
Influence of Tunneled Hemodialysis-Catheters on Inflammation and Mortality in Dialyzed Patients


 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. The Scope of the Study
2.2. Population, Sampling and Inclusion Criteria
2.2.1. Dialysis Scheme
2.2.2. Nursing Care of HDCs
2.3. Study Design
2.4. Study Variables and Labs
Cell Cultures
2.5. Legal and Ethical Issues
2.6. Statistical Analysis
3. Results
3.1. Study Sample Description
3.2. Inflammation and Microinflammation Parameters
3.3. Analytic Values, Dialysis Efficacy, Comorbidity and Hospital Admissions
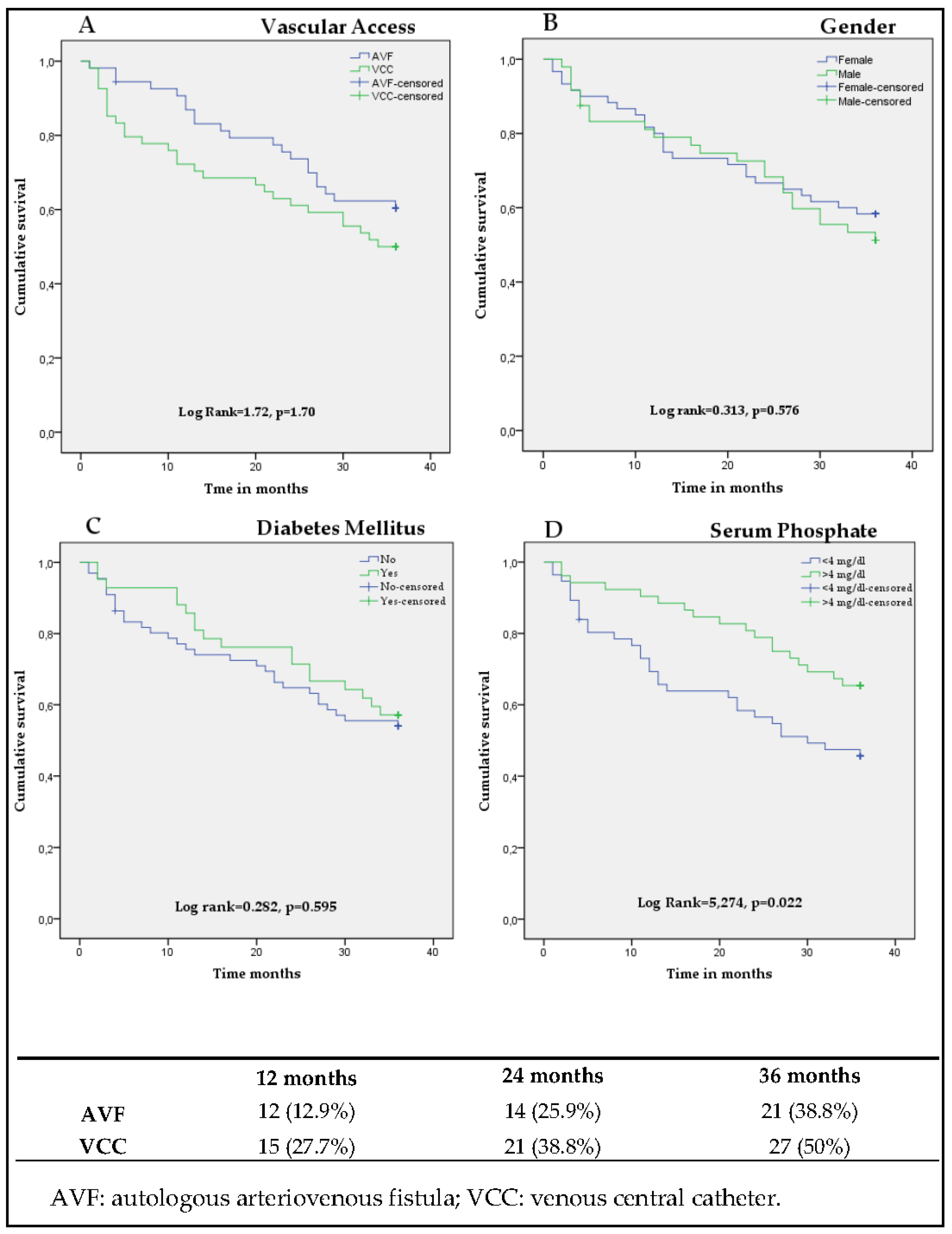
3.4. Survival Analysis
3.5. Cox Regression
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vascular Access Work Group. Clinical practice guidelines for vascular access. Am. J. Kidney Dis. 2006, 48, S176–S247. [Google Scholar] [CrossRef] [PubMed]
- Sidawy, A.N.; Spergel, L.M.; Besarab, A.; Allon, M.; Jennings, W.C.; Padberg, F.T., Jr.; Murad, M.H.; Montori, V.; O’Hare, A.M.; Calligaro, K.D.; et al. Society for Vascular Surgery. The Society for Vascular Surgery: Clinical practice guidelines for the surgical placement and maintenance of arteriovenous hemodialysis access. J. Vasc. Surg. 2008, 48 (Suppl. 5), S2–S25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rayner, H.C.; Pisoni, R. The increasing use of hemodialysis catheters: Evidence from the DOPPS on its significance and ways to reverse it. Semin. Dial. 2010, 23, 6–10. [Google Scholar] [CrossRef] [PubMed]
- Noordzij, M.; Jager, K.J.; Van Der Veer, S.N.; Kramar, R.; Collart, F.; Heaf, J.G.; Stojceva-Taneva, O.; Leivestad, T.; Buturovic-Ponikvar, J.; Sanchez, M.B.; et al. Use of vascular access for haemodialysis in Europe: A report from the ERA-EDTA Registry. Nephrol. Dial. Transplant. 2014, 29, 1956–1964. [Google Scholar] [CrossRef] [Green Version]
- Vachharajani, T.J.; Moossavi, S.; Jordan, J.R.; Vachharajani, V.; Freedman, B.I.; Burkart, J.M. Re-evaluating the fistula first initiative in octogenarians on hemodialysis. Clin. J. Am. Soc. Nephrol. 2011, 6, 1663–1667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, B.M.; Bieber, B.; Pisoni, R.L.; Port, F.K. Dialysis Outcomes and Practice Patterns Study (DOPPS): Its Strengths, Limitations, and Role in Informing Practices and Policies. Clin. J. Am. Soc. Nephrol. 2012, 7, 1897–1905. [Google Scholar] [CrossRef]
- DeSilva, R.N.; Patibandla, B.K.; Vin, Y.; Narra, A.; Chawla, V.; Brown, R.S.; Goldfarb-Rumyantzev, A.S. Fistula first is not always the best strategy for the elderly. J. Am. Soc. Nephrol. 2013, 24, 1297–1304. [Google Scholar] [CrossRef] [Green Version]
- Ibeas, J.; Roca-Tey, R.; Vallespín, J.; Moreno, T.; Moñux, G.; Martí-Monrós, A.; Del Pozo, J.L.; Gruss, E.; De Arellano, M.R.; Fontseré, N.; et al. Grupo Español Multidisciplinar del Acceso Vascular (GEMAV). Spanish Clinical Guidelines on Vascular Access for Haemodialysis. Nefrologia 2017, 37 (Suppl. 1), 1–177. [Google Scholar] [CrossRef]
- Bray, B.; Boyd, J.; Daly, C.; Donaldson, K.; Doyle, A.; Fox, J.G.; Innes, A.; Khan, I.; Peel, R.K.; Severn, A.; et al. Vascular access type and risk of mortality in a national prospective cohort of haemodialysis patients. QJM Int. J. Med. 2012, 105, 1097–1103. [Google Scholar] [CrossRef] [Green Version]
- Dhingra, R.K.; Young, E.W.; Hulbert-Shearon, T.; Leavey, S.F.; Port, F.K. Type of vascular access and mortality in U.S. hemodialysis patients. Kidney Int. 2001, 60, 1443–1451. [Google Scholar] [CrossRef] [Green Version]
- Polkinghorne, K.R.; McDonald, S.P.; Atkins, R.C.; Kerr, P.G. Vascular Access and All-Cause Mortality: A Propensity Score Analysis. J. Am. Soc. Nephrol. 2004, 15, 477–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pastan, S.; Soucie, J.M.; McClellan, W.M. Vascular access and increased risk of death among hemodialysis patients. Kidney Int. 2002, 62, 620–626. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sachdeva, M.; Hung, A.; Kovalchuk, O.; Bitzer, M.; Mokrzycki, M.H. The Initial Vascular Access Type Contributes to Inflammation in Incident Hemodialysis Patients. Int. J. Nephrol. 2011, 2012, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Dukkipati, R.; Molnar, M.Z.; Park, J.; Jing, J.; Kovesdy, C.P.; Kajani, R.; Kalantar-Zadeh, K. Association of Vascular Access Type with Inflammatory Marker Levels in Maintenance Hemodialysis Patients. Semin. Dial. 2013, 27, 415–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hung, A.; Pupim, L.; Yu, C.; Shintani, A.; Siew, E.; Ayus, C.; Hakim, R.M.; Ikizler, T.A. Determinants of C-reactive protein in chronic hemodialysis patients: Relevance of dialysis catheter utilization. Hemodial. Int. 2008, 12, 236–243. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, T.; Kim, S.J.; Astor, B.; Shafi, T.; Coresh, J.; Powe, N.R. Vascular Access Type, Inflammatory Markers, and Mortality in Incident Hemodialysis Patients: The Choices for Healthy Outcomes in Caring for End-Stage Renal Disease (CHOICE) Study. Am. J. Kidney Dis. 2014, 64, 954–961. [Google Scholar] [CrossRef] [Green Version]
- Wystrychowski, G.; Kitzler, T.M.; Thijssen, S.; Usvyat, L.; Kotanko, P.; Levin, N.W. Impact of switch of vascular access type on key clinical and laboratory parameters in chronic haemodialysis patients. Nephrol. Dial. Transplant. 2009, 24, 2194–2200. [Google Scholar] [CrossRef]
- Merino, A.; Nogueras, S.; Buendia, P.; Ojeda, R.; Carracedo, J.; Ramirez-Chamond, R.; Martín-Malo, A.; Aljama, P. Microinflammation and Endothelial Damage in Hemodialysis. Contrib Nephrol. 2008, 161, 83–88. [Google Scholar] [CrossRef]
- Cafiero, C.; Gigante, M.; Brunetti, G.; Simone, S.; Chaoul, N.; Oranger, A.; Ranieri, E.; Colucci, S.; Pertosa, G.B.; Grano, M.; et al. Inflammation induces osteoclast differentiation from peripheral mononuclear cells in chronic kidney disease patients: Crosstalk between the immune and bone systems. Nephrol Dial Transplant. 2018, 33, 65–75. [Google Scholar] [CrossRef] [Green Version]
- Colì, L.; Donati, G.; Cappuccilli, M.; Cianciolo, G.; Comai, G.; Cuna, V.; Carretta, E.; La Manna, G.; Stefoni, S. Role of the hemodialysis vascular access type in inflammation status and monocyte activation. Int. J. Artif. Organs 2011, 34, 481–488. [Google Scholar] [CrossRef]
- Fux, C.A.; Uehlinger, D.; Bodmer, T.; Droz, S.; Zellweger, C.; Mühlemann, K. Dynamics of hemodialysis catheter colonization by coagulase-negative staphylococci. Infect. Control. Hosp. Epidemiology 2005, 26, 567–574. [Google Scholar] [CrossRef] [PubMed]
- Thomson, P.C.; Stirling, C.M.; Geddes, C.C.; Morris, S.T.; Mactier, R.A. Vascular access in haemodialysis patients: A modifiable risk factor for bacteraemia and death. QJM Int. J. Med. 2007, 100, 415–422. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, S.L.; Ikizler, T.A.; Zappitelli, M.; Silverstein, D.M.; Ayus, J.C. Non-infected hemodialysis catheters are associated with increased inflammation compared to arteriovenous fistulas. Kidney Int. 2009, 76, 1063–1069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poinen, K.; Quinn, R.R.; Clarke, A.; Ravani, P.; Hiremath, S.; Miller, L.M.; Blake, P.G.; Oliver, M.J. Complications From Tunneled Hemodialysis Catheters: A Canadian Observational Cohort Study. Am. J. Kidney Dis. 2019, 73, 467–475. [Google Scholar] [CrossRef]
- Murea, M.; James, K.M.; Russell, G.B.; Byrum, G.V., 3rd; Yates, J.E.; Tuttle, N.S.; Bleyer, A.J.; Burkart, J.M.; Freedman, B.I. Risk of catheter-related bloodstream infection in elderly patients on hemodialysis. Clin. J. Am. Soc. Nephrol. 2014, 9, 764–770. [Google Scholar] [CrossRef] [Green Version]
- Albalate, M.; García, R.P.; De Sequera, P.; Alcázar, R.; Puerta, M.; Ortega, M.; Mossé, A.; Crespo, E.; Albalate, M.; García, R.P.; et al. Have we forgotten the most important thing to prevent bacteremias associated with tunneled hemodialysis catheters? Nefrología 2010, 30, 573–577. [Google Scholar] [CrossRef] [PubMed]
- Crespo-Garrido, M.; Ruiz-Parrado, M.C.; Gómez-Pozo, M.; Crespo-Montero, R. The bacteraemia related to the tunnelled catheter of haemodialysis and nursing care. Enferm. Nefrol. 2017, 20, 353–355. [Google Scholar] [CrossRef]
- Canaud, B.; Leray-Moragues, H.; Kerkeni, N.; Bosc, J.-Y.; Martin, K. Effective flow performances and dialysis doses delivered with permanent catheters: A 24-month comparative study of permanent catheters versus arterio-venous vascular accesses. Nephrol. Dial. Transplant. 2002, 17, 1286–1292. [Google Scholar] [CrossRef] [Green Version]
- Maduell, F.; Ramos, R.; Palomares, I.; Martín-Malo, A.; Molina, M.; Bustamante, J.; Pérez-García, R.; Grassmann, A.; Merello, J.I.; on behalf of the ORD Group. Impact of targeting Kt instead of Kt/V. Nephrol. Dial. Transplant. 2013, 28, 2595–2603. [Google Scholar] [CrossRef] [Green Version]
- National Kidney Foundation. KDOQI clinical practice guideline for hemodialysis adequacy: 2015 update. Am. J. Kidney Dis. 2015, 66, 884–930. [Google Scholar] [CrossRef] [Green Version]
- Tentori, F.; Zhang, J.; Li, Y.; Karaboyas, A.; Kerr, P.; Saran, R.; Bommer, J.; Port, F.; Akiba, T.; Pisoni, R.; et al. Longer dialysis session length is associated with better intermediate outcomes and survival among patients on in-center three times per week hemodialysis: Results from the Dialysis Outcomes and Practice Patterns Study (DOPPS). Nephrol. Dial. Transplant. 2012, 27, 4180–4188. [Google Scholar] [CrossRef]
- Brunelli, S.M.; Chertow, G.M.; Ankers, E.D.; Lowrie, E.G.; Thadhani, R. Shorter dialysis times are associated with higher mortality among incident hemodialysis patients. Kidney Int. 2010, 77, 630–636. [Google Scholar] [CrossRef] [Green Version]
- Maduell, F.; Ramos, R.; Varas, J.; Martin-Malo, A.; Molina, M.; Pérez-Garcia, R.; Marcelli, D.; Moreso, F.; Aljama, P.; Merello, J.I. Hemodialysis patients receiving a greater Kt dose than recommended have reduced mortality and hospitalization risk. Kidney Int. 2016, 90, 1332–1341. [Google Scholar] [CrossRef] [Green Version]
- Rebollo-Rubio, A.; Morales-Asencio, J.M.; Pons-Raventos, M.E.; Mansilla-Francisco, J.J. Review of studies on health related quality of life in patients with advanced chronic kidney disease in Spain. Nefrologia 2015, 35, 92–109. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Park, J.I.; Lee, J.P.; Kim, Y.-L.; Kang, S.-W.; Yang, C.W.; Kim, N.-H.; Kim, Y.S.; Lim, C.S. The effects of vascular access types on the survival and quality of life and depression in the incident hemodialysis patients. Ren. Fail. 2019, 42, 30–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ng, L.J.; Chen, F.; Pisoni, R.L.; Krishnan, M.; Mapes, D.; Keen, M.; Bradbury, B.D. Hospitalization risks related to vascular access type among incident US hemodialysis patients. Nephrol Dial Transplant. 2011, 26, 3659–3666. [Google Scholar] [CrossRef] [Green Version]
- Bradbury, B.D.; Fissell, R.B.; Albert, J.; Anthony, M.S.; Critchlow, C.W.; Pisoni, R.L.; Port, F.K.; Gillespie, B.W. Predictors of Early Mortality among Incident US Hemodialysis Patients in the Dialysis Outcomes and Practice Patterns Study (DOPPS). Clin. J. Am. Soc. Nephrol. 2007, 2, 89–99. [Google Scholar] [CrossRef]
- Allon, M.; Daugirdas, J.; Depner, T.A.; Greene, T.; Ornt, D.; Schwab, S.J. Effect of change in vascular access on patient mortality in hemodialysis patients. Am. J. Kidney Dis. 2006, 47, 469–477. [Google Scholar] [CrossRef]
- Astor, B.C.; Eustace, J.A.; Powe, N.R.; Klag, M.J.; Fink, N.E.; Coresh, J. CHOICE Study. Type of vascular access and survival among incident hemodialysis patients: The Choices for Healthy Outcomes in Caring for ESRD (CHOICE) Study. J. Am. Soc. Nephrol. 2005, 16, 1449–1455. [Google Scholar] [CrossRef] [Green Version]
- Pisoni, R.L.; Arrington, C.J.; Albert, J.; Ethier, J.; Kimata, N.; Krishnan, M.; Rayner, H.C.; Saito, A.; Sands, J.J.; Saran, R.; et al. Facility hemodialysis vascular access use and mortality in countries participating in DOPPS: An instrumental variable analysis. Am. J. Kidney Dis. 2009, 53, 475–491. [Google Scholar] [CrossRef]
- Di Iorio, B.R.; Bellizzi, V.; Cillo, N.; Cirillo, M.; Avella, F.; Andreucci, V.E.; De Santo, N.G. Vascular access for hemodialysis: The impact on morbidity and mortality. J. Nephrol. 2004, 17, 19–25. [Google Scholar]
- Ravani, P.; Palmer, S.C.; Oliver, M.J.; Quinn, R.R.; MacRae, J.; Tai, D.J.; Pannu, N.I.; Thomas, C.; Hemmelgarn, B.R.; Craig, J.; et al. Associations between hemodialysis access type and clinical outcomes: A systematic review. J. Am. Soc. Nephrol. 2013, 24, 465–473. [Google Scholar] [CrossRef]
- De Clerck, D.; Bonkain, F.; Cools, W.; Van Der Niepen, P. Vascular access type and mortality in haemodialysis: A retrospective cohort study. BMC Nephrol. 2020, 21, 231. [Google Scholar] [CrossRef]
- Quinn, R.R.; Oliver, M.J.; DeVoe, D.; Poinen, K.; Kabani, R.; Kamar, F.; Mysore, P.; Lewin, A.; Hiremath, S.; MacRae, J.; et al. The impact of fistula attempt pre-dialysis on risk of all-cause and access-related death. J. Am. Soc. Nephrol. 2017, 28, 613–620. [Google Scholar] [CrossRef] [Green Version]
- Brown, R.S.; Patibandla, B.K.; Goldfarb-Rumyantzev, A.S. The survival benefit of “Fistula First, Catheter Last” in hemodialysis is primarily due to patient factors. J. Am. Soc. Nephrol. 2017, 28, 645–652. [Google Scholar] [CrossRef] [Green Version]
- Mehrotra, R.; Cheung, A.K.; Meyer, T.; Nath, K.A. Vascular Access for Hemodialysis and Value-Based Purchasing for ESRD. J. Am. Soc. Nephrol. 2017, 28, 395–397. [Google Scholar] [CrossRef] [Green Version]
- Drew, D.A.; Lok, C.; Cohen, J.; Wagner, M.; Tangri, N.; Weiner, D.E. Vascular access choice in incident hemodialysis patients: A decision analysis. J. Am. Soc. Nephrol. 2014, 26, 183–191. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total Patients (n = 108) | AVF (n = 54) | VCC (n = 54) | p-Value | |
|---|---|---|---|---|
| Age (years) | 79 (70–83) | 79 (70–83) | 79.5 (69–84) | 0.848 |
| Sex (women) | 60 (56%) | 30 (56%) | 30 (56%) | |
| Time on HD regimen (months) | 62.6 ± 39.5 | 62.3 ± 39.6 | 62.8 ± 39.8 | 0.952 |
| Presence of diabetes | 42 (39%) | 21 (39%) | 21 (39%) | |
| Dialysis Technique Mode | ||||
| HD mode | 80 (74%) | 29 (31%) | 51 (69%) | * |
| OL-HDF | 28 (26%) | 25 (89%) | 3 (11%) | * |
| CKD aetiology | ||||
| CKD of unknown origin | 45 (42%) | 25 (46%) | 20 (37%) | * |
| Diabetic nephropathy | 22 (20%) | 11 (20%) | 11 (20%) | * |
| Glomerulonephritis | 11 (10%) | 5 (9%) | 6 (11%) | * |
| Polycystic | 11 (10%) | 5 (9%) | 6 (11%) | * |
| Interstitial | 7 (7%) | 3 (6%) | 4 (8%) | * |
| Vascular | 4 (4%) | 2 (4%) | 2 (4%) | * |
| Other | 8 (8%) | 3 (6%) | 5 (9%) | * |
| Total Patients (n = 108) | AVF (n = 54) | VCC (n = 54) | p-Value | |
|---|---|---|---|---|
| CRP (mg/L) | 4.9 (2.4–11.4) | 3.4 (1.5–7.9) | 7.4 (3.6–17.6) | 0.002 |
| Serum albumin (g/dL) | 3.7 (3.4–3.9) | 3.8 (3.5–3.9) | 3.7 (3.3–3.9) | 0.078 |
| Serum ferritin (ng/dL) | 540.8 ± 353.2 | 455.2 ± 352.7 | 625.5 ± 335.9 | 0.011 |
| % CD14+/CD16+ monocytes | 47.4 ± 12.3 | 43.6 ± 12.7 | 51.2 ± 10.9 | 0.001 |
| % CD14+/CD16- monocytes | 26.8 ± 12.3 | 27.4 ± 13.1 | 26.1 ± 11.7 | 0.595 |
| Total Patients (n = 108) | AVF (n = 54) | VCC (n = 54) | p-Value | |
|---|---|---|---|---|
| SBP (mmHg) | 140.1 ± 28 | 145.2 ± 27 | 135 ± 28 | 0.069 |
| DBP (mmHg) | 71.3 ± 17 | 71.7 ± 14 | 71 ± 19 | 0.806 |
| Haemoglobin (g/dL) | 11.1 ± 1.2 | 11.4 ± 1 | 10.9 ± 1.5 | 0.55 |
| Phosphate (mg/dL) | 4.0 ± 1.0 | 3.8 ± 1.0 | 4.2 ± 1.1 | 0.083 |
| Potassium (mEq/L) | 5.1 ± 0.8 | 4.8 ± 0.8 | 5.4 ± 0.8 | 0.000 |
| PTH pg/mL | 229.6 (141–365) | 223.6 (138–346) | 276.2 (142–412) | 0.588 |
| HD session duration (minutes) | 250 (245–250) | 250.3 (245–250) | 249.3 (245–252) | 0.564 |
| Volume of treated blood (liters) | 94.1 ± 19.4 | 102.3 ± 19.5 | 85.8 ± 15.4 | 0.000 |
| Blood flow (mL/min) | 388.7 ± 75.8 | 421.2 ± 75.2 | 354.9 ± 54.1 | 0.000 |
| Kt (liters) | 52.8 ± 8.9 | 57.5 ± 7.3 | 48.4 ± 7.8 | 0.000 |
| Kt/V | 1.9 ± 0.5 | 2.0 ± 0.5 | 1.74 ± 0.5 | 0.005 |
| CCI (points) | 7 (6–9) | 7 (6–9) | 7 (6–9) | 0.899 |
| Hospitalization (days) | 8 (0–19) | 7 (0–18.2) | 9 (0–25) | 0.526 |
| Total Patients (n = 108) | AVF Deaths (n = 21) | VCC Deaths (n = 27) | |
|---|---|---|---|
| Undetermined cause | 10 (21%) | 6 (29%) | 4 (14%) |
| Septicemia | 5 (11%) | 1 (4%) | 4 (14%) |
| Other causes of heart failure | 5 (11%) | 4 (19%) | 1 (4%) |
| Stroke | 5 (11%) | 1 (4%) | 4 (14%) |
| Mesenteric infarction | 4 (8%) | 1 (4%) | 3 (11%) |
| Malignant disease | 3 (6%) | 1 (4%) | 2 (7%) |
| Other bleeds | 3 (6%) | 2 (10%) | 1 (4%) |
| Lung infection | 3 (6%) | 1 (4%) | 2 (7%) |
| Treatment interruption | 2 (4%) | 1 (4%) | 1 (4%) |
| CRP of unknown origin | 2 (4%) | 2 (10%) | |
| Epileptic status | 1 (2%) | 1 (4%) | |
| Acute myocardial infarction | 1 (2%) | 1 (4%) | |
| Cachexia | 1 (2%) | 1 (4%) | |
| Subdural haematoma | 1 (2%) | 1 (4%) | |
| Septic shock | 1 (2%) | 1 (4%) | |
| Peritonitis | 1 (2%) | 1 (4%) |
| Crude Estimate | Adjusted Estimate | |||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Age | 1.064 | 1.024–1.106 | 0.001 | 1.056 | 1.015–1.098 | 0.007 |
| Sex (ref. woman) | 1.174 | 0.666–2.069 | 0.579 | |||
| Vascular access (ref. AVF) | 1.458 | 0.824–2.579 | 0.195 | |||
| Diabetes (ref. absence of diabetes) | 0.855 | 0.476–1.533 | 0.598 | |||
| SBP | 0.998 | 0.988–1.008 | 0.673 | |||
| DBP | 0.984 | 0.967–1.003 | 0.094 | |||
| Kt/V | 1.314 | 0.735–2.349 | 0.357 | |||
| Kt | 0.974 | 0.944–1.005 | 0.094 | |||
| HD session duration | 0.989 | 0.970–1.008 | 0.249 | |||
| Volume of treated blood | 0.995 | 0.980–1.010 | 0.520 | |||
| Blood flow | 1.000 | 0.996–1.004 | 0.928 | |||
| CRP | 1.005 | 0.995–1.016 | 0.306 | |||
| Serum albumin | 0.466 | 0.244–0.890 | 0.021 | 0.435 | 0.224–0.845 | 0.014 |
| Serum ferritin | 1.001 | 1.000–1.001 | 0.113 | |||
| CCI | 1.165 | 1.023–1.327 | 0.021 | |||
| HD weather | 1.005 | 0.998–1.012 | 0.165 | |||
| % CD14+/CD16+ | 1.012 | 0.989–1.036 | 0.317 | 1.022 | 0.997–1.047 | 0.089 |
| % CD14+/CD16- | 0.994 | 0.972–1.018 | 0.635 | |||
| Haemoglobin | 0.932 | 0.749–1.159 | 0.534 | |||
| Serum phosphorus | 0.687 | 0.520–0.909 | 0.009 | 0.750 | 0.569–0.989 | 0.041 |
| Serum potassium | 0.832 | 0.586–1.180 | 0.302 | |||
| PTH | 1.000 | 0.999–1.001 | 0.507 | |||
| Length of stay | 0.996 | 0.976–1.016 | 0.684 | |||
| Dialysis mode | 0.706 | 0.352–1.418 | 0.328 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crespo-Montero, R.; Gómez-López, V.E.; Guerrero-Pavón, F.; Carmona-Muñoz, A.; Romero-Saldaña, M.; Ranchal-Sanchez, A.; Aljama-García, P. Influence of Tunneled Hemodialysis-Catheters on Inflammation and Mortality in Dialyzed Patients. Int. J. Environ. Res. Public Health 2021, 18, 7605. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147605
Crespo-Montero R, Gómez-López VE, Guerrero-Pavón F, Carmona-Muñoz A, Romero-Saldaña M, Ranchal-Sanchez A, Aljama-García P. Influence of Tunneled Hemodialysis-Catheters on Inflammation and Mortality in Dialyzed Patients. International Journal of Environmental Research and Public Health. 2021; 18(14):7605. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147605
Chicago/Turabian StyleCrespo-Montero, Rodolfo, Victoria E. Gómez-López, Fátima Guerrero-Pavón, Andrés Carmona-Muñoz, Manuel Romero-Saldaña, Antonio Ranchal-Sanchez, and Pedro Aljama-García. 2021. "Influence of Tunneled Hemodialysis-Catheters on Inflammation and Mortality in Dialyzed Patients" International Journal of Environmental Research and Public Health 18, no. 14: 7605. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147605