
Do Age-Friendly Rural Communities Affect Quality of Life? A Comparison of Perceptions from Middle-Aged and Older Adults in China

Abstract
:1. Introduction
2. Literature Review
3. Research Methods
4. Results
4.1. The Demographic Characteristics of Middle-Aged and Older Adults
4.2. Reliability Analysis
4.3. Independent Sample t-Test
4.4. Multiple Regression
5. Discussion
6. Recommendations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Bureau of Statistics. In 2019 China Statistical Yearbook; 2020. Available online: http://www.stats.gov.cn/tjsj/ndsj/2019/indexch.htm (accessed on 6 March 2020).
- Ryoo, Y.; Lee, J. A Social Service Strategy for a Low Birth Rate and an Aged Society. Asian J. Hum. Serv. 2015, 9, 17–32. [Google Scholar] [CrossRef] [Green Version]
- Yi, F.; Liu, C.; Xu, Z. Identifying the effects of migration on parental health: Evidence from left-behind elders in China. China Econ. Rev. 2019, 54, 218–236. [Google Scholar] [CrossRef]
- State Council. The State Plans for A New Type of Urbanization (2014–2020). 2014. Available online: http://www.gov.cn/gongbao/content/2014/content_2644805.html (accessed on 24 April 2020).
- Ministry of Civil Affairs. 2018 Statistical Bulletin on Development of Civil Affairs. 2019. Available online: http://images3.mca.gov.cn/www2017/file/201908/1565920301578.pdf (accessed on 17 March 2020).
- State Council. Suggestions on Accelerating the Development of the Elderly Care Service Indus-try. 2013. Available online: http://www.gov.cn/xxgk/pub/govpublic/mrlm/201309/t20130913_66389.html (accessed on 17 March 2020).
- State Council Strategic Plan for Rural Revitalization 2018–2022. 2018. Available online: http://www.farmer.com.cn/zt2018/zxgh/tt/201811/t20181109_1415642.html (accessed on 17 March 2020).
- Neville, S.; Napier, S.; Adams, J.; Wham, C.; Jackson, D. An integrative review of the factors related to building age-friendly rural communities. J. Clin. Nurs. 2016, 25, 2402–2412. [Google Scholar] [CrossRef]
- National Aging Population Office of China. Guidelines on Promoting Aging-Friendly Environment. 2016. Available online: http://www.gov.cn/xinwen/2016-11/25/content_5137617.html (accessed on 5 January 2020).
- Hancock, S.; Winterton, R.; Wilding, C.; Blackberry, I. Understanding ageing well in Australian rural and regional settings: Applying an age-friendly lens. Aust. J. Rural. Heal. 2019, 27, 298–303. [Google Scholar] [CrossRef]
- Menec, V.H.; Hutton, L.; Newall, N.E.G.; Nowicki, S.; Spina, J.; Veselyuk, D. How ‘age-friendly’ are rural communities and what community characteristics are related to age-friendliness? The case of rural Manitoba, Canada. Ageing Soc. 2015, 35, 203–223. [Google Scholar] [CrossRef]
- National Bureau of Statistics. Sixth Nationwide Population Census. 2011. Available online: http://www.stats.gov.cn/tjsj/tjgb/rkpcgb/qgrkpcgb/201104/t20110428_30327.html (accessed on 16 March 2020).
- John, D.H.; Gunter, K. Engage in community: Using mixed methods to mobilize older people to elucidate the age-friendly at-tributes of urban and rural places. J. Appl. Gerontol. 2016, 35, 1095–1120. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Global Age-Friendly Cities: A Guide; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Ball, M.S.; Lawler, K. Changing practice and policy to move to scale: A framework for AFC across the United States. J. Aging Soc. Policy 2014, 26, 19–32. [Google Scholar] [CrossRef] [PubMed]
- Brooks-Cleator, L.A.; Giles, A.R.; Flaherty, M. Community-level factors that contribute to First Nations and Inuit older adults feeling supported to age well in a Canadian city. J. Aging Stud. 2019, 48, 50–59. [Google Scholar] [CrossRef]
- Gibney, S.; Zhang, M.; Brennan, C. Age-friendly environments and psychosocial wellbeing: A study of older urban residents in Ireland. Aging Ment. Health 2020, 24, 2022–2033. [Google Scholar] [CrossRef]
- Chui, C.H.-K.; Chan, O.F.; Tang, J.Y.M.; Lum, T.Y.S. Fostering Civic Awareness and Participation Among Older Adults in Hong Kong: An Empowerment-Based Participatory Photo-Voice Training Model. J. Appl. Gerontol. 2019, 39, 1008–1015. [Google Scholar] [CrossRef]
- Aird, R.L.; Buys, L. Active Aging: Exploration into Self-Ratings of “Being Active,” Out-of-Home Physical Activity, and Participation among Older Australian Adults Living in Four Different Settings. J. Aging Res. 2015, 2015, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Schorr, A.V.; Khalaila, R. Aging in place and quality of life among the elderly in Europe: A moderated mediation model. Arch. Gerontol. Geriatr. 2018, 77, 196–204. [Google Scholar] [CrossRef]
- Cao, Q.; Dabelko-Schoeny, H.I.; White, K.M.; Choi, M. AFC and perceived disconnectedness: The role of built environment and social engagement. J. Aging Health 2019. [Google Scholar] [CrossRef]
- Wilson, N.; Couper, I.; de Vries, E.; Reid, S.; Fish, T.; Marais, B. A critical review of interventions to redress the inequitable distribution of healthcare professionals to rural and remote areas. Rural Remote Health 2009, 9, 1–21. [Google Scholar] [CrossRef]
- Keating, N.; Eales, J.; Phillips, J.E. Age-friendly rural communities: Conceptualizing “best-fit”. Can. J. Aging 2013, 32, 319–332. [Google Scholar] [CrossRef]
- Brooks-Cleator, L.A.; Giles, A.R. Physical Activity Policy for Older Adults in the Northwest Territories, Canada: Gaps and Opportunities for Gains. Arctic 2016, 69, 169–176. [Google Scholar] [CrossRef]
- Lamanna, M.; Klinger, C.A.; Liu, A.; Mirza, R.M. The Association between Public Transportation and Social Isolation in Older Adults: A Scoping Review of the Literature. Can. J. Aging Rev. Can. Vieil. 2019, 39, 393–405. [Google Scholar] [CrossRef] [PubMed]
- Winterton, R. Organizational responsibility for age-friendly social participation: Views of Australian rural community stake-holders. J. Aging Soc. Policy 2016, 28, 261–276. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Measuring the Age-Friendliness of Cities: A Guide to Using Core Indicators; WHO: Geneva, Switzerland, 2015; ISBN 9789241509695. [Google Scholar]
- Bond, M.; Brown, J.R.; Wood, J. Adapting to challenge: Examining older adult transportation in rural communities. Case Stud. Transp. Policy 2017, 5, 707–715. [Google Scholar] [CrossRef]
- Ao, Y.; Zhang, Y.; Wang, Y.; Chen, Y.; Yang, L. Influences of rural built environment on travel mode choice of rural residents: The case of rural Sichuan. J. Transp. Geogr. 2020, 85, 102708. [Google Scholar] [CrossRef]
- Elmet, C.A.; Moceri, J.T. The importance of social connectedness in building AFC. J. Aging Res. 2012, 10, 173247. [Google Scholar] [CrossRef] [Green Version]
- Zheng, D.; Gong, J.; Zhang, C. Efficiency of medical service systems in the rural areas of Mainland China: A comparative study from 2013 to 2017. Public Health 2019, 171, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Nuntaboot, K.; Boonsawasdgulchai, P.; Bubpa, N. Roles of mutual help of local community networks in community heath ac-tivities: Improvement for the quality of life of older people in Thailand. Int. J. Nurs. Sci. 2019, 6, 266–271. [Google Scholar] [PubMed]
- World Health Organization (WHO). Age-Friendly Environments in Europe: A Handbook of Domains for Policy Action; WHO: Geneva, Switzerland, 2017; ISBN 978 92 890 5288 7. [Google Scholar]
- Barnes, S. The design in caring environments study group. The design of caring environments and the quality of life of older people. Ageing Soc. 2002, 22, 775–789. [Google Scholar] [CrossRef] [Green Version]
- WHOQOL Group. The world health organization quality of life assessment (WHOQOL): Position paper from the world health organization. Soc. Sci. Med. 1995, 41, 1403–1409. [Google Scholar] [CrossRef]
- Frisch, M.B. Quality of life therapy and assessment in health care. Clin. Psychol. Sci. Pr. 1998, 5, 19–40. [Google Scholar] [CrossRef]
- Leung, M.Y.; Liang, Q. Developing structural facilities management-quality of life models for the elderly in the common areas of public and subsidized housings. Habitat Int. 2019, 94, 102067. [Google Scholar] [CrossRef]
- Lei, P.; Xu, L.; Nwaru, B.; Long, Q.; Wu, Z. Social networks and health-related quality of life among Chinese old adults in urban areas: Results from 4th National Household Health Survey. Public Health 2016, 131, 27–39. [Google Scholar] [CrossRef] [PubMed]
- Van Leeuwen, K.; Malley, J.; Bosmans, J.; Jansen, A.; Ostelo, R.; Van Der Horst, H.; Netten, A.; Van Leeuwen, K. What can local authorities do to improve the social care-related quality of life of older adults living at home? Evidence from the Adult Social Care Survey. Health Place 2014, 29, 104–113. [Google Scholar] [CrossRef]
- Huang, B.; Liu, Y.; Chen, Y.; Wei, H.; Dong, G.; Helbich, M. Establishing associations between residential greenness and markers of adiposity among middle-aged and older Chinese adults through multilevel structural equation models. Int. J. Hyg. Environ. Health 2020, 230, 113606. [Google Scholar] [CrossRef]
- Li, C.; Zhou, Y. Residential environment and depressive symptoms among Chinese middle- and old-aged adults: A longitudinal population-based study. Health Place 2020, 66, 102463. [Google Scholar] [CrossRef]
- Yu, J.Y.; Ma, G.X.; Cai, S. Disparities in the provision of aging-friendly communities in old and new urban neighborhoods in China. Eng. Constr. Archit. Manag. 2019, 26, 1277–1293. [Google Scholar] [CrossRef]
- WHOQOL Group. Development of the world health organization WHOQOL-BREF quality of life assessment. Psychol. Med. 1998, 28, 551–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization (WHO). Ageing and Health 2018. Available online: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health (accessed on 27 February 2021).
- Hair, J.F.J.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis, 7th ed.; Prentice-Hall: Hoboken, NJ, USA, 2010. [Google Scholar]
- Feng, I.M.; Chen, J.H.; Zhu, B.W.; Xiong, L. Assessment of and improvement strategies for the housing of health elderly: Improving quality of life. Sustainability 2018, 10, 722. [Google Scholar] [CrossRef] [Green Version]
- Menec, V.; Nowicki, S. Examining the relationship between communities’ ‘age-friendliness’ and life satisfaction and self-perceived health in rural Manitoba, Canada. Rural Remote Health 2014, 14, 2594. [Google Scholar] [PubMed]
- Jiang, G.; He, X.; Qu, Y.; Zhang, R.; Meng, Y. Functional evolution of rural housing land: A comparative analysis across four typical areas representing different stages of industrialization in China. Land Use Policy 2016, 57, 645–654. [Google Scholar] [CrossRef]
- Kim, S. Assessing mobility in an aging society: Personal and built environment factors associated with older people’s subjective transportation deficiency in the US. Transp. Res. Part F Traffic Psychol. Behav. 2011, 14, 422–429. [Google Scholar] [CrossRef]
- Leung, M.Y.; Famakin, I.O. Developing an integrated indoor Built Environment–QoL model for elderly in public and subsidized housing. Eng. Constr. Archit. Manag. 2019, 26, 1498–1517. [Google Scholar] [CrossRef]
- Davis, S.; Bartlett, H. Review Article: Healthy ageing in rural Australia: Issues and challenges. Australas. J. Ageing 2008, 27, 56–60. [Google Scholar] [CrossRef]
- Kay, R. Managing everyday (in)securities: Normative values, emotional security and symbolic recognition in the lives of Russian rural elders. J. Rural Stud. 2012, 28, 63–71. [Google Scholar] [CrossRef]
- Igarashi, A.; Matsumoto, H.; Takaoka, M.; Kugai, H.; Suzuki, M.; Yamamoto-Mitani, N. Educational Program for Promoting Collaboration Between Community Care Professionals and Convenience Stores. J. Appl. Gerontol. 2020, 39, 760–769. [Google Scholar] [CrossRef] [PubMed]
- Curl, A.L.; Stowe, J.D.; Cooney, T.M.; Proulx, C.M. Giving Up the Keys: How Driving Cessation Affects Engagement in Later Life. Gerontologist 2013, 54, 423–433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
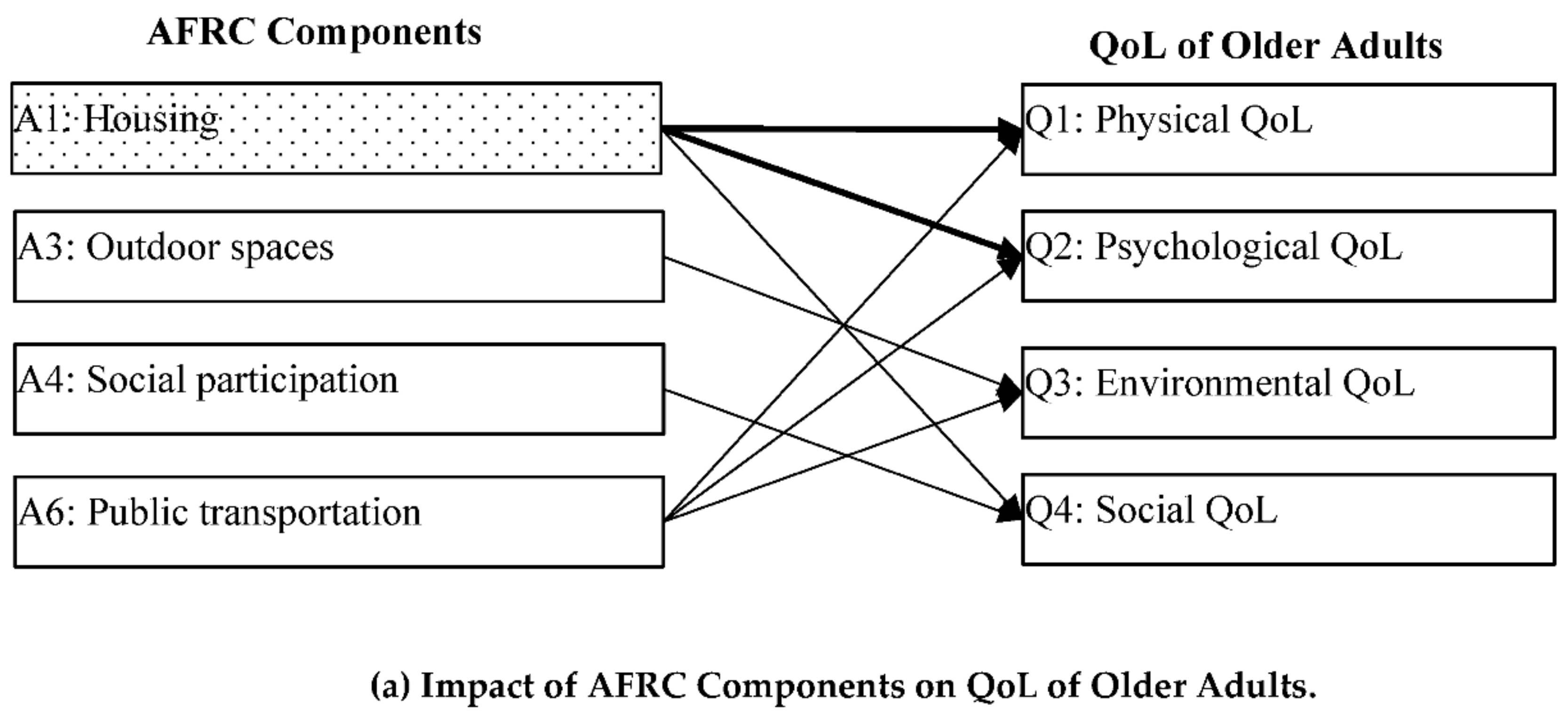
 Indicates components that significantly influence the QoL of both middle-aged and older adults.
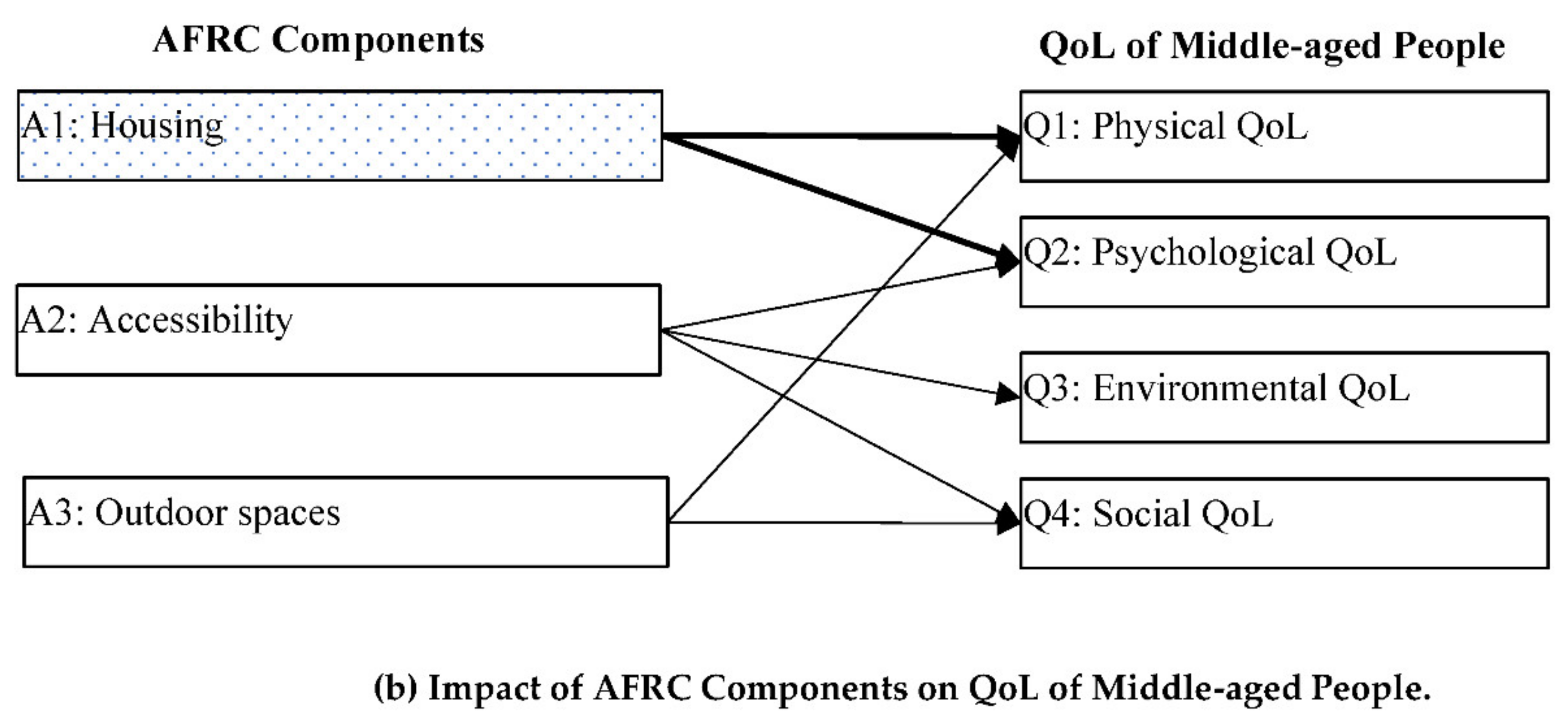
Indicates components that significantly influence the QoL of both middle-aged and older adults.
Indicates components that significantly influence the QoL of both middle-aged and older adults.
Indicates components that significantly influence the QoL of both middle-aged and older adults.


{kind=link}
{kind=link}
| Variables | Total | Older Adults (%) | Middle-Aged (%) |
|---|---|---|---|
| Overall | 863 | 470 (54.5) | 393 (45.5) |
| Gender | |||
| Male | 459 (54.0) | 306 (36.1) | 153 (17.9) |
| Female | 396 (46.0) | 158 (18.4) | 238 (27.6) |
| p-Value | 0.000 | ||
| Education | |||
| Primary | 337 (40.4) | 256 (30.3) | 85 (10.1) |
| Middle school | 288 (34.0) | 123 (14.5) | 165 (19.5) |
| High school | 197 (23.2) | 68 (8.0) | 129 (15.2) |
| College or above | 20 (2.4) | 11 (1.3) | 9 (1.1) |
| p-Value | 0.000 | ||
| Living Methods | |||
| Living alone | 49 (5.8) | 27 (3.2) | 22 (2.6) |
| Living with spouse | 294 (35.0) | 217 (25.9) | 77 (9.2) |
| Living with children | 395 (47.1) | 169 (20.1) | 226 (26.9) |
| Living with spouse and children | 101(12.0) | 43 (5.1) | 58 (6.9) |
| p-Value | 0.000 | ||
| Health Conditions | |||
| Good health | 431 (48.7) | 217 (25.6) | 196 (23.1) |
| Neutral | 344 (40.6) | 176 (20.8) | 168 (19.8) |
| Bad health | 91 (10.7) | 65 (7.6) | 26 (3.1) |
| p-Value | 0.063 | ||
| Independence | |||
| Independent | 743 (92.8) | 398 (49.7) | 345 (43.1) |
| Dependent | 58 (7.2) | 26 (3.8) | 22 (3.4) |
| p-Value | 0.680 | ||
| Income | |||
| <1000 Reminbi (RMB) ($154.7) | 163 (19.6) | 113 (13.5) | 51(6.1) |
| 1000–2500 RMB ($154.7–$386.8) | 353 (42.3) | 172 (20.6) | 181 (21.7) |
| 2500–5000 RMB ($386.8–$773.5) | 191 (22.9) | 103 (12.3) | 88 (10.5) |
| >5000 RMB ($773.5) | 124 (14.9) | 58 (6.9) | 66 (7.9) |
| p-Value | 0.002 |
| Factors | Items | Descriptions | Alpha (α) |
|---|---|---|---|
| Age-Friendly Rural Communities | |||
| A1: Housing | a1 | Well-constructed housing provides safe and comfortable shelter. | 0.876 |
| a2 | Interior spaces and level surfaces allow easy movement. | ||
| a3 | The daylighting and ventilation of housing is good. | ||
| A2: Accessibility | a4 | Community services are situated together and are accessible. | 0.836 |
| a5 | Transport stations are accessible and have adequate seating and shelter. | ||
| a6 | Community services are conveniently located and accessible by public transportation. | ||
| a7 | Health service facilities such as hospitals are fully accessible. | ||
| a8 | Pavements are non-slip and barrier-free for walking. | ||
| A3: Outdoor spaces | a9 | Public areas are clean and pleasant in rural communities. | 0.712 |
| a10 | Outdoor spaces in rural communities are sufficient for gathering and social activities. | ||
| a11 | Public toilets in rural areas are sufficient, well-maintained, and accessible. | ||
| a12 | Rural public facilities are sufficient and well-maintained. | ||
| A4: Social participation | a13 | Adequate community support services are offered for promoting quality of life of residents in rural areas. | 0.794 |
| a14 | Community activities and events can be attended by adults of different generations. | ||
| a15 | Community activities are affordable, with no additional participation costs. | ||
| a16 | The security and safety of all residents in rural communities can be guaranteed. | ||
| a17 | Community service facilities are safely constructed. | ||
| A5: Communication and information | a18 | A basic and effective communication system reaches rural community residents of all ages. | 0.851 |
| a19 | Regular and widespread distribution of information is provided. | ||
| a20 | Telephone answering services give instructions slowly and clearly for rural community residents of all ages. | ||
| a21 | Rural residents are regularly consulted on how they can be better served. | ||
| A6: Public transportation | a22 | Public transportation costs are consistent, clearly displayed, and affordable. | 0.880 |
| a23 | All rural areas and services are accessible by public transport, with good connections and well-marked routes and vehicles. | ||
| a24 | Public transportation services in rural communities are reliable and frequent. | ||
| a25 | Vehicles are clean and have priority seating. | ||
| Quality of Life (QoL) | |||
| Q1: Physical QoL | q1 | To what extent do you feel that pain prevents you from doing what you need to do? | 0.708 |
| q2 | How much do you need any medical treatment to function in your daily life? | ||
| q3 | How well are you able to get around? | ||
| q4 | Do you have enough energy for everyday life? | ||
| q5 | How satisfied are you with your ability to perform your daily living activities? | ||
| q6 | How satisfied are you with your work capacity? | ||
| q7 | How satisfied are you with your sleep? | ||
| Q2: Psychological QoL | q8 | How satisfied are you with yourself? | 0.715 |
| q9 | How much do you enjoy life? | ||
| q10 | How well are you able to concentrate? | ||
| q11 | How often do you have negative feelings? | ||
| q12 | Are you able to accept your bodily appearance? | ||
| Q3: Environmental QoL | q13 | How safe do you feel in your daily life? | 0.837 |
| q14 | How healthy is your physical environment? | ||
| q15 | Have you enough money to meet your needs? | ||
| q16 | How accessible is the information you need in day-to-day life? | ||
| q17 | How satisfied are you with the conditions of your living place? | ||
| q18 | How satisfied are you with access to health services? | ||
| q19 | How satisfied are you with your transport? | ||
| Q4: Social QoL | q20 | To what extent do you have the opportunity for leisure activities? | 0.761 |
| q21 | How satisfied are you with your personal relationships? | ||
| q22 | How satisfied are you with the support you get from your friends? | ||
| Factors | Middle-Aged | Older Adults | Mean Difference | t-Value | p-Value |
|---|---|---|---|---|---|
| A1: Housing | 3.916 | 3.495 | 0.421 | 5.306 | 0.000 |
| A2: Accessibility | 3.545 | 2.859 | 0.686 | 9.210 | 0.000 |
| A3: Outdoor spaces | 3.593 | 2.927 | 0.667 | 7.785 | 0.000 |
| A4: Community services | 3.472 | 2.851 | 0.621 | 7.099 | 0.000 |
| A5: Communication & info. | 3.475 | 2.767 | 0.708 | 8.484 | 0.000 |
| A6: Public transportation | 3.451 | 2.878 | 0.573 | 6.656 | 0.000 |
| Q1: Physical QoL | 3.605 | 3.404 | 0.201 | 3.803 | 0.000 |
| Q2: Psychological QoL | 3.713 | 3.721 | −0.008 | −0.135 | 0.891 |
| Q3: Social QoL | 3.738 | 3.447 | 0.292 | 5.912 | 0.000 |
| Q4: Environmental QoL | 3.833 | 3.599 | 0.234 | 4.127 | 0.000 |
| Dependent | Independent | B | t | Sig. t | R2 | F | Significance. F |
|---|---|---|---|---|---|---|---|
| Q1: Physical QoL | Constant | 2.834 | 20.882 | 0.000 | 0.109 | 18.427 | 0.000 |
| A6: Public transportation | 0.110 | 3.386 | 0.000 | ||||
| A1: Housing | 0.097 | 2.758 | 0.000 | ||||
| Q2: Psychological QoL | Constant | 2.831 | 17.180 | 0.000 | 0.104 | 15.614 | 0.000 |
| A1: Housing | 0.143 | 3.322 | 0.001 | ||||
| A6: Public transportation | 0.091 | 2.273 | 0.024 | ||||
| Q3: Social QoL | Constant | 2.611 | 22.228 | 0.000 | 0.241 | 54.193 | 0.000 |
| A3: Outdoor spaces | 0.191 | 4.046 | 0.000 | ||||
| A6: Public transportation | 0.125 | 2.523 | 0.012 | ||||
| Q4: Environmental QoL | Constant | 2.615 | 16.412 | 0.000 | 0.188 | 40.232 | 0.000 |
| A4: Social participation | 0.256 | 6.430 | 0.000 | ||||
| A1: Housing | 0.084 | 1.981 | 0.048 |
| Dependent | Independent | B | t | Sig.t | R2 | F | Sig.F |
|---|---|---|---|---|---|---|---|
| Q1: Physical QoL | Constant | 2.351 | 14.720 | 0.000 | 0.153 | 25.593 | 0.000 |
| A3: Outdoor spaces | 0.175 | 4.412 | 0.000 | ||||
| A1: Housing | 0.155 | 3.549 | 0.000 | ||||
| Q2: Psychological QoL | Constant | 2.487 | 12.775 | 0.000 | 0.128 | 20.909 | 0.000 |
| A2: Accessibility | 0.225 | 3.907 | 0.000 | ||||
| A1: Housing | 0.165 | 3.850 | 0.000 | ||||
| Q3: Social QoL | Constant | 2.338 | 17.851 | 0.000 | 0.205 | 74.526 | 0.000 |
| A2: Accessibility | 0.379 | 8.633 | 0.000 | ||||
| Q4: Environmental QoL | Constant | 2.719 | 16.609 | 0.000 | 0.119 | 20.042 | 0.000 |
| A3: Outdoor spaces | 0.167 | 3.796 | 0.000 | ||||
| A2: Accessibility | 0.137 | 2.108 | 0.036 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, J.; Ma, G.; Wang, S. Do Age-Friendly Rural Communities Affect Quality of Life? A Comparison of Perceptions from Middle-Aged and Older Adults in China. Int. J. Environ. Res. Public Health 2021, 18, 7283. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147283
Yu J, Ma G, Wang S. Do Age-Friendly Rural Communities Affect Quality of Life? A Comparison of Perceptions from Middle-Aged and Older Adults in China. International Journal of Environmental Research and Public Health. 2021; 18(14):7283. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147283
Chicago/Turabian StyleYu, Jingyu, Guixia Ma, and Shuxia Wang. 2021. "Do Age-Friendly Rural Communities Affect Quality of Life? A Comparison of Perceptions from Middle-Aged and Older Adults in China" International Journal of Environmental Research and Public Health 18, no. 14: 7283. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147283