
Community-Level Participation in Volunteer Groups and Individual Depressive Symptoms in Japanese Older People: A Three-Year Longitudinal Multilevel Analysis Using JAGES Data

 , , , ,
, , , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
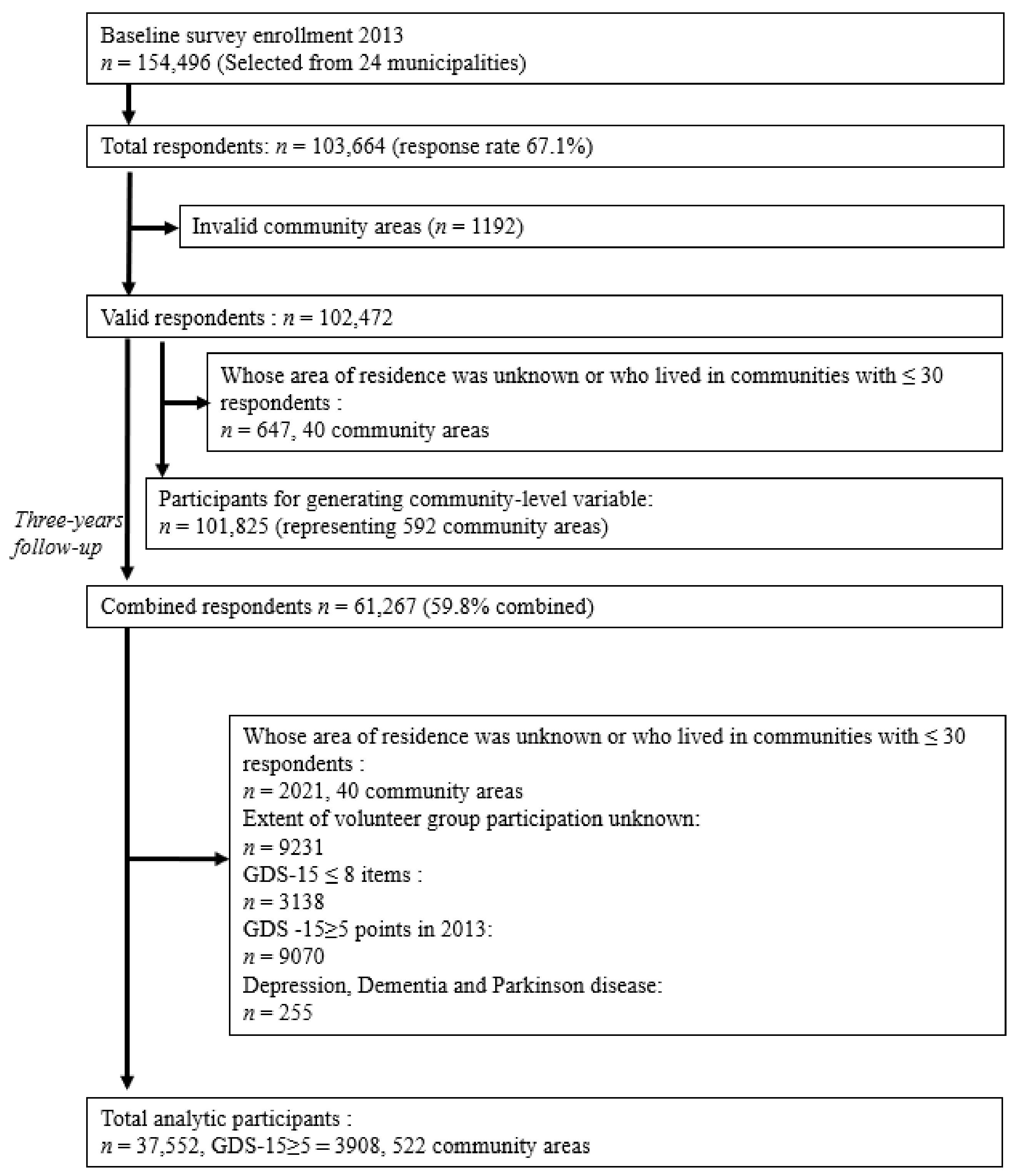
2.1. Study Design and Subjects
2.2. Measurements
2.2.1. Individual-Level Depressive Symptoms
2.2.2. Individual- and Community-Level Participation in Volunteer Groups
2.2.3. Individual-Level Covariates
2.2.4. Community-Level Covariates
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Depression and Other Common Mental Disorders Global Health Estimates. 2017. Available online: https://apps.who.int/iris/bitstream/handle/10665/254610/WHO-MSD-MER-2017.2-eng.pdf;#:~:text=Common mental disorders refer to a range of anxiety and,and 3.6%25 from anxiety disorder (accessed on 20 May 2020).
- Lopez, A.D.; Murray, C.C.J.L. The global burden of disease, 1990–2020. Nat. Med. 1998, 4, 1241–1243. [Google Scholar] [CrossRef]
- Blazer, D.G. Depression in Late Life: Review and Commentary. J. Gerontol. Med. Sci. 2003, 58, M249–M265. Available online: https://0-academic-oup-com.brum.beds.ac.uk/biomedgerontology/article/58/3/M249/684130 (accessed on 20 May 2020). [CrossRef] [PubMed] [Green Version]
- Fiske, A.; Wetherell, J.L.; Gatz, M.; Fiske, A.; Wetherell, J.L.; Gatz, M. Depression in Older Adults. Annu. Rev. Clin. Psychol. 2009, 5, 363–389. [Google Scholar] [CrossRef] [PubMed]
- Livingston, G.; Sommerlad, A.; Orgeta, V.; Costafreda, S.G.; Huntley, J.; Ames, D.; Ballard, C.; Banerjee, S.; Burns, A.; Cohen-Mansfield, J.; et al. Dementia prevention, intervention, and care. Lancet 2017, 390, 2673–2734. [Google Scholar] [CrossRef] [Green Version]
- White Paper on Aging Society. 2020. Available online: https://www8.cao.go.jp/kourei/whitepaper/w-2020/html/zenbun/index.html (accessed on 9 December 2020).
- Sugihara, Y.; Sugisawa, H.; Shibata, H.; Harada, K. Productive Roles, Gender, and Depressive Symptoms: Evidence From a National Longitudinal Study of Late-Middle-Aged Japanese. J. Gerontol. Ser. B 2008, 63, P227–P234. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health. Labour and Welfare. Volunteer Activities. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/hukushi_kaigo/seikatsuhogo/volunteer/index.html (accessed on 6 November 2020).
- Fujiwara, Y.; Sugihara, Y.; Shinkai, S. Effects of volunteer activities on the mental and physical health of the elderly: Significance of volunteer activities for the elderly in community health and welfare. Jpn. J. Public Health 2005, 52, 293–307. [Google Scholar] [CrossRef]
- Thoits, P.A.; Hewitt, L.N. Volunteer Work and Well-Being. J. Health Soc. Behav. 2001, 42, 115–131. [Google Scholar] [CrossRef]
- Musick, M.A.; Wilson, J. Volunteering and depression: The role of psychological and social resources in different age groups. Soc. Sci. Med. 2003, 56, 259–269. [Google Scholar] [CrossRef]
- Lin, N.; Ye, X.; Ensel, W.M. Social Support and Depressed Mood: A Structural Analysis. J. Health Soc. Behav. 2019, 40, 119–134. [Google Scholar] [CrossRef]
- Fujihara, S.; Tsuji, T.; Miyaguni, Y.; Aida, J.; Saito, M.; Koyama, S.; Kondo, K. Does Community-Level Social Capital Predict Decline in Instrumental Activities of Daily Living? A JAGES Prospective Cohort Study. Int. J. Environ. Res. Public Health 2019, 16, 828. [Google Scholar] [CrossRef] [Green Version]
- Nakagomi, A.; Shiba, K.; Hanazato, M.; Kondo, K.; Kawachi, I. Does community-level social capital mitigate the impact of widowhood & living alone on depressive symptoms? A prospective, multi-level study. Soc. Sci. Med. 2020, 259, 113140. [Google Scholar] [CrossRef]
- Tsuji, T.; Miyaguni, Y.; Kanamori, S.; Hanazato, M.; Kondo, K. Community-level Sports Group Participation and Older Individuals’ Depressive Symptoms. Med. Sci. Sports Exerc. 2018, 50, 1199–1205. [Google Scholar] [CrossRef]
- Sauzet, O.; Leyland, A.H. Contextual effects on health inequalities: A research agenda. Eur. J. Public Health 2017, 27, 587–588. [Google Scholar] [CrossRef] [Green Version]
- Saito, M.; Kondo, N.; Aida, J.; Kawachi, I.; Koyama, S.; Ojima, T.; Kondo, K. Development of an instrument for community-level health related social capital among Japanese older people: The JAGES Project. J. Epidemiol. 2017, 27, 221–227. [Google Scholar] [CrossRef]
- Yamaguchi, M.; Inoue, Y.; Shinozaki, T.; Saito, M.; Takagi, D.; Kondo, K.; Kondo, N. Community Social Capital and Depressive Symptoms Among Older People in Japan: A Multilevel Longitudinal Study. J. Epidemiol. 2019, 29, 363–369. [Google Scholar] [CrossRef] [Green Version]
- Park, M.-J. Impact of social capital on depression trajectories of older women in Korea. Aging Ment. Health 2017, 21, 354–361. [Google Scholar] [CrossRef]
- Kondo, K.; Rosenberg, M. (Eds.) Advancing Universal Health Coverage through Knowledge Translation for Healthy Ageing Lessons Learnt from the Japan Gerontological Evaluation Study: Lessons Learnt from the Japan Gerontological Evaluation Study; World Health Organization: Geneva, Switzerland, 2018; Available online: http://apps.who.int/bookorders (accessed on 20 May 2020).
- Tsuji, T.; Kanamori, S.; Miyaguni, Y.; Hanazato, M.; Kondo, K. Community-Level Sports Group Participation and the Risk of Cognitive Impairment. Med. Sci. Sports Exerc. 2019, 51, 2217–2223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takagi, D.; Kondo, K.; Kawachi, I. Social participation and mental health: Moderating effects of gender, social role and rurality. BMC Public Health 2013, 13, 701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nyunt, M.S.Z.; Fones, C.; Niti, M.; Ng, T.-P. Criterion-Based Validity and Reliability of the Geriatric Depression Screening Scale (GDS-15) in a Large Validation Sample of Community-Living Asian Older Adults. Aging Mental Health 2009, 13, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Schreiner, A.S.; Hayakawa, H.; Morimoto, T.; Kakuma, T. Screening for late life depression: Cut-off scores for the Geriatric Depression Scale and the Cornell Scale for Depression in Dementia among Japanese subjects. Int. J. Geriatr. Psychiatry 2003, 18, 498–505. [Google Scholar] [CrossRef]
- Yesavage, J.A.; Brink, T.L.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.; Leirer, O. Geriatric Depression Scale. Psychopharm. Bull 1988, 24, 709–710. [Google Scholar] [CrossRef]
- The Japan Geriatrics Society. Geriatric Depression Scale 15 (GDS15): Useful Tools for Medical Care of the Older People. Available online: https://www.jpn-geriat-soc.or.jp/tool/ (accessed on 15 February 2021).
- Tani, Y.; Sasaki, Y.; Haseda, M.; Kondo, K.; Kondo, N. Eating alone and depression in older men and women by cohabitation status: The JAGES longitudinal survey. Age Ageing 2015, 44, 1019–1026. [Google Scholar] [CrossRef] [Green Version]
- Nonaka, K.; Suzuki, H.; Murayama, H.; Hasebe, M.; Koike, T.; Kobayashi, E.; Fujiwara, Y. For how many days and what types of group activities should older Japanese adults be involved in to maintain health? A 4-year longitudinal study. PLoS ONE 2017, 12, e0183829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, S.J.; Woo, H.-T.; Cho, S.; Park, K.; Jeong, S.; Lee, Y.J.; Kang, D.; Shin, A. Association between body size, weight change and depression: Systematic review and meta-analysis. Br. J. Psychiatry 2017, 211, 14–21. [Google Scholar] [CrossRef]
- Nozaki, T. Diabetes mellitus, obesity and depression. In Proceedings of the 51st Annual Meeting of the Japanese Society of Psychosomatic Medicine, Sendai, Japan, 26–27 June 2010; Volume 51, pp. 886–895. [Google Scholar]
- Kuniaki, S. Factor Promoting Volunteer Activity in the Middle-Aged and the Elderly and Community Life Satisfaction: An Analysis Based on JGSS-2006; JGSS Research Series No.5: Japan edition General Social Surveys Research Papers; Faculty of Business Administration, Osaka University of Commerce: Osaka, Japan, 2009; Volume 8, pp. 41–65. [Google Scholar]
- Sato, J.; Mizoguchi, H.; Fukaya, K. Weather change and Mood Disorder. Weather change and Mood Disorder. J. Jpn. Soc. Biometeorol. 2011, 48, 3–7. [Google Scholar]
- O’Hare, C.; O Sullivan, V.; Flood, S.; Kenny, R.A. Seasonal and meteorological associations with depressive symptoms in older adults: A geo-epidemiological study. J. Affect. Disord. 2016, 191, 172–179. [Google Scholar] [CrossRef] [Green Version]
- Japan Meteorological Agency. What Is the Definition of Sunshine Duration? Available online: https://www.jma.go.jp/jma/kishou/know/faq/faq5.html (accessed on 20 May 2020).
- Ministry of Land, Infrastructure, Transport and Tourism. Available online: https://www.river.go.jp/kawabou/reference/index08.html (accessed on 20 May 2020).
- Zhang, J.; Yu, K.F. What’s the relative risk? A method of correcting the odds ratio in cohort studies of common outcomes. J. Am. Med. Assoc. 1998, 280, 1690–1691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawachi, I.; Berkman, L.F. Social Capital, Social Cohesion, and Health. In Social Epidemiology Second Edition; Berkman, L.F., Kawachi, I., Glymour, M.M., Eds.; Oxford University Press: New York, NY, USA, 2014; pp. 290–319. [Google Scholar] [CrossRef]
- Christakis, N.A.; Fowler, J.H. The collective dynamics of smoking in a large social network. N. Engl. J. Med. 2008, 358, 2249–2258. [Google Scholar] [CrossRef] [Green Version]
- Murata, C.; Saito, Y.; Kondo, K.; Hirai, H. Relationship between social support and depression in community-dwelling elderly: AGES Project. Gerontol. Soc. Sci. 2011, 33, 15–22. [Google Scholar]
- Zunzunegui, M.V.; Béland, A.O.F. Support from children, living arrangements, self-rated health and depressive symptoms of older people in Spain. Int. J. Epidemiol. 2001, 30, 1090–1099. [Google Scholar] [CrossRef] [Green Version]
- Kameyama, A.; Sakamoto, M.; Tanaka, E.; Sato, K.; Neichi, E.; Ohno, H. Relationships between social support and depression among community-dwelling middle-aged and elderly people: Investigation in town A in Aomori Prefecture. Jpn. J. Stress Sci. 2007, 22, 191–199. [Google Scholar]
- Shimanuki, H.; Honda, H.; Ito, T.; Kasai, T.; Takato, J.; Sakamoto, Y.; Inuzuka, G.; Ito, Y.; Arayama, N.; Ueki, S.; et al. Relationship between volunteer activities to promote long-term care prevention and social and physical health and QOL of community-dwelling elderly. Jpn. J. Public Health 2007, 54, 749–759. [Google Scholar]
- Hattori, S.; Ichida, Y.; Wada, Y.; Kondo, K. Volunteer Activities of the Elderly: Life Satisfaction, Higher Life Functions, and Background Factors; Japan Longevity and Social Development Center, Research on Life Satisfaction: Tokyo, Japan, 2017; Volume 23, pp. 28–47. [Google Scholar]
- National Council of Social Welfare, National Center for the Advancement of Volunteerism and Citizenship. Annual Report on Volunteer Activities 2011; Shin Kasumigaseki Building: Tokyo, Japan, 2012. [Google Scholar]


{kind=link}
| Developing Depressive Symptoms (GDS-15 ≥ 5) a | |||
|---|---|---|---|
| Individual-Level Variables | Total N | Number of Cases | Cumulative Incidence |
| Total | 37,552 | 3908 | 10.40% |
| Frequency of participation in a volunteer group | |||
| ≥4 day/week | 509 | 36 | 7.10% |
| 2–3 day/week | 977 | 74 | 7.60% |
| 1 day/week | 1144 | 81 | 7.10% |
| 1–3 day/month | 3200 | 248 | 7.80% |
| A few times a day/year | 3598 | 345 | 9.60% |
| Zero | 28,124 | 3124 | 11.10% |
| Sex | |||
| Man | 17,575 | 1788 | 10.20% |
| Woman | 19,977 | 2120 | 10.60% |
| Age, year | |||
| 65–69 | 12,346 | 1063 | 8.60% |
| 70–74 | 12,879 | 1241 | 9.60% |
| 75–79 | 7683 | 881 | 11.50% |
| 80–84 | 3489 | 511 | 14.60% |
| ≥85 | 1155 | 212 | 18.40% |
| Education, year | |||
| <6 | 263 | 51 | 19.40% |
| 6–9 | 13,165 | 1673 | 12.70% |
| 10–12 | 14,849 | 1454 | 9.80% |
| ≥13 | 8801 | 668 | 7.60% |
| Other and missing | 474 | 62 | 13.10% |
| Annual equivalent income, JPY | |||
| <2,000,000 | 13,905 | 1750 | 12.60% |
| 2,000,000–3,999,999 | 13,925 | 1214 | 8.70% |
| ≥4,000,000 | 4284 | 272 | 6.30% |
| Missing | 5438 | 672 | 12.40% |
| Disease status in treatment | |||
| Stroke no | 34,413 | 3624 | 10.50% |
| Stroke yes | 868 | 112 | 12.90% |
| Stroke missing | 2271 | 172 | 7.60% |
| Hypertension no | 19,354 | 2005 | 10.40% |
| Hypertension yes | 15,927 | 1731 | 10.90% |
| Hypertension missing | 2271 | 172 | 7.60% |
| Diabetes no | 30,916 | 3225 | 10.40% |
| Diabetes yes | 4365 | 511 | 11.70% |
| Diabetes missing | 2271 | 172 | 7.60% |
| Ear disease no | 33,451 | 3470 | 10.40% |
| Ear disease yes | 1830 | 266 | 14.50% |
| Ear disease missing | 2271 | 172 | 7.60% |
| Living alone | |||
| No | 32,829 | 3327 | 10.10% |
| Yes | 3383 | 405 | 12.00% |
| Missing | 1340 | 176 | 13.10% |
| Drinking status | |||
| None | 21,690 | 2397 | 11.10% |
| Past | 1442 | 207 | 14.40% |
| Current | 14,029 | 1261 | 9.00% |
| Missing | 391 | 43 | 11.00% |
| Smoking status | |||
| None | 27,987 | 2863 | 10.20% |
| Past | 5909 | 611 | 10.30% |
| Current | 3246 | 382 | 11.80% |
| Missing | 410 | 52 | 12.70% |
| BMI b (kg/m2) | |||
| <18.5 | 2127 | 279 | 13.10% |
| ≥18.5 and <25 | 26,106 | 2593 | 9.90% |
| ≥25 and <30 | 7441 | 784 | 10.50% |
| ≥30 and <50 | 679 | 73 | 10.80% |
| Missing | 1199 | 179 | 14.90% |
| Model 1: Adjusted for Outcome, Individual-Level, Community-Level, Cross-Level, Age and Sex | ||
|---|---|---|
| Total, N = 37,552 | IRR b | 95% CI c |
| Fixed effects | ||
| Volunteer participation at the individual level | 0.70 | (0.63–0.78) |
| Proportion of volunteer participation at the community level 10% estimation a | 0.86 | (0.77–0.97) |
| Cross-level interaction | 1.06 | (0.79–1.42) |
| Age, y | ||
| 65–69 | 1.00 | |
| 70–74 | 1.13 | (1.04–1.22) |
| 75–79 | 1.35 | (1.23–1.47) |
| 80–84 | 1.71 | (1.54–1.90) |
| ≧85 | 2.12 | (1.83–2.46) |
| Sex | ||
| Man | 1.00 | |
| Woman | 1.04 | (0.98–1.11) |
| Intercept (SE) d | 0.08 | 1.807 |
| Random effect | ||
| Ωμ (SE) d | 0.005 | 0.022 |
| a. Cross-level interaction: community-level exposure 10% estimation × individual-level exposure. | ||
| b. IRR: incidence rate ratio. | ||
| c. CI: confidence interval. | ||
| d. SE: standard error. | ||
| Model 2: Model 1 Adjusted for Community-Level Covariates | ||
| Total, N = 37,552 | IRR b | 95% CI c |
| Fixed effects | ||
| Volunteer participation at the individual level | 0.70 | (0.63–0.77) |
| Proportion of volunteer participation at the community level 10% estimation a | 0.87 | (0.78–0.98) |
| Cross-level interaction | 1.06 | (0.79–1.43) |
| Population density, persons per kilometer squared of inhabitable area | ||
| Highest quartile (≥11,385) | 1.00 | |
| Second quartile (9028–11,378) | 1.00 | (0.86–1.16) |
| Third quartile (5194–8977) | 1.06 | (0.91–1.22) |
| Lowest quartile (<5158) | 1.21 | (1.06–1.38) |
| Total annual sunshine hours | ||
| Highest quartile (≥ 2076) | ||
| Second quartile (2047–2075) | 0.92 | (0.81–1.03) |
| Third quartile (1911–2047) | 0.97 | (0.83–1.13) |
| Lowest quartile (<1911) | 0.98 | (0.87–1.11) |
| Annual Rainfall (mm) | ||
| Highest quartile (≥1622) | 1.00 | |
| Second quartile (1521–1621) | 0.90 | (0.76–1.06) |
| Third quartile (1483–1520) | 0.98 | (0.84–1.14) |
| Lowest quartile (<1483) | 0.82 | (0.72–0.95) |
| Age, y | ||
| 65–69 | 1.00 | |
| 70–74 | 1.13 | (1.04–1.22) |
| 75–79 | 1.34 | (1.22–1.47) |
| 80–84 | 1.70 | (1.53–1.89) |
| ≧85 | 2.09 | (1.80–2.43) |
| Sex | ||
| Man | 1.00 | |
| Woman | 1.04 | (0.98–1.11) |
| Intercept (SE) d | 0.08 | 0.008 |
| Random effect | ||
| Community-level variance | ||
| Ωμ (SE) d | 0.036 | 0.008 |
| a. Cross-level interaction: community-level exposure 10% estimation × individual-level exposure. | ||
| b. IRR: incidence rate ratio. | ||
| c. CI: confidence interval. | ||
| d. SE: standard error. | ||
| Model 3: Model 2 Adjusted for Individual-Level Covariates | ||
| Total, N = 37,552 | IRR b | 95% CI c |
| Fixed effects | ||
| Volunteer participation at the individual level | 0.72 | (0.65–0.80) |
| Proportion of volunteer participation at the community level 10% estimation a | 0.90 | (0.80–1.01) |
| Cross-level interaction | 1.06 | (0.79–1.42) |
| Population density, persons per kilometer squared of inhabitable area | ||
| Highest quartile (≥11,385) | 1.00 | |
| Second quartile (9028–11,378) | 0.99 | (0.85–1.15) |
| Third quartile (5194–8977) | 1.02 | (0.88–1.19) |
| Lowest quartile (<5158) | 1.12 | (0.99–1.28) |
| Total annual sunshine hours | ||
| Highest quartile (≥2076) | 1.00 | |
| Second quartile (2047–2075) | 0.91 | (0.81–1.02) |
| Third quartile (1911–2047) | 0.96 | (0.83–1.12) |
| Lowest quartile (<1911) | 0.96 | (0.84–1.08) |
| Annual Rainfall (mm) | ||
| Highest quartile (≥1622) | 1.00 | |
| Second quartile (1521–1621) | 0.88 | (0.75–1.04) |
| Third quartile (1483–1520) | 0.98 | (0.84–1.14) |
| Lowest quartile (<1483) | 0.83 | (0.73–0.96) |
| Age, y | ||
| 65–69 | 1.00 | |
| 70–74 | 1.08 | (1.00–1.18) |
| 75–79 | 1.25 | (1.14–1.37) |
| 80–84 | 1.55 | (1.39–1.73) |
| ≧ 85 | 1.88 | (1.62–2.20) |
| Sex | ||
| Man | 1.00 | |
| Woman | 1.02 | (0.94–1.10) |
| Education, y | ||
| ≧6 | 1.00 | |
| <6 | 1.24 | (0.94–1.64) |
| Other and missing | 1.16 | (0.85–1.58) |
| Annual equivalent income, JPY | ||
| ≧4,000,000 | 1.00 | |
| <2,000,000 | 1.83 | (1.61–2.09) |
| 2,000,000-3,999,999 | 1.35 | (1.19–1.54) |
| Missing | 1.72 | (1.50–1.99) |
| Disease status in treatment | ||
| Stroke no | 1.00 | |
| Stroke yes | 1.13 | (0.93–1.36) |
| Hypertension no | 1.00 | |
| Hypertension yes | 1.04 | (0.98–1.11) |
| Diabetes no | 1.00 | |
| Diabetes yes | 1.14 | (1.04–1.30) |
| Ear disease no | 1.00 | |
| Ear disease yes | 1.32 | (1.16–1.50) |
| Family structure | ||
| No | 1.00 | |
| Yes (living alone) | 1.07 | (0.97–1.20) |
| Missing | 1.13 | (0.97–1.32) |
| Drinking status | ||
| None | 1.00 | |
| Past | 1.21 | (1.04–1.41) |
| Current | 0.86 | (0.79–0.93) |
| Missing | 0.78 | (0.51–1.18) |
| Smoking status | ||
| None | 1.00 | |
| Past | 1.10 | (0.99–1.22) |
| Current | 1.29 | (1.15–1.44) |
| Missing | 1.30 | (0.89–1.90) |
| BMI e (kg/m2) | ||
| ≧18.5 | 1.00 | |
| <18.5 | 1.24 | (1.10–1.41) |
| Missing | 1.24 | (1.06–1.44) |
| Intercept (SE) e | 0.06 | 0.007 |
| Random effect | ||
| Community-level variance | ||
| Ωμ (SE) e | 0.035 | 0.008 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tamura, M.; Hattori, S.; Tsuji, T.; Kondo, K.; Hanazato, M.; Tsuno, K.; Sakamaki, H. Community-Level Participation in Volunteer Groups and Individual Depressive Symptoms in Japanese Older People: A Three-Year Longitudinal Multilevel Analysis Using JAGES Data. Int. J. Environ. Res. Public Health 2021, 18, 7502. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147502
Tamura M, Hattori S, Tsuji T, Kondo K, Hanazato M, Tsuno K, Sakamaki H. Community-Level Participation in Volunteer Groups and Individual Depressive Symptoms in Japanese Older People: A Three-Year Longitudinal Multilevel Analysis Using JAGES Data. International Journal of Environmental Research and Public Health. 2021; 18(14):7502. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147502
Chicago/Turabian StyleTamura, Motoki, Shinji Hattori, Taishi Tsuji, Katsunori Kondo, Masamichi Hanazato, Kanami Tsuno, and Hiroyuki Sakamaki. 2021. "Community-Level Participation in Volunteer Groups and Individual Depressive Symptoms in Japanese Older People: A Three-Year Longitudinal Multilevel Analysis Using JAGES Data" International Journal of Environmental Research and Public Health 18, no. 14: 7502. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147502