
Roles of the Maternal and Child Health Handbook and Other Home-Based Records on Newborn and Child Health: A Systematic Review

 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Patient and Public Involvement Statement
2.2. Review Protocol
2.3. Selection Criteria
2.3.1. Population
2.3.2. Intervention
2.3.3. Comparison
2.3.4. Outcome
2.3.5. Types of Studies
2.4. Search Strategy
2.5. Evidence Retrieval
2.6. Data Extraction
2.7. Risk of Bias and Quality of Evidence
2.8. Data Analysis
- Should home-based records (intervention) compared to no use of any home-based records (control) be used for improving newborn/child health outcomes?
- Should a different type of home-based record (intervention) compared to a standard home-based record (control) be used for improving newborn/child health outcomes?
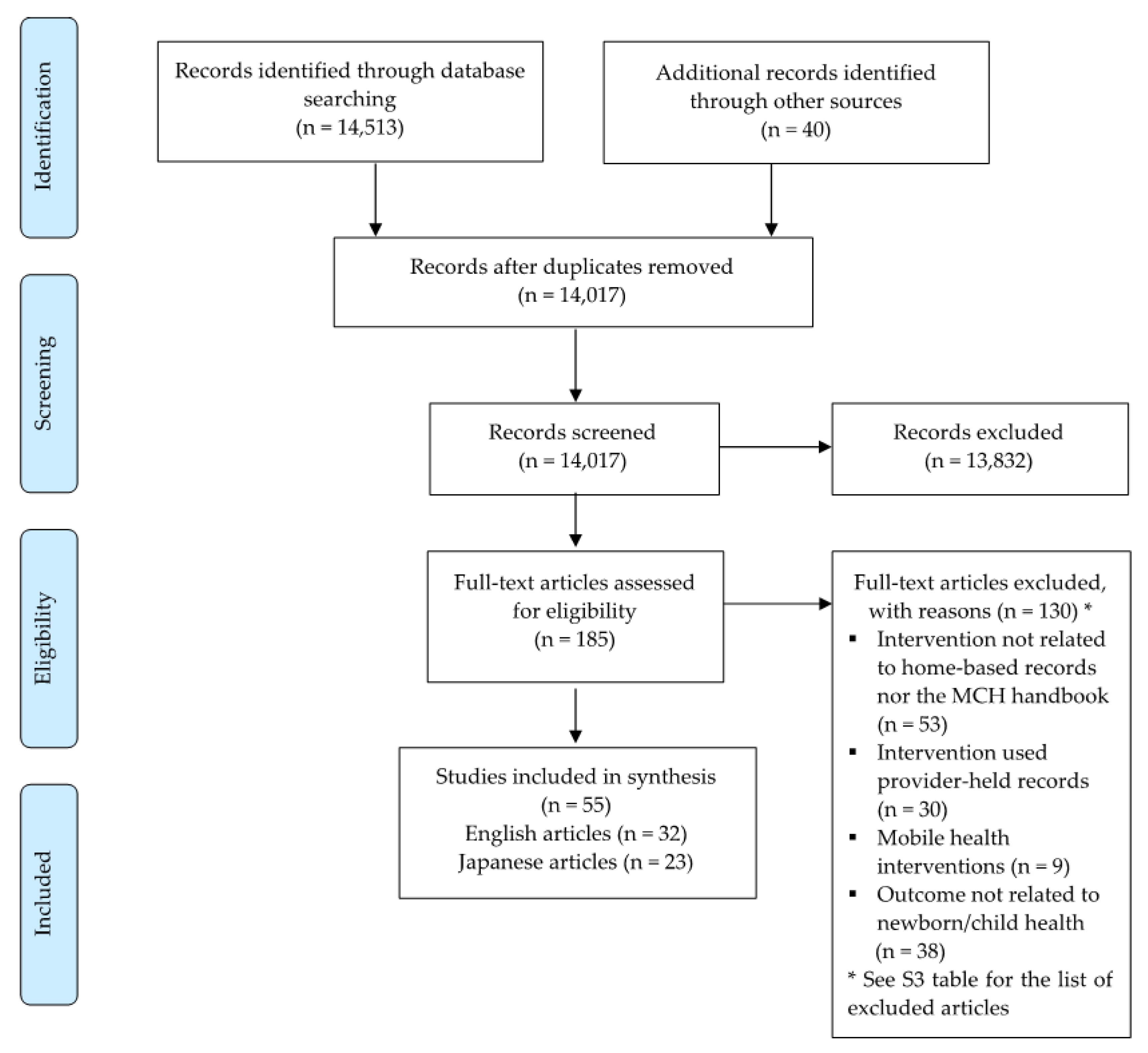
3. Results
3.1. Characteristics of Included Studies
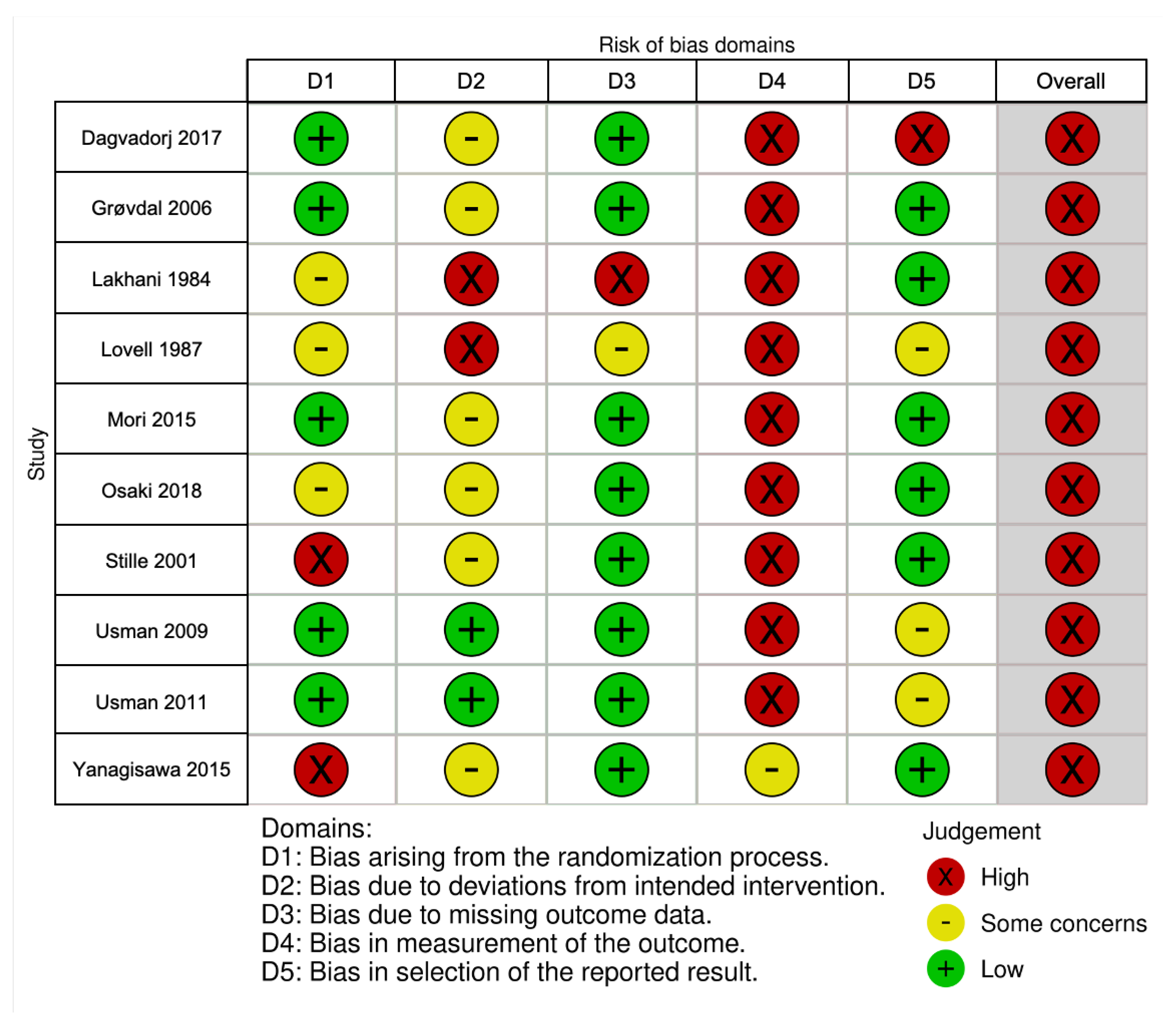
3.2. Risk of Bias in Included Studies
3.3. Roles of Home-Based Records on Newborn Health
3.4. Roles of Home-Based Records on Child Health
4. Discussion
5. Implications for Future Research
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. WHO Recommendations on Home-Based Records for Maternal, Newborn and Child Health. Available online: https://www.who.int/maternal_child_adolescent/documents/home-based-records-guidelines/en/ (accessed on 21 May 2021).
- Osaki, K.; Aiga, H. Adapting home-based records for maternal and child health to users’ capacities. Bull. World Health Organ. 2019, 97, 296–305. [Google Scholar] [CrossRef]
- Magwood, O.; Kpadé, V.; Thavorn, K.; Oliver, S.; Mayhew, A.D.; Pottie, K. Effectiveness of home-based records on maternal, newborn and child health outcomes: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0209278. [Google Scholar]
- Nakamura, Y. The role of maternal and child health (MCH) handbook in the era of sustainable development goals (SDGs). J. Glob. Health Sci. 2019, 1, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Osaki, K.; Aiga, H. What Is Maternal and Child Health Handbook? Available online: https://www.jica.go.jp/english/our_work/thematic_issues/health/technical_brief_mc.html (accessed on 21 May 2021).
- Osaki, K.; Hattori, T.; Toda, A.; Mulati, E.; Hermawan, L.; Pritasari, K.; Bardosono, S.; Kosen, S. Maternal and child health handbook use for maternal and child care: A cluster randomized controlled study in rural Java, Indonesia. J. Public Health 2019, 41, 170–182. [Google Scholar] [CrossRef] [PubMed]
- Mori, R.; Yonemoto, N.; Noma, H.; Ochirbat, T.; Barber, E.; Soyolgerel, G.; Nakamura, Y.; Lkhagvasuren, O. The maternal and child health (MCH) handbook in Mongolia: A cluster-randomized, controlled trial. PLoS ONE 2015, 10, e0119772. [Google Scholar] [CrossRef] [Green Version]
- Isaranurug, S. Maternal and child health handbook in Thailand. Kokusai Hoken Iryo. (J. Int. Health) 2009, 24, 61–66. [Google Scholar]
- Nakamura, Y. Maternal and child health handbook in Japan. JMAJ 2010, 53, 259–265. [Google Scholar]
- Aiga, H.; Pham Huy, T.K.; Nguyen, V.D. Cost savings through implementation of an integrated home-based record: A case study in Vietnam. Public Health 2018, 156, 124–131. [Google Scholar] [CrossRef]
- Every Woman Every Child. The Global Strategy for Women’s, Children’s and Adolescents’ Health 2016–2030. Available online: http://globalstrategy.everywomaneverychild.org/pdf/EWEC_globalstrategyreport_200915_FINAL_WEB.pdf (accessed on 21 May 2021).
- World Health Organization. Maternal, Newborn, Child and Adolescent Health. Available online: https://www.who.int/maternal_child_adolescent/documents/levels_trends_child_mortality_2019/en/ (accessed on 21 May 2021).
- World Health Organization. Children: Improving Survival and Well-Being. Available online: https://www.who.int/news-room/fact-sheets/detail/children-reducing-mortality (accessed on 21 May 2021).
- Svefors, P.; Selling, K.E.; Shaheen, R.; Khan, A.I.; Persson, L.; Lindholm, L. Cost-effectiveness of prenatal food and micronutrient interventions on under-five mortality and stunting: Analysis of data from the MINIMat randomized trial, Bangladesh. PLoS ONE 2018, 13, e0191260. [Google Scholar] [CrossRef] [Green Version]
- Goudet, S.; Jayaraman, A.; Chanani, S.; Osrin, D.; Devleesschauwer, B.; Bogin, B.; Madise, N.; Griffiths, P. Cost effectiveness of a community based prevention and treatment of acute malnutrition programme in Mumbai slums, India. PLoS ONE 2018, 13, e0205688. [Google Scholar] [CrossRef]
- Pitt, C.; Tawiah, T.; Soremekun, S.; ten Asbroek, A.H.; Manu, A.; Tawiah-Agyemang, C.; Hill, Z.; Owusu-Agyei, S.; Kirkwood, B.R.; Hanson, K. Cost and cost-effectiveness of newborn home visits: Findings from the Newhints cluster-randomised controlled trial in rural Ghana. Lancet Glob. Health. 2016, 4, e45–e56. [Google Scholar] [CrossRef] [Green Version]
- Gowani, S.; Yousafzai, A.K.; Armstrong, R.; Bhutta, Z.A. Cost effectiveness of responsive stimulation and nutrition interventions on early child development outcomes in Pakistan. Ann. N. Y. Acad. Sci. 2014, 1308, 149–161. [Google Scholar] [CrossRef] [Green Version]
- Fischer, T.K.; Anh, D.D.; Antil, L.; Cat, N.D.; Kilgore, P.E.; Thiem, V.D.; Rheingans, R.; Thole, H.; Glass, R.I.; Bresee, J.S. Health care costs of diarrheal disease and estimates of the cost-effectiveness of rotavirus vaccination in Vietnam. J. Infect. Dis. 2005, 192, 1720–1726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Cochrane. RoB 2: A Revised Cochrane Risk-of-Bias Tool for Randomized Trials. Available online: https://methods.cochrane.org/bias/resources/rob-2-revised-cochrane-risk-bias-tool-randomized-trials (accessed on 21 May 2021).
- Cochrane. ROBINS-I Tool. Available online: https://methods.cochrane.org/methods-cochrane/robins-i-tool (accessed on 21 May 2021).
- National Heart, Lung, and Blood Institute. Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 21 May 2021).
- Critical Appraisal Skills Programme. CASP Qualitative Studies Checklist. Available online: https://casp-uk.net/casp-tools-checklists/ (accessed on 21 May 2021).
- Hong, Q.N.; Fàbregues, S.; Bartlett, G.; Boardman, F.; Cargo, M.; Dagenais, P.; Gagnon, M.P.; Griffiths, F.; Nicolau, B.; O’Cathain, A.; et al. The mixed methods appraisal tool (MMAT) version 2018 for information professionals and researchers. Educ Inform. 2018, 34, 285–291. [Google Scholar] [CrossRef] [Green Version]
- Granholm, A.; Alhazzani, W.; Møller, M.H. Use of the GRADE approach in systematic reviews and guidelines. Br. J. Anaesth. 2019, 123, 554–559. [Google Scholar] [CrossRef]
- Campbell, M.; McKenzie, J.E.; Sowden, A.; Katikireddi, S.V.; Brennan, S.E.; Ellis, S.; Hartmann-Boyce, J.; Ryan, R.; Shepperd, S.; Thomas, J.; et al. Synthesis without meta-analysis (SWiM) in systematic reviews: Reporting guideline. BMJ 2020, 368, l6890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The World Bank. World Bank Country and Lending Groups. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (accessed on 21 May 2021).
- Shah, P.M.; Selwyn, B.J.; Shah, K.; Kumar, V. Evaluation of the home-based maternal record: A WHO collaborative study. Bull. World Health Organ. 1993, 71, 535–548. [Google Scholar] [PubMed]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (robvis): An R package and shiny web app for visualizing risk-of-bias assessments. Res. Synth. Methods 2021, 12, 55–61. [Google Scholar] [CrossRef]
- Kaneko, K.; Niyonkuru, J.; Juma, N.; Mbonabuca, T.; Osaki, K.; Aoyama, A. Effectiveness of the maternal and child health handbook in Burundi for increasing notification of birth at health facilities and postnatal care uptake. Glob. Health Action 2017, 10, 1297604. [Google Scholar] [CrossRef] [Green Version]
- Haeri Mazanderani, A.; Sherman, G.G.; Moyo, F.; Goga, A.E.; Feucht, U. Leveraging the road to health booklet as a unique patient identifier to monitor the prevention of mother-to-child transmission programme. S. Afr. Med. J. 2018, 108, 729–733. [Google Scholar] [CrossRef] [Green Version]
- Nasir, N.M.; Amran, Y.; Nakamura, Y. Changing knowledge and practices of mothers on newborn care through mother class: An intervention study in Indonesia. J. Trop Pediatr. 2017, 63, 440–446. [Google Scholar] [CrossRef] [Green Version]
- Yanagisawa, S.; Soyano, A.; Igarashi, H.; Ura, M.; Nakamura, Y. Effect of a maternal and child health handbook on maternal knowledge and behaviour: A community-based controlled trial in rural Cambodia. Health Policy Plan. 2015, 30, 1184–1192. [Google Scholar] [CrossRef] [Green Version]
- Lovell, A.; Zander, L.I.; James, C.E.; Foot, S.; Swan, A.V.; Reynolds, A. The St. Thomas’s hospital maternity case notes study: A randomised controlled trial to assess the effects of giving expectant mothers their own maternity case notes. Paediatr Perinat Epidemiol. 1987, 1, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Lakhani, A.D.; Avery, A.; Gordon, A.; Tait, N. Evaluation of a home based health record booklet. Arch. Dis. Child. 1984, 59, 1076–1081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stille, C.J.; Christison-Lagay, J.; Bernstein, B.A.; Dworkin, P.H. A simple provider-based educational intervention to boost infant immunization rates: A controlled trial. Clin. Pediatr. 2001, 40, 365–373. [Google Scholar] [CrossRef]
- Usman, H.R.; Akhtar, S.; Habib, F.; Jehan, I. Redesigned immunization card and center-based education to reduce childhood immunization dropouts in urban Pakistan: A randomized controlled trial. Vaccine 2009, 27, 467–472. [Google Scholar] [CrossRef]
- Usman, H.R.; Rahbar, M.H.; Kristensen, S.; Vermund, S.H.; Kirby, R.S.; Habib, F.; Chamot, E. Randomized controlled trial to improve childhood immunization adherence in rural Pakistan: Redesigned immunization card and maternal education. Trop. Med. Int. Health 2011, 16, 334–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inoue, M.; Takanashi, S.; Ushijima, H.; Okitsu, S.; Sakiyama, H.; Mizuguchi, M. Cumulative vaccination rate of rotavirus vaccines in Fuchu City, Tokyo [in Japanese]. J. Jpn. Pediatric Soc. 2015, 119, 525–537. [Google Scholar]
- Yamamoto, Y.; Nakano, C.; Suga, H. Study on caregiver awareness on vaccination- current status of caregiver support and reality after revision of vaccination law [in Japanese]. Bull. Kobe City Jun Coll. Nurs. 1998, 17, 61–66. [Google Scholar]
- Kimura, M. History of infection and vaccination for varicella and mumps among children and importance of immunization against these infections [in Japanese]. Jpn. J. Pediatric 2010, 63, 1959–1963. [Google Scholar]
- Jeffs, D.; Nossar, V.; Bailey, F.; Smith, W.; Chey, T. Retention and use of personal health records: A population-based study. J. Paediatr. Child. Health 1994, 30, 248–252. [Google Scholar] [CrossRef]
- McMaster, P.; McMaster, H.J.; Southall, D.P. Personal child health record and advice booklet programme in Tuzla, Bosnia Herzegovina. J. R. Soc. Med. 1996, 89, 202–204. [Google Scholar] [CrossRef]
- Kreuter, M.W.; Caburnay, C.A.; Chen, J.J.; Donlin, M.J. Effectiveness of individually tailored calendars in promoting childhood immunization in urban public health centers. Am. J. Public Health 2004, 94, 122–127. [Google Scholar] [CrossRef]
- Mukanga, D.O.; Kiguli, S. Factors affecting the retention and use of child health cards in a slum community in Kampala, Uganda, 2005. Matern. Child. Health J. 2006, 10, 545–552. [Google Scholar] [CrossRef] [PubMed]
- McElligott, J.T.; Darden, P.M. Are patient-held vaccination records associated with improved vaccination coverage rates? Pediatrics 2010, 125, e467–e472. [Google Scholar] [CrossRef] [PubMed]
- Abbott, P.; Menzies, R.; Davison, J.; Moore, L.; Wang, H. Improving immunisation timeliness in aboriginal children through personalised calendars. BMC Public Health 2013, 13, 598. [Google Scholar] [CrossRef] [Green Version]
- Kanno, T.; Wada, H. Study of vaccination history of children entering elementary school (from 2 school registration in Morioka years S61 and 62) [in Japanese]. Jpn. Med. J. 1988, 3335, 30–34. [Google Scholar]
- Shimizu, I. Introducing a maternal child health handbook in the province of Dajabón, Dominican Republic: Prospects and issues from the perspectives of sustainability and replicability [in Japanese]. J. Int. Health. 2007, 22, 153–161. [Google Scholar]
- Ogasawara, T. Issues of MCH handbook utilization during disasters [in Japanese]. Jpn. J. Telemed. Telecare 2016, 12, 102–104. [Google Scholar]
- Kawakatsu, Y.; Sugishita, T.; Oruenjo, K.; Wakhule, S.; Kibosia, K.; Were, E.; Honda, S. Effectiveness of and factors related to possession of a mother and child health handbook: An analysis using propensity score matching. Health Educ. Res. 2015, 30, 935–946. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Y.Y.; Leith, W.M.; Li, H.; Tom, J.O. Personal health record use for children and health care utilization: Propensity score-matched cohort analysis. J. Am. Med. Inform. Assoc. 2015, 22, 748–754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bjerkeli Grøvdal, L.; Grimsmo, A.; Ivar Lund Nilsen, T. Parent-held child health records do not improve care: A randomized controlled trial in Norway. Scand. J. Prim. Health Care 2006, 24, 186–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mudany, M.A.; Sirengo, M.; Rutherford, G.W.; Mwangi, M.; Nganga, L.W.; Gichangi, A. Enhancing maternal and child health using a combined mother & child health booklet in Kenya. J. Trop. Pediatr. 2015, 61, 442–447. [Google Scholar]
- Nakazawa, M.; Takahashi, S.; Sato, T.; Ishikawa, K. The relationship between the result of diagnosis after neonatal hearing screening and the achievement of the hearing development checklist [in Japanese]. Audiol. Jpn. 2007, 50, 113–121. [Google Scholar] [CrossRef]
- Bhuiyan, S.; Nakamura, Y.; Qureshi, N. Study on the development and assessment of maternal and child health (MCH) handbook in Bangladesh. J. Public Health Dev. 2006, 4, 45–59. [Google Scholar]
- Tom, J.O.; Chen, C.; Zhou, Y.Y. Personal health record use and association with immunizations and well-child care visits recommendations. J. Pediatr. 2014, 164, 112–117. [Google Scholar] [CrossRef]
- Moore, J.; Brindle, A.; Goraya, P.; Monk, S.; Rennie, D.; Tamhne, R.; Watterson, J.; Stretch, D. A personal child health record for children with a disability. Ambulatory Child. Health 2000, 6, 261–267. [Google Scholar] [CrossRef]
- Yahata, H.; Tanaka, T. How to improve the measles vaccination rate? [in Japanese]. J. Jpn. Soc. Health Educ. Health Promot. 2005, 13, 286–287. [Google Scholar]
- Oguchi, T.; Kumakura, M. Measles and rubella—Vaccine use and strategies for their elimination in “A” prefecture, Japan [in Japanese]. Bull. Dokkyo Med. Univ. School Nurs. 2014, 7, 1–9. [Google Scholar]
- Kamiya, S.; Kumita, A.; Okamoto, K.; Shimizu, N.; Komatsu, M. Childrearing mother’s state and difficulties faced when gathering vaccination information [in Japanese]. Bull. Aichi Prefect. Coll. Nurs. Health 2016, 22, 37–44. [Google Scholar]
- Hagiwara, A.; Ueyama, M.; Ramlawi, A.; Sawada, Y. Is the maternal and child health (MCH) handbook effective in improving health-related behavior? Evidence from Palestine. J. Public Health Policy 2013, 34, 31–45. [Google Scholar] [CrossRef] [PubMed]
- Aiga, H.; Nguyen, V.D.; Nguyen, C.D.; Nguyen, T.T.; Nguyen, L.T. Knowledge, attitude and practices: Assessing maternal and child health care handbook intervention in Vietnam. BMC Public Health 2016, 16, 129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamagiwa, I.; Akiyama, T. The questionnaire survey on the level of knowledge and interest about biliary atresia of pregnant women [in Japanese]. Niigata Seiryo Acad. Soc. 2009, 1, 113–119. [Google Scholar]
- Hirayama, Y.; Naito, S.; Iinuma, Y.; Hashizume, N.; Iida, H.; Nitta, K. A strategy for the early detection of biliary atresia by appending the stool color card to the maternal and child health handbook [in Japanese]. J. Jpn. Soc. Perinat. Neonat. Med. 2011, 47, 78–81. [Google Scholar]
- Yokoi, A.; Isono, K. Examination of the usefulness of stool color card in early detection of biliary atresia [in Japanese]. J. Jpn. Soc. Pediatric Surg. 2019, 55, 945–950. [Google Scholar]
- Ichikawa, M. Arial relationship between mother’s knowledge of the SIDS and a child-rearing source [in Japanese]. Bull. Hokkaido Univ. Sci. 2016, 41, 55–60. [Google Scholar]
- Nokubo, M.; Okabe, M.; Miyata, S.; Sakurai, S. Mothers’ awareness on the prevention of infant accidents [in Japanese]. Mie Nurs. J. 2006, 8, 75–86. [Google Scholar]
- Brown, D.W.; Tabu, C.; Sergon, K.; Shendale, S.; Mugoya, I.; Machekanyanga, Z.; Okoth, P.; Onuekwusi, I.U.; Ogbuanu, I.U. Home-based record (HBR) ownership and use of HBR recording fields in selected Kenyan communities: Results from the Kenya missed opportunities for vaccination assessment. PLoS ONE 2018, 13, e0201538. [Google Scholar] [CrossRef]
- Enokido, F.; Iizuka, T. Study on MCH handbook use [in Japanese]. Jpn J. Matern Health. 1965, 6, 18–20. [Google Scholar]
- Fujimoto, M.; Nakamura, Y.; Ikeda, M.; Takeda, Y.; Higurashi, M. Study on MCH handbook utilization [in Japanese]. Jpn. J. Public Health 2001, 48, 486–494. [Google Scholar]
- Hamilton, L.; Wyver, S. Parental use and views of the child personal health record. Aust. Educ. Dev. Psychol. 2012, 29, 66–77. [Google Scholar] [CrossRef]
- Araujo, E.M.N.d.; Gouveia, M.T.d.O.; Pedraza, D.F. Use of a child health surveillance instrument focusing on growth. A cross-sectional study. Sao Paulo Med J. 2017, 135, 541–547. [Google Scholar] [CrossRef] [Green Version]
- Hokama, T.; Hamamoto, I.; Oomine, F.; Sakamoto, R.; Takeda, M. Second report on the study of MCH handbook utilization—from the results of a survey of mothers of 3-5 months old children [in Japanese]. Jpn. J. Matern. Health 2000, 41, 336–339. [Google Scholar]
- Aoki, M.; Kasuya, K.; Fujimaki, W. Attempt to optimize the usage of the maternal and child health handbook using a questionnaire survey of guardians of preschool child [in Japanese]. J. Child. Health 2009, 68, 575–582. [Google Scholar]
- Shibahara, M. Support for infants with lower limb disability living at home: Creation of a health and living log [in Japanese]. Rigakuryoho Kagaku 2010, 25, 693–697. [Google Scholar] [CrossRef] [Green Version]
- Fujii, M.; Sato, T. Perception regarding maternal and child health handbook of mothers who gave birth to twins [in Japanese]. J. Jpn. Red Cross Soc. Nurs. Sci. 2020, 20, 52–60. [Google Scholar]
- Dagvadorj, A.; Nakayama, T.; Inoue, E.; Sumya, N.; Mori, R. Cluster randomised controlled trial showed that maternal and child health handbook was effective for child cognitive development in Mongolia. Acta Paediatr. 2017, 106, 1360–1361. [Google Scholar] [CrossRef]
- Osaki, K.; Hattori, T.; Kosen, S. The role of home-based records in the establishment of a continuum of care for mothers, newborns, and children in Indonesia. Glob. Health Action 2013, 6, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Yuge, M.; Kawasaki, K.; Maruyama, Y.; Kinjo, H. The utility and its factor of the maternal and child health handbook—Survey on mothers’ consciousness with 4 months, 18 months, or three-year-old children [in Japanese]. Jpn. J. Health Sci. Res. 2010, 4, 65–72. [Google Scholar]
- Adachi, M.; Hori, H.; Komada, Y. Evaluation of the usefulness of the maternal and child health handbook in continuous care developed in the Kinan area of Mie Prefecture [in Japanese]. J. Child Health 2010, 69, 325–328. [Google Scholar]
- World Health Organization. Towards a Grand Convergence for Child Survival and Health. Available online: https://apps.who.int/iris/bitstream/handle/10665/251855/WHO-MCA-16.04-eng.pdf (accessed on 21 May 2021).
- Chutiyami, M.; Wyver, S.; Amin, J. Are parent-held child health records a valuable health intervention? A systematic review and Meta-Analysis. Int. J. Environ. Res. Public Health 2019, 16, 220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.; Welch, V. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]



{kind=link}
{kind=link}
| Outcome | Intervention | No Effect, (n) | Mixed Effect, (n) | Positive Effect, n (%) | Total Times Outcome Reported, (n) |
|---|---|---|---|---|---|
| Newborn care seeking | |||||
| Care seeking for newborn complications [6] | MCH handbook | 1 | 0 | 0 (0) | 1 |
| Care seeking after delivery [30] | MCH handbook | 0 | 0 | 1 (100) | 1 |
| Use of laboratory services [31] | RTH booklet | 0 | 0 | 1 (100) | 1 |
| Total (newborn care seeking) | 1 | 0 | 2 (67) | 3 | |
| Newborn care knowledge | |||||
| Immediate breastfeeding [32,33] | MCH handbook | 0 | 0 | 2 (100) | 2 |
| Giving colostrum [32] | MCH handbook | 0 | 0 | 1 (100) | 1 |
| Exclusive breastfeeding Duration [32] | MCH handbook | 0 | 0 | 1 (100) | 1 |
| Use of antibiotic for eyes [32] | MCH handbook | 0 | 0 | 1 (100) | 1 |
| Hepatitis B immunization at birth [32] | MCH handbook | 0 | 0 | 1 (100) | 1 |
| Thermal protection [32] | MCH handbook | 0 | 0 | 1 (100) | 1 |
| Cord care [32] | MCH handbook | 0 | 0 | 1 (100) | 1 |
| Recognize the danger signs in newborns [32] | MCH handbook | 0 | 0 | 1 (100) | 1 |
| Total (newborn care knowledge) | 0 | 0 | 9 (100) | 9 | |
| Newborn care practices | |||||
| Immediate breastfeeding [7,34] | MCH handbook; maternity case notes | 2 | 0 | 0 (0) | 2 |
| Good newborn care and self-care [28,32] | MCH handbook; home-based maternal record | 0 | 0 | 2 (100) | 2 |
| Total (newborn care practices) | 2 | 0 | 2 (50) | 4 | |
| Perinatal mortality and morbidity | |||||
| Neonatal deaths [7,34] | MCH handbook; maternity case notes | 2 | 0 | 0 (0) | 2 |
| APGAR score [7] | MCH handbook | 1 | 0 | 0 (0) | 1 |
| Total (perinatal mortality and morbidity) | 3 | 0 | 0 (0) | 3 |
| Outcome | Intervention | No Effect, (n) | Mixed Effect, (n) | Positive Effect, n (%) | Total Times Outcome Reported, (n) |
|---|---|---|---|---|---|
| Vaccination use/uptake | |||||
| DTP3 completion [35,36,37,38] | Home-based health record booklet; educational immunization cards; redesigned immunization card | 2 | 0 | 2 (50) | 4 |
| Rotavirus vaccination [39] | MCH handbook | 0 | 1 | 0 (0) | 1 |
| BCG and polio vaccination [40] | MCH handbook | 0 | 1 | 0 (0) | 1 |
| Mumps, measles, chickenpox [41] | MCH handbook | 0 | 1 | 0 (0) | 1 |
| Total (vaccination use/uptake) | 2 | 3 | 2 (29) | 7 | |
| Vaccination history/records [42,43,44,45,46,47,48,49,50] | MCH handbook; personal health record; personal child health record and advice booklet; individually tailored calendar; child health card; patient-held vaccination records; personalized calendar | 0 | 1 | 8 (89) | 9 |
| Childcare seeking | |||||
| Care seeking for child Illnesses [6,51,52,53] | MCH handbook; personal health record; parent-held child health record | 2 | 0 | 2 (50) | 4 |
| Use of healthcare and laboratory Services [53,54,55] | MCH handbook; parent-held child health record | 1 | 0 | 2 (67) | 3 |
| Adherence to recommended Immunizations [56,57] | MCH handbook; personal health record | 0 | 0 | 2 (100) | 2 |
| Adherence to childcare visit Recommendations [57] | Personal health record | 0 | 0 | 1 (100) | 1 |
| Total (childcare seeking) | 3 | 0 | 7 (70) | 10 | |
| Child healthcare knowledge | |||||
| General health [51,53,58] | MCH handbook; personal child health record; parent-held child health record | 2 | 0 | 1 (33) | 3 |
| Immunization [32,56,59,60,61] | MCH handbook | 3 | 1 | 1 (20) | 5 |
| Exclusive breastfeeding [56,62,63] | MCH handbook | 0 | 0 | 3 (100) | 3 |
| Detection of biliary atresia [64,65,66] | MCH handbook stool card | 0 | 2 | 1 (33) | 3 |
| Sudden infant death syndrome [67] | MCH handbook | 0 | 1 | 0 (0) | 1 |
| Accident prevention of infant [68] | MCH handbook | 0 | 0 | 1 (100) | 1 |
| Total (child healthcare knowledge) | 5 | 4 | 7 (44) | 16 | |
| Child healthcare practices | |||||
| Exclusive breastfeeding [6,56,63] | MCH handbook | 1 | 0 | 2 (67) | 3 |
| Continued breastfeeding [6] | MCH handbook | 0 | 0 | 1 (100) | 1 |
| Complementary feeding [6] | MCH handbook | 0 | 0 | 1 (100) | 1 |
| Proper feeding order [6] | MCH handbook | 0 | 0 | 1 (100) | 1 |
| Varied foods feeding [6] | MCH handbook | 0 | 0 | 1 (100) | 1 |
| Complementary feeding [6] | MCH handbook | 0 | 0 | 1 (100) | 1 |
| Proper feeding order [6] | MCH handbook | 0 | 0 | 1 (100) | 1 |
| Varied foods feeding [6] | MCH handbook | 0 | 0 | 1 (100) | 1 |
| Self-feeding training [6] | MCH handbook | 0 | 0 | 1 (100) | 1 |
| Recording immunizations [35,45,69,70,71] | MCH handbook; home-based health record booklet; child health record; home-based record | 1 | 2 | 2 (40) | 5 |
| Growth monitoring [45,70,72,73,74,75,76,77] | MCH handbook; child health card; child personal health record; child health handbook; health and living log | 3 | 2 | 4 (44) | 9 |
| Total (child healthcare practices) | 5 | 4 | 13 (59) | 22 | |
| Infant and child illness management | |||||
| Home care for cough [6] | MCH handbook | 0 | 0 | 1 (100) | 1 |
| Home care for diarrhea [6,49] | MCH handbook | 1 | 0 | 1 (50) | 2 |
| Vitamin A use [6,56] | MCH handbook | 0 | 0 | 2 (100) | 2 |
| Total (infant and child illness management) | 1 | 0 | 4 (80) | 5 | |
| Child mortality and morbidity | |||||
| Underweight children [6] | MCH handbook | 0 | 0 | 1 (100) | 1 |
| Stunted growth [6] | MCH handbook | 0 | 0 | 1 (100) | 1 |
| Wasting [6] | MCH handbook | 1 | 0 | 0 (0) | 1 |
| Risk of cognitive delay [78] | MCH handbook | 0 | 0 | 1 (100) | 1 |
| Total (child mortality and morbidity) | 1 | 0 | 3 (75) | 4 | |
| Continuum of care [6,28,30,49,63,79,80,81] | MCH handbook; home-based maternal record | 0 | 1 | 7 (88) | 8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carandang, R.R.; Sakamoto, J.L.; Kunieda, M.K.; Shibanuma, A.; Yarotskaya, E.; Basargina, M.; Jimba, M. Roles of the Maternal and Child Health Handbook and Other Home-Based Records on Newborn and Child Health: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 7463. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147463
Carandang RR, Sakamoto JL, Kunieda MK, Shibanuma A, Yarotskaya E, Basargina M, Jimba M. Roles of the Maternal and Child Health Handbook and Other Home-Based Records on Newborn and Child Health: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(14):7463. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147463
Chicago/Turabian StyleCarandang, Rogie Royce, Jennifer Lisa Sakamoto, Mika Kondo Kunieda, Akira Shibanuma, Ekaterina Yarotskaya, Milana Basargina, and Masamine Jimba. 2021. "Roles of the Maternal and Child Health Handbook and Other Home-Based Records on Newborn and Child Health: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 14: 7463. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147463