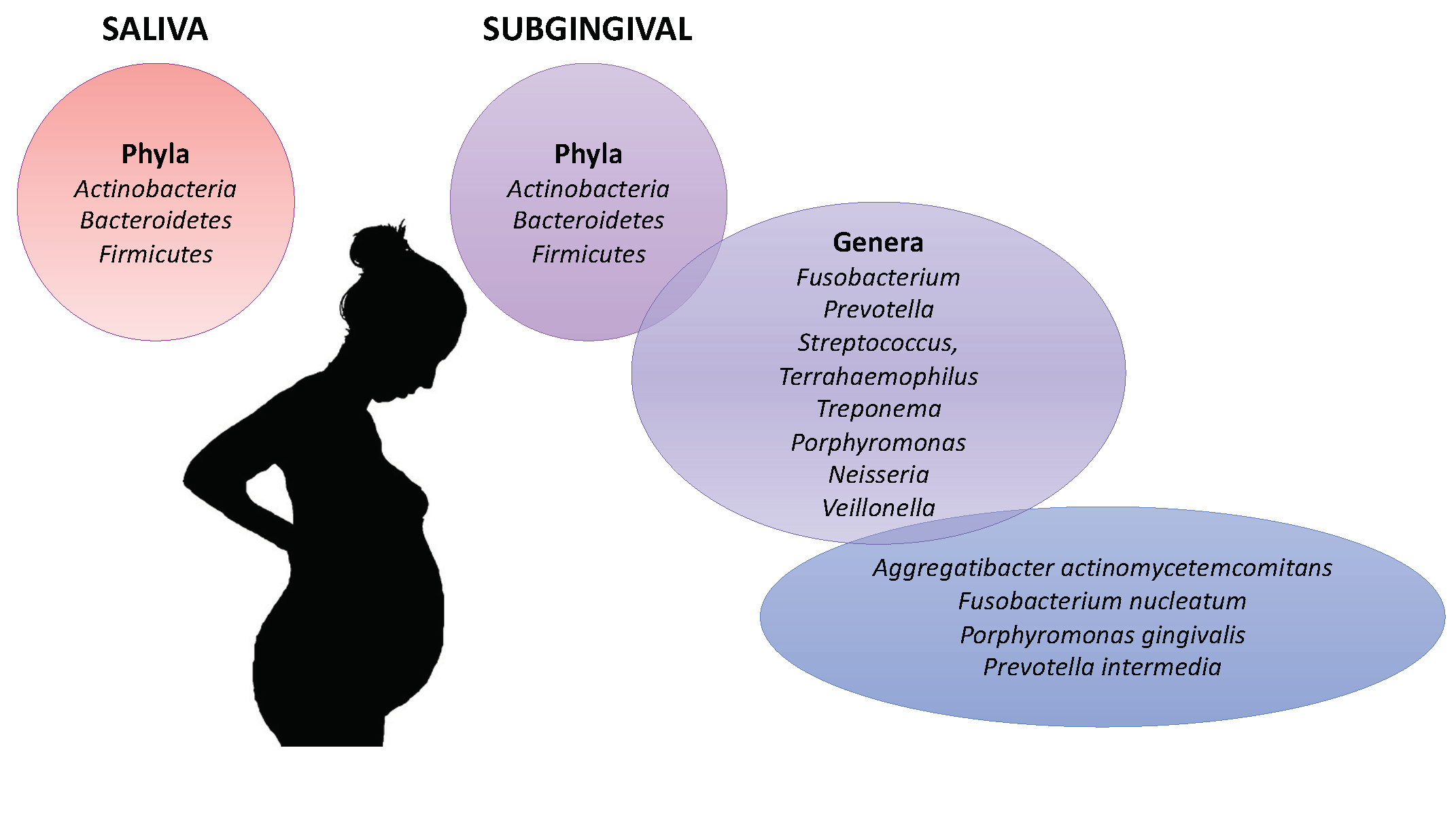
4.2. Hormonal Oral, Immunological and Oral Microbiota Changes and Their Impact on Periodontal Disease during the Pregnancy
4.3. Periodontal Pathogens and Pre-Eclampsia
4.4. Oral Lifestyles as an Actor to Reduce the Incidence of Periodontal Pathogens and Periodontal Disease
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Amir, M.; Brown, J.A.; Rager, S.L.; Sanidad, K.Z.; Ananthanarayanan, A.; Zeng, M.Y. Maternal Microbiome and Infections in Pregnancy. Microorganisms 2020, 8, 1996. [Google Scholar] [CrossRef] [PubMed]
- Edwards, S.M.; Cunningham, S.A.; Dunlop, A.L.; Corwin, E.J. The Maternal Gut Microbiome during Pregnancy. Mcn Am. J. Matern. Child. Nurs 2017, 42, 310–317. [Google Scholar] [CrossRef] [PubMed]
- Prince, A.L.; Chu, D.M.; Seferovic, M.D.; Antony, K.M.; Ma, J.; Aagaard, K.M. The Perinatal Microbiome and Pregnancy: Moving Beyond the Vaginal Microbiome. Cold Spring Harb. Perspect. Med. 2015, 5. [Google Scholar] [CrossRef]
- Magee, L.A.; von Dadelszen, P. State-of-the-Art Diagnosis and Treatment of Hypertension in Pregnancy. Mayo. Clin. Proc. 2018, 93, 1664–1677. [Google Scholar] [CrossRef] [Green Version]
- ACOG. Practice Bulletin No. 202: Gestational Hypertension and Preeclampsia. Obs. Gynecol. 2019, 133, 1. [Google Scholar] [CrossRef]
- Magee, L.A.; Sharma, S.; Nathan, H.L.; Adetoro, O.O.; Bellad, M.B.; Goudar, S.; Macuacua, S.E.; Mallapur, A.; Qureshi, R.; Sevene, E.; et al. The Incidence of Pregnancy Hypertension in India, Pakistan, Mozambique, and Nigeria: A Prospective Population-Level Analysis. PLoS Med. 2019, 16, e1002783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uzan, J.; Carbonnel, M.; Piconne, O.; Asmar, R.; Ayoubi, J.-M. Pre-Eclampsia: Pathophysiology, Diagnosis, and Management. Vasc. Health Risk Manag. 2011, 7, 467–474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braunthal, S.; Brateanu, A. Hypertension in Pregnancy: Pathophysiology and Treatment. Sage Open Med. 2019, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McElwain, C.J.; Tuboly, E.; McCarthy, F.P.; McCarthy, C.M. Mechanisms of Endothelial Dysfunction in Pre-Eclampsia and Gestational Diabetes Mellitus: Windows into Future Cardiometabolic Health? Front. Endocrinol. (Lausanne) 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Saadaoui, M.; Singh, P.; Al Khodor, S. Oral Microbiome and Pregnancy: A Bidirectional Relationship. J. Reprod. Immunol. 2021, 145, 103293. [Google Scholar] [CrossRef]
- Jepsen, S.; Caton, J.G.; Albandar, J.M.; Bissada, N.F.; Bouchard, P.; Cortellini, P.; Demirel, K.; de Sanctis, M.; Ercoli, C.; Fan, J.; et al. Periodontal Manifestations of Systemic Diseases and Developmental and Acquired Conditions: Consensus Report of Workgroup 3 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89 (Suppl. 1), S237–S248. [Google Scholar] [CrossRef]
- Bourgeois, D.; Inquimbert, C.; Ottolenghi, L.; Carrouel, F. Periodontal Pathogens as Risk Factors of Cardiovascular Diseases, Diabetes, Rheumatoid Arthritis, Cancer, and Chronic Obstructive Pulmonary Disease-Is There Cause for Consideration? Microorganisms 2019, 7, 424. [Google Scholar] [CrossRef] [Green Version]
- Gómez, L.A.; De Avila, J.; Castillo, D.M.; Montenegro, D.A.; Trujillo, T.G.; Suárez, L.J.; Lafaurie, G.I. Porphyromonas Gingivalis Placental Atopobiosis and Inflammatory Responses in Women With Adverse Pregnancy Outcomes. Front. Microbiol. 2020, 11, 591626. [Google Scholar] [CrossRef]
- Hajishengallis, G.; Darveau, R.P.; Curtis, M.A. The Keystone-Pathogen Hypothesis. Nat. Rev. Microbiol. 2012, 10, 717–725. [Google Scholar] [CrossRef]
- Radaic, A.; Kapila, Y.L. The Oralome and Its Dysbiosis: New Insights into Oral Microbiome-Host Interactions. Comput. Struct. Biotechnol. J. 2021, 19, 1335–1360. [Google Scholar] [CrossRef]
- Horliana, A.C.R.T.; Chambrone, L.; Foz, A.M.; Artese, H.P.C.; Rabelo, M.D.S.; Pannuti, C.M.; Romito, G.A. Dissemination of Periodontal Pathogens in the Bloodstream after Periodontal Procedures: A Systematic Review. PLoS ONE 2014, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sucharew, H.; Macaluso, M. Progress Notes: Methods for Research Evidence Synthesis: The Scoping Review Approach. J. Hosp. Med. 2019, 14, 416–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arksey, H.; O’Malley, L. Scoping Studies: Towards a Methodological Framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic Review or Scoping Review? Guidance for Authors When Choosing between a Systematic or Scoping Review Approach. BMC Med. Res. Methodol. 2018, 18. [Google Scholar] [CrossRef]
- Burns, P.B.; Rohrich, R.J.; Chung, K.C. The Levels of Evidence and Their Role in Evidence-Based Medicine. Plast. Reconstr. Surg. 2011, 128, 305–310. [Google Scholar] [CrossRef] [Green Version]
- What Is GRADE? | BMJ Best Practice. Available online: https://0-bestpractice-bmj-com.brum.beds.ac.uk/info/toolkit/learn-ebm/what-is-grade/ (accessed on 5 June 2021).
- Balshem, H.; Helfand, M.; Schünemann, H.J.; Oxman, A.D.; Kunz, R.; Brozek, J.; Vist, G.E.; Falck-Ytter, Y.; Meerpohl, J.; Norris, S.; et al. GRADE Guidelines: 3. Rating the Quality of Evidence. J. Clin. Epidemiol 2011, 64, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Figuero, E.; Carrillo-de-Albornoz, A.; Martín, C.; Tobías, A.; Herrera, D. Effect of Pregnancy on Gingival Inflammation in Systemically Healthy Women: A Systematic Review. J. Clin. Periodontol. 2013, 40, 457–473. [Google Scholar] [CrossRef] [PubMed]
- Cristi, M.C.; Gambacorta, V.; Di Giovanni, A.; Pindozzi, S.; Tassi, L.; Daniele, P.; Ricci, G. Increased Epulis Gravidarum Prevalence in Women with Both Nasal and Oral Symptoms—Openventio Publishers. Otolaryngol. Open J. 2019, 1, 18–21. [Google Scholar] [CrossRef]
- Figueiredo, M.G.O.P.; Takita, S.Y.; Dourado, B.M.R.; Mendes, H.D.S.; Terakado, E.O.; Nunes, H.R.D.C.; da Fonseca, C.R.B. Periodontal Disease: Repercussions in Pregnant Woman and Newborn Health—A Cohort Study. PLoS ONE 2019, 14. [Google Scholar] [CrossRef] [PubMed]
- Onigbinde, O.; Sorunke, M.; Braimoh, M.; Adeniyi, A. Periodontal Status and Some Variables among Pregnant Women in a Nigeria Tertiary Institution. Ann. Med. Health Sci. Res. 2014, 4, 852–857. [Google Scholar] [CrossRef] [Green Version]
- Wu, M.; Chen, S.-W.; Jiang, S.-Y. Relationship between Gingival Inflammation and Pregnancy. Mediat. Inflamm. 2015, 2015, 623427. [Google Scholar] [CrossRef]
- Preethi, R.; Ramamurthy, J. Pregnancy Gingivitis. Res. J. Pharm. Biol. Chem. Sci. 2015, 6, 7–10. [Google Scholar]
- Medina-Leyte, D.J.; Domínguez-Pérez, M.; Mercado, I.; Villarreal-Molina, M.T.; Jacobo-Albavera, L. Use of Human Umbilical Vein Endothelial Cells (HUVEC) as a Model to Study Cardiovascular Disease: A Review. Appl. Sci. 2020, 10, 938. [Google Scholar] [CrossRef] [Green Version]
- Yunita Sari, E.; Saddki, N.; Yusoff, A. Association between Perceived Oral Symptoms and Presence of Clinically Diagnosed Oral Diseases in a Sample of Pregnant Women in Malaysia. Int J. Env. Res. Public Health 2020, 17, 7337. [Google Scholar] [CrossRef]
- da Silva, F.G.; Pola, N.M.; Casarin, M.; Silva, C.F.E.; Muniz, F.W.M.G. Association between Clinical Measures of Gingival Inflammation and Obesity in Adults: Systematic Review and Meta-Analyses. Clin. Oral Investig. 2021. [Google Scholar] [CrossRef]
- Gonçalves, T.E.D.; Zimmermann, G.S.; Figueiredo, L.C.; Souza, M.D.C.; da Cruz, D.F.; Bastos, M.F.; da Silva, H.D.P.; Duarte, P.M. Local and Serum Levels of Adipokines in Patients with Obesity after Periodontal Therapy: One-Year Follow-Up. J. Clin. Periodontol. 2015, 42, 431–439. [Google Scholar] [CrossRef]
- Silva de Araujo Figueiredo, C.; Gonçalves Carvalho Rosalem, C.; Costa Cantanhede, A.L.; Abreu Fonseca Thomaz, É.B.; Fontoura Nogueira da Cruz, M.C. Systemic Alterations and Their Oral Manifestations in Pregnant Women. J. Obs. Gynaecol. Res. 2017, 43, 16–22. [Google Scholar] [CrossRef] [Green Version]
- Donos, N. The Periodontal Pocket. Periodontol. 2000 2018, 76, 7–15. [Google Scholar] [CrossRef]
- González-Jaranay, M.; Téllez, L.; Roa-López, A.; Gómez-Moreno, G.; Moreu, G. Periodontal Status during Pregnancy and Postpartum. PLoS ONE 2017, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foratori-Junior, G.A.; Jesuino, B.G.; Caracho, R.A.; Orenha, E.S.; Groppo, F.C.; Sales-Peres, S.H.d.C. Association between Excessive Maternal Weight, Periodontitis during the Third Trimester of Pregnancy, and Infants’ Health at Birth. J. Appl. Oral Sci. 2020, 28, e20190351. [Google Scholar] [CrossRef]
- Lain, K.Y.; Catalano, P.M. Metabolic Changes in Pregnancy. Clin. Obs. Gynecol. 2007, 50, 938–948. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Würtz, P.; Auro, K.; Mäkinen, V.-P.; Kangas, A.J.; Soininen, P.; Tiainen, M.; Tynkkynen, T.; Jokelainen, J.; Santalahti, K.; et al. Metabolic Profiling of Pregnancy: Cross-Sectional and Longitudinal Evidence. BMC Med. 2016, 14, 205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Machado, F.C.; Cesar, D.E.; Assis, A.V.D.A.; Diniz, C.G.; Ribeiro, R.A. Detection and Enumeration of Periodontopathogenic Bacteria in Subgingival Biofilm of Pregnant Women. Braz. Oral Res. 2012, 26, 443–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Souza Massoni, R.S.; Aranha, A.M.F.; Matos, F.Z.; Guedes, O.A.; Borges, Á.H.; Miotto, M.; Porto, A.N. Correlation of Periodontal and Microbiological Evaluations, with Serum Levels of Estradiol and Progesterone, during Different Trimesters of Gestation. Sci. Rep. 2019, 9, 11762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gürsoy, M.; Gürsoy, U.K.; Liukkonen, A.; Kauko, T.; Penkkala, S.; Könönen, E. Salivary Antimicrobial Defensins in Pregnancy. J. Clin. Periodontol. 2016, 43, 807–815. [Google Scholar] [CrossRef] [PubMed]
- Preshaw, P.M. Oral Contraceptives and the Periodontium. Periodontology 2013, 61, 125–159. [Google Scholar] [CrossRef] [PubMed]
- Tang, Z.-R.; Zhang, R.; Lian, Z.-X.; Deng, S.-L.; Yu, K. Estrogen-Receptor Expression and Function in Female Reproductive Disease. Cells 2019, 8, 1123. [Google Scholar] [CrossRef] [Green Version]
- Zheng, Y.; Murphy, L.C. Regulation of Steroid Hormone Receptors and Coregulators during the Cell Cycle Highlights Potential Novel Function in Addition to Roles as Transcription Factors. Nucl. Recept. Signal. 2016, 14, e001. [Google Scholar] [CrossRef] [Green Version]
- Wu, M.; Chen, S.-W.; Su, W.-L.; Zhu, H.-Y.; Ouyang, S.-Y.; Cao, Y.-T.; Jiang, S.-Y. Sex Hormones Enhance Gingival Inflammation without Affecting IL-1β and TNF-α in Periodontally Healthy Women during Pregnancy. Mediat. Inflamm. 2016, 2016. [Google Scholar] [CrossRef] [Green Version]
- Abu-Raya, B.; Michalski, C.; Sadarangani, M.; Lavoie, P.M. Maternal Immunological Adaptation during Normal Pregnancy. Front. Immunol 2020, 11, 575197. [Google Scholar] [CrossRef] [PubMed]
- Markou, E.; Eleana, B.; Lazaros, T.; Antonios, K. The Influence of Sex Steroid Hormones on Gingiva of Women. Open Dent. J. 2009, 3, 114–119. [Google Scholar] [CrossRef] [Green Version]
- Carbonne, B.; Dallot, E.; Haddad, B.; Ferré, F.; Cabrol, D. Effects of Progesterone on Prostaglandin E(2)-Induced Changes in Glycosaminoglycan Synthesis by Human Cervical Fibroblasts in Culture. Mol. Hum. Reprod. 2000, 6, 661–664. [Google Scholar] [CrossRef] [Green Version]
- Jafri, Z.; Bhardwaj, A.; Sawai, M.; Sultan, N. Influence of Female Sex Hormones on Periodontium: A Case Series. J. Nat. Sci. Biol. Med. 2015, 6, S146–149. [Google Scholar] [CrossRef] [Green Version]
- Mascarenhas, P.; Gapski, R.; Al-Shammari, K.; Wang, H.-L. Influence of Sex Hormones on the Periodontium. J. Clin. Periodontol 2003, 30, 671–681. [Google Scholar] [CrossRef]
- Mor, G.; Aldo, P.; Alvero, A.B. The Unique Immunological and Microbial Aspects of Pregnancy. Nat. Rev. Immunol. 2017, 17, 469–482. [Google Scholar] [CrossRef]
- Challis, J.R.; Lockwood, C.J.; Myatt, L.; Norman, J.E.; Strauss, J.F.; Petraglia, F. Inflammation and Pregnancy. Reprod. Sci. 2009, 16, 206–215. [Google Scholar] [CrossRef]
- Yang, I.; Knight, A.K.; Dunlop, A.L.; Corwin, E.J. Characterizing the Subgingival Microbiome of Pregnant African American Women. J. Obs. Gynecol Neonatal. Nurs. 2019, 48, 140–152. [Google Scholar] [CrossRef]
- Zoller, A.L.; Kersh, G.J. Estrogen Induces Thymic Atrophy by Eliminating Early Thymic Progenitors and Inhibiting Proliferation of Beta-Selected Thymocytes. J. Immunol 2006, 176, 7371–7378. [Google Scholar] [CrossRef] [PubMed]
- Kanda, N.; Tamaki, K. Estrogen Enhances Immunoglobulin Production by Human PBMCs. J. Allergy Clin. Immunol. 1999, 103, 282–288. [Google Scholar] [CrossRef]
- Gürsoy, M.; Zeidán-Chuliá, F.; Könönen, E.; Moreira, J.C.F.; Liukkonen, J.; Sorsa, T.; Gürsoy, U.K. Pregnancy-Induced Gingivitis and OMICS in Dentistry: In Silico Modeling and in Vivo Prospective Validation of Estradiol-Modulated Inflammatory Biomarkers. OMICS 2014, 18, 582–590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borgo, P.V.; Rodrigues, V.A.A.; Feitosa, A.C.R.; Xavier, K.C.B.; Avila-Campos, M.J. Association between Periodontal Condition and Subgingival Microbiota in Women during Pregnancy: A Longitudinal Study. J. Appl. Oral Sci. 2014, 22, 528–533. [Google Scholar] [CrossRef]
- Nuriel-Ohayon, M.; Neuman, H.; Koren, O. Microbial Changes during Pregnancy, Birth, and Infancy. Front. Microbiol. 2016, 7, 1031. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujiwara, N.; Tsuruda, K.; Iwamoto, Y.; Kato, F.; Odaki, T.; Yamane, N.; Hori, Y.; Harashima, Y.; Sakoda, A.; Tagaya, A.; et al. Significant Increase of Oral Bacteria in the Early Pregnancy Period in Japanese Women. J. Investig Clin. Dent. 2017, 8. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.; Jiang, W.; Hu, X.; Gao, L.; Ai, D.; Pan, H.; Niu, C.; Yuan, K.; Zhou, X.; Xu, C.; et al. Ecological Shifts of Supragingival Microbiota in Association with Pregnancy. Front. Cell Infect. Microbiol 2018, 8. [Google Scholar] [CrossRef]
- Balan, P.; Chong, Y.S.; Umashankar, S.; Swarup, S.; Loke, W.M.; Lopez, V.; He, H.G.; Seneviratne, C.J. Keystone Species in Pregnancy Gingivitis: A Snapshot of Oral Microbiome during Pregnancy and Postpartum Period. Front. Microbiol. 2018, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DiGiulio, D.B.; Callahan, B.J.; McMurdie, P.J.; Costello, E.K.; Lyell, D.J.; Robaczewska, A.; Sun, C.L.; Goltsman, D.S.A.; Wong, R.J.; Shaw, G.; et al. Temporal and Spatial Variation of the Human Microbiota during Pregnancy. Proc. Natl. Acad. Sci. USA 2015, 112, 11060–11065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cobb, C.M.; Kelly, P.J.; Williams, K.B.; Babbar, S.; Angolkar, M.; Derman, R.J. The Oral Microbiome and Adverse Pregnancy Outcomes. Int. J. Womens Health 2017, 9, 551–559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tellapragada, C.; Eshwara, V.K.; Acharya, S.; Bhat, P.; Kamath, A.; Vishwanath, S.; Mukhopadhyay, C. Prevalence of Clinical Periodontitis and Putative Periodontal Pathogens among South Indian Pregnant Women. Int. J. Microbiol. 2014, 2014, 420149. [Google Scholar] [CrossRef] [Green Version]
- Abusleme, L.; Dupuy, A.K.; Dutzan, N.; Silva, N.; Burleson, J.A.; Strausbaugh, L.D.; Gamonal, J.; Diaz, P.I. The Subgingival Microbiome in Health and Periodontitis and Its Relationship with Community Biomass and Inflammation. ISME J. 2013, 7, 1016–1025. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, B.-J.; Chen, Y.-J.; Yu, L.; Wu, B. Periodontal Disease and Risk of Preeclampsia: A Meta-Analysis of Observational Studies. PLoS ONE 2013, 8, e70901. [Google Scholar] [CrossRef]
- Fischer, L.A.; Demerath, E.; Bittner-Eddy, P.; Costalonga, M. Placental Colonization with Periodontal Pathogens: The Potential Missing Link. Am. J. Obs. Gynecol. 2019, 221, 383–392.e3. [Google Scholar] [CrossRef]
- Konopka, T.; Zakrzewska, A. Periodontitis and Risk for Preeclampsia - a Systematic Review. Ginekol. Pol. 2020, 91, 158–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daalderop, L.A.; Wieland, B.V.; Tomsin, K.; Reyes, L.; Kramer, B.W.; Vanterpool, S.F.; Been, J.V. Periodontal Disease and Pregnancy Outcomes: Overview of Systematic Reviews. JDR Clin. Trans. Res. 2018, 3, 10–27. [Google Scholar] [CrossRef] [PubMed]
- Matevosyan, N.R. Periodontal Disease and Perinatal Outcomes. Arch. Gynecol Obs. 2011, 283, 675–686. [Google Scholar] [CrossRef]
- Sgolastra, F.; Petrucci, A.; Severino, M.; Gatto, R.; Monaco, A. Relationship between Periodontitis and Pre-Eclampsia: A Meta-Analysis. PLoS ONE 2013, 8, e71387. [Google Scholar] [CrossRef] [Green Version]
- Desai, K.; Desai, P.; Duseja, S.; Kumar, S.; Mahendra, J.; Duseja, S. Significance of Maternal Periodontal Health in Preeclampsia. J. Int Soc. Prev. Community Dent. 2015, 5, 103–107. [Google Scholar] [CrossRef] [Green Version]
- Huang, X.; Wang, J.; Liu, J.; Hua, L.; Zhang, D.; Hu, T.; Ge, Z.-L. Maternal Periodontal Disease and Risk of Preeclampsia: A Meta-Analysis. J. Huazhong Univ Sci Technol. Med. Sci 2014, 34, 729–735. [Google Scholar] [CrossRef] [PubMed]
- Popova, C.; Dosseva-Panova, V.; Panov, V. Microbiology of Periodontal Diseases. A Review. Biotechnol. Biotechnol. Equip. 2013, 27, 3754–3759. [Google Scholar] [CrossRef]
- Fox, R.; Kitt, J.; Leeson, P.; Aye, C.Y.L.; Lewandowski, A.J. Preeclampsia: Risk Factors, Diagnosis, Management, and the Cardiovascular Impact on the Offspring. J. Clin. Med. 2019, 8, 1625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beckers, K.F.; Sones, J.L. Maternal Microbiome and the Hypertensive Disorder of Pregnancy, Preeclampsia. Am. J. Physiol. Heart Circ. Physiol. 2020, 318, H1–H10. [Google Scholar] [CrossRef] [PubMed]
- Aagaard, K.; Ma, J.; Antony, K.M.; Ganu, R.; Petrosino, J.; Versalovic, J. The Placenta Harbors a Unique Microbiome. Sci. Transl. Med. 2014, 6, 237ra65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amarasekara, R.; Jayasekara, R.W.; Senanayake, H.; Dissanayake, V.H.W. Microbiome of the Placenta in Pre-Eclampsia Supports the Role of Bacteria in the Multifactorial Cause of Pre-Eclampsia. J. Obs. Gynaecol. Res. 2015, 41, 662–669. [Google Scholar] [CrossRef]
- Barak, S.; Oettinger-Barak, O.; Machtei, E.E.; Sprecher, H.; Ohel, G. Evidence of Periopathogenic Microorganisms in Placentas of Women with Preeclampsia. J. Periodontol. 2007, 78, 670–676. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.W. Oral Health and Adverse Pregnancy Outcomes—What’s Next? J. Dent. Res. 2011, 90, 289–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrukhov, O.; Ulm, C.; Reischl, H.; Nguyen, P.Q.; Matejka, M.; Rausch-Fan, X. Serum Cytokine Levels in Periodontitis Patients in Relation to the Bacterial Load. J. Periodontol. 2011, 82, 885–892. [Google Scholar] [CrossRef]
- Parthiban, P.S.; Mahendra, J.; Logaranjani, A.; Shanmugam, S.; Balakrishnan, A.; Junaid, M.; Namasivayam, A. Association between Specific Periodontal Pathogens, Toll-like Receptor-4, and Nuclear Factor-ΚB Expression in Placental Tissues of Pre-Eclamptic Women with Periodontitis. J. Investig. Clin. Dent. 2018, 9. [Google Scholar] [CrossRef] [PubMed]
- Cleys, E.R.; Halleran, J.L.; Enriquez, V.A.; da Silveira, J.C.; West, R.C.; Winger, Q.A.; Anthony, R.V.; Bruemmer, J.E.; Clay, C.M.; Bouma, G.J. Androgen Receptor and Histone Lysine Demethylases in Ovine Placenta. PLoS ONE 2015, 10, e0117472. [Google Scholar] [CrossRef] [PubMed]
- Soory, M. Bacterial Steroidogenesis by Periodontal Pathogens and the Effect of Bacterial Enzymes on Steroid Conversions by Human Gingival Fibroblasts in Culture. J. Periodontal Res. 1995, 30, 124–131. [Google Scholar] [CrossRef]
- Khong, Y.; Brosens, I. Defective Deep Placentation. Best Pr. Res. Clin. Obs. Gynaecol. 2011, 25, 301–311. [Google Scholar] [CrossRef]
- Brosens, I.; Pijnenborg, R.; Vercruysse, L.; Romero, R. The “Great Obstetrical Syndromes” Are Associated with Disorders of Deep Placentation. Am. J. Obs. Gynecol 2011, 204, 193–201. [Google Scholar] [CrossRef] [Green Version]
- Vigliani, M.B.; Bakardjiev, A.I. Intracellular Organisms as Placental Invaders. Fetal. Matern. Med. Rev. 2014, 25, 332–338. [Google Scholar] [CrossRef] [Green Version]
- Chaparro, A.; Blanlot, C.; Ramírez, V.; Sanz, A.; Quintero, A.; Inostroza, C.; Bittner, M.; Navarro, M.; Illanes, S.E. Porphyromonas Gingivalis, Treponema Denticola and Toll-like Receptor 2 Are Associated with Hypertensive Disorders in Placental Tissue: A Case-Control Study. J. Periodontal Res. 2013, 48, 802–809. [Google Scholar] [CrossRef]
- Swati, P.; Ambika Devi, K.; Thomas, B.; Vahab, S.A.; Kapaettu, S.; Kushtagi, P. Simultaneous Detection of Periodontal Pathogens in Subgingival Plaque and Placenta of Women with Hypertension in Pregnancy. Arch. Gynecol Obs. 2012, 285, 613–619. [Google Scholar] [CrossRef]
- Vanterpool, S.F.; Been, J.V.; Houben, M.L.; Nikkels, P.G.J.; De Krijger, R.R.; Zimmermann, L.J.I.; Kramer, B.W.; Progulske-Fox, A.; Reyes, L. Porphyromonas Gingivalis within Placental Villous Mesenchyme and Umbilical Cord Stroma Is Associated with Adverse Pregnancy Outcome. PLoS ONE 2016, 11, e0146157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reyes, L.; Phillips, P.; Wolfe, B.; Golos, T.G.; Walkenhorst, M.; Progulske-Fox, A.; Brown, M. Porphyromonas Gingivalis and Adverse Pregnancy Outcome. J. Oral Microbiol. 2018, 10, 1374153. [Google Scholar] [CrossRef] [Green Version]
- Golic, M.; Haase, N.; Herse, F.; Wehner, A.; Vercruysse, L.; Pijnenborg, R.; Balogh, A.; Saether, P.C.; Dissen, E.; Luft, F.C.; et al. Natural Killer Cell Reduction and Uteroplacental Vasculopathy. Hypertension 2016, 68, 964–973. [Google Scholar] [CrossRef] [Green Version]
- Tavarna, T.; Phillips, P.L.; Wu, X.-J.; Reyes, L. Fetal Growth Restriction Is a Host Specific Response to Infection with an Impaired Spiral Artery Remodeling-Inducing Strain of Porphyromonas Gingivalis. Sci. Rep. 2020, 10, 14606. [Google Scholar] [CrossRef]
- Axelsson, P.; Nyström, B.; Lindhe, J. The Long-Term Effect of a Plaque Control Program on Tooth Mortality, Caries and Periodontal Disease in Adults. Results after 30 Years of Maintenance. J. Clin. Periodontol. 2004, 31, 749–757. [Google Scholar] [CrossRef]
- Chapple, I.L.C.; Van der Weijden, F.; Doerfer, C.; Herrera, D.; Shapira, L.; Polak, D.; Madianos, P.; Louropoulou, A.; Machtei, E.; Donos, N.; et al. Primary Prevention of Periodontitis: Managing Gingivitis. J. Clin. Periodontol. 2015, 42 (Suppl. 16), S71–76. [Google Scholar] [CrossRef] [Green Version]
- Haffajee, A.D.; Thompson, M.; Torresyap, G.; Guerrero, D.; Socransky, S.S. Efficacy of Manual and Powered Toothbrushes (I). Effect on Clinical Parameters. J. Clin. Periodontol. 2001, 28, 937–946. [Google Scholar] [CrossRef] [PubMed]
- Dörfer, C.E.; Staehle, H.J.; Wolff, D. Three-Year Randomized Study of Manual and Power Toothbrush Effects on Pre-Existing Gingival Recession. J. Clin. Periodontol. 2016, 43, 512–519. [Google Scholar] [CrossRef] [PubMed]
- Pitchika, V.; Pink, C.; Völzke, H.; Welk, A.; Kocher, T.; Holtfreter, B. Long-Term Impact of Powered Toothbrush on Oral Health: 11-Year Cohort Study. J. Clin. Periodontol. 2019, 46, 713–722. [Google Scholar] [CrossRef] [PubMed]
- Preda, C.; Butera, A.; Pelle, S.; Pautasso, E.; Chiesa, A.; Esposito, F.; Oldoini, G.; Scribante, A.; Genovesi, A.M.; Cosola, S. The Efficacy of Powered Oscillating Heads vs. Powered Sonic Action Heads Toothbrushes to Maintain Periodontal and Peri-Implant Health: A Narrative Review. Int. J. Env. Res. Public Health 2021, 18, 1468. [Google Scholar] [CrossRef]
- Carrouel, F.; Viennot, S.; Santamaria, J.; Veber, P.; Bourgeois, D. Quantitative Molecular Detection of 19 Major Pathogens in the Interdental Biofilm of Periodontally Healthy Young Adults. Front. Microbiol. 2016, 7. [Google Scholar] [CrossRef]
- Bourgeois, D.; David, A.; Inquimbert, C.; Tramini, P.; Molinari, N.; Carrouel, F. Quantification of Carious Pathogens in the Interdental Microbiota of Young Caries-Free Adults. PLoS ONE 2017, 12, e0185804. [Google Scholar] [CrossRef] [Green Version]
- Mwatha, A.; Olson, M.; Souza, S.; Ward, M.; Jenkins, W.; Amini, P.; Gallob, J.; Fafard, T. Gingival Health and Plaque Regrowth Response Following a Four-Week Interdental Hygiene Intervention. J. Clin. Dent. 2017, 28, A36–A44. [Google Scholar] [PubMed]
- Graziani, F.; Palazzolo, A.; Gennai, S.; Karapetsa, D.; Giuca, M.R.; Cei, S.; Filice, N.; Petrini, M.; Nisi, M. Interdental Plaque Reduction after Use of Different Devices in Young Subjects with Intact Papilla: A Randomized Clinical Trial. Int. J. Dent. Hyg. 2018, 16, 389–396. [Google Scholar] [CrossRef] [PubMed]
- Bourgeois, D.; Bravo, M.; Llodra, J.-C.; Inquimbert, C.; Viennot, S.; Dussart, C.; Carrouel, F. Calibrated Interdental Brushing for the Prevention of Periodontal Pathogens Infection in Young Adults—A Randomized Controlled Clinical Trial. Sci. Rep. 2019, 9, 15127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bourgeois, D.; Saliasi, I.; Llodra, J.C.; Bravo, M.; Viennot, S.; Carrouel, F. Efficacy of Interdental Calibrated Brushes on Bleeding Reduction in Adults: A 3-Month Randomized Controlled Clinical Trial. Eur. J. Oral Sci. 2016, 124, 566–571. [Google Scholar] [CrossRef] [PubMed]
- Kotsakis, G.A.; Lian, Q.; Ioannou, A.L.; Michalowicz, B.S.; John, M.T.; Chu, H. A Network Meta-Analysis of Interproximal Oral Hygiene Methods in the Reduction of Clinical Indices of Inflammation. J. Periodontol. 2018, 89, 558–570. [Google Scholar] [CrossRef] [PubMed]
- Sälzer, S.; Slot, D.E.; Van der Weijden, F.A.; Dörfer, C.E. Efficacy of Inter-Dental Mechanical Plaque Control in Managing Gingivitis—A Meta-Review. J. Clin. Periodontol. 2015, 42 (Suppl. 16), S92–S105. [Google Scholar] [CrossRef] [Green Version]
- Carrouel, F.; Viennot, S.; Ottolenghi, L.; Gaillard, C.; Bourgeois, D. Nanoparticles as Anti-Microbial, Anti-Inflammatory, and Remineralizing Agents in Oral Care Cosmetics: A Review of the Current Situation. Nanomaterials (Basel) 2020, 10, 140. [Google Scholar] [CrossRef] [Green Version]
- Hosadurga, R.; Boloor, V.A.; Rao, S.N.; MeghRani, N. Effectiveness of Two Different Herbal Toothpaste Formulations in the Reduction of Plaque and Gingival Inflammation in Patients with Established Gingivitis - A Randomized Controlled Trial. J. Tradit. Complement. Med. 2018, 8, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Butera, A.; Gallo, S.; Maiorani, C.; Molino, D.; Chiesa, A.; Preda, C.; Esposito, F.; Scribante, A. Probiotic Alternative to Chlorhexidine in Periodontal Therapy: Evaluation of Clinical and Microbiological Parameters. Microorganisms 2020, 9, 69. [Google Scholar] [CrossRef]
- Martinon, P.; Fraticelli, L.; Giboreau, A.; Dussart, C.; Bourgeois, D.; Carrouel, F. Nutrition as a Key Modifiable Factor for Periodontitis and Main Chronic Diseases. J. Clin. Med. 2021, 10, 197. [Google Scholar] [CrossRef] [PubMed]
- Isolauri, E.; Kirjavainen, P.V.; Salminen, S. Probiotics: A Role in the Treatment of Intestinal Infection and Inflammation? Gut 2002, 50 (Suppl. 3), III54–III59. [Google Scholar] [CrossRef] [PubMed]
- Matsubara, V.H.; Bandara, H.M.H.N.; Ishikawa, K.H.; Mayer, M.P.A.; Samaranayake, L.P. The Role of Probiotic Bacteria in Managing Periodontal Disease: A Systematic Review. Expert Rev. Anti Infect. 2016, 14, 643–655. [Google Scholar] [CrossRef] [PubMed]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gare, J.; Kanoute, A.; Meda, N.; Viennot, S.; Bourgeois, D.; Carrouel, F. Periodontal Conditions and Pathogens Associated with Pre-Eclampsia: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 7194. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137194
Gare J, Kanoute A, Meda N, Viennot S, Bourgeois D, Carrouel F. Periodontal Conditions and Pathogens Associated with Pre-Eclampsia: A Scoping Review. International Journal of Environmental Research and Public Health. 2021; 18(13):7194. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137194
Chicago/Turabian StyleGare, Jocelyne, Aida Kanoute, Nicolas Meda, Stephane Viennot, Denis Bourgeois, and Florence Carrouel. 2021. "Periodontal Conditions and Pathogens Associated with Pre-Eclampsia: A Scoping Review" International Journal of Environmental Research and Public Health 18, no. 13: 7194. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137194