
Individual Resilience Interventions: A Systematic Review in Adult Population Samples over the Last Decade




Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Study Selection
2.4. Data Collection
2.5. Quality Assessment
3. Results
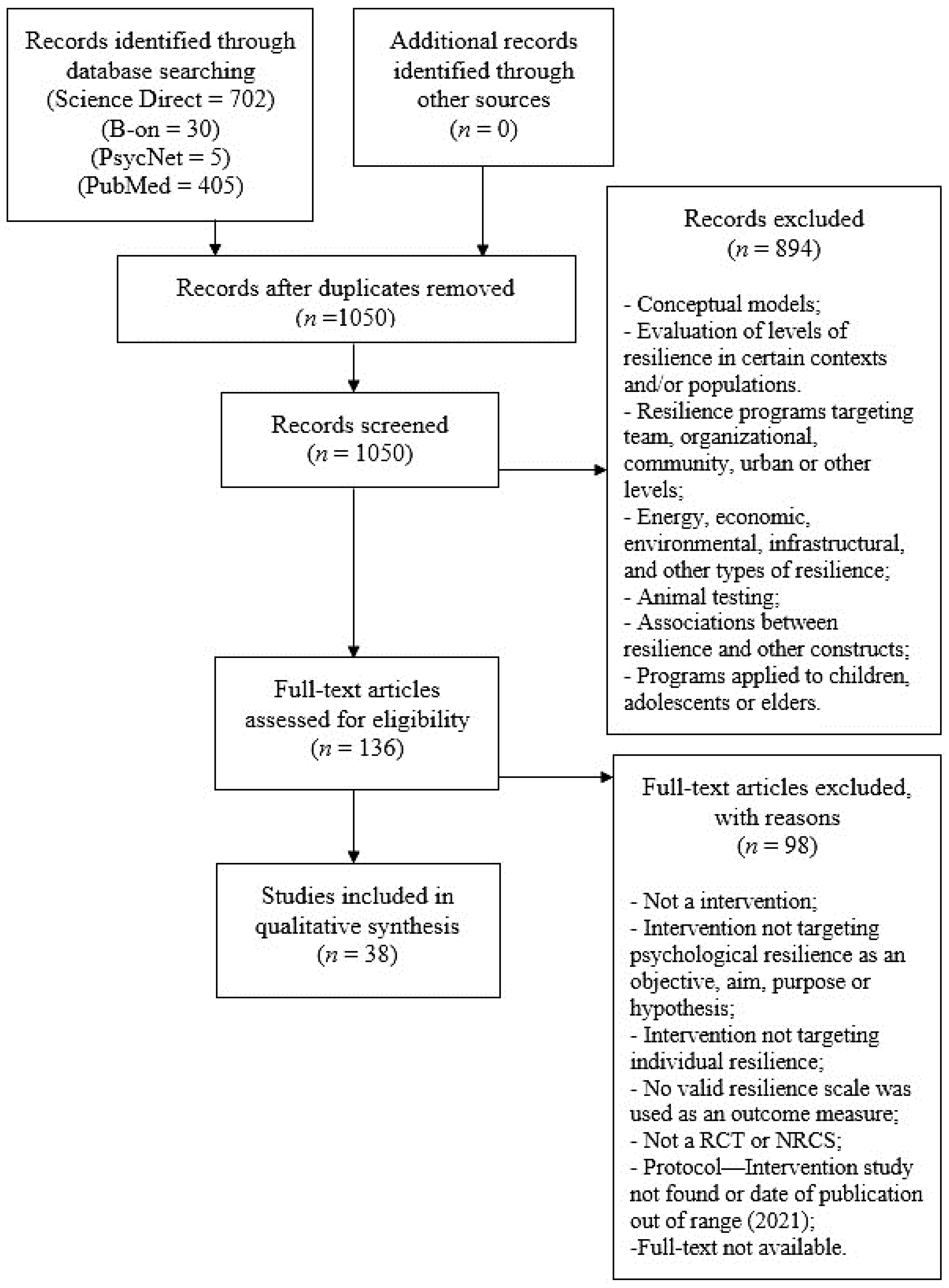
3.1. Study Selection
3.2. Study Characteristics
3.2.1. Setting
3.2.2. Population
3.2.3. Study Groups
3.2.4. Objectives
3.2.5. Theoretical Framework and Treatment Approach
3.2.6. Resilience Definition
3.2.7. Outcome Measures
3.2.8. Measurement Time Points and Length of Follow-Up
3.2.9. Moment of Intervention Concerning Stress Exposure
3.2.10. Intervention Details
3.2.11. Effectiveness
3.2.12. Methodological Quality
4. Discussion
4.1. Summary of Findings
4.2. Limitations of the Studies
4.3. Strengths and Limitations of This Review
4.4. Recommendations for Future Studies
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Electronic Search Strategy

{kind=link}
{kind=link}
| Terms | |
| Resilience/resilient/resiliency | |
| Promot * | |
| Intervention | |
| Program * | |
| Building | |
| Incres * | |
| Control * | |
| ID | Search |
| #1 | resilience OR resilient OR resiliency with Publication Year from 2010 to 2020 |
| #2 | promot * or intervention * or program * or train * or building or increase * with Publication Year from 2010 to 2020 |
| #3 | (resilience OR resilient OR resiliency) AND (promot * or intervention * or program * or train * or building or increase *) with Publication Year from 2010 to 2020 |
| #4 | (individual resilience OR resilient OR resiliency): ti, ab, kw AND (promot * or in tervention * or program * or train * or building or increase *): ti, ab, kw with Publication Year from 2010 to 2020 |
| #5 | (resilience OR resilient OR resiliency): ti, ab, kw AND (promot * or intervention * or program * or train * or building or increase *): ti, ab, kw AND (control *): ti, ab, kw |
- B-on (Synthesized)
- Science Direct (Synthesized)
- PubMed (Synthesized)
- APA PsycNet (Synthesized)
References
- Brandão, J.M.; Mahfoud, M.; Gianordoli-Nascimento, I.F. A construção do conceito de resiliência em psicologia: Discutindo as origens. Paidéia 2011, 21, 263–271. [Google Scholar] [CrossRef]
- Nawai, R.N.; Vasques, L.V. O Papel Da Resiliência No Desenvolvimento De Competencias Individuais. In 9o Congresso Pós-Graduação UNIS; Fundação de Ensino e Pesquisa do Sul de Minas, Brazil: Cataguases, Minas Gerais, Brazil, 2016; pp. 1–13. Available online: http://repositorio.unis.edu.br/handle/prefix/518 (accessed on 12 December 2020).
- Yunes, M.A.M. Psicologia positiva e resiliência: O foco no indivíduo e na família. Psicol. Estud. 2003, 8, 75–84. [Google Scholar] [CrossRef]
- Yunes, M.A.M.; Szymanski, H.; Tavares, J. Resiliência: Noção, conceitos afins e considerações críticas. Resil. Educ. 2001, 2, 13–43. [Google Scholar]
- Comas-Diaz, L.; Luthar, S.S.; Maddi, S.R.; O’Neill, K.H.; Saakvitne, K.W.; Tedeschi, R.G. The Road to Resilience; American Psychological Association: Washington, DC, USA, 2016. [Google Scholar]
- Adger, W.N. Social and ecological resilience: Are they related? Prog. Hum. Geogr. 2000, 24, 347–364. [Google Scholar] [CrossRef]
- Britt, E.; Carter, J.; Conradson, D.; Scott, A.; Vargo, J.; Moss, H. Report for Ministry of Social Development Resilience Framework and Guidelines for Practice; Universisty of Canterbury: Christchurch, New Zealand, 2012; Available online: https://ir.canterbury.ac.nz/handle/10092/9821 (accessed on 16 December 2020).
- Bonanno, G.A. Loss, Trauma, and Human Resilience: Have We Underestimated the Human Capacity to Thrive after Extremely Aversive Events? Am. Psychol. 2004, 59, 20–28. [Google Scholar] [CrossRef] [Green Version]
- Gonçalves, C. Regiões, cidades e comunidades resilientes: Novos princípios de desenvolvimento. Urbe 2017, 9, 371–385. [Google Scholar] [CrossRef] [Green Version]
- Grotberg, E.H. The International Resilience Project: Research and Application; Civitan International: Birmingham, AL, USA, 1995; ED:423955. [Google Scholar]
- Joyce, S.; Shand, F.; Tighe, J.; Laurent, S.J.; Bryant, R.A.; Harvey, S.B. Road to resilience: A systematic review and meta-analysis of resilience training programmes and interventions. BMJ Open 2018, 8, e017858. [Google Scholar] [CrossRef] [Green Version]
- Seligman, M.E.P.; Csikszentmihalyi, M. Positive psychology: An introduction. Am. Psychol. 2000, 55, 5–14. [Google Scholar] [CrossRef] [PubMed]
- Reppold, C.T.; Mayer, J.C.; Almeida, L.S.; Hutz, C.S. Avaliação da resiliência: Controvérsia em torno do uso das escalas. Psicol. Reflect. Crit. 2012, 25, 248–255. [Google Scholar] [CrossRef] [Green Version]
- Carmello, E. Resiliência: A Transformação Como Ferramenta par Construir Empresas de Valor; Editora Gente: São Paulo, Brazil, 2008. [Google Scholar]
- Pfefferbaum, B.J.; Reissman, D.B.; Pfefferbaum, R.L.; Klomp, R.W.; Gurwitch, R.H. Building Resilience to Mass Trauma Events. In Handbook of Injury and Violence Prevention; Doll, L., Bonzo, S., Sleet, D., Mercy, J., Haas, E.N., Eds.; Springer: Boston, MA, USA, 2007; pp. 347–358. [Google Scholar] [CrossRef] [Green Version]
- Benjet, C.; Bromet, E.J.; Karam, E.G.; Kessler, R.C.; McLaughlin, K.A.; Ruscio, A.M.; Shahly, V.; Stein, D.; Petukhova, M.; Hill, E.; et al. The epidemiology of traumatic event exposure worldwide: Results from the World Mental Health Survey Consortium. Psychol. Med. 2016, 46, 327–343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kessler, R.C.; Aguilar-Gaxiola, S.; Alonso, J.; Chatterji, S.; Lee, S.; Ormel, J.; Üstün, T.B.; Wang, P.S. The global burden of mental disorders: An update from the WHO World Mental Health (WMH) Surveys. Epidemiol. Psichiatr. Soc. 2009, 18, 23–33. [Google Scholar] [CrossRef] [Green Version]
- Kessler, R.C.; Aguilar-Gaxiola, S.; Alonso, J.; Benjet, C.; Bromet, E.J.; Cardoso, G.; Degenhardt, L.; de Girolamo, G.; Dinolova, R.V.; Ferry, F.; et al. Trauma and PTSD in the WHO World Mental Health Surveys. Eur. J. Psychotraumatol. 2017, 8, 1353383. [Google Scholar] [CrossRef] [PubMed]
- Pai, A.; Suris, A.M.; North, C.S. Posttraumatic Stress Disorder in the DSM-5: Controversy, Change, and Conceptual Considerations. Behav. Sci. 2017, 7, 7. [Google Scholar] [CrossRef] [PubMed]
- Leppin, A.L.; Bora, P.R.; Tilburt, J.C.; Gionfriddo, M.; Zeballos-Palacios, C.; Dulohery, M.M.; Sood, A.; Erwin, P.J.; Brito, J.P.; Boehmer, K.R.; et al. The Efficacy of Resiliency Training Programs: A Systematic Review and Meta-Analysis of Randomized Trials. PLoS ONE 2014, 9, e111420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Investing in Mental Health; World Health Organization: Geneva, Switzerland, 2003; ISBN 92-4-156257-9. [Google Scholar]
- Chmitorz, A.; Kunzler, A.; Helmreich, I.; Tüscher, O.; Kalisch, R.; Kubiak, T.; Wessa, M.; Lieb, K. Intervention studies to foster resilience—A systematic review and proposal for a resilience framework in future intervention studies. Clin. Psychol. Rev. 2018, 59, 78–100. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- Windle, G.; Bennett, K.M.; Noyes, J. A methodological review of resilience measurement scales. Health Qual. Life Outcomes 2011, 9, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [Green Version]
- Aikens, K.A.; Astin, J.; Pelletier, K.R.; Levanovich, K.; Baase, C.M.; Park, Y.Y.; Bodnar, C.M. Mindfulness Goes to Work: Impact of an Online Workplace Intervention. J. Occup. Environ. Med. 2014, 56, 721–731. [Google Scholar] [CrossRef] [Green Version]
- Burton, L.E.; Qeadan, F.; Burge, M.R. Efficacy of equine-assisted psychotherapy in veterans with posttraumatic stress disorder. J. Integr. Med. 2019, 17, 14–19. [Google Scholar] [CrossRef]
- Hendriks, T.; Schotanus-Dijkstra, M.; Hassankhan, A.; Sardjo, W.; Graafsma, T.; Bohlmeijer, E.; De Jong, J. Resilience and well-being in the Caribbean: Findings from a randomized controlled trial of a culturally adapted multi-component positive psychology intervention. J. Posit. Psychol. 2019, 15, 238–253. [Google Scholar] [CrossRef]
- Van Grieken, A.; Horrevorts, E.M.; Mieloo, C.L.; Bannink, R.; Bouwmeester-Landweer, M.B.; Groen, E.H.-D.; Broeren, S.; Raat, H. A Controlled Trial in Community Pediatrics to Empower Parents Who Are at Risk for Parenting Stress: The Supportive Parenting Intervention. Int. J. Environ. Res. Public Health 2019, 16, 4508. [Google Scholar] [CrossRef] [Green Version]
- Houston, J.B.; First, J.; Spialek, M.L.; Sorenson, M.E.; Mills-Sandoval, T.; Lockett, M.; First, N.L.; Nitiéma, P.; Allen, S.F.; Pfefferbaum, B. Randomized controlled trial of the Resilience and Coping Intervention (RCI) with undergraduate university students. J. Am. Coll. Health 2016, 65, 1–9. [Google Scholar] [CrossRef]
- Hsieh, H.-F.; Huang, I.-C.; Liu, Y.; Chen, W.-L.; Lee, Y.-W.; Hsu, H.-T. The Effects of Biofeedback Training and Smartphone-Delivered Biofeedback Training on Resilience, Occupational Stress, and Depressive Symptoms among Abused Psychiatric Nurses. Int. J. Environ. Res. Public Health 2020, 17, 2905. [Google Scholar] [CrossRef]
- Hwang, W.J.; Lee, T.Y.; Lim, K.-O.; Bae, D.; Kwak, S.; Park, H.-Y.; Kwon, J.S. The effects of four days of intensive mindfulness meditation training (Templestay program) on resilience to stress: A randomized controlled trial. Psychol. Health Med. 2017, 23, 497–504. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.I.; Yun, J.-Y.; Park, H.; Park, S.-Y.; Ahn, Y.; Lee, H.; Kim, T.-K.; Yoon, S.; Lee, Y.-J.; Oh, S.; et al. A Mobile Videoconference-Based Intervention on Stress Reduction and Resilience Enhancement in Employees: Randomized Controlled Trial. J. Med. Internet Res. 2018, 20, e10760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiropoulos, L.A.; Kilpatrick, T.; Holmes, A.; Threader, J. A pilot randomized controlled trial of a tailored cognitive behavioural therapy based intervention for depressive symptoms in those newly diagnosed with multiple sclerosis. BMC Psychiatry 2016, 16, 435. [Google Scholar] [CrossRef] [Green Version]
- Kovacs, A.H.; Grace, S.; Kentner, A.; Nolan, R.P.; Silversides, C.K.; Irvine, M.J. Feasibility and Outcomes in a Pilot Randomized Controlled Trial of a Psychosocial Intervention for Adults with Congenital Heart Disease. Can. J. Cardiol. 2018, 34, 766–773. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.; Lee, W.J.; Choi, S.-H.; Jang, J.-H.; Kang, D.-H. Long-term beneficial effects of an online mind-body training program on stress and psychological outcomes in female healthcare providers: A non-randomized controlled study. Medicine 2020, 99, e21027. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; He, G.; Yan, J.; Gu, C.; Xie, J. The Effects of a Modified Mindfulness-Based Stress Reduction Program for Nurses: A Randomized Controlled Trial. Work. Health Saf. 2018, 67, 111–122. [Google Scholar] [CrossRef]
- Champion, L.; Economides, M.; Chandler, C. The efficacy of a brief app-based mindfulness intervention on psychosocial outcomes in healthy adults: A pilot randomised controlled trial. PLoS ONE 2018, 13, e0209482. [Google Scholar] [CrossRef]
- Loprinzi, C.E.; Prasad, K.; Schroeder, D.R.; Sood, A. Stress Management and Resilience Training (SMART) Program to Decrease Stress and Enhance Resilience Among Breast Cancer Survivors: A Pilot Randomized Clinical Trial. Clin. Breast Cancer 2011, 11, 364–368. [Google Scholar] [CrossRef]
- Mache, S.; Vitzthum, K.; Klapp, B.F.; Groneberg, D.A. Evaluation of a Multicomponent Psychosocial Skill Training Program for Junior Physicians in Their First Year at Work: A Pilot Study. Fam. Med. 2015, 47, 693–698. [Google Scholar] [PubMed]
- McCann, T.V.; Songprakun, W.; Stephenson, J.C. Efficacy of a self-help manual in increasing resilience in carers of adults with depression in Thailand. Int. J. Ment. Health Nurs. 2016, 25, 62–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGonagle, A.; Beatty, J.E.; Joffe, R. Coaching for workers with chronic illness: Evaluating an intervention. J. Occup. Health Psychol. 2014, 19, 385–398. [Google Scholar] [CrossRef]
- Mealer, M.; Conrad, D.; Evans, J.; Jooste, K.; Solyntjes, J.; Rothbaum, B.; Moss, M. Feasibility and Acceptability of a Resilience Training Program for Intensive Care Unit Nurses. Am. J. Crit. Care 2014, 23, e97–e105. [Google Scholar] [CrossRef]
- Mondanaro, J.F.; Sara, G.A.; Thachil, R.; Pranjić, M.; Rossetti, A.; Sim, G.E.; Canga, B.; Harrison, I.B.; Loewy, J.V. The Effects of Clinical Music Therapy on Resiliency in Adults Undergoing Infusion: A Randomized, Controlled Trial. J. Pain Symptom Manag. 2021, 61, 1099–1108. [Google Scholar] [CrossRef]
- Pidgeon, A.M.; Ford, L.; Klaassen, F. Evaluating the effectiveness of enhancing resilience in human service professionals using a retreat-based Mindfulness with Metta Training Program: A randomised control trial. Psychol. Health Med. 2013, 19, 355–364. [Google Scholar] [CrossRef] [PubMed]
- Senders, A.; Hanes, D.; Bourdette, D.; Carson, K.; Marshall, L.M.; Shinto, L. Impact of mindfulness-based stress reduction for people with multiple sclerosis at 8 weeks and 12 months: A randomized clinical trial. Mult. Scler. J. 2019, 25, 1178–1188. [Google Scholar] [CrossRef]
- Songprakun, W.; McCann, T.V. Effectiveness of a self-help manual on the promotion of resilience in individuals with depression in Thailand: A randomised controlled trial. BMC Psychiatry 2012, 12, 12. [Google Scholar] [CrossRef] [Green Version]
- Sood, A.; Prasad, K.; Schroeder, D.; Varkey, P. Stress Management and Resilience Training Among Department of Medicine Faculty: A Pilot Randomized Clinical Trial. J. Gen. Intern. Med. 2011, 26, 858–861. [Google Scholar] [CrossRef] [Green Version]
- Christopher, M.; Hunsinger, M.; Goerling, L.R.J.; Bowen, S.; Rogers, B.S.; Gross, C.R.; Dapolonia, E.; Pruessner, J.C. Mindfulness-based resilience training to reduce health risk, stress reactivity, and aggression among law enforcement officers: A feasibility and preliminary efficacy trial. Psychiatry Res. 2018, 264, 104–115. [Google Scholar] [CrossRef]
- Sood, A.; Sharma, V.; Schroeder, D.R.; Gorman, B. Stress Management and Resiliency Training (SMART) Program among Department of Radiology Faculty: A Pilot Randomized Clinical Trial. Explore 2014, 10, 358–363. [Google Scholar] [CrossRef]
- Weiss, L.A.; Voshaar, M.A.H.O.; Bohlmeijer, E.T.; Westerhof, G.J. The long and winding road to happiness: A randomized controlled trial and cost-effectiveness analysis of a positive psychology intervention for lonely people with health problems and a low socio-economic status. Health Qual. Life Outcomes 2020, 18, 1–17. [Google Scholar] [CrossRef]
- Wesner, A.C.; Behenck, A.; Finkler, D.; Beria, P.; Guimarães, L.S.; Manfro, G.G.; Blaya, C.; Heldt, E. Resilience and coping strategies in cognitive behavioral group therapy for patients with panic disorder. Arch. Psychiatr. Nurs. 2019, 33, 428–433. [Google Scholar] [CrossRef] [PubMed]
- Wild, J.; El-Salahi, S.; Degli Esposti, M.; Thew, G.R. Evaluating the effectiveness of a group-based resilience intervention versus psychoeducation for emergency responders in England: A randomised controlled trial. PLoS ONE 2020, 15, e0241704. [Google Scholar] [CrossRef] [PubMed]
- Wong, W.C.-W.; Yuen, W.W.-Y.; Tang, C.S.-K.; Holroyd, E.; Fong, D.Y.-T. Evaluation and mechanism analysis of HIV prevention programme using resilience framework among female sex workers: A randomised controlled trial. Prev. Med. Rep. 2019, 13, 229–237. [Google Scholar] [CrossRef]
- Wu, P.-H.; Chen, S.-W.; Huang, W.-T.; Chang, S.-C.; Hsu, M.-C. Effects of a Psychoeducational Intervention in Patients with Breast Cancer Undergoing Chemotherapy. J. Nurs. Res. 2018, 26, 266–279. [Google Scholar] [CrossRef] [PubMed]
- Ye, Z.J.; Qiu, H.Z.; Liang, M.Z.; Liu, M.L.; Li, P.F.; Chen, P.; Sun, Z.; Yu, Y.L.; Ni Wang, S.; Zhang, Z.; et al. Effect of a mentor-based, supportive-expressive program, Be Resilient to Breast Cancer, on survival in metastatic breast cancer: A randomised, controlled intervention trial. Br. J. Cancer 2017, 117, 1486–1494. [Google Scholar] [CrossRef]
- Yu, N.X.; Stewart, S.M.; Chui, J.P.; Ho, J.L.; Li, A.C.; Lam, T.H. A Pilot Randomized Controlled Trial to Decrease Adaptation Difficulties in Chinese New Immigrants to Hong Kong. Behav. Ther. 2014, 45, 137–152. [Google Scholar] [CrossRef] [PubMed]
- Clarkson, M.; Heads, G.; Hodgson, D.; Probst, H. Does the intervention of mindfulness reduce levels of burnout and compassion fatigue and increase resilience in pre-registration students? A pilot study. Radiography 2019, 25, 4–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Denkova, E.; Zanesco, A.P.; Rogers, S.L.; Jha, A.P. Is resilience trainable? An initial study comparing mindfulness and relaxation training in firefighters. Psychiatry Res. 2020, 285, 112794. [Google Scholar] [CrossRef] [PubMed]
- Roig, A.E.; Mooney, O.; Salamanca-Sanabria, A.; Lee, C.T.; Farrell, S.; Richards, D. Assessing the Efficacy and Acceptability of a Web-Based Intervention for Resilience Among College Students: Pilot Randomized Controlled Trial. JMIR Form. Res. 2020, 4, e20167. [Google Scholar] [CrossRef] [PubMed]
- Erogul, M.; Singer, G.; McIntyre, T.; Stefanov, D.G. Abridged Mindfulness Intervention to Support Wellness in First-Year Medical Students. Teach. Learn. Med. 2014, 26, 350–356. [Google Scholar] [CrossRef] [PubMed]
- Fikretoglu, D.; Liu, A.; Nazarov, A.; Blackler, K. A group randomized control trial to test the efficacy of the Road to Mental Readiness (R2MR) program among Canadian military recruits. BMC Psychiatry 2019, 19, 326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giovannetti, A.M.; Quintas, R.; Tramacere, I.; Giordano, A.; Confalonieri, P.; Uccelli, M.M.; Solari, A.; Pakenham, K.I. A resilience group training program for people with multiple sclerosis: Results of a pilot single-blind randomized controlled trial and nested qualitative study. PLoS ONE 2020, 15, e0231380. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 Explanation and Elaboration: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c869. [Google Scholar] [CrossRef] [Green Version]
- Bodeker, G. Mental Welness in Asia; Asian Development Bank: Mandaluyong City, Metro Manila, Philippines, 2020. [Google Scholar]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer Publishing Company: New York, NY, USA, 1984. [Google Scholar]
- Connor, K.M.; Davidson, J.R.T. Development of a new resilience scale: The Connor-Davidson Resilience Scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef]
- Campbell-Sills, L.; Stein, M.B. Psychometric analysis and refinement of the connor–davidson resilience scale (CD-RISC): Validation of a 10-item measure of resilience. J. Trauma. Stress 2007, 20, 1019–1028. [Google Scholar] [CrossRef]
- Wagnild, G.; Young, H. Development and Pshycometric evaluation of a Recilience Scale. J. Nurs. Meas. 1993, 1, 165–178. [Google Scholar]
- Friborg, O.; Barlaug, D.; Martinussen, M.; Rosenvinge, J.H.; Hjemdal, O. Resilience in relation to personality and intelligence. Int. J. Methods Psychiatr. Res. 2005, 14, 29–42. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.W.; Dalen, J.; Wiggins, K.; Tooley, E.; Christopher, P.; Bernard, J. The brief resilience scale: Assessing the ability to bounce back. Int. J. Behav. Med. 2008, 15, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Babíc, R.; Babíc, M.; Rastovi, P.; Curlin, M.; Simic, J.; Mandi, K.; Pavlovic, K. Resilience in health and illness. Psychiatr. Danub. 2020, 32, 226–232. [Google Scholar]
- PeConga, E.K.; Gauthier, G.M.; Holloway, A.; Walker, R.S.W.; Rosencrans, P.L.; Zoellner, L.A.; Bedard-Gilligan, M. Resilience is spreading: Mental health within the COVID-19 pandemic. Psychol. Trauma Theory Res. Pract. Policy 2020, 12, S47–S48. [Google Scholar] [CrossRef]
- Oliveira, K.D.S.; Nakano, T.D.C. Avaliação da resiliência em Psicologia: Revisão do cenário científico brasileiro. Rev. Psicol. Pesqui. 2018, 12, 1–11. [Google Scholar] [CrossRef]
- Riehm, K.E.; Brenneke, S.G.; Adams, L.B.; Gilan, D.; Lieb, K.; Kunzler, A.M.; Smail, E.J.; Holingue, C.; Stuart, E.A.; Kalb, L.G.; et al. Association between psychological resilience and changes in mental distress during the COVID-19 pandemic. J. Affect. Disord. 2021, 282, 381–385. [Google Scholar] [CrossRef]
- Freedland, K.E.; Mohr, D.; Davidson, K.; Schwartz, J. Usual and Unusual care: Existing Practice Control Groups in Randomized Controlled Trials of Behavioral Interventions. Psychosom. Med. 2011, 73, 323–335. [Google Scholar] [CrossRef]
- Luthar, S.S.; Cicchetti, D.; Becker, B. The Construct of Resilience: A Critical Evaluation and Guidelines for Future Work. Child Dev. 2000, 71, 543–562. [Google Scholar] [CrossRef]
- Macedo, T.; Wilheim, L.; Gonçalves, R.; Coutinho, E.S.F.; Vilete, L.; Figueira, I.; Ventura, P. Building resilience for future adversity: A systematic review of interventions in non-clinical samples of adults. BMC Psychiatry 2014, 14, 227. [Google Scholar] [CrossRef] [Green Version]


| Group | Studies |
|---|---|
| General Population | |
| General population | Champion et al. [38]; Hwang et al. [32] |
| General population in a specific context | Hendriks et al. [28] |
| Vulnerable adults | Weiss et al. [51] |
| New immigrants | Yu et al. [57] |
| Groups Considered at Risk Due to Occupation | |
| Employees Emergency workers (general) Law enforcement officers Military recruits Firefighters Female sex workers Human service professionals Health care workers (general) Physicians Nurses College students | Aikens et al. [26]; Kim et al. [33] Wild et al. [53] Christopher et al. [49] Fikretoglu et al. [62] Denkova et al. [59] Wong et al. [54] Pidgeon, Ford & Klaassen [45] Lee et al. [36] Mache et al. [40]; Sood et al. [48]; Sood et al. [50] Hsieh et al. [31]; Lin et al. [37]; Mealer et al. [43] Clarkson at al. [58]; Erogul et al. [61]; Houston et al. [30] Roig et al. [60] |
| Groups Considered at Risk Due to Clinical Condition | |
| Workers with chronic health condition | McGonagle, Beatty & Joffe [42] |
| Individuals with multiple sclerosis | Giovannetti et al. [63]; Senders et al. [46] |
| Depressed individuals with multiple sclerosis | Kiropoulos et al. [34] |
| Individuals with Congenital Heart Disease | Kovacs et al. [35] |
| Breast cancer survivors | Loprinzi et al. [39]; Ye et al. [56] |
| Breast cancer patients doing chemotherapy | Wu et al. [55] |
| Cancer patients doing infusion therapy | Mondanaro et al. [44] |
| Individuals with depression | Songprakun & McCann [47] |
| Individuals with panic disorder | Wesner et al. [52] |
| Veterans with PTSD | Burton, Qeadan & Burge [27] |
| Groups Considered at Risk Due to Caretaking | |
| Primary caregivers of family members with depression | McCann, Songprakun & Stephenson [41] |
| Parents at risk | van Grieken et al. [29] |
| Approach | Study | Definition |
|---|---|---|
| Trait-Oriented | Burton, Qeadan & Burge [27] | “ability of individuals to adapt positively in the face of trauma” (p. 16) |
| Clarkson et al. [58] | “hardiness and ability to cope in adversity (Foureur, Besley, Burton, Yu & Crisp, 2013)” (p. 90) | |
| Denkova et al. [59] | “ability to effectively adapt to adverse situations (Fletcher and Sarkar, 2013, 2016; Joyce, Shand, Tighe, Laurent, Bryant & Harvey, 2018)”; “malleable characteristic that can be trained and bolstered (Joyce et al., 2018)” (p. 1); “key protective factor” (p. 5) | |
| Houston et al. [30] | “ability to positively adapt in the face of adversity, trauma or stress (Masten, 2001)” (p. 1) | |
| Lin et al. [37] | “competency to cope and adapt in the face of adversity, is considered a significant protective factor against the negative effects of job stress (Hart, Brannan, & De Chesnay, 2014)” (p. 118) | |
| Loprinzi et al. [39] | “ability to thrive despite stress and adversity (Connor & Davidson, 2003)”; “described as invulnerability and hardiness (Kobasa, 1979)”; “the source of resilience is an individual’s innate strength that helps the individual adapt to stressors and pursue life’s meaning and purpose” (p. 365) | |
| Mache et al. [40] | “individual protective factors such as resilience”; “ability of an individual to withstand adversity and is often seen as a form of self-recovery with positive emotional and cognitive outcomes, which in turn has an important role in realising greater adaptability and life satisfaction (Luthar, Cicchetti & Becker, 2000; Rutter, 1999)” (p. 693) | |
| McGonagle, Beatty & Joffe [42] | “positive adaptability or ability to thrive in the face of adversity (Campbell-Sills & Stein, 2007; Luthans, 2002)” (p. 387) | |
| Mealer et al. [43] | “psychological characteristic that has been defined as a trait or capacity depending on the underlying theory adopted”; “one of the most important factors in successful adaptation following exposure to a traumatic event (Charney, 2004)” (p. 98) | |
| Pidgeon, Ford & Klaassen [45] | “competence to cope and adapt in the face of adversity and to bounce back when stressors become overwhelming is considered a significant protective factor against instances of compassion fatigue, burnout and mental and physical illness (Thomas & Otis, 2010)” (p. 1) | |
| Songprakun & McCann [47] | “psychosocial capacity of the person to maintain positive adaptive functioning which minimises negative thoughts and promotes recovery of strength and coping ability and to have a positive outlook in the face of difficult circumstances (Reivich, Gillham, Chaplin & Seligman, 2005)”; “protective factor that facilitates successful coping in conditions of adversity (Fergus & Zimmerman, 2005)” (p. 2) | |
| Sood et al. [48] | “ability of an individual to withstand adversity (Connor & Davidson, 2003)” (p. 858) | |
| Wesner et al. [52] | “individual’s competence in overcoming stressful life events and adversities (Rutter, 2012)” (p. 428) | |
| Wild et al. [53] | “capacity to maintain wellbeing in response to adversity or stress (Carleton, Afifi, Turner, Taillieu, Duranceau, et al. 2017)” (p. 2) | |
| Wong et al. [54] | “the ability to adapt and function competently after adversity” (p. 230) | |
| Ye et al. [56] | “capacity to bounce back after encountering a traumatic event (Connor and Davidson, 2003; Haglund et al., 2007)” (p. 1487) | |
| Yu et al. [57] | “effective coping and adaptation when one experiences loss, hardship, or adversity (Tugade & Fredrickson, 2004)” (p. 138) | |
| Process-Oriented | Erogul et al. [61] | “thought to be a state rather than a trait, meaning it is mutable in response to experience or training instead of an innate quality that is fixed and not subject to modification” (p. 353) |
| Hsieh et al. [31] | “process of adapting well in the face of adversity, trauma, tragedy, threats, stress, serious health problems, or workplace conflict—it means “bouncing back” from difficult experiences (APA, 2014)” (p. 2) | |
| Hwang et al. [32] | “the process of adapting well in the face of adversity, trauma, tragedy, threats or even significant sources of threat (APA)” (p. 2); “factor that potentially buffers against the negative impact of work stress (Howard, 2008)” (p. 5) | |
| Kim et al. [33] | “refers to the process that allows individuals to adapt positively despite stress or trauma (Luthar, Cicchetti & Becker, 2000)” (p. 8) | |
| McCann, Songprakun & Stephenson [41] | “process of coping with adversity, change, or opportunity in a manner that results in the identification, fortification, and enrichment of resilient qualities or protective factors (Richardson 2002, p. 308)” (pp. 62,63) | |
| Roig et al. [60] | “may be understood as the personal assets (internal factors, e.g., optimism) and environmental resources (external factors, e.g., social support) that contribute to positive psychological adaption, despite exposure to adversity (Helmereich, Kunzler, Chmitorz, König, Binder & Wessa, 2017)” (p. 2) | |
| Trait-Process | Giovannetti et al. [63] | “an internal resource for alleviating the adverse effects of stress and sustaining good mental health through adversity (Leppin, Bora, Tilburt, Gionfriddo, Zeballos-Palacios, Dulohery, et al., 2014). It entails the process of negotiating, managing and adapting to significant stressors or trauma through drawing on internal (…), and external (…) resources (Windle, Bennet & Noyes, 2011)” (p. 2) |
| Trait-Process-Outcome | Hendriks et al. [28] | “capacity to deal effectively with stress and adversity, to adapt successfully to setbacks (Luthar, Cicchetti, & Becker, 2000; Zautra, Hall, & Murray, 2008), and to bounce back after negative emotional experiences (Tugade & Fredrickson, 2004). Resilience refers to positive outcomes in spite of threats to adaptation or development (Masten, 2001) and factors and mechanisms that play a role in dealing functionally with, and contribute to successful adaptation to problems (Friborg, Hjemdal, Martinussen, & Rosenvinge, 2009). Resilience is an active process” (p. 2); “set of personal characteristics” (p. 3) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferreira, M.; Marques, A.; Gomes, P.V. Individual Resilience Interventions: A Systematic Review in Adult Population Samples over the Last Decade. Int. J. Environ. Res. Public Health 2021, 18, 7564. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147564
Ferreira M, Marques A, Gomes PV. Individual Resilience Interventions: A Systematic Review in Adult Population Samples over the Last Decade. International Journal of Environmental Research and Public Health. 2021; 18(14):7564. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147564
Chicago/Turabian StyleFerreira, Mafalda, António Marques, and Paulo Veloso Gomes. 2021. "Individual Resilience Interventions: A Systematic Review in Adult Population Samples over the Last Decade" International Journal of Environmental Research and Public Health 18, no. 14: 7564. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147564