
mHealth for the Monitoring of Brace Compliance and Wellbeing in Adolescents with Idiopathic Scoliosis: Study Protocol for a Feasibility Study

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
- Age between 10 and 18 years when the brace is prescribed, Risser 0–2 and, if female, either before menarche or less than 1 year after menarche
- Primary curve angles 25°–40°.
- No prior brace treatment.
- The patient has a mobile phone with an Android or iOS operating system.
- The patient has the physical ability to use the mobile application.
- The patient does not present a serious psychological and/or cognitive problem or language alterations.
- Signed informed consent.
- Exclusion criteria:
- Not having a mobile phone or having a mobile phone with incompatible characteristics (i.e., unable to download the app).
- The patient has cognitive impairment or language problems to understand the use of the app and/or answer its questions.
- The patient has a serious mental health or substance abuse problem.
2.2. Recruitment and Procedures
2.3. Usual AIS Treatment + App-Based Ecological Momentary Assessment
2.4. Physical Medicine and Rehabilitation Service Support According to Clinical Alarms
2.5. Outcome Measures
- The usability and acceptability of the app will be assessed by both patients (end users) and clinicians (relevant stakeholders). In the patients, this is evaluated both objectively and subjectively. To obtain an objective feasibility result, we calculate the adherence with the app by dividing the number of completed assessments by the number of planned evaluations and provide the response rate. To obtain a subjective measure of usability and acceptability, at the end of the study period (3 months after the first use of the app), we administer the System Usability Scale (SUS) [31] using an online survey tool that will be sent by mail (Qualtrics).In the clinicians, the acceptability of the new app-based monitoring method is evaluated using an assessment protocol developed for a similar earlier study [16]. As reported in Appendix D, this includes items that are consistent with the technology acceptance model [32], including perceived utility, acceptability, and intended use. This will be evaluated at the end of the study with the Qualtrics online survey tool anonymously.
- Brace adherence: Ad hoc self-reported item: “When have you been able to wear the brace since you went to bed yesterday?” Response options cover all daily periods (morning only, afternoon only, only for sleeping, or any combination of these). To avoid bias due to socially desirable responses, honesty will be encouraged both during recruitment and in the informed consent.
- Treatment safety: An ad hoc question has been created including the most frequent side effects of brace use according to the literature [10,12] and the authors’ clinical expertise. These include: pain due to pressure, pain due to friction, excessive heat/sweating, movement difficulties, and being teased by peers or close ones.
- Clinical alarms: in addition to the assessment of brace adherence and side effects, several items were adapted from validated questionnaires (Appendix D) to assess pain intensity, unpleasant emotions, interference, avoidance, discomfort, and social support daily. Clinical alarms will be automatically generated and sent to the physicians by the app depending on the patients’ responses to these items (Table 1).
2.6. Ethics and Protection Data
3. Data Plan Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. SPIRIT 2013 Checklist: Recommended Items to Address in a Clinical Trial Protocol and Related Documents
| Section/Item | Item Nº | Description | Addressed on Page Number |
| Administrative Information | |||
| Title | 1 | Descriptive title identifying the study design, population, interventions, and, if applicable, trial acronym | 1 |
| Trial registration | 2a | Trial identifier and registry name. If not yet registered, name of intended registry | 4 |
| 2b | All items from the World Health Organization Trial Registration Data Set | 1 | |
| Protocol version | 3 | Date and version identifier | 4 |
| Funding | 4 | Sources and types of financial, material, and other support | 11 |
| Roles and responsibilities | 5a | Names, affiliations, and roles of protocol contributors | 1,11 |
| 5b | Name and contact information for the trial sponsor | 11 | |
| 5c | Role of study sponsor and funders, if any, in study design; collection, management, analysis, and interpretation of data; writing of the report; and the decision to submit the report for publication, including whether they will have ultimate authority over any of these activities | 11 | |
| 5d | Composition, roles, and responsibilities of the coordinating center, steering committee, endpoint adjudication committee, data management team, and other individuals or groups overseeing the trial, if applicable | 4–5 | |
| Introduction | |||
| Background and rationale | 6a | Description of research question and justification for undertaking the trial, including summary of relevant studies (published and unpublished) examining benefits and harms for each intervention | 1–3 |
| 6b | Explanation for choice of comparators | NA | |
| Objectives | 7 | Specific objectives or hypotheses | 2 |
| Trial design | 8 | Description of trial design including type of trial (e.g., parallel group, crossover, factorial, single group), allocation ratio, and framework (e.g., superiority, equivalence, noninferiority, exploratory) | 4 |
| Methods: Participants, interventions, and outcomes | |||
| Study setting | 9 | Description of study settings (e.g., community clinic, academic hospital) and list of countries where data will be collected. Reference to where list of study sites can be obtained | 4–6 |
| Eligibility criteria | 10 | Inclusion and exclusion criteria for participants. If applicable, eligibility criteria for study centers and individuals who will perform the interventions (e.g., surgeons, psychotherapists) | 4 |
| Interventions | 11a | Interventions for each group with sufficient detail to allow replication, including how and when they will be administered | 4–7 |
| 11b | Criteria for discontinuing or modifying allocated interventions for a given trial participant (e.g., drug dose change in response to harms, participant request, or improving/worsening disease) | 8–9 | |
| 11c | Strategies to improve adherence to intervention protocols, and any procedures for monitoring adherence (e.g., drug tablet return, laboratory tests) | 5–6,9 | |
| 11d | Relevant concomitant care and interventions that are permitted or prohibited during the trial | 5–7 | |
| Outcomes | 12 | Primary, secondary, and other outcomes, including the specific measurement variable (e.g., systolic blood pressure), analysis metric (e.g., change from baseline, final value, time to event), method of aggregation (e.g., median, proportion), and time point for each outcome. Explanation of the clinical relevance of chosen efficacy and harm outcomes is strongly recommended | 7–8, Appendix D |
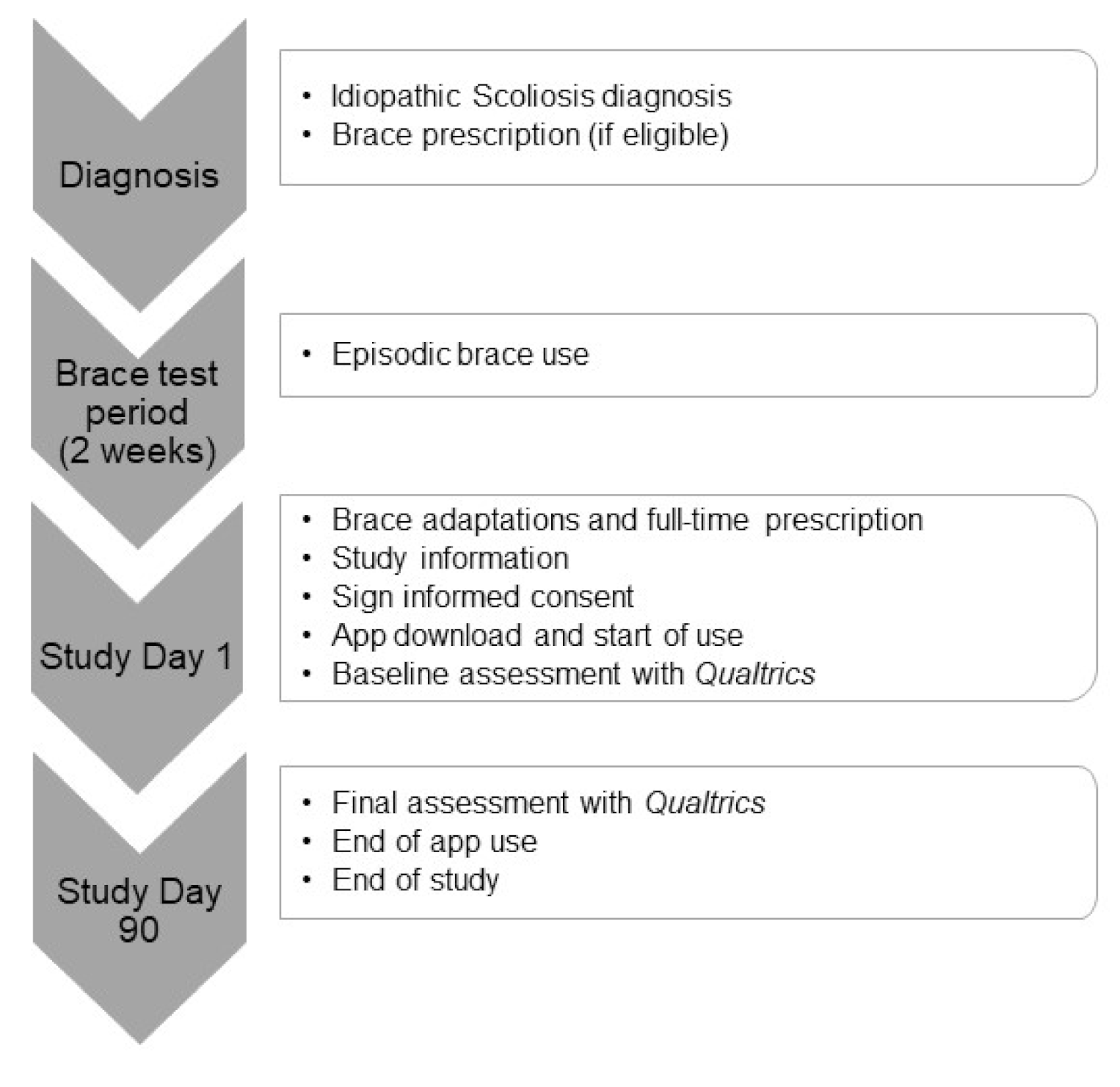
| Participant timeline | 13 | Time schedule of enrolment, interventions (including any run-ins and washouts), assessments, and visits for participants. A schematic diagram is highly recommended (see Figure 1) | 5 |
| Sample size | 14 | Estimated number of participants needed to achieve study objectives and how it was determined, including clinical and statistical assumptions supporting any sample size calculations | 4 |
| Recruitment | 15 | Strategies for achieving adequate participant enrolment to reach target sample size | 4 |
| Methods: Assignment of interventions (for controlled trials) | |||
| Allocation: | |||
| Sequence generation | 16a | Method of generating the allocation sequence (e.g., computer-generated random numbers), and list of any factors for stratification. To reduce predictability of a random sequence, details of any planned restriction (e.g., blocking) should be provided in a separate document that is unavailable to those who enroll participants or assign interventions | NA |
| Allocation concealment mechanism | 16b | Mechanism of implementing the allocation sequence (e.g., central telephone; sequentially numbered, opaque, sealed envelopes), describing any steps to conceal the sequence until interventions are assigned | NA |
| Implementation | 16c | Who will generate the allocation sequence, who will enroll participants, and who will assign participants to interventions | 4-5 |
| Blinding (masking) | 17a | Who will be blinded after assignment to interventions (e.g., trial participants, care providers, outcome assessors, data analysts), and how | NA |
| 17b | If blinded, circumstances under which unblinding is permissible, and procedure for revealing a participant’s allocated intervention during the trial | NA | |
| Methods: Data collection, management, and analysis | |||
| Data collection methods | 18a | Plans for assessment and collection of outcome, baseline, and other trial data, including any related processes to promote data quality (e.g., duplicate measurements, training of assessors) and a description of study instruments (e.g., questionnaires, laboratory tests) along with their reliability and validity, if known. Reference to where data collection forms can be found, if not in the protocol | 9 |
| 18b | Plans to promote participant retention and complete follow-up, including list of any outcome data to be collected for participants who discontinue or deviate from intervention protocols | 5-7 | |
| Data management | 19 | Plans for data entry, coding, security, and storage, including any related processes to promote data quality (e.g., double data entry; range checks for data values). Reference to where details of data management procedures can be found, if not in the protocol | 8-9 |
| Statistical methods | 20a | Statistical methods for analyzing primary and secondary outcomes. Reference to where other details of the statistical analysis plan can be found, if not in the protocol | 9 |
| 20b | Methods for any additional analyses (e.g., subgroup and adjusted analyses) | NA | |
| 20c | Definition of analysis population relating to protocol non-adherence (e.g., as randomized analysis), and any statistical methods to handle missing data (e.g., multiple imputation) | 9 | |
| Methods: Monitoring | |||
| Data monitoring | 21a | Composition of data monitoring committee (DMC); summary of its role and reporting structure; statement of whether it is independent from the sponsor and competing interests; and reference to where further details about its charter can be found, if not in the protocol. Alternatively, an explanation of why a DMC is not needed | 4 |
| 21b | Description of any interim analyses and stopping guidelines, including who will have access to these interim results and make the final decision to terminate the trial | 9 | |
| Harms | 22 | Plans for collecting, assessing, reporting, and managing solicited and spontaneously reported adverse events and other unintended effects of trial interventions or trial conduct | 6-9 |
| Auditing | 23 | Frequency and procedures for auditing trial conduct, if any, and whether the process will be independent from investigators and the sponsor | NA |
| Ethics and dissemination | |||
| Research ethics approval | 24 | Plans for seeking research ethics committee/institutional review board (REC/IRB) approval | 4, 11 |
| Protocol amendments | 25 | Plans for communicating important protocol modifications (e.g., changes to eligibility criteria, outcomes, analyses) to relevant parties (e.g., investigators, REC/IRBs, trial participants, trial registries, journals, regulators) | 8 |
| Consent or assent | 26a | Who will obtain informed consent or assent from potential trial participants or authorized surrogates, and how (see Item 32) | 4-5 |
| 26b | Additional consent provisions for collection and use of participant data and biological specimens in ancillary studies, if applicable | NA | |
| Confidentiality | 27 | How personal information about potential and enrolled participants will be collected, shared, and maintained in order to protect confidentiality before, during, and after the trial | 8-9 |
| Declaration of interests | 28 | Financial and other competing interests for principal investigators for the overall trial and each study site | 11 |
| Access to data | 29 | Statement of who will have access to the final trial dataset, and disclosure of contractual agreements that limit such access for investigators | 9 |
| Ancillary and post-trial care | 30 | Provisions, if any, for ancillary and post-trial care, and for compensation to those who suffer harm from trial participation | 8-9 |
| Dissemination policy | 31a | Plans for investigators and sponsor to communicate trial results to participants, healthcare professionals, the public, and other relevant groups (e.g., via publication, reporting in results databases, or other data sharing arrangements), including any publication restrictions | 9 |
| 31b | Authorship eligibility guidelines and any intended use of professional writers | NA | |
| 31c | Plans, if any, for granting public access to the full protocol, participant-level dataset, and statistical code | 9 | |
| Appendices | |||
| Informed consent materials | 32 | Model consent form and other related documentation given to participants and authorized surrogates | Appendix B |
| Biological specimens | 33 | Plans for collection, laboratory evaluation, and storage of biological specimens for genetic or molecular analysis in the current trial and for future use in ancillary studies, if applicable | NA |
Appendix B. Informed Consent
| Date and signature of the participant/relative/legal tutor | Date and signature of the researcher |
| Date and signature of the participant/relative/legal tutor |
Appendix C. Alphanumeric Code Linked with Identifying Information
| Number of Participant | Alphanumeric Code | Medical Registry Number |
| 1 | 1ESCVH0001 | 9999999 |
| 2 | 1ESCVH0002 | 9999998 |
| 3 | 1ESCVH0003 | 9999997 |
| 4 | 1ESCVH0004 | 9999996 |
| 5 | 1ESCVH0005 | 9999995 |
Appendix D. Assessment Protocol
- 1.
- Items in the Qualtrics Online Platform
- Sobberheim Stress Questionnaire (BSSQ brace) [33,34]. It contains eight items assessing psychological stress produced by brace in adolescents with IS (i.e., I find it hard to show my back in public”). Response use a 4-points Likert scale (0 = “most stress” to 3 = “least stress”). Total scores range from 0 to 24. Higher total scores indicate less stress. Cut-offs proposed in the original versions are: 0–8 (severe stress), 9–16 (moderate stress), and 17–24 (mild stress) [34].
- Italian Spine Youth Quality Of Life (ISYQOL) [35,36]. The scale is composed of 20 items. Some of them assess quality of life with respect to back problems and can be administered to all patients with spinal deformities (spine health domain = 13 items; “Despite your back problem, do you life a happy life?”). The remaining items are specifically designed for patients wearing a brace (brace domain = 7 items; “It is uncomfortable to wear your brace?”). Responses use a 3-point Likert scale (0 = “never”; 1 = “sometimes”; 2 = “often”). Items 5, 6, 10, and 13 are reverse coded. Total scores are converted into percentages [35]. Final scores range from 0% to 100%, where higher percentages indicate greater quality of life.
- Scoliosis Research Society-22 (SRS-22) [37,38]. This questionnaire is composed of 22 items that evaluate 5 scoliosis domains, namely function/activity (5 items; “What is your current level of activity?”), pain (5 items; “Which one of the following best describes the amount of pain you have experienced over the last month”), self-image/appearance (5 items; “How do you look in clothes?”), mental health (5 items; “Have you felt calm and peaceful during the last 6 months?”), and satisfaction with the treatment (2 items; “which one of the following best describes your pain medication use for back pain?”). Response scales range from 1 = “Severe/All of the time/Very unhappy/Bedridden/Very bad/Very often/Very poor/None of the time/Severely/Very unsatisfied/Definitely no” to 5 = “None/None of the time/Very happy/Full activities without restriction/Very good/Never/Very good/All the time/Very satisfied/Definitely yes”. Higher scores indicate better perceived health status.
- Hospital Anxiety and Depression Scale (HADS) [39,40]. The HADS consists of 14 items that assess anxiety (seven items; “I feel tense or wound up”) and depression (seven items; “I still enjoy the things I used to enjoy”). Each item is rated according to a 4-point Likert scale ranging from 0 = “as much as I always do” to 3 = “not at all”. Total scores range from 0 to 21 and higher scores represent higher anxiety and depressive symptoms. Cut-offs are stablished as follows: 0–7 (non-cases), 8–10 (doubtful case), and 11–21 (definite case) [39].
- System Usability Scale (administered only at the end of the study). The SUS evaluates whether a system is considered to be simple to use and useful (e.g., “I needed to learn many things before I could start using the system”). It is responded to according to a 5-point Likert scale (1 = “completely disagree” to 5 = “completely agree”). The score of half of the items has to be reverted so that higher scores indicate higher usability and acceptability. Then total score is multiplied by 2.5 so that final scores range from 0–100.
- 2.
- Items Assessed with the Pain Monitor Mobile Application
Appendix E. Response to Clinical Alarm
Coping Recommendations When Wearing a Brace
- Remember that the use of a brace is temporary.
- Be compassionate with yourself. Suffering is normal in this situation. Talk about it with the people you trust.
- Reward yourself. Do not isolate yourself from certain people or activities, as this will make things even harder for you. Reconnect with what you like by accepting the brace as a difficulty that you can live with. Try experiencing pleasant emotions with the activities you like.
- Do not avoid interacting with people or doing activities due to brace or the fear will become bigger and bigger. You can change and go back to enjoying the things you like (of course, wearing the corset makes it less pleasant, but still worth it).
- Some discomfort associated with wearing the brace is worth what you earn by participating in the things you like.
- Do not stop doing things that you like because they can judge you. Connect with what you like about your activities, with the joy. Accept that, although the brace makes things more difficult, the activities you like continue to be pleasant.
- Go ahead and participate in activities that you like, activities that can generate well-being even if your head tells you that they will judge you or that you will have a hard time. In the end, you may experience an uncomfortable moment (someone who asks about the brace or judges you), but it will only be episodic. Going through that short difficult moment will allow you to enjoy the rest of the activity.
- It is possible that, when you plan to do activities, your head shares difficult thoughts with you. These may include things like “they will see my corset”, “they will think I am different”, “they will judge me…”. In those moments, it can be useful to remember the reasons why you liked this activity before wearing the brace and remember the good times you have spent doing it.
- Allow yourself not to talk about it when you do not feel like it. Others have the right to ask, just as you have the right to not answering.
- Wearing a brace is not pleasant, but it is something that will help your health. It is normal that you do not like it and that you prefer not to wear it. However, accepting that now is the time to make this effort for your future well-being and understanding (and welcoming) that this entails difficulties and discomfort will allow you to better cope with it.
- Allows the corset to be there. Even allow it to be noticed externally. Instead of fighting against it so that it is not noticed, allowing it to be there and telling yourself that “nothing devastating happens if it is noticed” will help you to cope better. Of course, it would be more comfortable not to wear a brace, but you can wear it and at the same time do the things you like if you give up the fight against it.
- Enjoy who you are now. Do not wait to be that almost unreachable hypothetical perfect person to get involved in your life and do the things that give you a sense of fulfillment.
- Think that, even when somebody criticizes or judges you, that is temporary. You do not have to be liked by everyone at all times and you can do things that you like even when someone judges you. That judgment is a discomfort that you can carry along with you in the process of living a meaningful life that is worth living.
- Remember that the important thing is not to do things perfectly or without criticism. The important thing is to do things with interest and involvement, understanding and welcoming that things will not always be easy and that you will not always do things perfectly.
- Think about what YOU want to get out of life, not just what OTHER PEOPLE expect.
- Talk to yourself in a compassionate and kind manner. All of us go through bad times and make mistakes. What is important is to realize this and to be willing to make changes.
- Take care of yourself and give yourself messages of appreciation when you make efforts.
References
- Negrini, S.; Donzelli, S.; Aulisa, A.G.; Czaprowski, D.; Schreiber, S.; de Mauroy, J.C.; Diers, H.; Grivas, T.B.; Knott, P.; Kotwicki, T.; et al. 2016 SOSORT guidelines: Orthopaedic and rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis Spinal Disord. 2018, 13, 3. [Google Scholar] [CrossRef] [Green Version]
- Théroux, J.; Le May, S.; Fortin, C.; Labelle, H. Prevalence and management of back pain in adolescent idiopathic scoliosis patients: A retrospective study. Pain Res. Manag. 2015, 20, 153–157. [Google Scholar] [CrossRef] [Green Version]
- Yuan, W.; Shen, J.; Chen, L.; Wang, H.; Yu, K.; Cong, H.; Zhou, J.; Lin, Y. Differences in nonspecific low back pain between young adult females with and without lumbar scoliosis. Pain Res. Manag. 2019, 2019, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Tones, M.; Moss, N.; Polly, D.W. A Review of Quality of Life and Psychosocial Issues in Scoliosis. Spine 2006, 31, 3027–3038. [Google Scholar] [CrossRef]
- Reichel, D.; Schanz, J. Developmental psychological aspects of scoliosis treatment. Dev. Neurorehabil. 2003, 6, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Kuroki, H. Brace treatment for adolescent idiopathic scoliosis. J. Clin. Med. 2018, 7, 136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esparza Olcina, M.; García Aguado, J.; Martínez Rubio, A.; Mengual Gil, J.; Merio Moína, M.; Pallás Alonso, C.; Sánchez, F.; Colomer Revuelta, J.; Cortés Rico, O.; Galbe, J.; et al. Cribado de la escoliosis idiopatica Adolecente. Rev. Pediatr. Aten. Primaria 2015, 17, e159–e179. [Google Scholar] [CrossRef]
- Negrini, S.; Grivas, T.B.; Kotwicki, T.; Maruyama, T.; Rigo, M.; Weiss, H. Why do we treat adolescent idiopathic scoliosis? What we want to obtain and to avoid for our patients. SOSORT 2005 Consensus paper. Scoliosis 2006, 1. [Google Scholar] [CrossRef] [Green Version]
- Yang, S.; Andras, L.M.; Redding, G.J.; Skaggs, D.L. Early-Onset Scoliosis: A Review of History, Current Treatment, and Future Directions. Pediatrics 2015, 137, e20150709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hennrikus, W. Effects of Bracing in Adolescents with Idiopathic Scoliosis. AAP Gd. Rounds 2014, 31, 14. [Google Scholar] [CrossRef]
- Morton, A.; Riddle, R.; Buchanan, R.; Katz, D.; Birch, J. Accuracy in the prediction and estimation of adherence to bracewear before and during treatment of adolescent idiopathic scoliosis. J. Pediatr. Orthop. 2008, 28, 336–341. [Google Scholar] [CrossRef]
- Negrini, S.; Atanasio, S.; Zaina, F.; Romano, M. Rehabilitation of adolescent idiopathic scoliosis: Results of exercises and bracing from a series of clinical studies. Eur. J. Phys. Rehabil. Med. 2008, 44, 169–176. [Google Scholar] [PubMed]
- Miller, D.J.; Franzone, J.M.; Matsumoto, H.; Gomez, J.A.; Avendaño, J.; Hyman, J.E.; Roye, D.P.; Vitale, M.G. Electronic Monitoring Improves Brace-Wearing Compliance in Patients With Adolescent Idiopathic Scoliosis. Spine 2012, 37, 717–721. [Google Scholar] [CrossRef]
- Negrini, S.; Grivas, T.B.; Kotwicki, T.; Rigo, M.; Zaina, F. Guidelines on “Standards of management of idiopathic scoliosis with corrective braces in everyday clinics and in clinical research”: SOSORT Consensus 2008. Scoliosis 2009, 4, 2. [Google Scholar] [CrossRef] [Green Version]
- Wiley, J.W.; Thomson, J.D.; Mitchell, T.M.; Smith, B.G.; Banta, J.V. Effectiveness of The Boston Brace in Treatment of Large Curves in Adolescent Idiopathic Scoliosis. Spine 2000, 25, 2326–2332. [Google Scholar] [CrossRef]
- Suso-Ribera, C.; Mesas, Á.; Medel, J.; Server, A.; Márquez, E.; Castilla, D.; Zaragozá, I.; García-Palacios, A.; Mesas, A.; Medel, J.; et al. Improving pain treatment with a smartphone app: Study protocol for a randomized controlled trial. Trials 2018, 19, 145. [Google Scholar] [CrossRef] [Green Version]
- García-Palacios, A.; Herrero, R.; Belmonte, M.A.; Castilla, D.; Guixeres, J.; Molinari, G.; Banos, R.M.; Baños, R.M.; Botella, C.; Garcia-Palacios, A.; et al. Ecological momentary assessment for chronic pain in fibromyalgia using a smartphone: A randomized crossover study. Eur. J. Pain 2014, 18, 862–872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahman, T.; Sample, W.; Yorgova, P.; Neiss, G.; Rogers, K.; Shah, S.; Gabos, P.; Kritzer, D.; Bowen, J.R. Electronic monitoring of orthopedic brace compliance. J. Child. Orthop. 2015, 9, 365–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Global data Wearable technology in healthcare. Nat. Biotechnol. 2019, 37, 376. [CrossRef]
- Donzelli, S.; Zaina, F.; Negrini, S. In defense of adolescents: They really do use braces for the hours prescribed, if good help is provided. Results from a prospective everyday clinic cohort using thermobrace. Scoliosis 2012, 7, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Statcounter Global Stats Desktop vs. Mobile vs. Tablet Market Share Worldwide. Available online: https://gs.statcounter.com/platform-market-share/desktop-mobile-tablet/worldwide (accessed on 11 May 2021).
- Grist, R.; Cliffe, B.; Denne, M.; Croker, A.; Stallard, P. An online survey of young adolescent girls’ use of the internet and smartphone apps for mental health support. BJPsych Open 2018, 4, 302–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, S.-H.; Wang, Q.; Wang, L.-Q.; Wang, L.; Song, K.-P.; He, C.-Q. Effect of Internet-Based Rehabilitation Programs on Improvement of Pain and Physical Function in Patients with Knee Osteoarthritis: Systematic Review and Meta-analysis of Randomized Controlled Trials. J. Med. Internet Res. 2021, 23, e21542. [Google Scholar] [CrossRef]
- Karyotaki, E.; Efthimiou, O.; Miguel, C.; Bermpohl, F.M.g.; Furukawa, T.A.; Cuijpers, P.; Riper, H.; Patel, V.; Mira, A.; Gemmil, A.W.; et al. Internet-Based Cognitive Behavioral Therapy for Depression. JAMA Psychiatry 2021, 78, 361. [Google Scholar] [CrossRef]
- Hayes, W.; Naziri, Q.; De Tolla, J.E.; Akamnonu, C.P.; Merola, A.A.; Paulino, C. A Systematic Review of All Smart Phone Applications Specifically Aimed for Use as a Scoliosis Screening Tool. Spine J. 2013, 13, S38. [Google Scholar] [CrossRef]
- Zhu, C.; Wu, Q.; Xiao, B.; Wang, J.; Luo, C.; Yu, Q.; Liu, L.; Song, Y. A compliance real-time monitoring system for the management of the brace usage in adolescent idiopathic scoliosis patients: A pilot study. BMC Musculoskelet. Disord. 2021, 22, 152. [Google Scholar] [CrossRef]
- Browne, R.H. On the use of a pilot sample for sample size determination. Stat. Med. 1995, 14, 1933–1940. [Google Scholar] [CrossRef]
- Guidance for Industry and Food and Drug Administration Staff. Applying Human Factors and Usability Engineering to Medical Devices. Available online: https://www.fda.gov/media/80481/download (accessed on 11 May 2021).
- Suso-Ribera, C.; Castilla, D.; Zaragozá, I.; Ribera-Canudas, M.V.; Botella, C.; García-Palacios, A. Validity, Reliability, Feasibility, and Usefulness of Pain Monitor, a Multidimensional Smartphone App for Daily Monitoring of Adults with Heterogeneous Chronic Pain. Clin. J. Pain 2018, 34, 900–908. [Google Scholar] [CrossRef]
- Shiffman, S.; Stone, A.A.; Hufford, M.R. Ecological Momentary Assessment. Annu. Rev. Clin. Psychol. 2008, 4, 1–32. [Google Scholar] [CrossRef] [PubMed]
- Brooke, J. SUS: A “quick and dirty” usability scale. In Usability Evaluation in Industry; Jordan, P.W., Thomas, B., Weerdmeester, A.B., McClelland, I.L., Eds.; Taylor & Francis: London, UK, 1996; pp. 189–194. [Google Scholar]
- Davis, F.D.; Bagozzi, R.P.; Warshaw, P.R. User Acceptance of Computer Technology: A Comparison of Two Theoretical Models. Manag. Sci. 1989, 35, 982–1003. [Google Scholar] [CrossRef] [Green Version]
- Agata, E.D.; Testor, C.P.; Rigo, M. Spanish validation of Bad Sobernheim Stress Questionnaire (BSSQ (brace).es) for adolescents with braces. Scoliosis 2010, 5, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Botens-Helmus, C.; Klein, R.; Stephan, C. The reliability of the Bad Sobernheim Stress Questionnaire (BSSQbrace) in adolescents with scoliosis during brace treatment. Scoliosis 2006, 1, 22. [Google Scholar] [CrossRef] [Green Version]
- Caronni, A.; Sciumè, L.; Donzelli, S.; Zaina, F.; Negrini, S. ISYQOL: A Rasch-consistent questionnaire for measuring health-related quality of life in adolescents with spinal deformities. Spine J. 2017, 17, 1364–1372. [Google Scholar] [CrossRef]
- Sánchez-raya, J.; Agata, E.D.; Donzelli, S.; Caronni, A.; Bagó, J.; Rigo, M.; Figueras, C.; Negrini, S. Spanish validation of Italian Spine Youth Quality of Life (ISYQOL) Questionnaire. J. Phys. Med. Rehabil. 2020, 2, 8. [Google Scholar]
- Bago, J.; Climent, J.M.; Ey, A.; Perez-Grueso, F.J.S.; Izquierdo, E. The Spanish version of the SRS-22 Patient Questionnaire for idiopathic scoliosis: Transcultural adaptation and reliability analysis. Spine 2004, 29, 1676–1680. [Google Scholar] [CrossRef] [PubMed]
- Asher, M.; Min Lai, S.; Burton, D.; Manna, B. The Reliability and Concurrent Validity of the Scoliosis Research Society-22 Patient Questionnaire for Idiopathic Scoliosis. Spine 2003, 28, 63–69. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Herrero, M.J.; Blanch, J.; Peri, J.M.; De Pablo, J.; Pintor, L.; Bulbena, A. A validation study of the hospital anxiety and depression scale (HADS) in a Spanish population. Gen. Hosp. Psychiatry 2003, 25, 277–283. [Google Scholar] [CrossRef]
- World Medical Association (WMA). Declaration of Helsinki–Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Ono, M.; Schneider, S.; Junghaenel, D.U.; Stone, A.A. What Affects the Completion of Ecological Momentary Assessments in Chronic Pain Research? An Individual Patient Data Meta-Analysis. J. Med. Internet Res. 2019, 21, e11398. [Google Scholar] [CrossRef] [PubMed]
- Schwieger, T.; Campo, S.; Weinstein, S.L.; Dolan, L.A.; Ashida, S.; Steuber, K.R. Body Image and Quality of Life and Brace Wear Adherence in Females with Adolescent Idiopathic Scoliosis. J. Pediatr. Orthop. 2017, 37, 519–523. [Google Scholar] [CrossRef] [PubMed]
- Dunn, J.; Henrikson, N.B.; Morrison, C.C.; Blasi, P.R.; Nguyen, M.; Lin, J.S. Screening for adolescent idiopathic scoliosis evidence report and systematic review for the US preventive services task force. JAMA J. Am. Med. Assoc. 2018, 319, 173–187. [Google Scholar] [CrossRef] [PubMed]
- Suso-Ribera, C.; Castilla, D.; Zaragozá, I.; Mesas, Á.; Server, A.; Medel, J.; García-Palacios, A. Telemonitoring in chronic pain management using smartphone apps: A randomized controlled trial comparing usual assessment against app-based monitoring with and without clinical alarms. Int. J. Environ. Res. Public Health 2020, 17, 6568. [Google Scholar] [CrossRef] [PubMed]
- Villegas, F.; Martínez-Borba, V.; Suso-Ribera, C.; Castilla, D.; Zaragoza, I.; García-Palacios, A.; Ferrer, C. Characterizing breakthrough cancer pain using ecological momentary assessment with a smartphone app: Feasibility and clinical findings. Int. J. Environ. Res. Public Health 2021, 18, 5991. [Google Scholar] [CrossRef]
- Statista Internet, Mobile Internet & Apps. Available online: https://0-www-statista-com.brum.beds.ac.uk/statistics/477088/children-and-teens-smartphone-usage-by-age-germany/ (accessed on 11 May 2021).
- Statista Technology & Telecommunications. Available online: https://0-www-statista-com.brum.beds.ac.uk/statistics/408427/smartphone-penetration-in-france-by-age-group/ (accessed on 11 May 2021).
- Mulkey, M.A.; Hardin, S.R.; Schoemann, A.M. Conducting a Device Feasibility Study. Clin. Nurs. Res. 2019, 28, 255–262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colombo, D.; Suso-Ribera, C.; Fernandez-Álvarez, J.; Felipe, I.F.; Cipresso, P.; Palacios, A.G.; Riva, G.; Botella, C. Exploring Affect Recall Bias and the Impact of Mild Depressive Symptoms: An Ecological Momentary Study. In Pervasive Computing Paradigms for Mental Health; Cipresso, P., Serino, S., Villani, D., Eds.; Springer: Cham, Switzerland, 2019; pp. 208–215. [Google Scholar]
- Thatipelli, S.; Arun, A.; Chung, P.; Etemadi, M.; Heller, J.A.; Kwiat, D.; Imamura-Ching, J.; Harrison, M.R.; Roy, S. Review of Existing Brace Adherence Monitoring Methods to Assess Adherence. JPO J. Prosthet. Orthot. 2016, 28, 126–135. [Google Scholar] [CrossRef]
- Vasiliadis, E.; Grivas, T.B.; Gkoltsiou, K. Development and preliminary validation of Brace Questionnaire (BrQ): A new instrument for measuring quality of life of brace treated scoliotics. Scoliosis 2006, 1, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Domain | Clinical Alarms | Recommendations 1 |
|---|---|---|
| Side effects | ||
| Pressure pain | 3 consecutive days | Call the patient |
| Friction pain | 3 consecutive days | Call the patient |
| Excessive heat/sweating | 7 consecutive days | Call the patient |
| Movement difficulties | 3 consecutive days | Call the patient |
| Teased by peers/relatives | 4 consecutive days | Psychoeducation |
| Pain | ||
| Pain intensity | ≥3 during 3 consecutive days | Call the patient |
| Emotions | ||
| Sadness | 5 consecutive days | Psychoeducation |
| Anxiety | 5 consecutive days | Psychoeducation |
| Anger | 5 consecutive days | Psychoeducation |
| Shame | 5 consecutive days | Psychoeducation |
| Overwhelm | 5 consecutive days | Psychoeducation |
| Frustration | 5 consecutive days | Psychoeducation |
| Interference | ||
| Sleeping | 3 consecutive days | Call the patient |
| Basic movements | 3 consecutive days | Call the patient |
| Relationships (friends) | 5 consecutive days | Psychoeducation |
| Relationships (relatives) | 5 consecutive days | Psychoeducation |
| Leisure activities | 5 consecutive days | Psychoeducation |
| Academic activities | 5 consecutive days | Psychoeducation |
| Mood | 5 consecutive days | Psychoeducation |
| Dressing | 5 consecutive days | Psychoeducation |
| Self-image | 5 consecutive days | Psychoeducation |
| Motivation for going out | 3 consecutive days | Psychoeducation |
| Avoid talking about the brace | ≥7 during 7 consecutive days | Psychoeducation |
| Avoid activities/being with others | ≥5 during 5 consecutive days | Psychoeducation |
| Overall physical discomfort | ≥5 during 5 consecutive days | Call the patient |
| Brace adherence | ||
| Morning only (8–14 h) | 7 consecutive days | Call the patient |
| Afternoon only (14–19 h) | 7 consecutive days | Call the patient |
| Sleeping only (last night) | 7 consecutive days | Call the patient |
| Morning and afternoon only | 7 consecutive days | Call the patient |
| Sleeping and morning | 15 consecutive days | Call the patient |
| Sleeping and afternoon | 15 consecutive days | Call the patient |
| No use of the brace | 3 consecutive days | Call the patient |
| Poor social support | ||
| Friends | 5 consecutive days | Psychoeducation |
| Family | 5 consecutive days | Psychoeducation |
| Teachers | 5 consecutive days | Psychoeducation |
| Other people | 5 consecutive days | Psychoeducation |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Borba, V.; Suso-Ribera, C.; Díaz-García, A.; Salat-Batlle, J.; Castilla, D.; Zaragoza, I.; García-Palacios, A.; Sánchez-Raya, J. mHealth for the Monitoring of Brace Compliance and Wellbeing in Adolescents with Idiopathic Scoliosis: Study Protocol for a Feasibility Study. Int. J. Environ. Res. Public Health 2021, 18, 7767. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18157767
Martínez-Borba V, Suso-Ribera C, Díaz-García A, Salat-Batlle J, Castilla D, Zaragoza I, García-Palacios A, Sánchez-Raya J. mHealth for the Monitoring of Brace Compliance and Wellbeing in Adolescents with Idiopathic Scoliosis: Study Protocol for a Feasibility Study. International Journal of Environmental Research and Public Health. 2021; 18(15):7767. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18157767
Chicago/Turabian StyleMartínez-Borba, Verónica, Carlos Suso-Ribera, Amanda Díaz-García, Judith Salat-Batlle, Diana Castilla, Irene Zaragoza, Azucena García-Palacios, and Judit Sánchez-Raya. 2021. "mHealth for the Monitoring of Brace Compliance and Wellbeing in Adolescents with Idiopathic Scoliosis: Study Protocol for a Feasibility Study" International Journal of Environmental Research and Public Health 18, no. 15: 7767. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18157767