
Ontological Analysis of COVID-19 Vaccine Roll out Strategies: A Comparison of India and the United States of America


Abstract
:1. Introduction
2. Materials and Methods
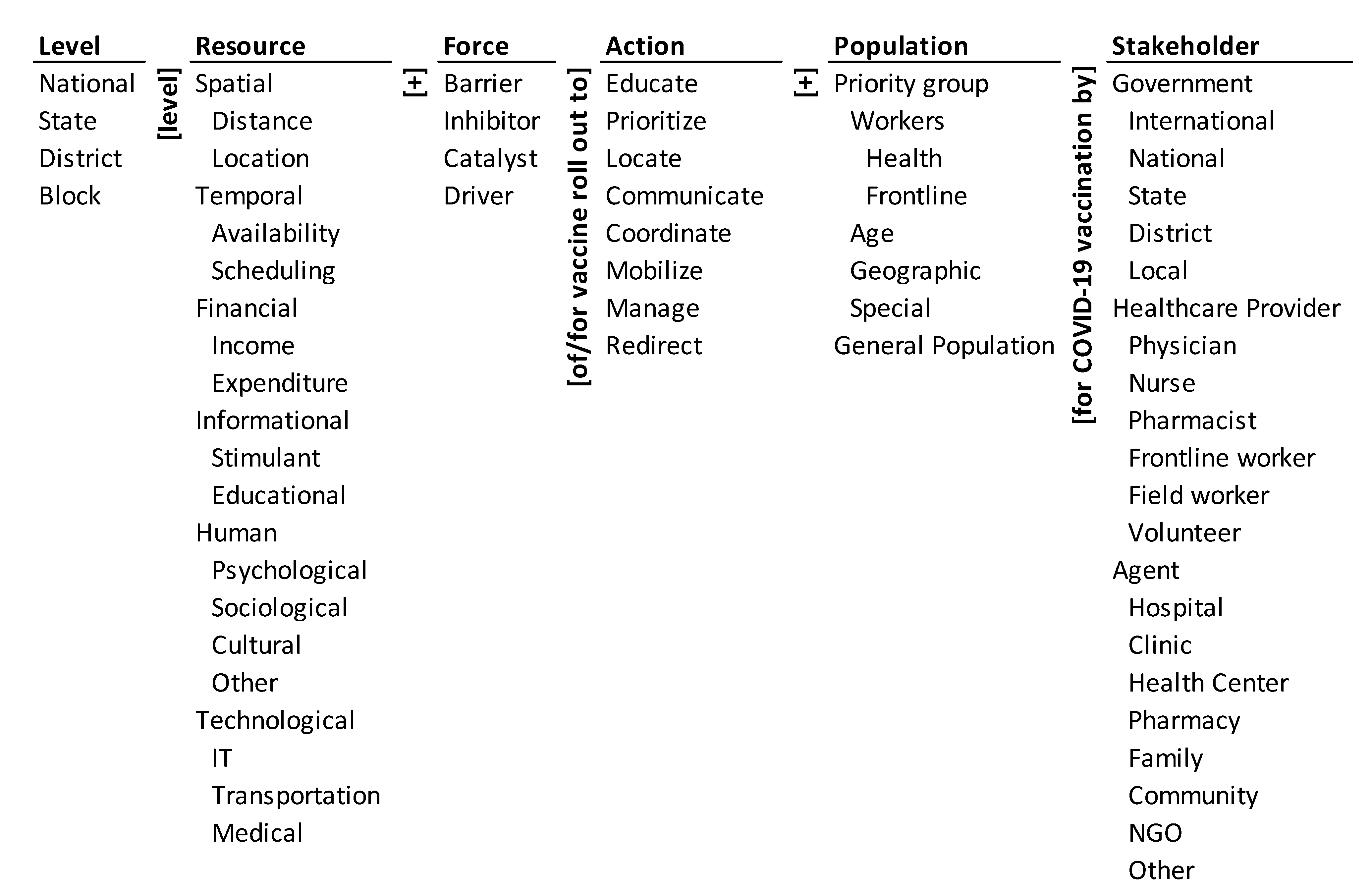
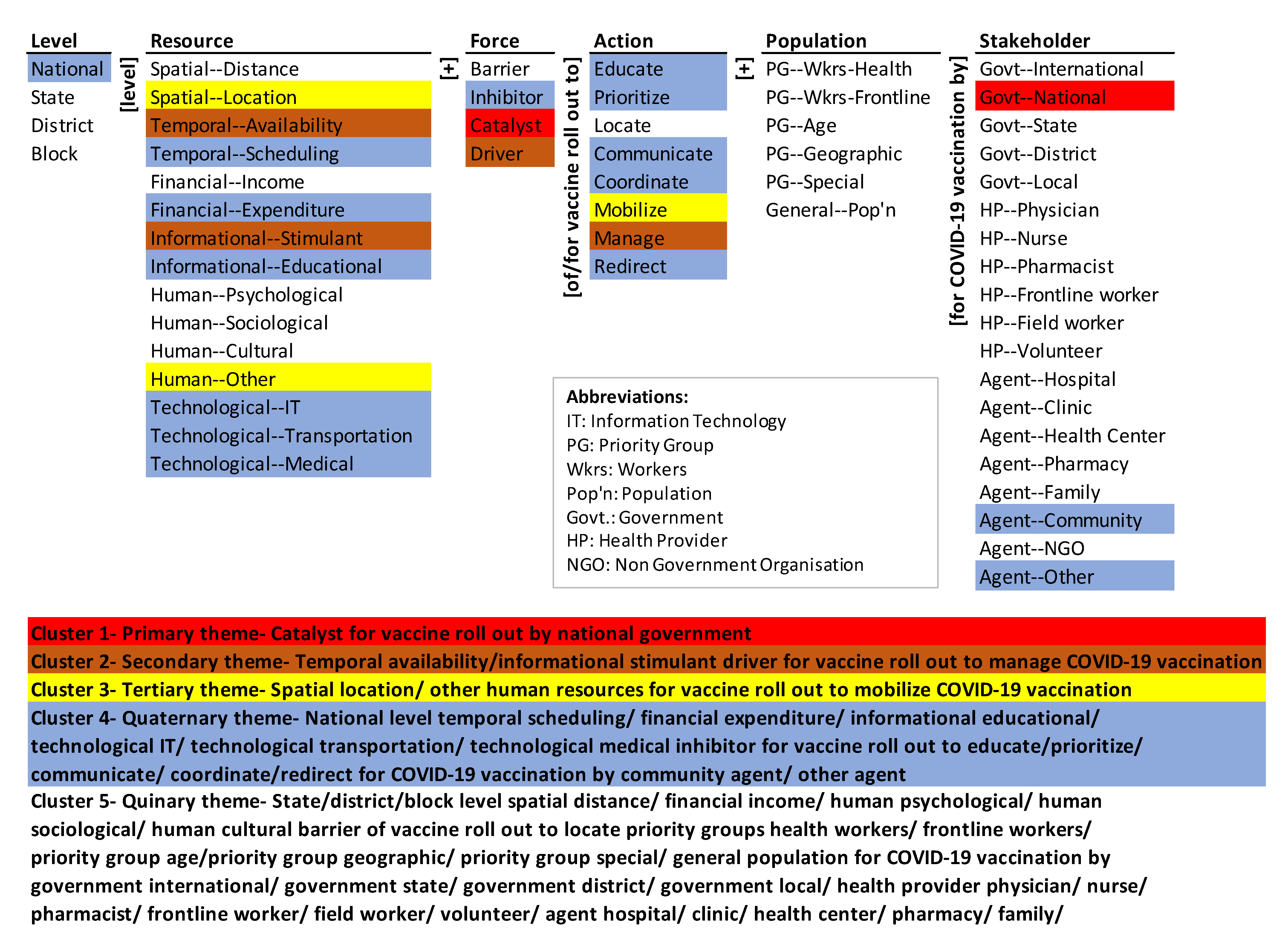
2.1. Ontology of COVID-19 Vaccine Roll Out
- National level spatial distance barrier for vaccine roll out to educate priority group workers health for COVID-19 vaccination by national government.
- Block level technological medical driver for vaccine rollout to redirect general population for COVID-19 vaccination by NGO.
2.2. Method
2.3. Mapping
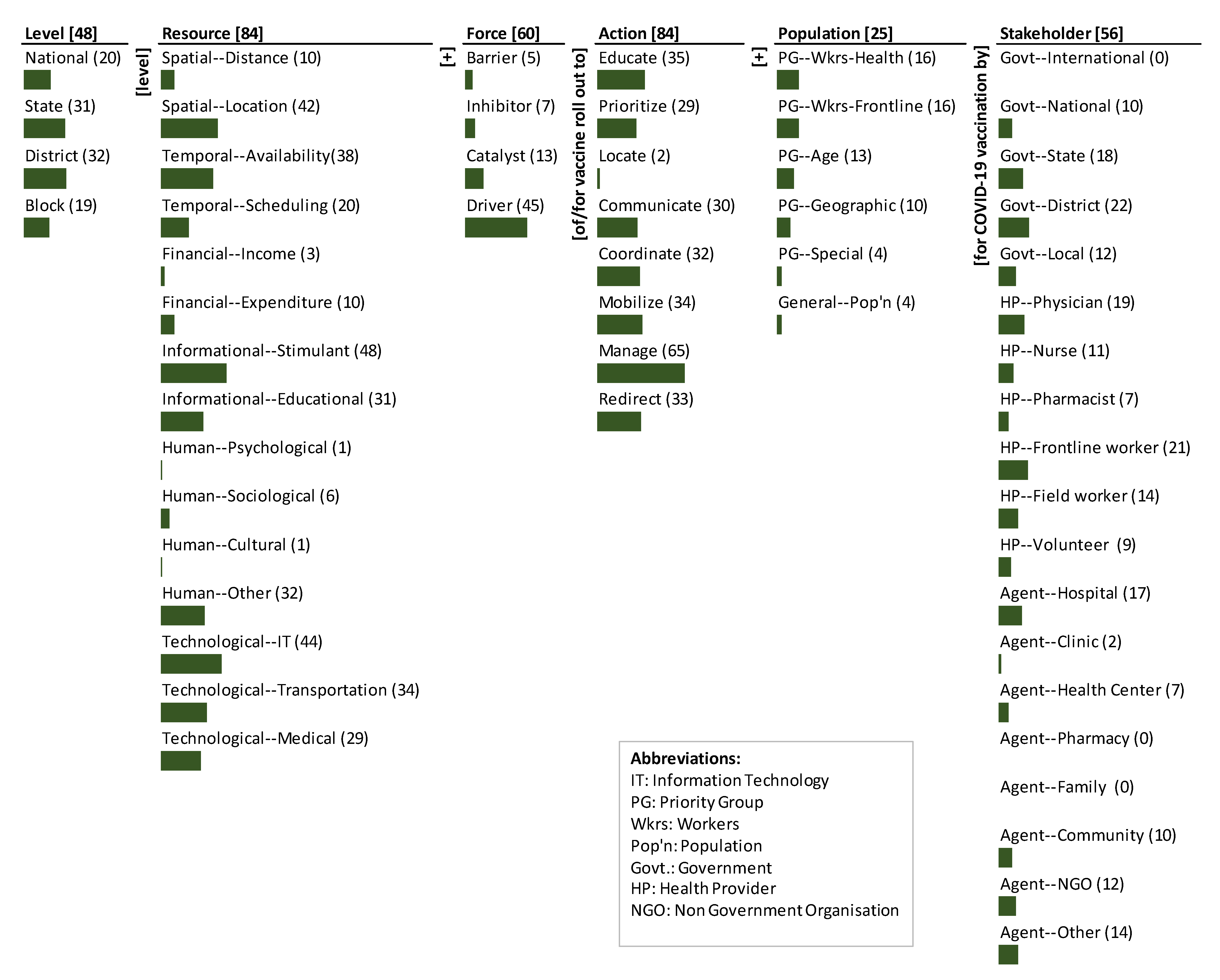
3. Results
3.1. India’s Monads Map
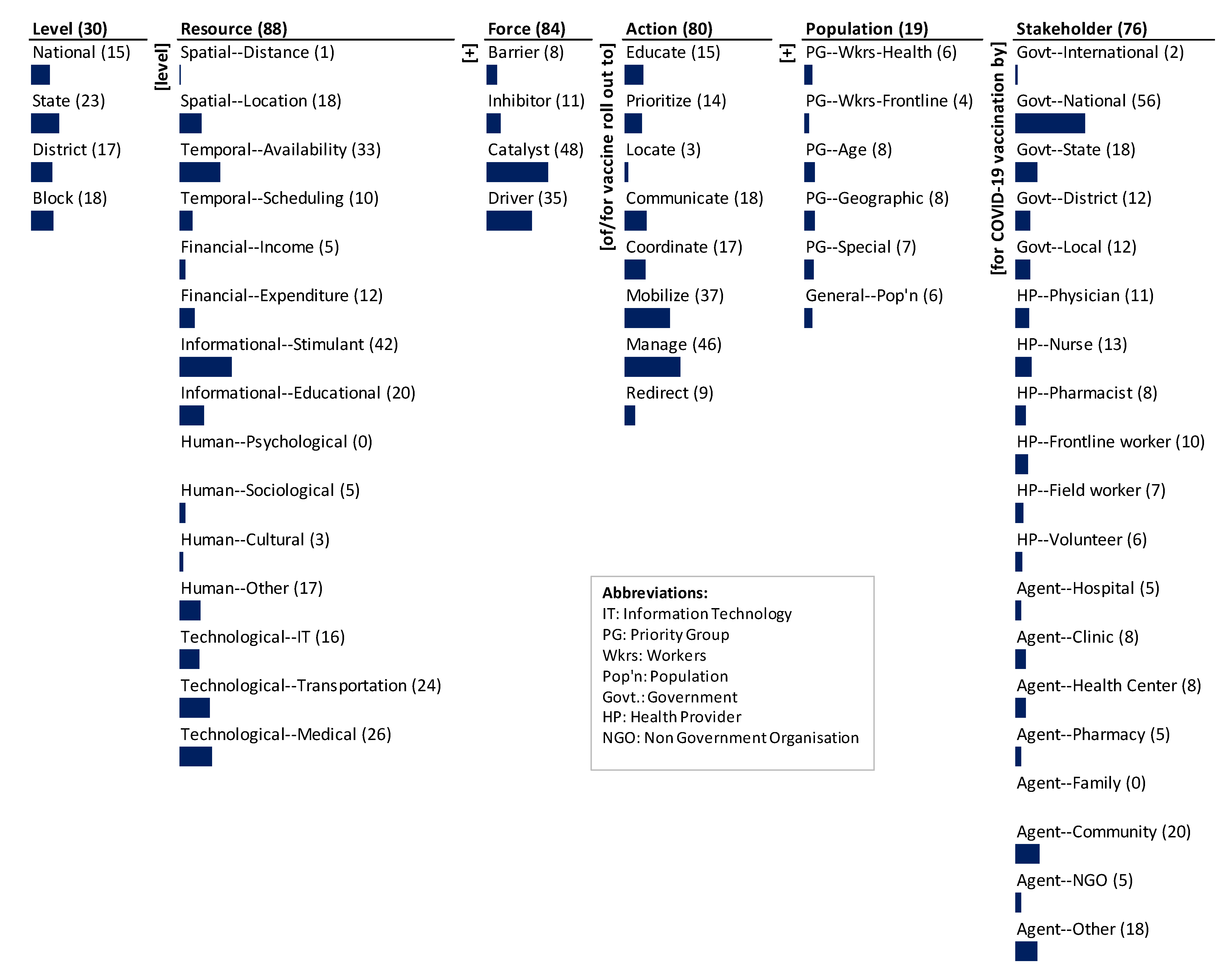
3.2. The U.S. Monads Map
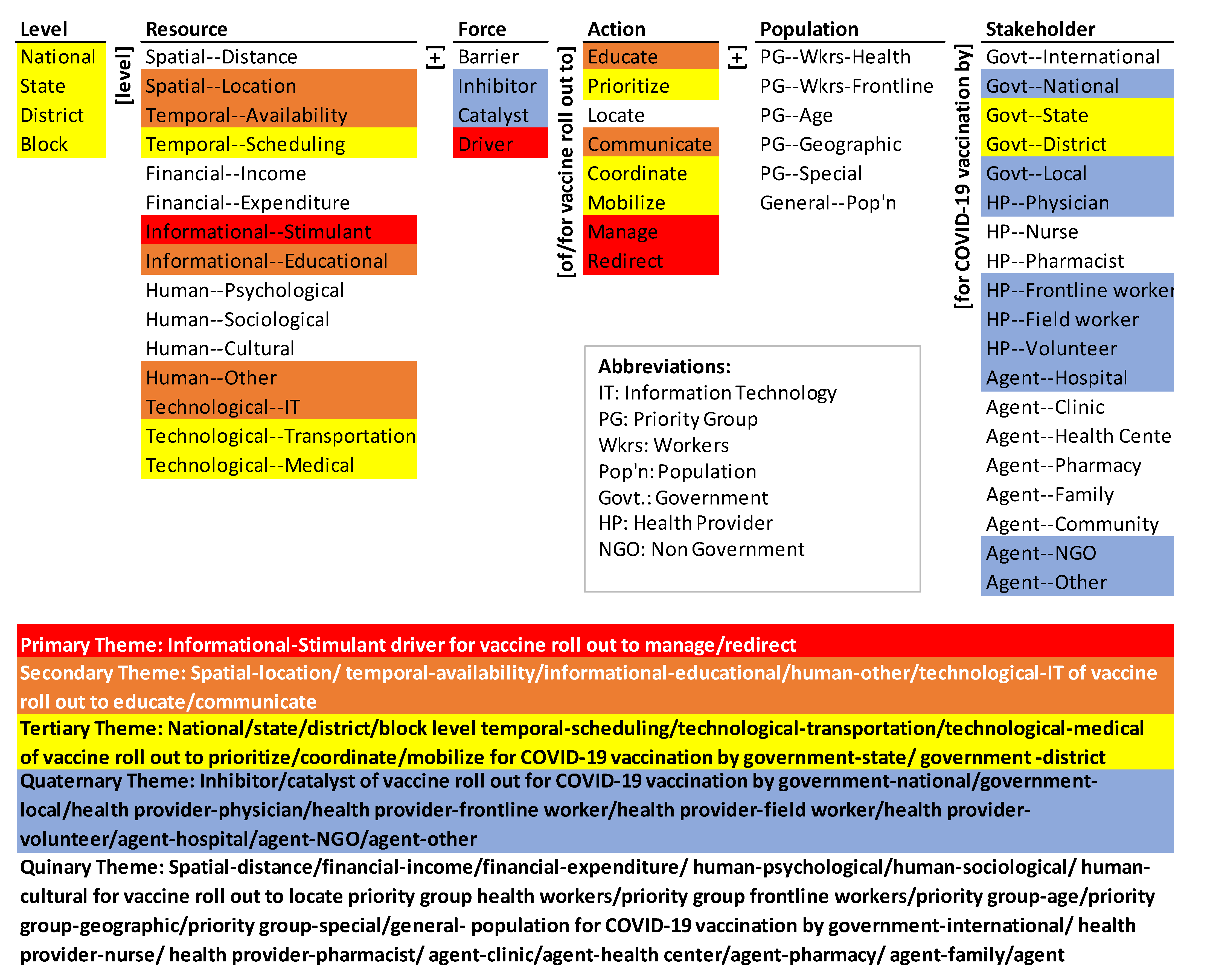
3.3. Theme Maps
3.3.1. India’s Themes Map
3.3.2. The U.S. Themes Map
4. Discussion
4.1. India’s COVID-19 Vaccines Operational Guidelines—Emphases and Gaps
4.2. The U.S. National Strategy for the COVID-19 Response and Pandemic Preparedness—Emphases and Gaps
4.3. Comparison of India’s COVID-19 Vaccines Operational Guidelines and the U.S. National Strategy for the COVID-19 Response
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
| Level: Level of jurisdiction and activities |
| National: National jurisdiction and national-level activities |
| State: State jurisdiction and state-level activities |
| District: District jurisdiction and district-level activities |
| Block: Block jurisdiction and block-level activities |
| Resources: a source or supply of from the provider to the recipient |
| Spatial: The geographical proximity of the recipient and provider for vaccine roll out |
| Distance: The physical proximity between the provider and recipient for vaccine roll out |
| Location: The place or position of the recipient and provider for vaccine roll out |
| Temporal: The timely availability and scheduling of resources for vaccine roll out |
| Availability: Obtaining or use of resources at a particular time by providers and recipients for vaccine roll out |
| Scheduling: Arranging or planning resources at a particular time by providers and recipients for vaccine roll out |
| Financial: The ability to afford and compensate for the direct and opportunity costs to access vaccine |
| Income: Money earned through wages/salary for paying the direct and opportunity costs to access vaccine |
| Expenditure: The amount of money spent for paying the direct and opportunity costs to access vaccine |
| Informational: Informational education provided to encourage the recipient and the benefits of for vaccine roll out |
| Stimulant: The incentive to recipients and the benefits of doing so |
| Educational: Educating the recipients and the benefits of doing so |
| Human: People seeking and, hence, accessing, and receiving and being able to access vaccine for vaccine roll out |
| Psychological: People’s mental and emotional state shaping their knowledge of, perception of, attitude towards, and actions for vaccine roll out |
| Sociological: Development, structure, and functioning of human society shaping people’s knowledge, perception, attitude, and action for vaccine roll out |
| Cultural: People’s ideas, customs and social behavior shaping their knowledge of, perception of, attitude towards, and actions for vaccine roll out |
| Other: Other-people factor shaping their knowledge of, perception of, attitude towards, and actions for vaccine roll out |
| Technological: The use of technology to transform the challenges of access to vaccine for vaccine roll out |
| IT: Computing technology such as networking, hardware, software, the internet, or the people that transform the challenges for vaccine roll out |
| Transportation: Use of technology for the movement of vaccine to the recipient and provider for vaccine roll out |
| Medical: Use of technology to practice medicine for vaccine roll out |
| Force: Strength or energy as an attribute of physical actions or movement |
| Barrier: An obstacle for vaccine roll out |
| Inhibitor: Slowing down or limiting vaccine roll out |
| Catalyst: Increase or precipitating vaccine roll out |
| Driver: Propelling or controlling vaccine roll out |
| Action: Steps or mechanisms undertaken for vaccine roll out |
| Educate: Actions to educate/train about COVID-19 vaccination. For example, education and training regarding vaccine administrations to frontline workers, ASHA workers. |
| Prioritize: Actions to prioritize for vaccine roll out |
| Locate: Actions to locate for vaccine roll out |
| Communicate: Actions to communicate/sensitize about COVID-19 vaccination for vaccine roll out |
| Coordinate: Actions to coordinate for vaccine roll out. For example, interdepartmental or intersectoral coordination |
| Mobilize: Actions to mobilize vaccine roll out |
| Manage: Actions to manage vaccine roll out, which include registration, allocation, administration, and monitoring |
| Redirect: Actions to redirect vaccine roll out, which include reviewing, evaluation, and follow-ups |
| Population: Target population and a group of people with a common characteristic |
| Priority group: Target group based on special priority |
| Workers: Priority group involving different workers |
| Health: Health workers as a priority group |
| Frontline: Frontline workers as a priority group |
| Age: Priority group based on age brackets or groups |
| Geographic: Priority group based on geographic location |
| Special: Priority group based on special categories such as tribals, underserved population, indigenous population etc. |
| General Population: General and rest of the population |
| Stakeholder: People, institutions, entities employed/involved in carrying actions for vaccine roll out |
| Government: Government agencies involved in vaccine roll out |
| International: International inter-governmental agencies involved directly or indirectly in vaccine roll out |
| National: Union government ministries, agencies, personnel involved directly or indirectly in vaccine roll out |
| State: State government departments, agencies, personnel involved directly or indirectly in vaccine roll out |
| District: District government departments, agencies, personnel involved directly or indirectly in vaccine roll out |
| Local: Local government departments, agencies, personnel involved directly or indirectly in vaccine roll out |
| Healthcare Provider: Healthcare personnel involved directly or indirectly in vaccine roll out |
| Physician: A person qualified to practice medicine |
| Nurse: A person formally educated and trained in the care of the sick or infirm who may even help doctors in treatment |
| Pharmacist: A person who is professionally qualified to prepare and dispense medicinal drugs |
| Frontline worker: Persons serving in healthcare settings directly and indirectly for patient care that have the potential for direct or indirect risk |
| Field worker: Non-medical staff serving in activities related to vaccine roll out. For example, teachers and other support staff |
| Volunteer: Persons who freely offer to take part in an enterprise or undertake a task for vaccine roll out |
| Agent: Public or private agents individual or entities involved in vaccine roll out |
| Hospital: Public or private medical hospitals |
| Clinic: Health facility for outpatient care |
| Health Center: Local establishment housing local medical services or the practice of a group of doctors |
| Pharmacy: A shop or hospital dispensary where medicinal drugs are prepared or sold |
| Family: A social group made up of parents and their children |
| Community: A group of people living in the same place or having a particular characteristic in common |
| NGO: Healthcare organization which is a legal entity that seeks charitable and philanthropic funds |
| Other: Other public or private agents involved in vaccine roll out |
References
- Mulberry, N.; Tupper, P.; Kirwin, E.; McCabe, C.; Colijn, C. Vaccine Rollout Strategies: The Case for Vaccinating Essential Workers Early. medRxiv 2021. [Google Scholar] [CrossRef]
- Kaur, S.P.; Gupta, V. COVID-19 Vaccine: A comprehensive status report. Virus Res. 2020, 288, 198114. [Google Scholar] [CrossRef]
- Cagle, T. Until now, what’s the quickest a vaccine has ever been developed? Nautilus, 24 May 2020. [Google Scholar]
- Ball, P. The lightning-fast quest for COVID vaccines—And what it means for other diseases. Nature 2020, 589, 16–18. [Google Scholar] [CrossRef]
- Blanding, M. The High Cost of the Slow COVID Vaccine Rollout. Available online: http://hbswk.hbs.edu/item/the-high-cost-of-the-slow-covid-vaccine-rollout (accessed on 27 May 2021).
- McMorrow, S.; Thomas, T.W. Historic Vaccination Patterns Provide Insights for COVID-19 Vaccine Rollout; Urban Institute: Washington, DC, USA, 2021; Volume 11. [Google Scholar]
- Mathieu, E.; Ritchie, H.; Ortiz-Ospina, E.; Roser, M.; Hasell, J.; Appel, C.; Giattino, C.; Rodés-Guirao, L. A global database of COVID-19 vaccinations. Nat. Hum. Behav. 2021. [Google Scholar] [CrossRef]
- Burki, T.K. Challenges in the rollout of COVID-19 vaccines worldwide. Lancet Respir. Med. 2021, 9, e42–e43. [Google Scholar] [CrossRef]
- Hardt, K.; Bonanni, P.; King, S.; Santos, J.I.; El-Hodhod, M.; Zimet, G.D.; Preiss, S. Vaccine strategies: Optimising outcomes. Vaccine 2016, 34, 6691–6699. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muzumdar, J.M.; Cline, R.R. Vaccine supply, demand, and policy: A primer. J. Am. Pharm. Assoc. 2009, 49, e87–e99. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health and Family Welfare, Government of India. COVID-19 Vaccines Operational Guidelines 2020. Available online: https://www.mohfw.gov.in/pdf/COVID19VaccineOG111Chapter16.pdf (accessed on 10 February 2021).
- The Biden Administration, United States of America. United States National Strategy for the COVID-19 Response and Pandemic Preparedness 2021. Available online: https://www.whitehouse.gov/wp-content/uploads/2021/01/National-Strategy-for-the-COVID-19-Response-and-Pandemic-Preparedness.pdf (accessed on 10 February 2021).
- Ramaprasad, A.; Syn, T. Ontological Meta-Analysis and Synthesis. Commun. Assoc. Inf. Syst. 2015, 37, 138–153. [Google Scholar] [CrossRef] [Green Version]
- Simon, H.A. The Architecture of Complexity. Proc. Am. Philos. Soc. 1962, 106, 467–482. [Google Scholar]
- Cimino, J.J. In defense of the Desiderata. J. Biomed. Inform. 2006, 39, 299–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cameron, J.D.; Ramaprasad, A.; Syn, T. An Ontology of and Roadmap for mHealth Research. Int. J. Med. Inform. 2017, 100, 16–25. [Google Scholar] [CrossRef]
- Chandrasekaran, B.; Josephson, J.R.; Benjamins, V.R. What Are Ontologies, and Why Do We Need Them? IEEE Intell. Syst. 1999, 14, 20–26. [Google Scholar] [CrossRef] [Green Version]
- Gruber, T.R. Toward Principles for the Design of Ontologies Used for Knowledge Sharing. Int. J. Hum. Comput. Stud. 1995, 43, 907–928. [Google Scholar] [CrossRef]
- Gruber, T.R. Ontology. In Encyclopedia of Database Systems; Liu, L., Özsu, M.T., Eds.; Springer: New York, NY, USA, 2008; ISBN 9780387355443. [Google Scholar]
- Ramaprasad, A. Cognitive Process as a Basis for MIS and DSS Design. Manag. Sci. Manag. Sci. 1987, 33, 139–148. [Google Scholar] [CrossRef]
- Ramaprasad, A.; Mitroff, I.I. On Formulating Strategic Problems. Acad. Manag. Rev. Acad. Manag. Rev. 1984, 9, 597–605. [Google Scholar] [CrossRef]
- Ramaprasad, A.; Poon, E. A Computerized Interactive Technique for Mapping Influence Diagrams (MIND). Strateg. Manag. J. 1985, 6, 377–392. [Google Scholar] [CrossRef]
- Ramaprasad, A. Revolutionary Change and Strategic Management. Behav. Sci. Behav. Sci. 1982, 27, 387–392. [Google Scholar] [CrossRef]
- Ramaprasad, A. On the Definition of Feedback. Behav. Sci. Behav. Sci. 1983, 28, 4–13. [Google Scholar] [CrossRef]
- Quine, W.V.O. From a Logical Point of View, 2nd ed.; Harvard University Press: Boston, MA, USA, 1961. [Google Scholar]
- Nunez, A.; Ramaprasad, A.; Syn, T. National Healthcare Policies in Chile: An Ontological Meta-Analysis. Stud. Health Technol. Inform. 2015, 1105. [Google Scholar] [CrossRef]
- Gadicherla, S.; Krishnappa, L.; Madhuri, B.; Mitra, S.G.; Ramaprasad, A.; Seevan, R.; Sreeganga, S.D.; Thodika, N.K.; Mathew, S.; Suresh, V. Envisioning a learning surveillance system for tuberculosis. PLoS ONE 2020, 15, e0243610. [Google Scholar] [CrossRef]
- Ramaprasad, A.; Singai, C.B.; Hasan, T.; Syn, T.; Thirumalai, M. India’s National Higher Education Policy Recommendations since Independence. J. Educ. Plan. Adm. 2016, 30, 5–24. [Google Scholar]
- Syn, T.; Ramaprasad, A. Megaprojects—Symbolic and Sublime: An Ontological Review. Int. J. Manag. Proj. Bus. 2019, 12, 377–399. [Google Scholar] [CrossRef]
- La Paz, A.; Merigó, J.M.; Powell, P.; Ramaprasad, A.; Syn, T. Twenty-Five Years of the Information Systems Journal: A Bibliometric and Ontological Overview. Inf. Syst. J. 2020, 30, 431–457. [Google Scholar] [CrossRef] [Green Version]
- Kumari, A.; Ranjan, P.; Chopra, S.; Kaur, D.; Kaur, T.; Kalanidhi, K.B.; Goel, A.; Singh, A.; Baitha, U.; Prakash, B.; et al. What Indians Think of the COVID-19 vaccine: A qualitative study comprising focus group discussions and thematic analysis|Elsevier Enhanced Reader. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 679–682. [Google Scholar] [CrossRef]
- Leatherby, L.; Walker, A.S. After a Sluggish Start, Vaccine Rollout Is Improving in Every State. The New York Times, 12 February 2021. [Google Scholar]
- McKee, M.; Rajan, S. What can we learn from Israel’s rapid roll out of COVID 19 vaccination? Isr. J. Health Policy Res. 2021, 10, 5. [Google Scholar] [CrossRef]
- Chandrashekhar, V. India Speeds up Vaccinations as Cases Soar Again. Science 2021, 372, 12–13. Available online: https://www.sciencemag.org/lookup/doi/10.1126/science.372.6537.12 (accessed on 10 February 2021).
- Mills, M.C.; Salisbury, D. The challenges of distributing COVID-19 vaccinations. EClinicalMedicine 2021, 31, 100674. [Google Scholar] [CrossRef]
- Nundy, S.; Kaur, M.; Singh, P. Preparing for and responding to Covid-19′s ‘second hit’. Healthcare 2020, 8, 100461. [Google Scholar] [CrossRef] [PubMed]
- Shet, A.; Dhaliwal, B.; Banerjee, P.; Carr, K.; DeLuca, A.; Britto, C.; Seth, R.; Parekh, B.; Basavaraj, G.V.; Shastri, D.; et al. COVID-19-related disruptions to routine vaccination services in India: A survey of paediatric providers. BMJ Paediatr. Open 2021, 5, e001060. [Google Scholar] [CrossRef] [PubMed]
- Shilo, S.; Rossman, H.; Segal, E. Signals of hope: Gauging the impact of a rapid national vaccination campaign. Nat. Rev. Immunol. 2021, 21, 198–199. [Google Scholar] [CrossRef] [PubMed]
- Wood, S.; Schulman, K. Beyond Politics—Promoting Covid-19 Vaccination in the United States. N. Engl. J. Med. 2021, 384, e23. [Google Scholar] [CrossRef] [PubMed]
- Murthy, B.P.; Sterrett, N.; Weller, D.; Zell, E.; Reynolds, L.; Toblin, R.L.; Murthy, N. Disparities in COVID-19 Vaccination Coverage between Urban and Rural Counties—United States, 14 December 2020–10 April 2021. MMWR Morb. Mortal Wkly. Rep. 2021, 70, 759. [Google Scholar] [CrossRef] [PubMed]
- OECD. Enhancing Public Trust in COVID-19 Vaccination: The Role of Governments 2021; OECD: Paris, France, 2021. [Google Scholar]
- U.S. Department of Health and Human Services; Department of Defense. United States of America From the Factory to the Frontlines The Operation Warp Speed Strategy for Distributing a COVID-19 Vaccine 2020.U.S.; Department of Health and Human Services: Washington, DC, USA; Department of Defense: Washington, DC, USA, 2020; p. 11. [Google Scholar]
- Michaud, J.; Kates, J. Distributing a COVID-19 Vaccine Across the U.S.—A Look at Key Issues—Issue Brief 2020. Available online: https://www.kff.org/report-section/distributing-a-covid-19-vaccine-across-the-u-s-a-look-at-key-issues-issue-brief/ (accessed on 10 February 2021).
- U.S. Food and Drug Administration. Pfizer-BioNTech COVID-19 Vaccine. Available online: https://www.fda.gov/emergency-preparedness-and-response/coronavirus-disease-2019-covid-19/pfizer-biontech-covid-19-vaccine (accessed on 28 May 2021).
- Interlandi, J.; Serkez, Y. What Are the Vaccine Roadblocks Where You Live? The New York Times, 25 February 2021. [Google Scholar]
- Schoch-Spana, M.; Brunson, E.K.; Long, R.; Ruth, A.; Ravi, S.J.; Trotochaud, M.; Borio, L.; Brewer, J.; Buccina, J.; Connell, N.; et al. The public’s role in COVID-19 vaccination: Human-centered recommendations to enhance pandemic vaccine awareness, access, and acceptance in the United States. Vaccine 2020. [Google Scholar] [CrossRef] [PubMed]
- Krouse, S.; Hopkins, J.S.; Mathews, A.W. The Mass Distribution of Covid-19 Vaccines Is Under Way. ‘Everything Has to Come Together’. Wall Street Journal, 13 December 2020. [Google Scholar]
- Hollingsworth, H.; Richmond, T. States Scale back Vaccine Orders as Interest in Shots Wanes. Available online: https://apnews.com/article/coronavirus-pandemic-coronavirus-vaccine-health-ad578143ffb2e934dc32ae200ff594bb (accessed on 28 May 2021).
- Weise, E.; Weintraub, K. Amid a chaotic COVID-19 vaccine rollout, states find ways to connect shots with arms. USA Today, 1 March 2021. [Google Scholar]
- Public Health England. COVID-19 Vaccine Surveillance Strategy; Public Health England: London, UK, 2021; p. 23. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name of the Document | Inclusion Criterion | Exclusion Criterion |
|---|---|---|
| COVID-19 Vaccines Operational Guidelines by the Government of India (GoI) National Strategy for the COVID-19 Response and Pandemic Preparedness by the office of President Joseph R. Biden, Jr. | Strategies/action points specifically pertaining to COVID-19 vaccine roll out | Strategies/action points not pertaining COVID-19 vaccine roll out. For example, Features of Co-WIN website (India’s document) was not considered for coding, since it was not directly related to vaccine roll out. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sreeganga, S.D.; Chandra, A.; Ramaprasad, A. Ontological Analysis of COVID-19 Vaccine Roll out Strategies: A Comparison of India and the United States of America. Int. J. Environ. Res. Public Health 2021, 18, 7483. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147483
Sreeganga SD, Chandra A, Ramaprasad A. Ontological Analysis of COVID-19 Vaccine Roll out Strategies: A Comparison of India and the United States of America. International Journal of Environmental Research and Public Health. 2021; 18(14):7483. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147483
Chicago/Turabian StyleSreeganga, S. D., Ajay Chandra, and Arkalgud Ramaprasad. 2021. "Ontological Analysis of COVID-19 Vaccine Roll out Strategies: A Comparison of India and the United States of America" International Journal of Environmental Research and Public Health 18, no. 14: 7483. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147483