
Is Hip Muscle Strength Associated with Dynamic Knee Valgus in a Healthy Adult Population? A Systematic Review

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Eligibility Criteria
2.2. Study Search Process
2.3. Data Collection and Extraction
2.4. Types of Outcome Measures
2.5. Assessment of Risk of Bias
3. Results
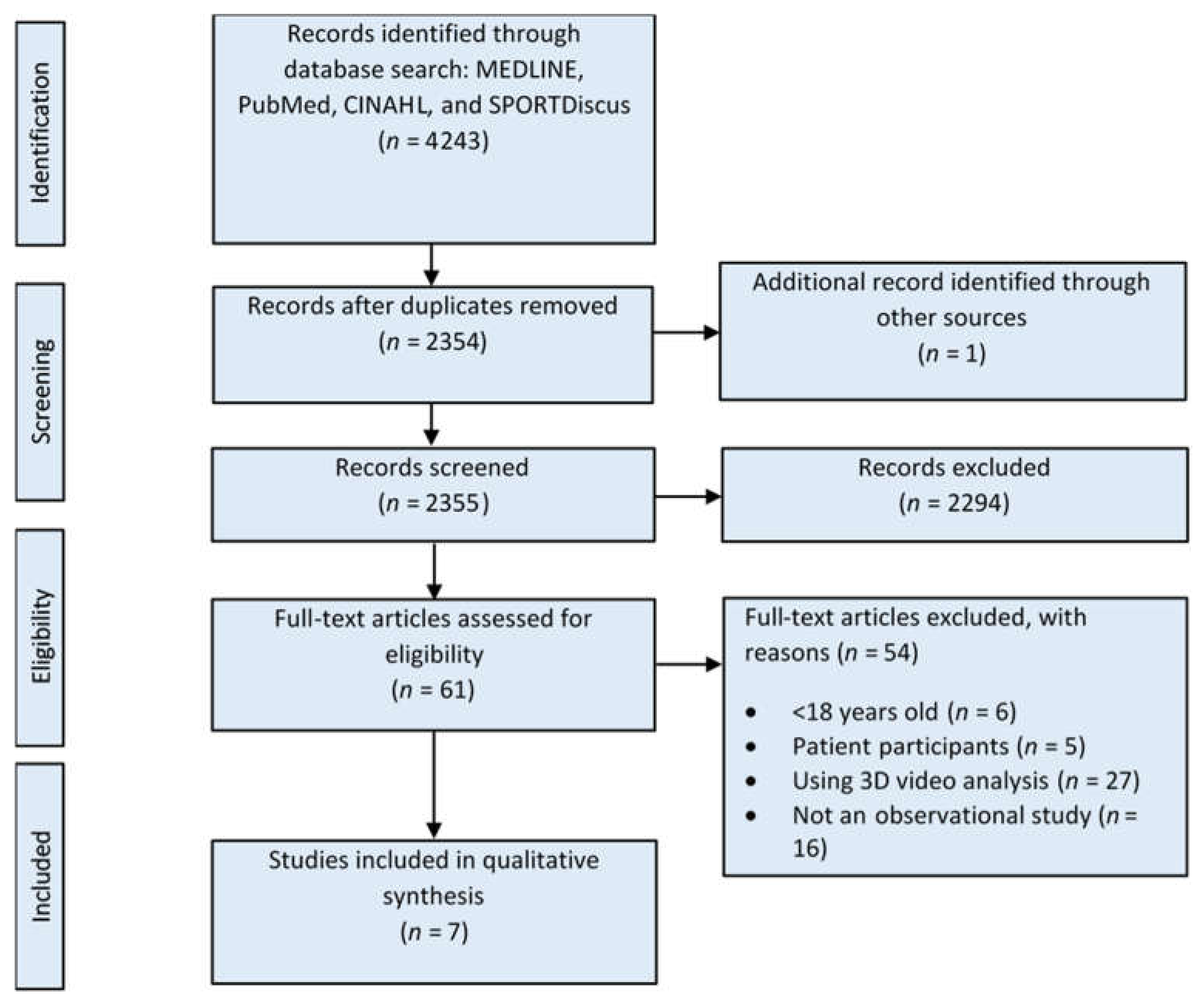
3.1. Results of the Search Process
3.2. Risk of Bias in the Included Studies
3.3. Characteristics of the Included Studies
3.4. Characteristics of the Participants
3.5. Measurement Methods of Hip Muscle Strength and Dynamic Knee Valgus
3.5.1. Hip Strength Assessment
3.5.2. Dynamic Knee Valgus Assessment
3.6. Relationship between the Strength of Hip Muscles and Dynamic Knee Valgus
3.6.1. Relationship between Hip Abductor Strength and Dynamic Knee Valgus
3.6.2. Relationship between Hip Extensor Strength and Dynamic Knee Valgus
3.6.3. Relationship between Hip External Rotator Strength and Dynamic Knee Valgus
4. Discussion
5. Conclusion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sharma, L.; Song, J.; Felson, D.T.; Cahue, S.; Shamiyeh, E.; Dunlop, D.D. The role of knee alignment in disease progression and functional decline in knee osteoarthritis. JAMA 2001, 286, 188–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanamas, S.; Hanna, F.S.; Cicuttini, F.M.; Wluka, A.E.; Berry, P.; Urquhart, D.M. Does knee malalignment increase the risk of development and progression of knee osteoarthritis? A systematic review. Arthritis Rheum. 2009, 61, 459–467. [Google Scholar] [CrossRef] [PubMed]
- Walden, M.; Krosshaug, T.; Bjorneboe, J.; Andersen, T.E.; Faul, O.; Hagglund, M. Three distinct mechanisms predominate in non-contact anterior cruciate ligament injuries in male professional football players: A systematic video analysis of 39 cases. Br. J. Sports Med. 2015, 49, 1452–1460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tetsworth, K.; Paley, D. Malalignment and degenerative arthropathy. Orthop. Clin. N. Am. 1994, 25, 367–377. [Google Scholar] [CrossRef]
- Reiman, M.P.; Bolgla, L.A.; Lorenz, D. Hip functions influence on knee dysfunction: A proximal link to a distal problem. J. Sport Rehabil. 2009, 18, 33–46. [Google Scholar] [CrossRef]
- Powers, C.M. The influence of abnormal hip mechanics on knee injury: A biomechanical perspective. J. Orthop. Sports Phys. Ther. 2010, 40, 42–51. [Google Scholar] [CrossRef] [Green Version]
- Vleeming, A. The role of the pelvic girdle in coupling the spine and the legs: A clinical–anatomical perspective on pelvic stability. In Movement, Stability & Lumbopelvic Pain; Vleeming, A., Mooney, V., Stoeckart, R., Wilson, P., Eds.; Churchill Livingstone: Edinburgh, UK, 1995; pp. 113–137. [Google Scholar]
- Williams, G.N.; Chmielewski, T.; Rudolph, K.; Buchanan, T.S.; Snyder-Mackler, L. Dynamic knee stability: Current theory and implications for clinicians and scientists. J. Orthop. Sports Phys. Ther. 2001, 31, 546–566. [Google Scholar] [CrossRef] [Green Version]
- Claiborne, T.L.; Armstrong, C.W.; Gandhi, V.; Pincivero, D.M. Relationship between hip and knee strength and knee valgus during a single leg squat. J. Appl. Biomech. 2006, 22, 41–50. [Google Scholar] [CrossRef] [Green Version]
- Cashman, G.E. The effect of weak hip abductors or external rotators on knee valgus kinematics in healthy subjects: A systematic review. J. Sport Rehabil. 2012, 21, 273–284. [Google Scholar] [CrossRef] [Green Version]
- Dix, J.; Marsh, S.; Dingenen, B.; Malliaras, P. The relationship between hip muscle strength and dynamic knee valgus in asymptomatic females: A systematic review. Phys. Ther. Sport 2019, 37, 197–209. [Google Scholar] [CrossRef] [Green Version]
- Hunter, D.J.; Zhang, Y.; Niu, J.; Tu, X.; Amin, S.; Goggins, J.; Lavalley, M.; Guermazi, A.; Gale, D.; Felson, D.T. Structural factors associated with malalignment in knee osteoarthritis: The Boston osteoarthritis knee study. J. Rheumatol. 2005, 32, 2192–2199. [Google Scholar]
- Baida, S.R.; Gore, S.J.; Franklyn-Miller, A.D.; Moran, K.A. Does the amount of lower extremity movement variability differ between injured and uninjured populations? A systematic review. Scand. J. Med. Sci. Sports 2018, 28, 1320–1338. [Google Scholar] [CrossRef]
- Rabelo, N.; Lucareli, P.R.G. Do hip muscle weakness and dynamic knee valgus matter for the clinical evaluation and decision-making process in patients with patellofemoral pain? Braz. J. Phys. Ther. 2018, 22, 105–109. [Google Scholar] [CrossRef]
- Ekegren, C.L.; Miller, W.C.; Celebrini, R.G.; Eng, J.J.; Macintyre, D.L. Reliability and validity of observational risk screening in evaluating dynamic knee valgus. J. Orthop. Sports Phys. Ther. 2009, 39, 665–674. [Google Scholar] [CrossRef] [Green Version]
- McLean, S.G.; Walker, K.; Ford, K.R.; Myer, G.D.; Hewett, T.E.; van den Bogert, A.J. Evaluation of a two dimensional analysis method as a screening and evaluation tool for anterior cruciate ligament injury. Br. J. Sports Med. 2005, 39, 355–362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maykut, J.N.; Taylor-Haas, J.A.; Paterno, M.V.; DiCesare, C.A.; Ford, K.R. Concurrent validity and reliability of 2d kinematic analysis of frontal plane motion during running. Int. J. Sports Phys. Ther. 2015, 10, 136–146. [Google Scholar] [PubMed]
- Herrington, L.; Alenezi, F.; Alzhrani, M.; Alrayani, H.; Jones, R. The reliability and criterion validity of 2D video assessment of single leg squat and hop landing. J. Electromyogr. Kinesiol. 2017, 34, 80–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; Group, P.-P. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Zou, K.H.; Tuncali, K.; Silverman, S.G. Correlation and simple linear regression. Radiology 2003, 227, 617–622. [Google Scholar] [CrossRef]
- Joanna Briggs Institute. The Joanna Briggs Institute Critical Appraisal Tools. Available online: https://jbi.global/critical-appraisal-tools (accessed on 2 July 2021).
- Almeida, G.P.; Silva, A.P.; Franca, F.J.; Magalhaes, M.O.; Burke, T.N.; Marques, A.P. Relationship between frontal plane projection angle of the knee and hip and trunk strength in women with and without patellofemoral pain. J. Back Musculoskelet. Rehabil. 2016, 29, 259–266. [Google Scholar] [CrossRef]
- Hollman, J.H.; Ginos, B.E.; Kozuchowski, J.; Vaughn, A.S.; Krause, D.A.; Youdas, J.W. Relationships between knee valgus, hip-muscle strength, and hip-muscle recruitment during a single-limb step-down. J. Sport Rehabil. 2009, 18, 104–117. [Google Scholar] [CrossRef]
- Willson, J.D.; Ireland, M.L.; Davis, I. Core strength and lower extremity alignment during single leg squats. Med. Sci. Sports Exerc. 2006, 38, 945–952. [Google Scholar] [CrossRef] [Green Version]
- Bin Hussein, A. The Relationship between Hip Strength and Peak Knee Valgus Angle during Single Leg Squat. Nurs. Health Sci. 2016, 5, 99–106. [Google Scholar] [CrossRef]
- Stickler, L.; Finley, M.; Gulgin, H. Relationship between hip and core strength and frontal plane alignment during a single leg squat. Phys. Ther. Sport 2015, 16, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Thijs, Y.; Van Tiggelen, D.; Willems, T.; De Clercq, D.; Witvrouw, E. Relationship between hip strength and frontal plane posture of the knee during a forward lunge. Br. J. Sports Med. 2007, 41, 723–727. [Google Scholar] [CrossRef] [Green Version]
- Waldhelm, A.; Li, L. Weak Relationships Between Three Clinical Assessments and Core Stability Tests. EC Orthop. 2017, 7, 88. [Google Scholar]
- Willson, J.D.; Davis, I.S. Utility of the frontal plane projection angle in females with patellofemoral pain. J. Orthop. Sports Phys. Ther. 2008, 38, 606–615. [Google Scholar] [CrossRef]
- Katoh, M.; Yamasaki, H. Comparison of reliability of isometric leg muscle strength measurements made using a hand-held dynamometer with and without a restraining belt. J. Phys. Ther. Sci. 2009, 21, 37–42. [Google Scholar] [CrossRef] [Green Version]
- Thorborg, K.; Petersen, J.; Magnusson, S.P.; Holmich, P. Clinical assessment of hip strength using a hand-held dynamometer is reliable. Scand. J. Med. Sci. Sports 2010, 20, 493–501. [Google Scholar] [CrossRef]
- Thorborg, K.; Bandholm, T.; Schick, M.; Jensen, J.; Holmich, P. Hip strength assessment using handheld dynamometry is subject to intertester bias when testers are of different sex and strength. Scand. J. Med. Sci. Sports 2013, 23, 487–493. [Google Scholar] [CrossRef]
- Zeller, B.L.; McCrory, J.L.; Kibler, W.B.; Uhl, T.L. Differences in kinematics and electromyographic activity between men and women during the single-legged squat. Am. J. Sports Med. 2003, 31, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Donohue, M.R.; Ellis, S.M.; Heinbaugh, E.M.; Stephenson, M.L.; Zhu, Q.; Dai, B. Differences and correlations in knee and hip mechanics during single-leg landing, single-leg squat, double-leg landing, and double-leg squat tasks. Res. Sports Med. 2015, 23, 394–411. [Google Scholar] [CrossRef] [PubMed]
- Lima, Y.L.; Ferreira, V.; de Paula Lima, P.O.; Bezerra, M.A.; de Oliveira, R.R.; Almeida, G.P.L. The association of ankle dorsiflexion and dynamic knee valgus: A systematic review and meta-analysis. Phys. Ther. Sport 2018, 29, 61–69. [Google Scholar] [CrossRef]
- Horan, S.A.; Watson, S.L.; Carty, C.P.; Sartori, M.; Weeks, B.K. Lower-limb kinematics of single-leg squat performance in young adults. Physiother. Can. 2014, 66, 228–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Earl, J.E.; Monteiro, S.K.; Snyder, K.R. Differences in lower extremity kinematics between a bilateral drop-vertical jump and a single-leg step-down. J. Orthop. Sports Phys. Ther. 2007, 37, 245–252. [Google Scholar] [CrossRef]
- Mornieux, G.; Gehring, D.; Tokuno, C.; Gollhofer, A.; Taube, W. Changes in leg kinematics in response to unpredictability in lateral jump execution. Eur. J. Sport Sci. 2014, 14, 678–685. [Google Scholar] [CrossRef]
- Pappas, E.; Hagins, M.; Sheikhzadeh, A.; Nordin, M.; Rose, D. Biomechanical differences between unilateral and bilateral landings from a jump: Gender differences. Clin. J. Sport Med. 2007, 17, 263–268. [Google Scholar] [CrossRef]
- McLean, S.G.; Walker, K.B.; van den Bogert, A.J. Effect of gender on lower extremity kinematics during rapid direction changes: An integrated analysis of three sports movements. J. Sci. Med. Sport 2005, 8, 411–422. [Google Scholar] [CrossRef] [Green Version]
- Krosshaug, T.; Nakamae, A.; Boden, B.P.; Engebretsen, L.; Smith, G.; Slauterbeck, J.R.; Hewett, T.E.; Bahr, R. Mechanisms of anterior cruciate ligament injury in basketball: Video analysis of 39 cases. Am. J. Sports Med. 2007, 35, 359–367. [Google Scholar] [CrossRef]
- Case, L.D.; Ambrosius, W.T. Power and Sample Size. In Topics in Biostatistics; Ambrosius, W.T., Ed.; Humana Press: Totowa, NJ, USA, 2007; ISBN 978-1-59745-530-5. [Google Scholar]
- Kraemer, H.C.; Blasey, C. How Many Subjects? Statistical Power Analysis in Research; Sage Publications: Thousand Oaks, CA, USA, 2015; ISBN 978-1-4833-1954-4. [Google Scholar]


{kind=link}
| Search | Query |
|---|---|
| 1 | Hip* |
| 2 | Results of item number 1 limited to English and human studies |
| 3 | Knee* |
| 4 | Results of item number 3 limited to English and human studies |
| 5 | Step down* OR drop vertical jump test OR single leg* OR single limb* OR drop jump* OR dynamic activities OR functional task OR leg drop OR leg jump OR jump* OR leg hop* OR hop* |
| 6 | Results of item number 3 limited to English and human studies |
| 7 | Results of item numbers 2, 4, and 6 were combined with “AND” |
| Author, Year | Study Design | Population | Sex | Age, Weight, Height | Hip Muscle Strength Measurement | Kinematic Measurement | Camera Model | Software |
|---|---|---|---|---|---|---|---|---|
| Almeida et al. [22], 2016 | Cross-sectional case-control study | Healthy volunteers | 21 F | 18–45 (27.3 ± 4.5) years, 60.8 ± 7.3 kg, 1.63 ± 0.05 m | Isometric muscle torque using HHD | 2D video analysis | Sony Cyber-shot DSC-W35 | VirtualDub software (Copyright Avery Lee 1998–2009) |
| Bin Hussein [25], 2016 | Cross-sectional study | General college population | 17 F and 13 M | 18–38 years, 68.3 ± 9.8 kg, 171.1 ± 7.2 cm | Isometric muscle testing using a Dillon EDjunior dynamometer, measured in kilogram–force (kgf) | 2D video analysis | Sony DCRTRV19E (Japan) | SiliconCOACH Pro Version 6 (SiliconCOACH Ltd.; New Zealand) |
| Hollman et al. [23], 2009 | Cross-sectional study | Healthy volunteers | 20 F | 24 ± 2.6 years, 66.4 ± 9.3 kg, 169.1 ± 9.4 cm | Maximum isometric force production capability using HHD | 2D video analysis | Sony DCR-HC65 (Sony Corp. of America; New York, NY, USA) | DX9–Shareware version 2.6 software (The Rehabilitation Centre; Ottawa, ON, Canada) |
| Stickler et al. [26], 2015 | Cross-sectional study | Healthy volunteers | 40 F | 18–30 (22.88 ± 0.32) years, 60.36 ± 1.7 kg, 165.5 ± 0.86 cm | Isometric “make” test using HHD used to assess peak force | 2D video analysis | Sony Handycam DCR-HC37 | Dartfish (Alpharetta, GA, USA) |
| Thijs et al. [27], 2007 | Cross-sectional study | Healthy volunteers from a military academy | 8 F and 76 M | 18–30 years, average weight of 70.2 kg, average height of 177.7 cm | Isometric muscle testing using HHD with the examiner’s hand holding the dynamometer | 2D video analysis | Sony HC20E camera (Sony Corp.; Tokyo, Japan) | Dartfish video software solutions (Fribourg, Switzerland) |
| Waldhelm et al. [28], 2017 | Cross-sectional study | Healthy volunteers from a university population | 18 F and 18 M | F: 21.0 ± 1.2 years, 69.4 ± 13.2 kg, 165.4 ± 8.4 cm M: 30.4 ± 6.4 years, 69.8 ± 9.2 kg, 1.7 ± 0.1 m | Isometric strength tests using Biodex System 3 Pro | 2D video analysis | AIPTEK INC. (Irving, CA, USA) | CorrelDraw (Chicago, IL, USA) |
| Willson et al. [24], 2006 | Cross-sectional study | Active athletes | 22 F and 24 M | F: 19.4 ± 0.7 years, 66 ± 6.4 kg, 1.72 ± 0.07 m M: 19.9 ± 2.3 years, 79.8 ± 10.4 kg, 183 ± 0.10 m | Peak isometric torque using HHD | 2D video analysis | Digital camera | CorrelDraw (Chicago, IL, USA) |
| First Author, Year | Functional Tasks | Hip Muscle Group Measured | Relationship Between Hip Muscle Strength and Dynamic Knee Valgus |
|---|---|---|---|
| Almeida et al. [22], 2016 | Single-leg step-down | Abductors | Weak negative correlation (r = −0.31, p = 0.047) |
| Extensors | Nonsignificant correlation (r = −0.15, p > 0.05) | ||
| External rotators | Nonsignificant correlation (r = −0.28, p > 0.05) | ||
| Bin Hussein [25], 2016 | Single-leg squat | Abductors | Moderate negative correlation (r = −0.550, p = 0.002) |
| Extensors | Moderate negative correlation (r = −0.421, p = 0.021) | ||
| External rotators | Nonsignificant correlation (r = −0.206, p = 0.275) | ||
| Hollman et al. [23], 2009 | Single-limb step down | Abductors | Weak positive correlation (r = 0.455, p = 0.022) |
| External rotators | Nonsignificant correlation (r = 0.124, p > 0.05) | ||
| Stickler et al. [26], 2015 | Single-leg squat | Abductors | Weak positive correlation (r = 0.466, p = 0.002) |
| Extensors | Weak negative correlation (r = −0.396, p = 0.012) | ||
| External rotators | Weak positive correlation (r = 0.464, p = 0.003) | ||
| Thijs et al. [27], 2007 | Forward lunge | Abductors | Nonsignificant correlation (r = −0.002, p = 0.99) |
| Extensors | Nonsignificant correlation (r = 0.11, p = 0.49) | ||
| External rotators | Nonsignificant correlation (r = −0.05, p = 0.75) | ||
| Waldhelm et al. [28], 2017 | Single-leg squat and single-leg drop | Abductors | Single-leg squat: Nonsignificant correlation (r2 = 0.002, p > 0.05) Single-leg drop: Nonsignificant correlation (r2 = 0.00004, p > 0.05) |
| Extensors | Single-leg squat: Nonsignificant correlation (r2 = 0.006, p > 0.05) Single-leg drop: Nonsignificant correlation (r2 = 0.032, p > 0.05) | ||
| External rotators | Single-leg squat: Nonsignificant correlation (r2 = 0.02, p > 0.05) Single-leg drop: Nonsignificant correlation (r2 = 0.003, p > 0.05) | ||
| Willson et al. [24], 2006 | Single-leg squat | Abductors | Nonsignificant correlation (r = 0.23, p = 0.07) |
| External rotators | Weak positive correlation (r = 0.4, p = 0.004) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alzahrani, A.M.; Alzhrani, M.; Alshahrani, S.N.; Alghamdi, W.; Alqahtani, M.; Alzahrani, H. Is Hip Muscle Strength Associated with Dynamic Knee Valgus in a Healthy Adult Population? A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 7669. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147669
Alzahrani AM, Alzhrani M, Alshahrani SN, Alghamdi W, Alqahtani M, Alzahrani H. Is Hip Muscle Strength Associated with Dynamic Knee Valgus in a Healthy Adult Population? A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(14):7669. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147669
Chicago/Turabian StyleAlzahrani, Ali Mohammed, Msaad Alzhrani, Saeed Nasser Alshahrani, Wael Alghamdi, Mazen Alqahtani, and Hosam Alzahrani. 2021. "Is Hip Muscle Strength Associated with Dynamic Knee Valgus in a Healthy Adult Population? A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 14: 7669. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147669