
Oxidative Stress in Non-Dialysis-Dependent Chronic Kidney Disease Patients

 ,
,  , , and
, , and
Abstract
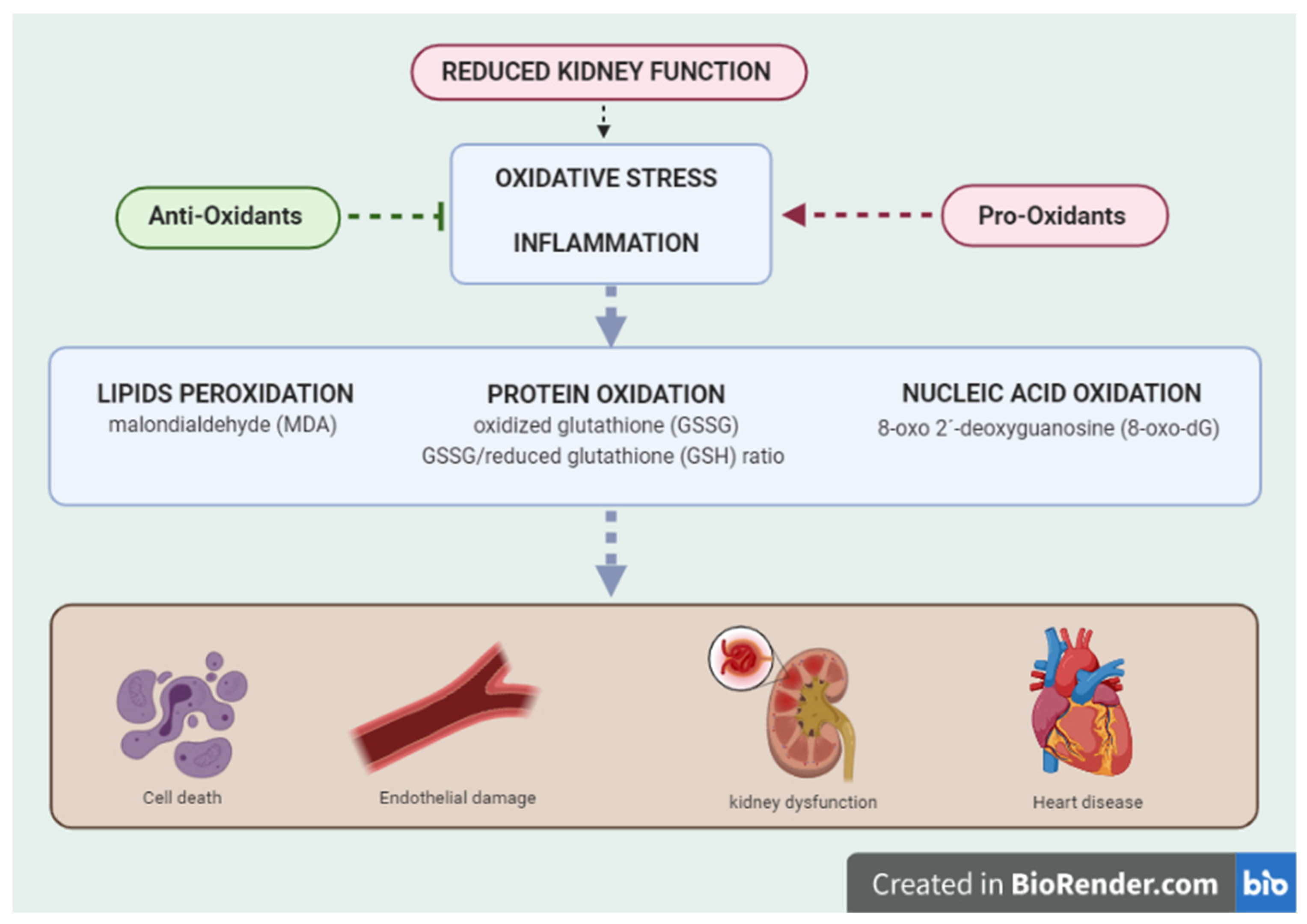
:1. Introduction
2. Methods
2.1. Study Inclusion Criteria
2.2. Exclusion Criteria
2.3. Population
2.4. Oxidative Stress Study
- 260 nm: wavelength of peak nucleic acid absorption.
- 280 nm: wavelength of maximum protein absorption.
2.5. Statistical Analysis
3. Results
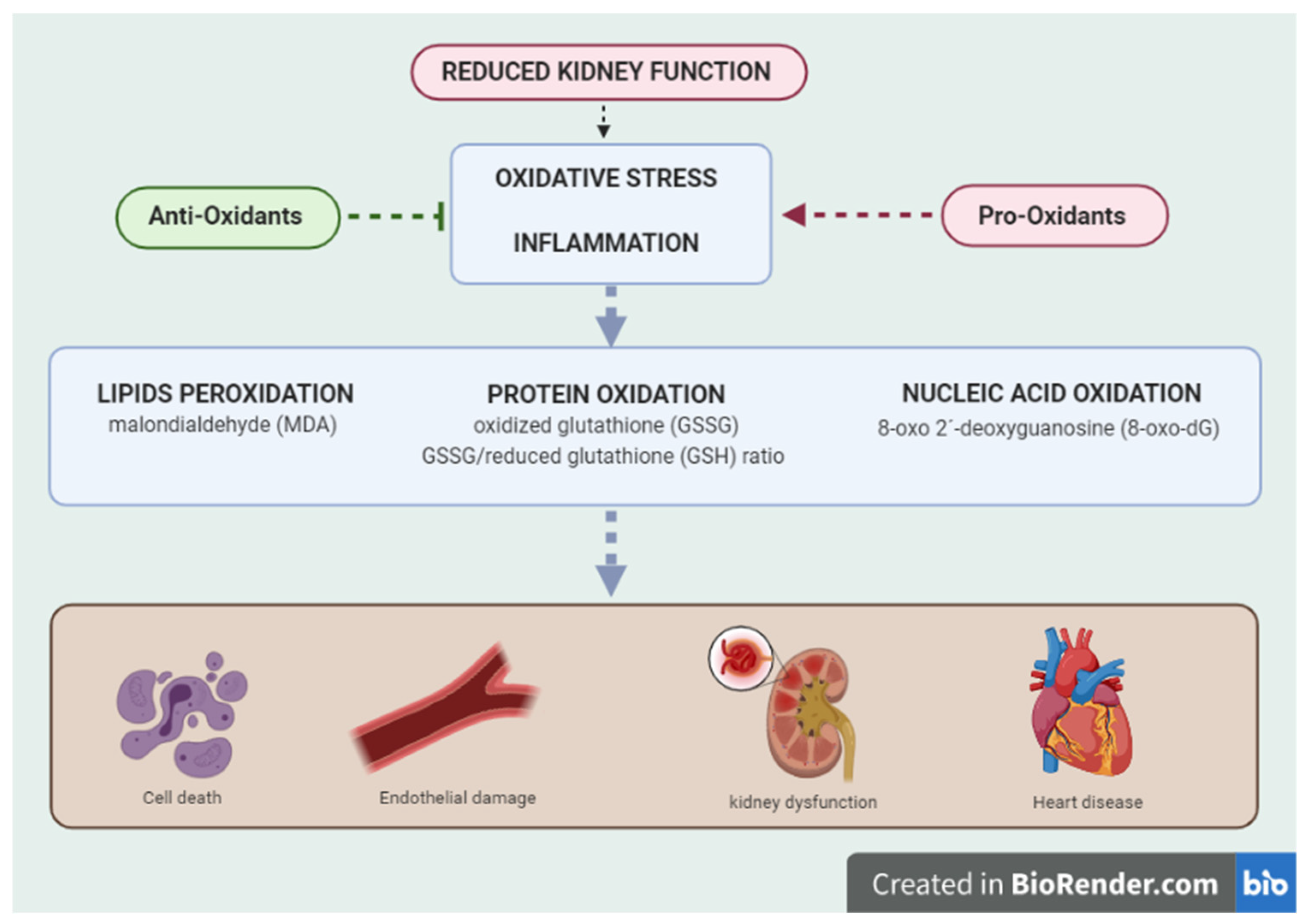
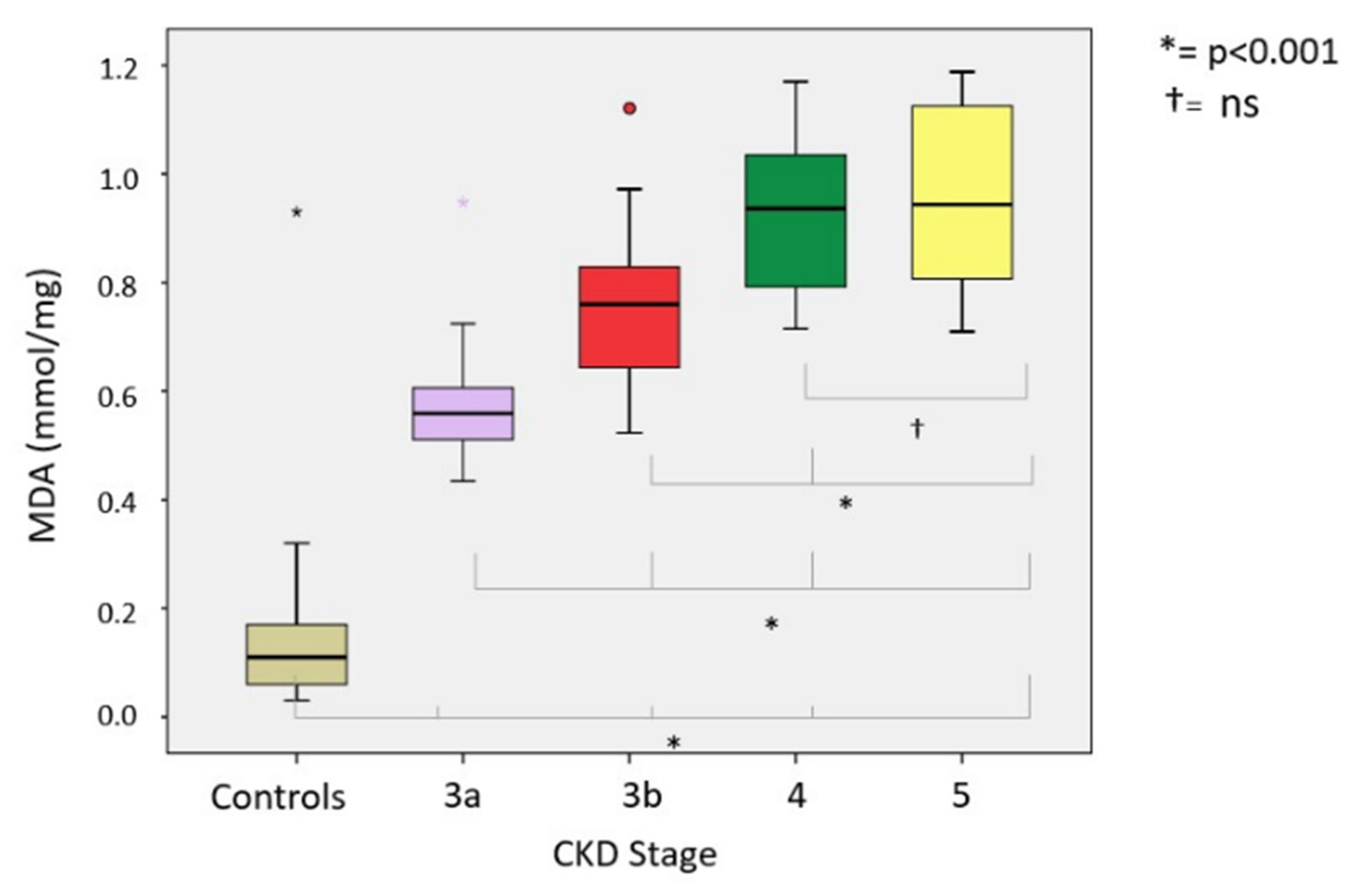
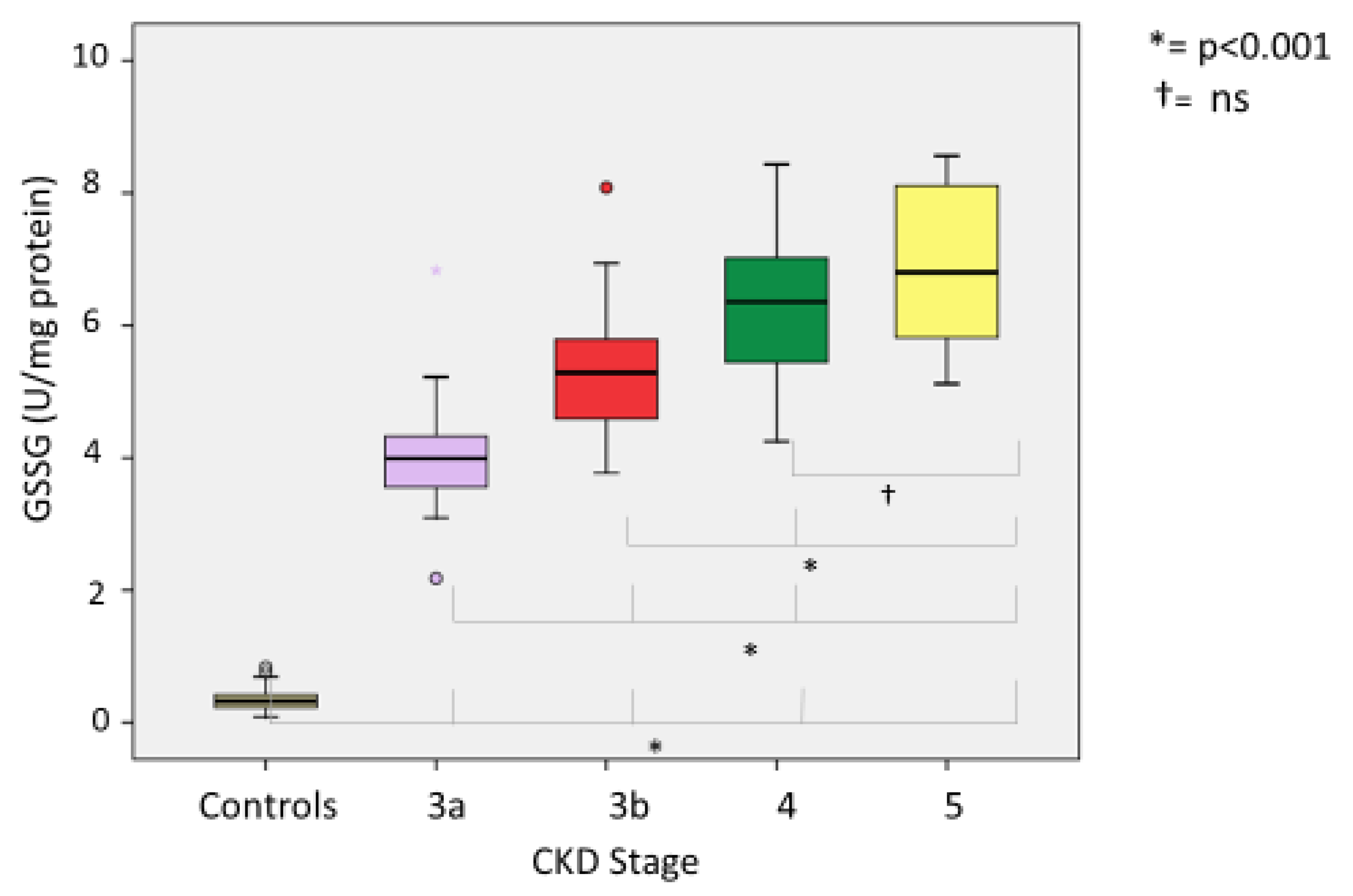
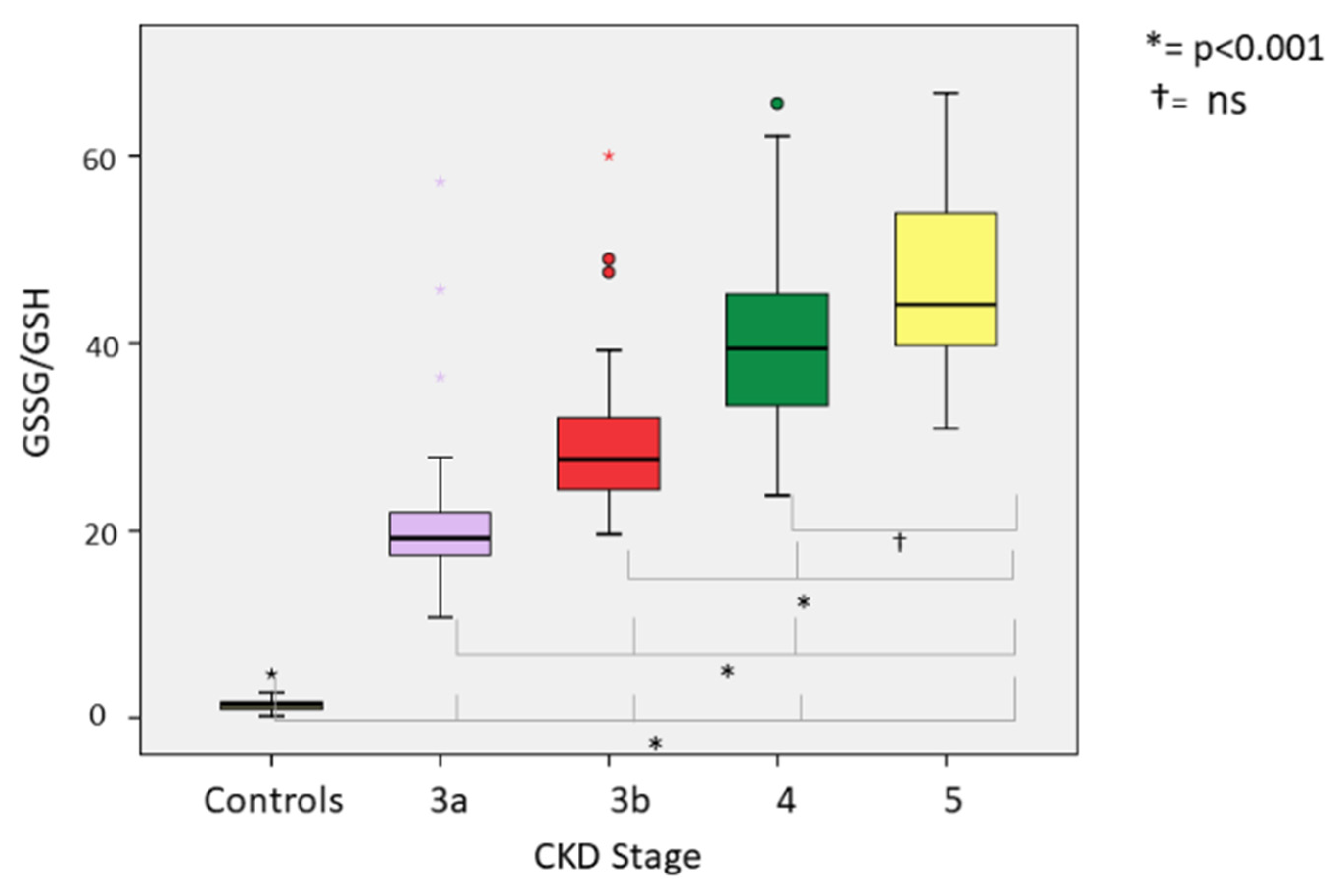
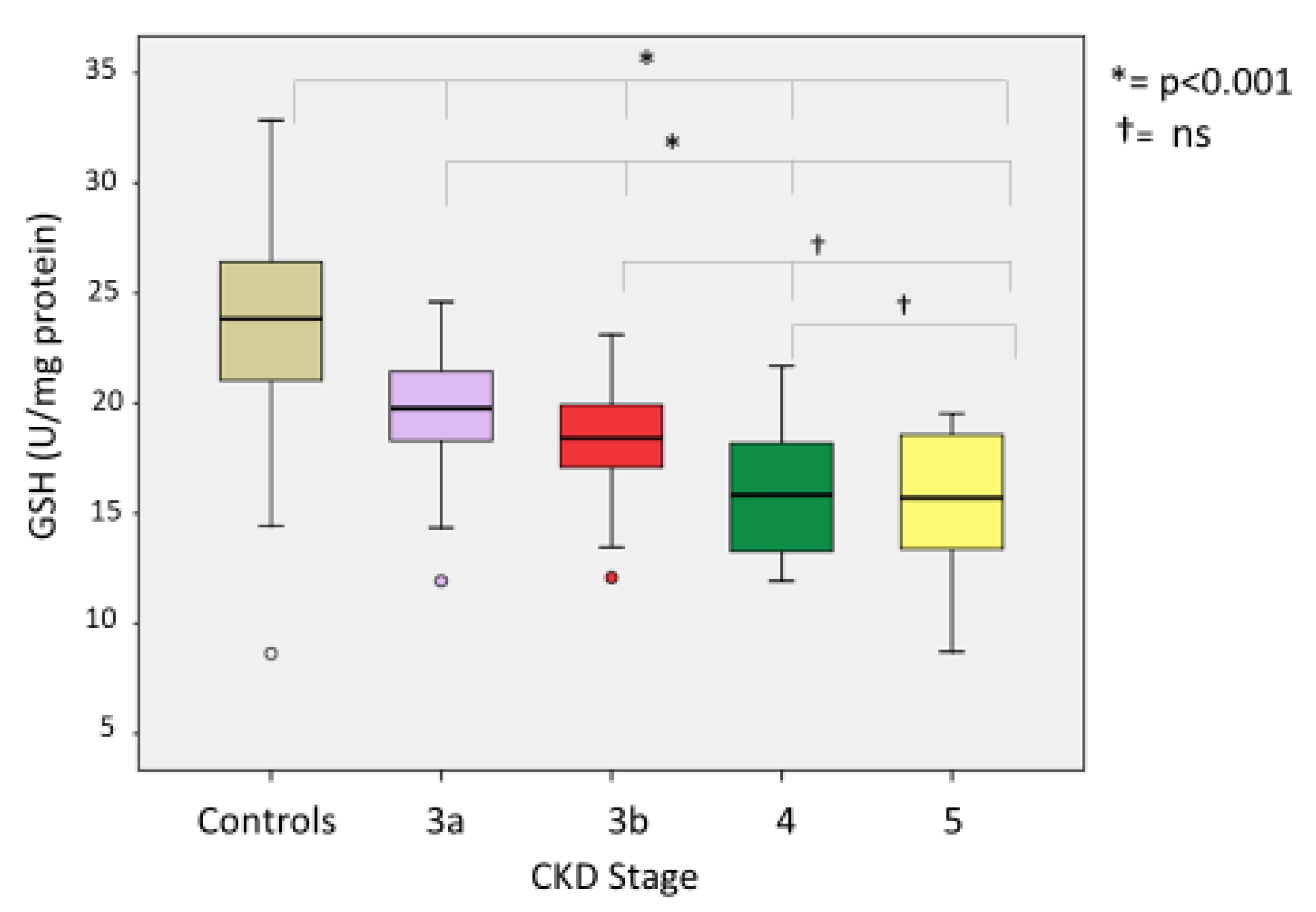
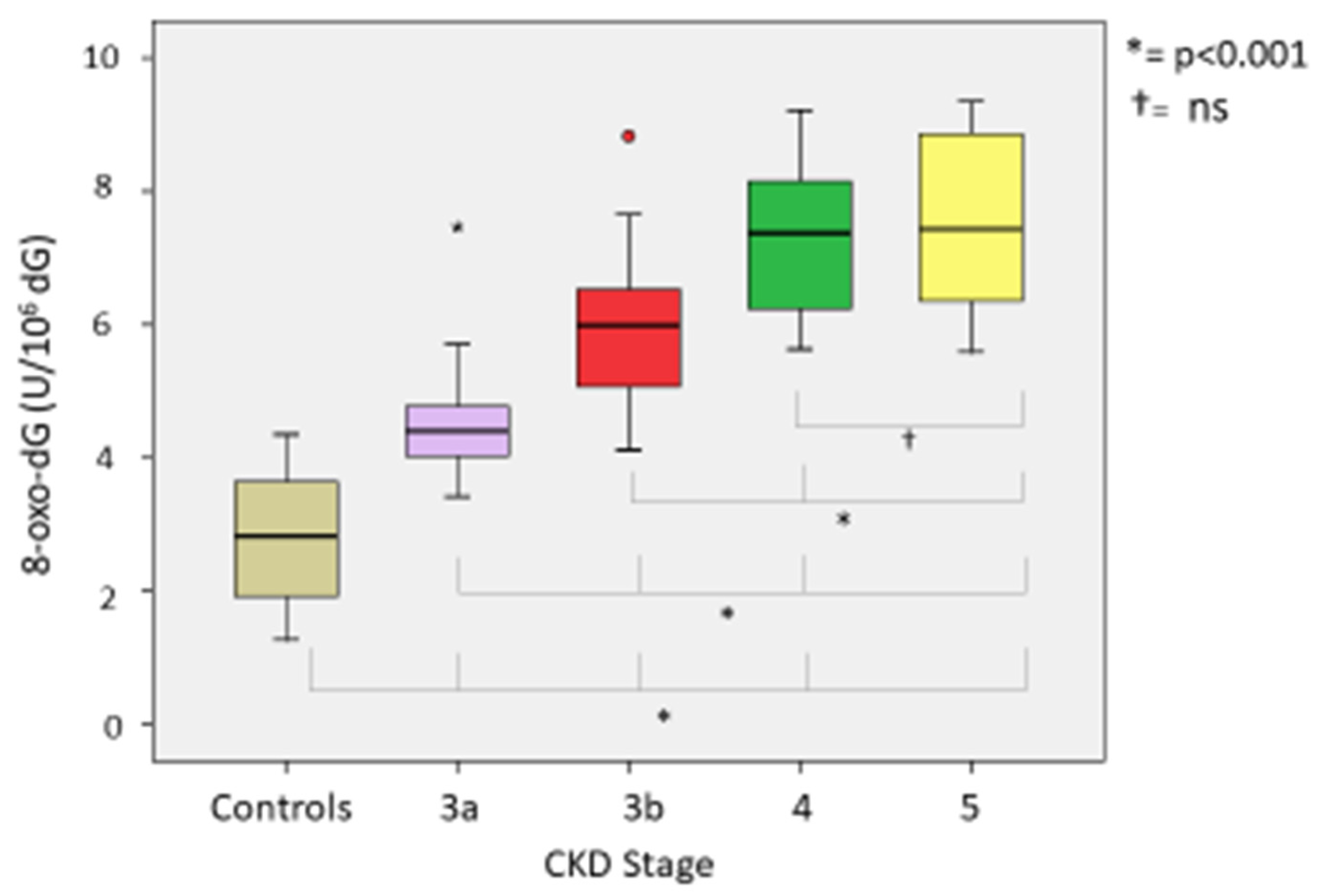
3.1. Oxidative Stress
3.2. Correlation of Oxidant and Antioxidant Parameters
3.3. Correlation between Glomerular Filtration and Oxidative and Antioxidant Parameters
3.4. Correlation between Oxidative Stress and Diabetes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Eknoyan, G. Cardiovascular Mortality and Morbidity in Dialysis Patients. Miner. Electrolyte Metab. 1999, 25, 100–104. [Google Scholar] [CrossRef]
- Arici, M.; Walls, J. End-stage renal disease, atherosclerosis, and cardiovascular mortality: Is C-reactive protein the missing link? Kidney Int. 2001, 59, 407–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- London, G.M.; Guérin, A.P.; Marchais, S.J.; Métivier, F.; Pannier, B.; Adda, H. Arterial media calcification in end-stage renal disease: Impact on all-cause and cardiovascular mortality. Nephrol. Dial. Transplant. 2003, 18, 1731–1740. [Google Scholar] [CrossRef]
- Stenvinkel, P.; Lindholm, B. Serum Albumin, C-Reactive Protein, Interleukin 6, and Fetuin A as Predictors of Malnutrition, Cardiovascular Disease, and Mortality in Patients With ESRD. Am. J. Kidney Dis. 2006, 47, 139–148. [Google Scholar]
- Böger, R.H.; Maas, R.; Schulze, F.; Schwedhelm, E. Asymmetric dimethylarginine (ADMA) as a prospective marker of cardiovascular disease and mortality—An update on patient populations with a wide range of cardiovascular risk. Pharmacol. Res. 2009, 60, 481–487. [Google Scholar] [CrossRef]
- Ponticelli, C.; Villa, M. Role of anaemia in cardiovascular mortality and morbidity in transplant patients. Nephrol. Dial. Transplant. 2002, 17, 41–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gyurászová, M.; Gurecká, R.; Bábíčková, J.; Tóthová, Ľ. Oxidative Stress in the Pathophysiology of Kidney Disease: Implications for Noninvasive Monitoring and Identification of Biomarkers. Oxid. Med. Cell Longev. 2020, 2020, 5478708. [Google Scholar] [CrossRef] [Green Version]
- Duni, A.; Liakopoulos, V.; Roumeliotis, S.; Peschos, D.; Dounousi, E. Oxidative Stress in the Pathogenesis and Evolution of Chronic Kidney Disease: Untangling Ariadne’s Thread. Int. J. Mol. Sci. 2019, 20, 3711. [Google Scholar] [CrossRef] [Green Version]
- Kanbay, M.; Yerlikaya, A.; Sag, A.A.; Ortiz, A.; Kuwabara, M.; Covic, A.; Wiecek, A.; Stenvinkel, P.; Afsar, B. A journey from microenvironment to macroenvironment: The role of metaflammation and epigenetic changes in cardiorenal disease. Clin. Kidney J. 2019, 12, 861–870. [Google Scholar] [CrossRef]
- Small, D.M.; Coombes, J.; Bennett, N.; Johnson, D.; Gobe, G.C. Oxidative stress, anti-oxidant therapies and chronic kidney disease. Nephrology 2012, 17, 311–321. [Google Scholar] [CrossRef]
- Duni, A.; Liakopoulos, V.; Rapsomanikis, K.-P.; Dounousi, E. Chronic Kidney Disease and Disproportionally Increased Cardiovascular Damage: Does Oxidative Stress Explain the Burden? Oxidative Med. Cell. Longev. 2017, 2017, 1–15. [Google Scholar] [CrossRef]
- D’Marco, L.; Bellasi, A.; Raggi, P. Cardiovascular Biomarkers in Chronic Kidney Disease: State of Current Research and Clinical Applicability. Dis. Markers 2015, 2015, 586569. [Google Scholar] [CrossRef] [Green Version]
- Zargari, M.; Sedighi, O. Influence of Hemodialysis on Lipid Peroxidation, Enzymatic and Non-Enzymatic Antioxidant Capacity in Chronic Renal Failure Patients. Nephro-Urol. Mon. 2015, 7, e28526. [Google Scholar] [CrossRef] [Green Version]
- Silva, R.E.; Simões-E-Silva, A.C.; Miranda, A.S.; Justino, P.B.I.; Brigagão, M.R.P.L.; Moraes, G.O.I.; Gonçalves, R.V.; Novaes, R.D. Potential Role of Nutrient Intake and Malnutrition as Predictors of Uremic Oxidative Toxicity in Patients with End-Stage Renal Disease. Oxidative Med. Cell. Longev. 2019, 2019, 463412. [Google Scholar] [CrossRef]
- González Rico, M.; Puchades, M.J.; García Ramón, R.; Saez, G.; Tormos, M.C.; Miguel, A. Efecto del tratamiento con hemodiálisis sobre el estrés oxidativo en pacientes con insuficiencia renal crónica [Effect of oxidative stress in patients with chronic renal failure]. Nefrologia 2006, 26, 218–225. [Google Scholar]
- Tbahriti, H.F.; Kaddous, A.; Bouchenak, M.; Mekki, K. Effect of Different Stages of Chronic Kidney Disease and Renal Replacement Therapies on Oxidant-Antioxidant Balance in Uremic Patients. Biochem. Res. Int. 2013, 2013, 358985. [Google Scholar] [CrossRef] [PubMed]
- Tarng, D.-C.; Huang, T.-P.; Wei, Y.-H.; Liu, T.-Y.; Chen, H.-W.; Chen, T.W.; Yang, W.-C. 8-Hydroxy-2′-Deoxyguanosine of leukocyte DNA as a marker of oxidative stress in chronic hemodialysis patients. Am. J. Kidney Dis. 2000, 36, 934–944. [Google Scholar] [CrossRef] [PubMed]
- Stevens, P.E.; Levin, A. Kidney Disease: Improving Global Outcomes Chronic Kidney Disease Guideline Development Work Group Members. Evaluation and management of chronic kidney disease: Synopsis of the kidney disease: Improving global outcomes 2012 clinical practice guideline. Ann. Intern. Med. 2013, 158, 825–830. [Google Scholar] [CrossRef] [Green Version]
- Muñiz, P.; Valls, V.; Perez-Broseta, C.; Iradi, A.; Climent, J.V.; Oliva, M.R.; Sáez, G. The role of 8-hydroxy-2′-deoxyguanosine in rifamycin-induced DNA damage. Free Radic. Biol. Med. 1995, 18, 747–755. [Google Scholar] [CrossRef]
- Higuchi, M.; Yoshida, F. Lowry Determination of Protein in the Presence of Sulfhydryi Compounds or Other Reducing Agents. Anal. Biochem. 1977, 2, 542–547. [Google Scholar] [CrossRef]
- Wells, W.W.; Rocque, P.A.; Yang, Y.; Deits, T.L.; Biophys Res, B.; Maellaro, E. Diversity of Glutathione Peroxidases. Adv. Enzymol. Relat. Areas Mol. Biol. 1991, 180, 471. [Google Scholar]
- Frenkel, K.; Zhong, Z.; Wei, H.; Karkoszka, J.; Patel, U.; Rashid, K.; Georgescu, M.; Solomon, J.J. Quantitative High-Performance Liquid Chromatography Analysis of DNA Oxidized in vitro and in viva. Anal. Biochem. 1991, 196, 126–136. [Google Scholar] [CrossRef]
- Berlett, B.S.; Stadtman, E.R. Protein Oxidation in Aging, Disease, and Oxidative Stress. J. Biol. Chem. 1997, 272, 20313–20316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Popolo, A.; Autore, G.; Pinto, A.; Marzocco, S. Oxidative stress in patients with cardiovascular disease and chronic renal failure. Free. Radic. Res. 2013, 47, 346–356. [Google Scholar] [CrossRef] [PubMed]
- Galvan, D.L.; Green, N.H.; Danesh, F.R. The hallmarks of mitochondrial dysfunction in chronic kidney disease. Kidney Int. 2017, 92, 1051–1057. [Google Scholar] [CrossRef] [PubMed]
- Modaresi, A.; Nafar, M.; Sahraei, Z. Oxidative stress in chronic kidney disease. Iran. J. Kidney Dis. 2015, 9, 165–179. [Google Scholar] [PubMed]
- Wei, P.Z.; Szeto, C.C. Mitochondrial dysfunction in diabetic kidney disease. Clin. Chim. Acta 2019, 496, 108–116. [Google Scholar] [CrossRef]
- Chakravarti, B.; Chakravarti, D.N. Oxidative modification of proteins: Age-related changes. Gerontology 2007, 53, 128–139. [Google Scholar] [CrossRef]
- Avery, S.V. Molecular targets of oxidative stress. Biochem. J. 2011, 434, 201–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halliwell, B.; Chirico, S. Lipid peroxidation: Its mechanism, measurement, and significance. Am. J. Clin. Nutr. 1993, 57, 715S–725S. [Google Scholar] [CrossRef] [Green Version]
- Evans, M.D.; Dizdaroglu, M.; Cooke, M.S. Oxidative DNA damage and disease: Induction, repair and significance. Mutat. Res. Mutat. Res. 2004, 567, 1195–1214. [Google Scholar] [CrossRef] [PubMed]
- Closa, D.; Puy, E.F. Oxygen Free Radicals and the Systemic Inflammatory Response. IUBMB Life 2004, 56, 185–191. [Google Scholar] [CrossRef]
- Mekki, K.; Taleb, W.; Bouzidi, N.; Kaddous, A.; Bouchenak, M. Effect of hemodialysis and peritoneal dialysis on redox status in chronic renal failure patients: A comparative study. Lipids Health Dis. 2010, 9, 93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atamer, A.; Kocyigit, Y.; Ecder, S.A.; Selek, Ş.; Ilhan, N.; Ecder, T.; Atamer, Y. Effect of oxidative stress on antioxidant enzyme activities, homocysteine and lipoproteins in chronic kidney disease. J. Nephrol. 2008, 21, 924–930. [Google Scholar] [PubMed]
- Puchades, M.; Rico, M.A.G.; Salguero, M.A.S.; Maicas, I.T.; Muñoz, M.C.T.; Tormo, G.S.; García, I.J.; Carrasco, A.M. Estudio del estrés oxidativo en enfermedad renal avanzada. Nefrologia 2009, 29, 464–473. [Google Scholar]
- Schupp, N.; Heidland, A.; Stopper, H. Genomic Damage in Endstage Renal Disease—Contribution of Uremic Toxins. Toxins 2010, 2, 2340. [Google Scholar] [CrossRef] [Green Version]
- Satoh, M.; Yamasaki, Y.; Nagake, Y.; Kasahara, J.; Hashimoto, M.; Nakanishi, N.; Makino, H. Oxidative stress is reduced by the long-term use of vitamin E-coated dialysis filters. Kidney Int. 2001, 59, 1943–1950. [Google Scholar] [CrossRef] [Green Version]
- Tarng, D.-C.; Liu, T.-Y.; Huang, T.-P. Protective effect of vitamin C on 8-hydroxy-2′-deoxyguanosine level in peripheral blood lymphocytes of chronic hemodialysis patients. Kidney Int. 2004, 66, 820–831. [Google Scholar] [CrossRef] [Green Version]
- Rangel-Lopez, A.; Paniagua-Medina, M.E.; Urban-Reyes, M.; Cortes-Arredondo, M.; Alvarez-Aguilar, C.; López-Meza, J.E.; Ochoa-Zarzosa, A.; Lindholm, B.; Garcia-Lopez, E.; Paniagua, J.R. Genetic damage in patients with chronic kidney disease, peritoneal dialysis and haemodialysis: A comparative study. Mutagenesis 2013, 28, 219–225. [Google Scholar] [CrossRef] [Green Version]
- Townsend, D.M.; Tew, K.D.; Tapiero, H. The importance of glutathione in human disease. Biomed. Pharmacother. 2003, 57, 145–155. [Google Scholar] [CrossRef]
- Ceballos-Picot, I.; Witko-Sarsat, V.; Merad-Boudia, M.; Nguyen, A.T.; Thévenin, M.; Jaudon, M.C.; Zingraff, J.; Verger, C.; Jingers, P.; Descamps-Latscha, B. Glutathione antioxidant system as a marker of oxidative stress in chronic renal failure. Free Radic. Biol. Med. 1996, 21, 845–853. [Google Scholar] [CrossRef]
- Annuk, M.; Fellström, B.; Akerblom, O.; Zilmer, K.; Vihalemm, T.; Zilmer, M. Oxidative stress markers in pre-uremic patients. Clin. Nephrol. 2001, 56, 208–214. [Google Scholar]
- Puchades, M.J.; Sáez, G.; Muñoz, M.C.; Gonzalez, M.; Torregrosa, I.; Juan, I.; Miguel, A. Study of oxidative stress in patients with advanced renal disease and undergoing either hemodialysis or peritoneal dialysis. Clin. Nephrol. 2013, 80, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Ureña-Torres, P.; D’Marco, L.; Raggi, P.; García–Moll, X.; Brandenburg, V.; Mazzaferro, S.; Lieber, A.; Guirado, L.; Bover, J. Valvular heart disease and calcification in CKD: More common than appreciated. Nephrol. Dial. Transplant. 2020, 35, 2046–2053. [Google Scholar] [CrossRef]
- Zager, R.A.; Johnson, A.C.; Guillem, A.; Keyser, J.; Singh, B. A Pharmacologic “Stress Test” for Assessing Select Antioxidant Defenses in Patients with CKD. Clin. J. Am. Soc. Nephrol. 2020, 15, 633–642. [Google Scholar] [CrossRef]
- Tang, Y.; Yang, Q.; Lu, J.; Zhang, X.; Suen, D.; Tan, Y.; Jin, L.; Xiao, J.; Xie, R.; Rane, M.; et al. Zinc supplementation partially prevents renal pathological changes in diabetic rats. J. Nutr. Biochem. 2010, 21, 237–246. [Google Scholar] [CrossRef]
- Parham, M.; Amini, M.; Aminorroaya, A.; Heidarian, E. Effect of Zinc Supplementation on Microalbuminuria in Patients with Type 2 Diabetes: A Double Blind, Randomized, Placebo-Controlled, Cross-Over Trial. Rev. Diabet. Stud. 2008, 5, 102–109. [Google Scholar] [CrossRef] [Green Version]
- Chin, M.P.; Bakris, G.L.; Block, G.A.; Chertow, G.M.; Goldsberry, A.; Inker, L.A.; Heerspink, H.J.; O’Grady, M.; Pergola, P.E.; Wanner, C.; et al. Bardoxolone Methyl Improves Kidney Function in Patients with Chronic Kidney Disease Stage 4 and Type 2 Diabetes: Post-Hoc Analyses from Bardoxolone Methyl Evaluation in Patients with Chronic Kidney Disease and Type 2 Diabetes Study. Am. J. Nephrol. 2018, 47, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Chertow, G.M.; Pergola, P.E.; Chen, F.; Kirby, B.J.; Sundy, J.S.; Patel, U.D. For the GS-US-223-1015 Investigators Effects of Selonsertib in Patients with Diabetic Kidney Disease. J. Am. Soc. Nephrol. 2019, 30, 1980–1990. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, H.H.; Stocker, R.; Vollbracht, C.; Paulsen, G.; Riley, D.; Daiber, A.; Cuadrado, A. Antioxidants in Translational Medicine. Antioxid. Redox Signal. 2015, 23, 1130–1143. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| G3A | G3B | G4 | G5-NDD | CONTROLS | |
|---|---|---|---|---|---|
| eGFR, mL/min/1.73 m2 | (60–45) | (45–30) | (30–15) | (<15) | (≥90) |
| Number of patients | 37 | 47 | 47 | 24 | 45 |
| Male (%) | 67.6 | 74.5 | 57.4 | 66.7 | 51.1 |
| Age, years * | 65.49 (31–80) | 68.62 (44–80) | 69.26 (42–80) | 68.79 (45–80) | 67.8 (33–80) |
| Etiology (%) | |||||
| Nephroangiosclerosis | 41.2 | 37.9 | 29.9 | 52.1 | |
| Diabetic kidney disease | 25.5 | 16.4 | 22.3 | 19.4 | |
| Interstitial Nephritis | 5.8 | 15.3 | 15.7 | 8.1 | |
| Obstructive nephropathy | 5.9 | 2.2 | 4.3 | -- | |
| Polycystic kidney disease | 8.8 | 8.7 | 8.5 | 4.3 | |
| Glomerulonephritis | 5.9 | 8.7 | 10.6 | 6.1 | |
| Others/Unknown etiology | 6.8 | 10.9 | 8.6 | 9.9 |
| Cardiovascular Risk Factors (%) | G3A | G3B | G4 | G5-NDD | TOTAL |
|---|---|---|---|---|---|
| Active smoker | 29.4 | 19.6 | 24.4 | 17.4 | 22.7 |
| Hypertension | 91.2 | 93.5 | 93.6 | 91.3 | 92.4 |
| Hypercholesterolemia | 79.4 | 89.1 | 91.5 | 95.7 | 88.9 |
| Hypertriglyceridemia | 23.5 | 23.9 | 21.3 | 30.4 | 24.8 |
| Type 2 Diabetes Mellitus | 54.1 | 44.7 | 48.9 | 41.7 | 47.4 |
| Hyperhomocisteinemia | 35.13 | 65.95 | 80.85 | 91.66 | 68.3 |
| CARDIOVASCULAR DISEASE (%) | G3A | G3B | G4 | G5-NDD | TOTAL |
|---|---|---|---|---|---|
| Coronary heart disease | 52.9 | 63 | 65.2 | 76.6 | 64.4 |
| Atrial fibrillation | 8.8 | 10.9 | 17 | 17.4 | 13.5 |
| Heart failure | 20.6 | 26.1 | 36.2 | 26.1 | 27.3 |
| Cerebrovascular disease | 8.8 | 13 | 6.4 | 4.3 | 8.1 |
| Peripheral artery disease | 23.5 | 21.7 | 21.3 | 39.1 | 26.4 |
| Biochemical/CKD | G3A | G3B | G4 | G5-NDD |
|---|---|---|---|---|
| eGFR (ml/min/1.73 m2) * | 50.55 ± 3.97 49.01–52.09 | 37.28 ± 4.82 35.71–38.84 | 23.29 ± 4.82 21.73–24.86 | 11.48 ± 1.86 10.55–12.41 |
| Uric acid (mg/dL) * | 6.95 ± 1.51 6.36–7.53 | 6.10 ± 1.49 5.62–6.58 | 6.42 ± 1.62 5.89–6.94 | 6.95 ± 2.59 5.66–8.24 |
| Total cholesterol (mg/dL) * | 172.11 ± 41.45 156.03–188.18 | 164.28 ± 31.00 154.23–174.33 | 158.46 ± 35.15 147.07–169.86 | 162.00 ± 37.71 143.25–180.75 |
| HDL-c (mg/dL) * | 46.79 ± 13.63 41.50–52.07 | 48.18 ± 10.49 44.78–51.58 | 44.59 ± 12.75 40.46–48.72 | 46.33 ± 13.94 39.40–53.27 |
| LDL-c (mg/dL) * | 107.36 ± 36.23 93.31–121.41 | 100.15 ± 23.16 92.64–107.66 | 94.67 ± 26.32 86.13–103.20 | 101.17 ± 31.62 85.44–116.89 |
| Triglycerides (mg/dL) ** | 129.5 94.25–171.00 | 117.00 81.00–168.5 | 144.00 99.50–195.00 | 112.00 78.00–171.00 |
| Total proteins (g/dL) * | 6.94 ± 0.32 6.82–7.07 | 7.13 ± 0.41 6.99–7.26 | 7.04 ± 0.46 6.89–7.19 | 6.9 ± 0.58 6.60–7.19 |
| Hemoglobin (g/dL) * | 13.43 ± 1.27 12.94–13.93 | 12.50 ± 1.70 11.95–13.05 | 12.51 ± 1.10 12.15–12.87 | 11.32 ± 1.31 10.67–11.97 |
| Glucose (mg/dL) ** | 112.5 100.25–144.5 | 112.00 95.00–136.00 | 116.00 100.00–142.00 | 101.5 91.00–135.00 |
| Serum creatinine (mg/dL) ** | 1.36 1.15–1.45 | 1.69 1.46–1.84 | 2.32 2.02–2.89 | 4.58 4.08–5.18 |
| Urea (mg/dL) ** | 56.5 46.5–67.00 | 72.00 58.5–82.5 | 93.00 86.5–112.00 | 144.00 126.00–179.00 |
| Iron (µg/dL) ** | 67.5 52.5–76.5 | 67.00 51.00–91.50 | 75.00 60.50–92.50 | 60.00 45.00–67.00 |
| TSAT (%) ** | 22.05 15.63–25.85 | 20.40 16.05–26.70 | 26.20 19.55–31.10 | 20.70 16.90–25.10 |
| Ferritin (ng/mL) ** | 95.00 32.25–140.05 | 94.00 64–150 | 92.00 60.50–200.00 | 192.50 146.00–310.00 |
| i-PTH (pg/mL) ** | 63.5 50.25–72.75 | 75.00 58.00–107.5 | 133.00 97.00–183.50 | 311.00 228.00–389.00 |
| 25-OH cholecalciferol (ng/mL) ** | 22.00 12.25–33.75 | 22.00 15.50–30.50 | 31.00 17.50–40.00 | 18.50 11.00–30.00 |
| Calcium (mg/dL)** | 9.76 9.52–10.17 | 9.60 9.30–9.95 | 9.60 9.30–9.85 | 9.20 8.90–9.50 |
| Phosphorus (mg/dL) ** | 3.15 2.8–3.45 | 3.2 2.9–3.5 | 3.50 3.20–4.10 | 4.80 4.20–5.70 |
| CKD | G3A | G3B | G4 | G5-NDD | CONTROLS | p |
|---|---|---|---|---|---|---|
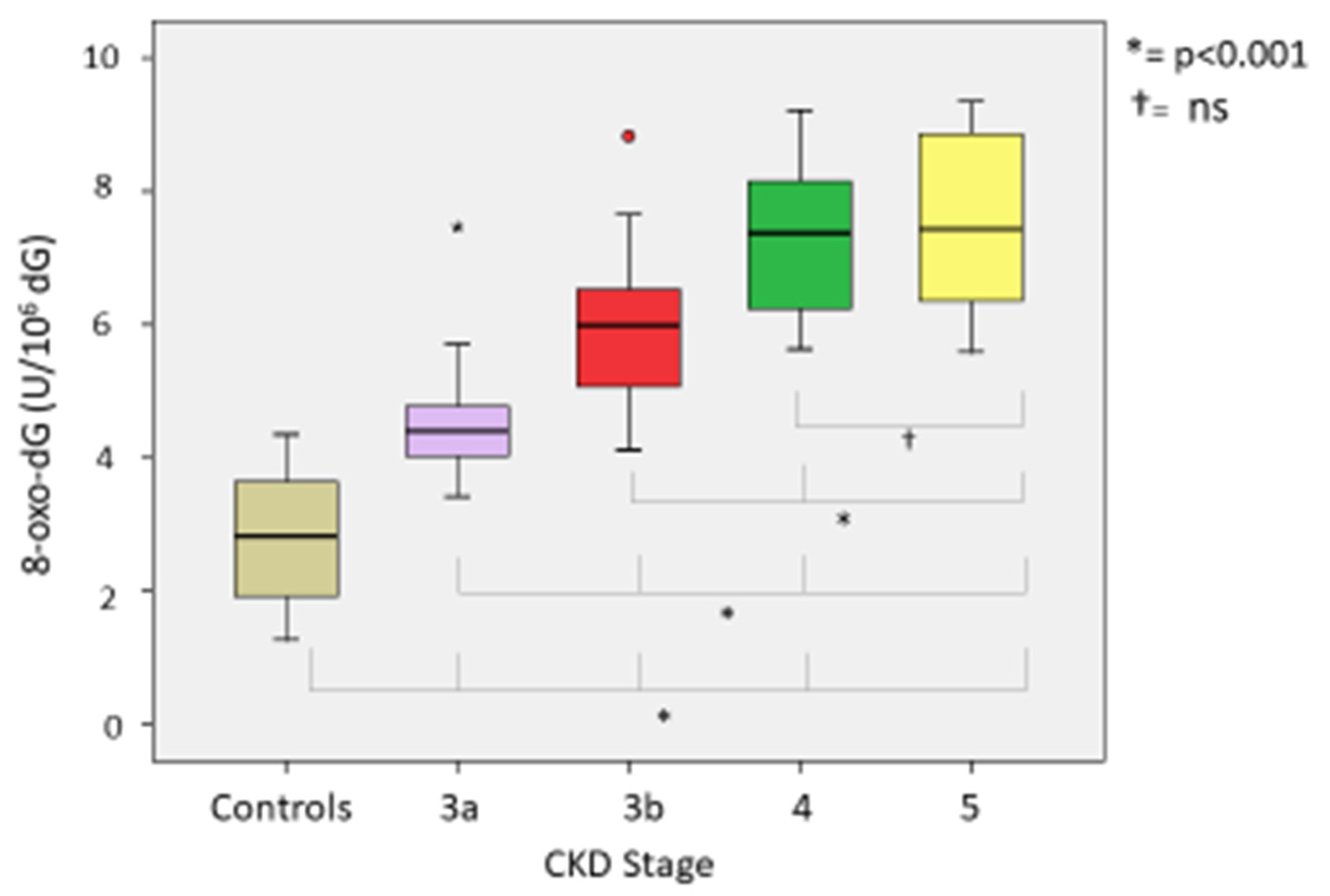
| 8-oxo-dG (U/106 dG) * | 4.51 ± 0.86 (4.22–4.8) | 5.88 ± 1.00 (5.59–6.18) | 7.31 ± 1.09 (6.99–7.63) | 7.59 ± 1.34 (7.02–8.15) | 2.75 ± 1.09 (2.43–3.08) | 0.001 |
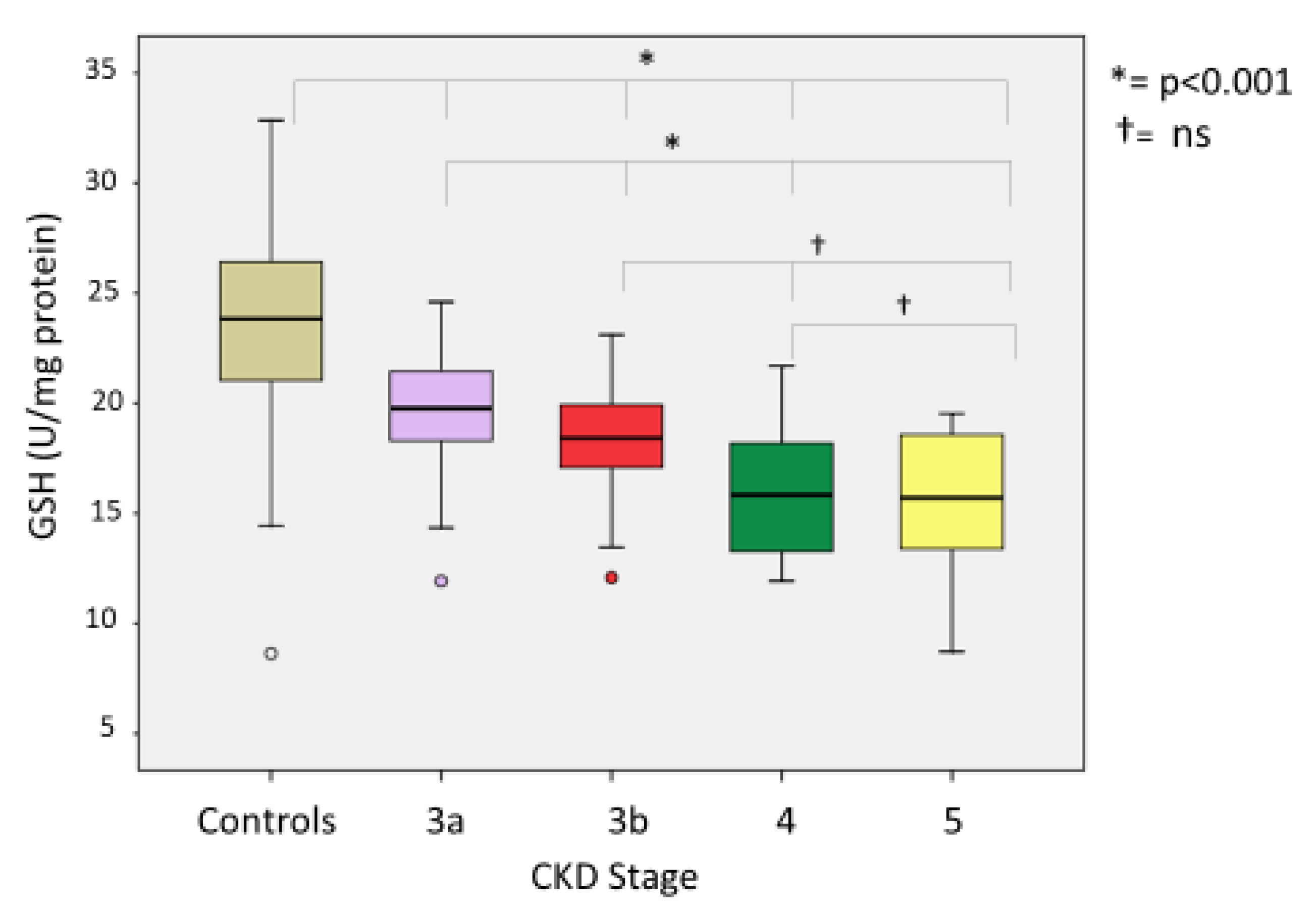
| GSH (U/mg protein) * | 19.52 ± 2.73 (18.61–20.43) | 18.31 ± 2.48 (17.58–19.04) | 15.92 ± 2.58 (15.16–16.68) | 15.50 ± 2.82 (14.30–16.69) | 23.35 ± 5.26 (21.79–24.92) | 0.001 |
| GSSG (U/mg protein) * | 4.02 ± 0.87 (3.73–4.32) | 5.28 ± 0.93 (5.01–5.56) | 6.25 ± 1.04 (5.94–6.56) | 6.94 ± 1.23 (6.42–7.46) | 0.33 ± 0.18 (0.28–0.38) | 0.001 |
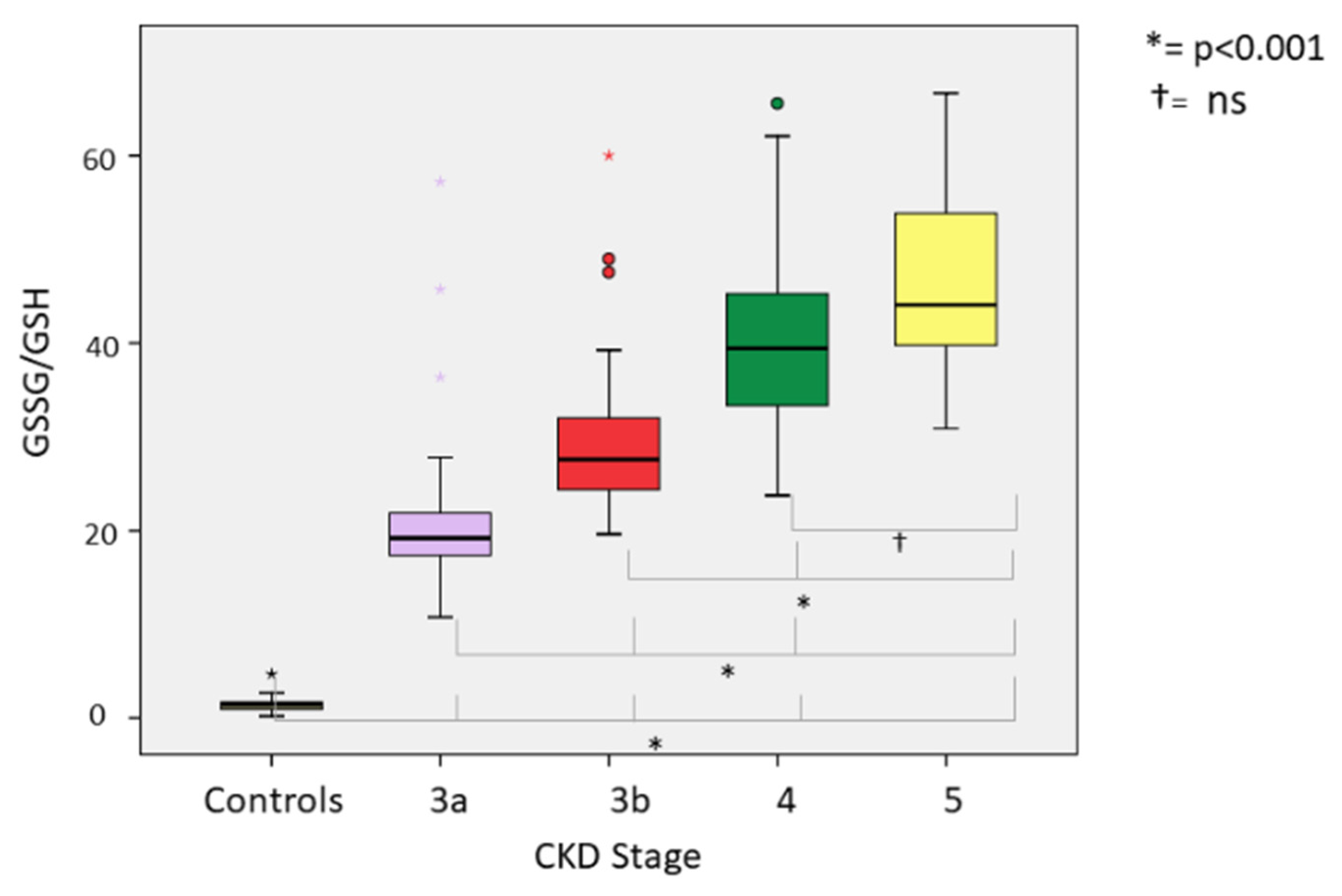
| GSSG/GSH * | 21.52 ± 8.53 (18.68–24.37) | 29.58 ± 7.92 (27.25–31.91) | 40.35 ± 9.75 (37.48–43.21) | 46.08±10.75 (41.53–50.62) | 1.33 ± 0.6 (1.15–1.51) | 0.001 |
| MDA (nmol/mg protein) * | 0.57 ± 0.11 (0.53–0.61) | 0.74 ± 0.12 (0.71–0.78) | 0.92 ± 0.13 (0.88–0.96) | 0.96 ± 0.17 (0.89–1.03) | 0.11 ± 0.05 (0.93–0.12) | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tomás-Simó, P.; D’Marco, L.; Romero-Parra, M.; Tormos-Muñoz, M.C.; Sáez, G.; Torregrosa, I.; Estañ-Capell, N.; Miguel, A.; Gorriz, J.L.; Puchades, M.J. Oxidative Stress in Non-Dialysis-Dependent Chronic Kidney Disease Patients. Int. J. Environ. Res. Public Health 2021, 18, 7806. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18157806
Tomás-Simó P, D’Marco L, Romero-Parra M, Tormos-Muñoz MC, Sáez G, Torregrosa I, Estañ-Capell N, Miguel A, Gorriz JL, Puchades MJ. Oxidative Stress in Non-Dialysis-Dependent Chronic Kidney Disease Patients. International Journal of Environmental Research and Public Health. 2021; 18(15):7806. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18157806
Chicago/Turabian StyleTomás-Simó, Patricia, Luis D’Marco, María Romero-Parra, Mari Carmen Tormos-Muñoz, Guillermo Sáez, Isidro Torregrosa, Nuria Estañ-Capell, Alfonso Miguel, José Luis Gorriz, and María Jesús Puchades. 2021. "Oxidative Stress in Non-Dialysis-Dependent Chronic Kidney Disease Patients" International Journal of Environmental Research and Public Health 18, no. 15: 7806. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18157806