
How Can We Develop an Efficient eHealth Service for Provision of Care for Elderly People with Balance Disorders and Risk of Falling? A Mixed Methods Study


Abstract
:1. Introduction
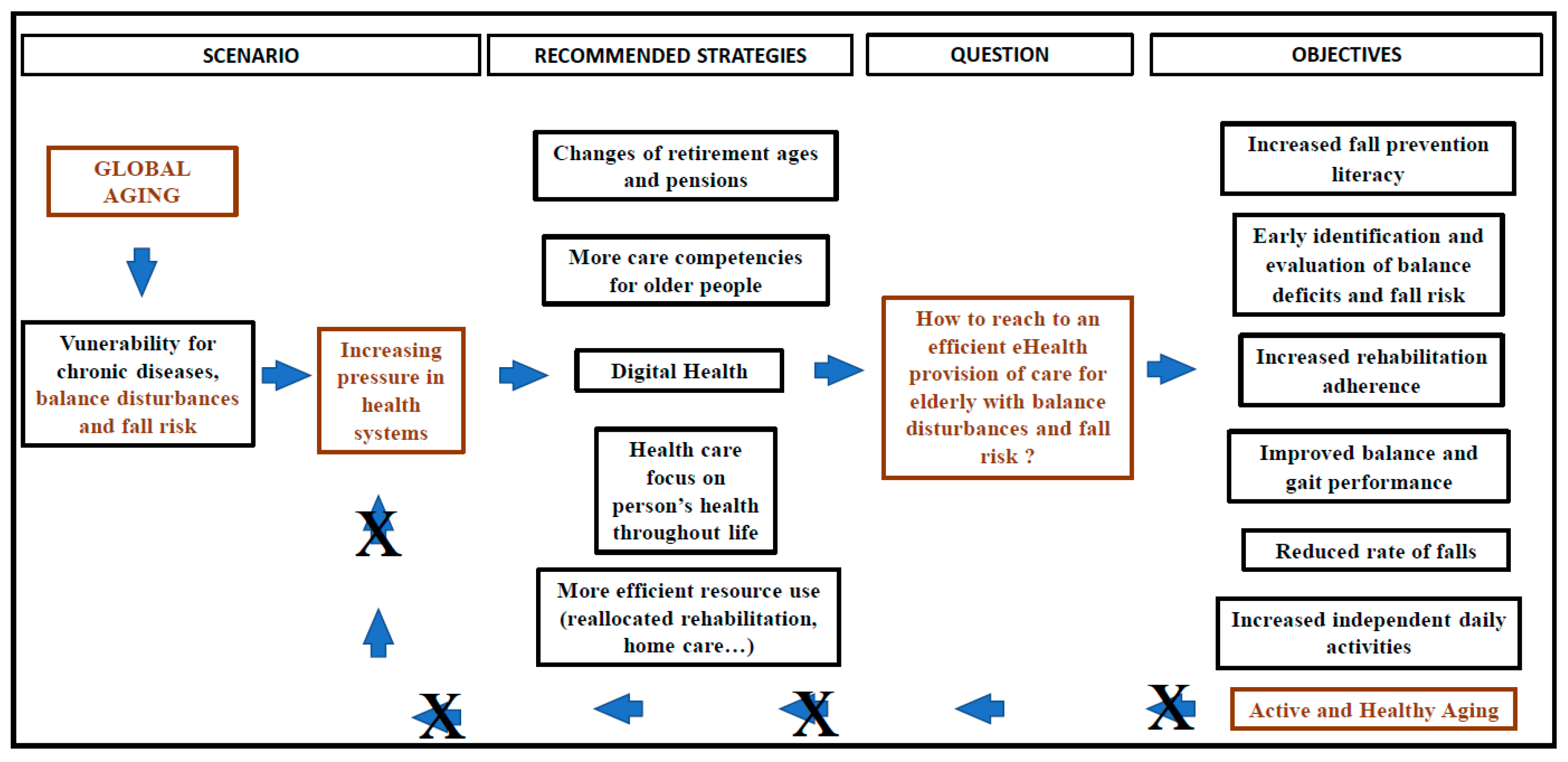
1.1. The Burden of an Ageing Population: Portugal and the World
1.2. Portugal and the Strategies Supported by IST
2. Materials and Methods
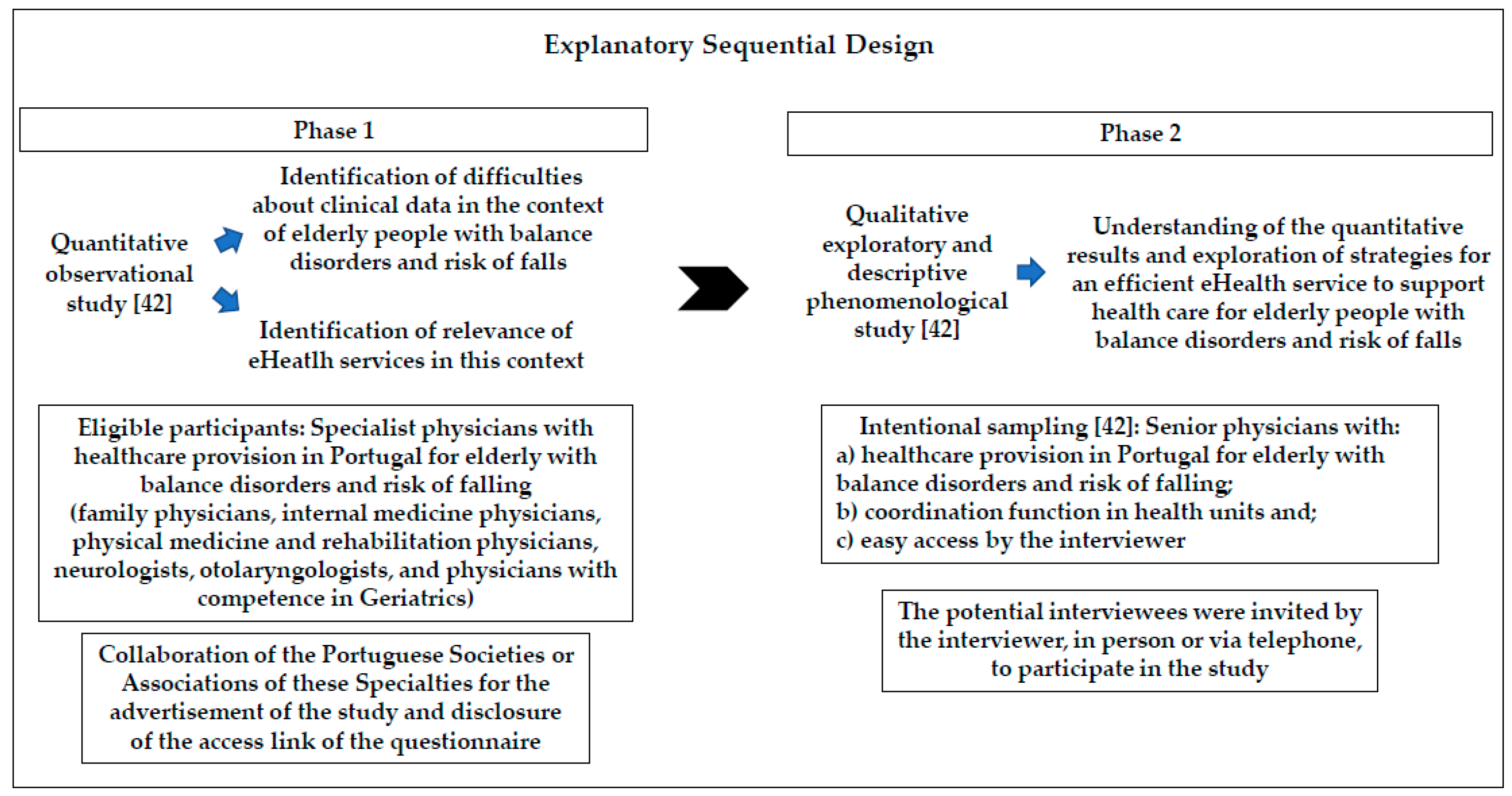
2.1. Study Design
2.2. Materials
2.3. Data Analysis
2.4. Ethical Considerations
3. Results
3.1. First Phase: Quantitative Research
3.1.1. Socio-Demographic Participant Data
3.1.2. Difficulties and Medical Satisfaction Level Related to Current Clinical Data in the EMR (Electronic Medical Registration)
3.1.3. Relevance of the Use of eHealth
3.2. Second phase: Qualitative Research
3.2.1. Socio-Demographic Participant Data
3.2.2. Content Analysis
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Number Question | Subject | Answer Choices |
|---|---|---|
| Q1 | Sex | Male Female |
| Q2 | Age | = or <30 31–40 41–50 51–60 = or >61 |
| Q3 | Specialty | Physical Medicine and Rehabilitation General and Family Medicine Internal Medicine Otorhinolaryngology Neurology |
| Q4 | Competence in Geriatrics | Yes No |
| Q5 | Main job | Personalized public health care unit Family health unit Public hospital Hospital in public-private partnership University hospital Private health unit |
| Q6 | Regional Health Administration | North Center Lisbon and Tejo Valey Alentejo Algarve Madeira Azores |
| Q7 | Monthly frequency of health care provision for elderly with balance disorders | = or <25% 26 a 50% 51 a 75% =or >76% Do not answer/Do not know |
| Q8 | Monthly frequency of health care provision for elderly with consequent falls | = or <25% 26 a 50% 51 a 75% = or >76% Do not answer/Do not know |
| Q9 | Need to access data from previous care consultations of elderly people with balance disorders and risk of falling | = or <25% 26 a 50% 51 a 75% = or >76% Do not answer/Do not know |
| Q10 | Access to data from previous care consultations for elderly people with balance disorders and risk of falling | Clinical paper process Electronic medical record (EMR) Paper information provided by the patient Do not answer/Do not know |
| Q11 | Relevance of data about previous health care to the elderly with balance disorders and risk of falling for a new provision of healthcare in this context | Never Rarely Sometimes Often Always Do not answer/Do not know |
| Q12 | Estimated time spent on Information Systems and Technologies (IST)-related activities | = or >76% 51 a 75% 26 a 50% = or <25% Do not use Do not answer/Do not know |
| Q13 | General usefulness of clinical data in the EMR | Excellent Very good Good Bad Very bad Do not use Do not answer/Do not know |
| Q14 | Satisfaction with time spent to access clinical data, in the EMR, from previous care consultations for elderly people with balance disorders and risk of falling | Very dissatisfied Dissatisfied Satisfied Very Satisfied Do not use Do not answer/Do not know |
| Q15 | Satisfaction with availability of sufficient and understandable clinical data, in the EMR, from previous care consultations for elderly people with balance disorders and risk of falling | Very dissatisfied Dissatisfied Satisfied Very Satisfied Do not use Do not answer/Do not know |
| Q16 | Satisfaction with time spent to fill-in new data, in the EMR, related to the provision of health care to the elderly with balance disorders and risk of falling | Very dissatisfied Dissatisfied Satisfied Very Satisfied Do not use Do not answer/Do not know |
| Q17 | General satisfaction with the use of IST (usefulness, quality) in the context of elderly with balance disorders and risk of falling | Very dissatisfied Dissatisfied Satisfied Very Satisfied Do not use Do not answer/Do not know |
| Q18 | Relevance of eHealth in the context of elderly with balance disorders and risk of falling | Very relevant Relevant No difference Irrelevant Very irrelevant Do not answer/Do not know |
Appendix B
| Thematic Categories | Questions |
|---|---|
| Current clinical data in Portugal | “What are the medical difficulties related with current clinical data in the context of health care provision for elderly with balance disorders and risk of falling?” |
| Interventions to improve the clinical data | What strategies can be implemented to improve clinical data? |
| eHealth contribution | “What do you think about the contribution of eHealth?” |
| Strategies to improve the use of eHealth services | How can eHealth services be suitable? What are the necessary strategies? What difficulties must be overcome? |
References
- European Innovation Partnership on Active and Healthy Ageing (EIP-AHA). Action Plan on Specific Action on Innovation in Support of Personalized Health Management, Starting with a Falls Prevention Initiative. 2013. Available online: https://ec.europa.eu/eip/ageing/library/action-plan-specific-action-innovation-support-personalized-health-management-starting-falls_en.html (accessed on 15 January 2020).
- The International Society for Quality in Health Care (ISQua). Health Systems and Their Sustainability: Dealing with the Impending Pressures of Ageing, Chronic and Complex Conditions, Technology and Resource Constraints. Whitepaper. 2016. Available online: https://isqua.org/resources-blog/resources?page=1&search=Health%20Systems%20and%20their%20Sustainability&date_range_start=&date_range_end= (accessed on 15 January 2020).
- National Institute for Health and Care Excellence (NICE). Multimorbility: Clinical Assessment and Management. 2016. Available online: https://www.nice.org.uk/guidance/ng56 (accessed on 15 January 2020).
- Simões, J.; Augusto, G.F.; Fronteira, I.; Hernández-Quevedo, C. Portugal: Health system review. Health Syst. Transit. 2017, 19, 1–184. Available online: http://www.healthobservatory.eu (accessed on 17 January 2020).
- Amalberti, R.; Vincent, C.; Nicklin, W.; Braithwaite, J. Coping with more people with more illness. Part 1: The nature of the challenge and the implications for safety and quality. Int. J. Qual. Health Care 2019, 31, 154–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- OECD. Health at a Glance 2019: OECD Indicators; OECD Publishing: Paris, France, 2019. [Google Scholar] [CrossRef]
- European Union. Ageing Europe—Looking at the Lives of Older People in the EU. 2020. Available online: https://ec.europa.eu/eurostat (accessed on 26 November 2020).
- Salzman, B. Gait and balance disorders in older adults. Am. FAM Physician 2010, 82, 61–68. [Google Scholar] [PubMed]
- Health Evidence Network (HEN)—WHO. What are the Main Risk Factors for Falls Amongst Older People and What are the Most Effective Interventions to Prevent These Falls? 2004. Available online: http://www.euro.who.int/document/E82552.pdf (accessed on 20 October 2020).
- Ha, V.A.T.; Nguyen, T.N.; Nguyen, T.X.; Nguyen, H.T.T.; Nguyen, T.T.H.; Nguyen, A.T.; Pham, T.; Thanh Vu, H.T. Prevalence and Factors Associated with Falls among Older Outpatients. Int. J. Environ. Res. Public Health 2021, 18, 4041. [Google Scholar] [CrossRef]
- Haagsma, J.A.; Olij, B.F.; Majdan, M.; van Beeck, E.F.; Vos, T.; Castle, C.D.; Dingels, Z.V.; Fox, J.T.; Hamilton, E.B.; Liu, Z.; et al. Falls in older aged adults in 22 European countries: Incidence, mortality and burden of disease from 1990 to 2017. INJ Prev. 2020, 26, i67–i74. [Google Scholar] [CrossRef] [PubMed]
- Kerber, K.A. Vertigo and Dizziness in the Emergency Department. Emerg. Med. Clin. N. Am. 2009, 27, 39–50. [Google Scholar] [CrossRef] [Green Version]
- Heinrich, S.; Rapp, K.; Rissmann, U.; Becker, C.; König, H.H. Cost of falls in old age: A systematic review. Osteoporos. Int. 2010, 21, 891–902. [Google Scholar] [CrossRef]
- Tehrani, A.S.S.; Coughlan, D.; Hsieh, Y.H.; Mantokoudis, G.; Korley, F.K.; Kerber, K.A.; Frick, K.D.; Newman-Toker, D.E. Rising Annual Costs of Dizziness Presentations to U.S. Emergency Departments. Acad. Emerg. Med. 2013, 20, 689–696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reis, L.; Lameiras, R.; Cavilhas, P.; Escada, P. Epidemiology of Vertigo on Hospital Emergency. Acta Med. Port. 2016, 29, 326–331. [Google Scholar] [CrossRef] [Green Version]
- Nolte, E.; Merkur, S.; Anell, A. Achieving Person-Centred Health Systems; Cambridge University Press: Cambridge, UK, 2020; pp. 1–396. [Google Scholar]
- Winter, A.; Takabayashi, K.; Jahn, F.; Kimura, E.; Engelbrecht, R.; Haux, R.; Honda, M.; Hübner, U.H.; Inoue, S.; Kohl, C.D.; et al. Quality Requirements for Electronic Health Record Systems. A Japanese-German Information Management Perspective. Methods Inf. Med. 2017, 56, e92–e104. [Google Scholar]
- Ammenwerth, E.; Duftschmid, G.; Al-Hamdan, Z.; Bawadi, H.; Cheung, N.T.; Cho, K.H.; Goldfarb, G.; Gülkesen, K.H.; Harel, N.; Kimura, M.; et al. International Comparison of Six Basic eHealth Indicators Across 14 Countries: An eHealth Benchmarking Study. Methods Inf. Med. 2020, 59, e46–e63. [Google Scholar] [PubMed]
- Lapão, L.V.; Dussault, G. The contribution of eHealth and mHealth to improving the performance of the health workforce: A review. Public Health Panorama. 2017, 3, 463–471. [Google Scholar]
- Blandford, A. HCI for health and wellbeing: Challenges and opportunities. Int J. Hum. Comput. Stud. 2019, 131, 41–51. [Google Scholar] [CrossRef]
- World Health Organization (WHO). mHealth Use of Appropriate Digital Technologies for Public Health—EB142/20. 2017. Available online: https://apps.who.int/gb/ebwha/pdf_files/EB142/B142_20-en.pdf (accessed on 15 January 2020).
- Uei, S.L.; Kuo, Y.M.; Tsai, C.H.; Kuo, Y.L. An Exploration of Intent to Use Telehealth at Home for Patients with Chronic Diseases. Int. J. Environ. Res. Public Health 2017, 14, 1544. [Google Scholar] [CrossRef] [Green Version]
- Sun, R.; Sosnoff, J.J. Novel sensing technology in fall risk assessment in older adults: A systematic review. BMC Geriatr. 2018, 18, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rucco, R.; Sorriso, A.; Liparoti, M.; Ferraioli, G.; Sorrentino, P.; Ambrosanio, M.; Baselice, F. Type and Location of Wearable Sensors for Monitoring Falls during Static and Dynamic Tasks in Healthy Elderly: A Review. Sensors 2018, 18, 1613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, H.; Mirza, F.; Naeem, M.A.; Baig, M.M. Falls management framework for supporting an independent lifestyle for older adults: A systematic review. Aging Clin. Exp. Res. 2018, 30, 1275–1286. [Google Scholar] [CrossRef]
- Leirós-Rodríguez, R.; García-Soidán, J.L.; Romo-Pérez, V. Analyzing the Use of Accelerometers as a Method of Early Diagnosis of Alterations in Balance in Elderly People: A Systematic Review. Sensors 2019, 19, 3883. [Google Scholar] [CrossRef] [Green Version]
- Montesinos, L.; Castaldo, R.; Pecchia, L. Wearable Inertial Sensors for Fall Risk Assessment and Prediction in Older Adults: A Systematic Review and Meta-Analysis. IEEE Trans. Neural Syst. Rehabil. Eng. 2018, 26, 573–582. [Google Scholar] [CrossRef] [Green Version]
- Bet, P.; Castro, P.C.; Ponti, M.A. Fall detection and fall risk assessment in older person using wearable sensors: A systematic review. Intern. J. Med. Inform. 2019, 130, 103946. [Google Scholar] [CrossRef]
- Gaspar, A.G.M.; Lapão, L.V. eHealth for Addressing Balance Disorders in the Elderly: Systematic Review. J. Med. Internet Res. 2021, 23, e22215. [Google Scholar] [CrossRef] [PubMed]
- Skjæret, N.; Nawaz, A.; Morat, T.; Schoene, D.; Helbostad, J.L.; Vereijken, B. Exercise and rehabilitation delivered through exergames in older adults: An integrative review of technologies, safety and efficacy. Int. J. Med. Inf. 2016, 85, 1–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, S.D.; Guo, L.; Kang, D.; Xiong, S. Exergame technology and interactive interventions for elderly fall prevention: A systematic literature review. Appl. Erg. 2017, 65, 570–581. [Google Scholar] [CrossRef]
- Eysenbach, G. What is e-health? J. Med. Internet Res. 2001, 3, E20. [Google Scholar] [CrossRef]
- Poenaru, C.; Poenaru, E.; Vinereanu, D. Current Perception of Telemedicine in an EU Country. Maedica 2014, 9, 367–374. [Google Scholar]
- Catan, G.; Espanha, R.; Mendes, R.V.; Toren, O.; Chinitz, D. Health information technology implementation—Impacts and policy considerations: A comparison between Israel and Portugal. ISR J. Health Policy Res. 2015, 4, 41. [Google Scholar] [CrossRef] [Green Version]
- Ayatollahi, H.; Sarabi, F.Z.P.; Langarizadeh, M. Clinicians’ Knowledge and Perception of Telemedicine Technology. Perspect Health Inf. Manag. 2015, 12, 1c. [Google Scholar]
- Radhakrishnan, K.; Xie, B.; Berkley, A.; Kim, M. Barriers and Facilitators for Sustainability of Tele-Homecare Programs: A Systematic Review. Health Serv. Res. 2016, 51, 48–75. [Google Scholar] [CrossRef] [Green Version]
- Albarraka, A.I.; Mohammedb, R.; Almarshoudc, N.; Almujalli, L.; Aljaeed, R.; Altuwaijiri, S.; Albohairy, T. Assessment of physician’s knowledge, perception and willingness of telemedicine in Riyadh region, Saudi Arabia. J. Infect. Public Health 2021, 14, 97–102. [Google Scholar] [CrossRef]
- Wynn, R.; Gabarron, E.; Johnsen, J.K.; Traver, V. Special Issue on E-Health Services. Int. J. Environ. Res. Public Health 2020, 17, 2885. [Google Scholar] [CrossRef] [PubMed]
- Gil, H. The elderly and the digital inclusion: A brief reference to the initiatives of the European union and Portugal. MOJ Gerontol. Ger. 2019, 4, 213–221. [Google Scholar] [CrossRef] [Green Version]
- SPMS, Portuguese National Centre of Telehealth (CNTS). National Strategic Telehealth Plan (PENTS) 2019–2022. Available online: https://www.spms.min-saude.pt/wp-content/uploads/2019/11/PENTS_Tradução.pdf (accessed on 15 February 2021).
- SPMS. SNS 24 Projeto Proximidade Senior. Available online: https://www.spms.min-saude.pt/pesquisa-geral/?_sf_s=idoso (accessed on 15 August 2020).
- Creswell, J.W.; Creswell, J.D. Research design. In Qualitative, Quantitative, and Mixed Methods Approaches, 5th ed.; SAGE Publications Inc.: Los Angeles, CA, USA, 2018. [Google Scholar]
- SurveyMonkey. Available online: https://help.surveymonkey.com/articles/en_US/kb/How-do-I-make-surveys-anonymous (accessed on 15 January 2019).
- Eysenbach, G. Improving the quality of Web surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J. Med. Internet Res. 2004, 6, e34. [Google Scholar] [CrossRef]
- IBM. SPSS Statistics. Available online: https://www.ibm.com/products/spss-statistics/details (accessed on 12 September 2019).
- Assembleia da República. Lei nº 58/2019 de 8 de Agosto de 2019. Diário da República n.º 151/2019, Série I de 2019-08-08. 3-40. Available online: https://data.dre.pt/eli/lei/58/2019/08/08/p/dre (accessed on 22 February 2021).
- Ordem dos Médicos de Portugal. Estatísticas 2019. Available online: https://ordemdosmedicos.pt/wp-content/uploads/2020/01/ESTATISTICAS_ESPECIALIDADES_2019.pdf (accessed on 17 July 2020).
- WHO. Active Ageing, A Policy Framework. A Contribution of the WHO to the Second United Nations World Assembly on Ageing, Madrid, Spain, April, 2002. Available online: https://extranet.who.int/agefriendlyworld/wp-content/uploads/2014/06/WHO-Active-Ageing-Framework.pdf (accessed on 17 January 2020).
- Aitken, C.; Power, R.; Dwyer, R. A very low response rate in an on-line survey of medical practitioners. Aust. N. Z. J. Public Health 2008, 32, 288–289. [Google Scholar] [CrossRef] [PubMed]
- Lapão, L.V.; Da Silva, M.M.; Gregório, J. Implementing an online pharmaceutical service using design science research. BMC Med. Inform. Decis. Mak. 2017, 17, 1–4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lapão, L.V.; Pisco, L. Primary health care reform in Portugal, 2005–2018: The future and challenges of coming of age. Cad. Saude Publica 2019, 35 (Suppl. 2), e00042418. [Google Scholar]
- Liotta, G.; Canhão, H.; Cenko, F.; Cutini, R.; Vellone, E.; Illario, M.; Kardas, P.; Poscia, A.; Sousa, R.D.; Palombi, L.; et al. Active Ageing in Europe: Adding Healthy Life to Years. Front. Med. 2018, 5. [Google Scholar] [CrossRef]
- Eysenbach, G.; Wyatt, J. Using the Internet for surveys and health research. J. Med. Internet Res. 2002, 4, E13. [Google Scholar] [CrossRef] [PubMed]


| Demographic Data/Specialty | Family Physician | Internal Medicine Physician | PMR Physician | Neurologist | Otolaryngologist | Total |
|---|---|---|---|---|---|---|
| Physician number according to Portuguese General Medical Council—year 2019 [47] | 7451 | 2847 | 691 | 549 | 676 | 12,214 |
| Number of participants of the study according to specialty (%) | 18 (15.3%) | 46 (39.0%) | 5 (4.2%) | 4 (3.4%) | 45 (38.1%) | 118 (100%) |
| Participation according to specialty total number of physicians (%) | 18/7451 (0.2%) | 46/2847 (1.6%) | 5/691 (0.7%) | 4/549 (0.7%) | 45/676 (6.7%) | 118/12 214 (1.0%) |
| Participant’s gender (M/F) | 3/15 | 15/31 | 3/2 | 1/3 | 24/21 | 46/72 |
| Participant age ≤ 50 years old/Total physician number age ≤ 50 years old a | 15/2390 | 34/1299 | 5/271 | 3/234 | 30/233 | 87/4427 |
| Participant age >51 years old/Total physician number age > 51 years old a | 3/5061 | 12/1548 | 0/420 | 1/315 | 15/443 | 31/7787 |
| Regional Health Administration of Portugal | ||||||
| -North | 2 | 13 | 1 | 0 | 8 | 24 |
| -Center | 0 | 7 | 1 | 0 | 12 | 20 |
| -Lisbon and Tejo Valey | 16 | 19 | 3 | 4 | 22 | 64 |
| -Alentejo | 0 | 3 | 0 | 0 | 1 | 4 |
| -Algarve | 0 | 4 | 0 | 0 | 2 | 6 |
| -Madeira | 0 | 0 | 0 | 0 | 0 | 0 |
| -Azores | 0 | 0 | 0 | 0 | 0 | 0 |
| Main job—Public sector | 17 | 43 | 4 | 4 | 29 | 97 |
| Main job—Private sector | 1 | 3 | 1 | 0 | 16 | 21 |
| Satisfaction Degree/Specialty | Family Physician | Internal Medicine Physician | PMR Physician | Neurologist | Otolaryngologist | Total |
|---|---|---|---|---|---|---|
| Time to data access (public and private main job) | ||||||
| -S | 1 | 12 | 3 | 1 | 25 | 42 (36%) |
| -D | 17 | 34 | 1 | 3 | 17 | 72 (61%) |
| -Others | 0 | 0 | 1 | 0 | 3 | 4 (3%) |
| TOTAL | 18 | 46 | 5 | 4 | 45 | 118 (100%) |
| Time to data access (public main job) | ||||||
| -S | 1 | 11 | 3 | 1 | 15 | 31 (32%) |
| -D | 16 | 32 | 0 | 3 | 12 | 63 (65%) |
| -Others | 0 | 0 | 1 | 0 | 2 | 3 (3%) |
| TOTAL | 17 | 43 | 4 | 4 | 29 | 97 (100%) |
| Sufficient/understandable data (public and private main job) | ||||||
| -S | 3 | 18 | 3 | 1 | 25 | 50 (42%) |
| -D | 15 | 27 | 2 | 3 | 18 | 65 (55%) |
| -Others | 0 | 1 | 0 | 0 | 2 | 3 (3%) |
| TOTAL | 18 | 46 | 5 | 4 | 45 | 118 (100%) |
| Sufficient/understandable data (public main job) | ||||||
| -S | 3 | 16 | 3 | 1 | 15 | 38 (39%) |
| -D | 14 | 26 | 1 | 3 | 13 | 57 (59%) |
| -Others | 0 | 1 | 0 | 0 | 1 | 2 (2%) |
| TOTAL | 17 | 43 | 4 | 4 | 29 | 97 (100%) |
| Time to fill data (public and private main job) | ||||||
| -S | 2 | 13 | 2 | 0 | 22 | 39 (33%) |
| -D | 16 | 29 | 3 | 4 | 20 | 72 (61%) |
| -Others | 0 | 4 | 0 | 0 | 3 | 7 (6%) |
| TOTAL | 18 | 46 | 5 | 4 | 45 | 118 (100%) |
| Time to fill data (public main job) | ||||||
| -S | 2 | 12 | 2 | 0 | 13 | 29 (30%) |
| -D | 15 | 27 | 2 | 4 | 14 | 62 (64%) |
| -Others | 0 | 4 | 0 | 0 | 2 | 6 (6%) |
| TOTAL | 17 | 43 | 4 | 4 | 29 | 97 (100%) |
| Relevance of eHealth / Specialty | Family Physician | Internal Medicine Physician | PMR Physician | Neurologist | Otolaryngologist | Total |
|---|---|---|---|---|---|---|
| Public and private main job | ||||||
| -Pertinent | 13 | 33 | 5 | 2 | 37 | 90 (76%) |
| -No pertinent | 2 | 3 | 0 | 1 | 3 | 9 (8%) |
| -Indifferent | 2 | 5 | 0 | 0 | 3 | 10 (8%) |
| -Others | 1 | 5 | 0 | 1 | 2 | 9 (8%) |
| TOTAL | 18 | 46 | 5 | 4 | 45 | 118 (100%) |
| Public main job | ||||||
| -Pertinent | 12 | 31 | 4 | 2 | 25 | 74 (77%) |
| -No pertinent | 2 | 3 | 0 | 1 | 1 | 7 (7%) |
| -Indifferent | 2 | 4 | 0 | 0 | 2 | 8 (8%) |
| -Others | 1 | 5 | 0 | 1 | 1 | 8 (8%) |
| TOTAL | 17 | 43 | 4 | 4 | 29 | 97 (100%) |
| Participant | Gender | Age | Specialty | Regional Health Administration of Portugal | Main Job | Interview | Audio Recording |
|---|---|---|---|---|---|---|---|
| 1 | M | 59 | Otolaryngology | LTV | Public sector | Face-to-face | Y |
| 2 | M | 55 | Neurology | LTV | Public sector | Face-to-face | Y |
| 3 | M | 53 | Internal Medicine | LTV | Public sector | Face-to-face | Y |
| 4 | M | 59 | Internal Medicine | LTV | Public sector | Face-to-face | Y |
| 5 | M | 47 | Family Medicine | LTV | Public sector | Face-to-face | Y |
| 6 | F | 66 | Family Medicine | Center | Public sector | Face-to-face | Y |
| 7 | F | 49 | Otolaryngology | LTV | Private sector | Face-to-face | Y |
| 8 | F | 55 | Otolaryngology | LTV | Private sector | Mobile phone | Y |
| Thematic Categories |
|---|
1. Current clinical data in the context of health provision for elderly with balance disorders and risk of falling: understanding of the medical dissatisfaction identified in the quantitative research
|
2. Interventions to improve the clinical data
|
3. eHealth contribution in this context: understanding of the relevance observed in the quantitative research
|
4. Strategies to improve eHealth services for a more effective healthcare provision
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gaspar, A.G.M.; Escada, P.; Lapão, L.V. How Can We Develop an Efficient eHealth Service for Provision of Care for Elderly People with Balance Disorders and Risk of Falling? A Mixed Methods Study. Int. J. Environ. Res. Public Health 2021, 18, 7410. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147410
Gaspar AGM, Escada P, Lapão LV. How Can We Develop an Efficient eHealth Service for Provision of Care for Elderly People with Balance Disorders and Risk of Falling? A Mixed Methods Study. International Journal of Environmental Research and Public Health. 2021; 18(14):7410. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147410
Chicago/Turabian StyleGaspar, Andréa Gomes Martins, Pedro Escada, and Luís Velez Lapão. 2021. "How Can We Develop an Efficient eHealth Service for Provision of Care for Elderly People with Balance Disorders and Risk of Falling? A Mixed Methods Study" International Journal of Environmental Research and Public Health 18, no. 14: 7410. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147410