
Emotional Exhaustion, Depersonalization, and Mental Health in Nurses from Huelva: A Cross-Cutting Study during the SARS-CoV-2 Pandemic

 ,
,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Evaluation Instruments
2.4. Statistical Analysis
3. Results
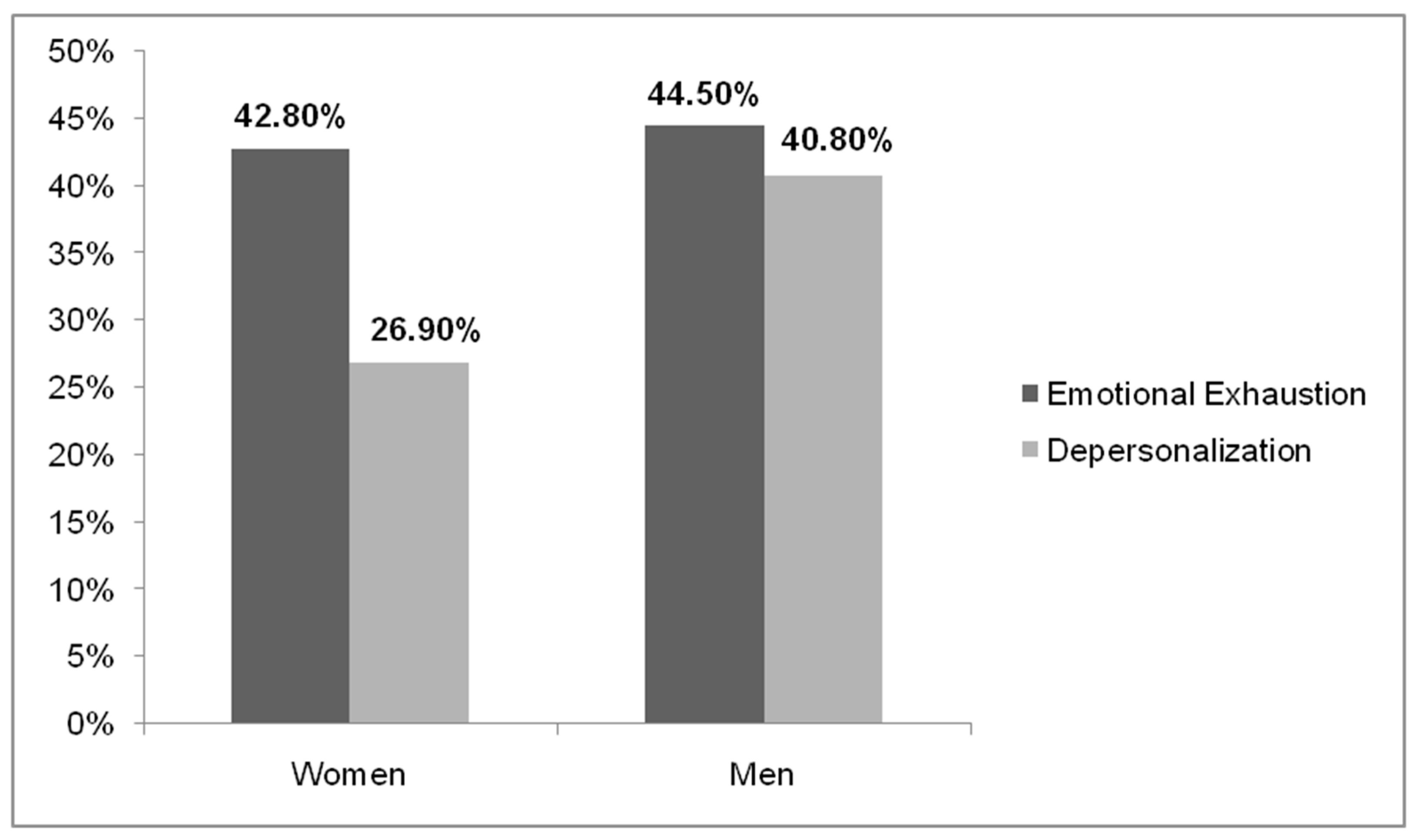
3.1. Differences in the Variables of Emotional Exhaustion and Depersonalization According to Gender
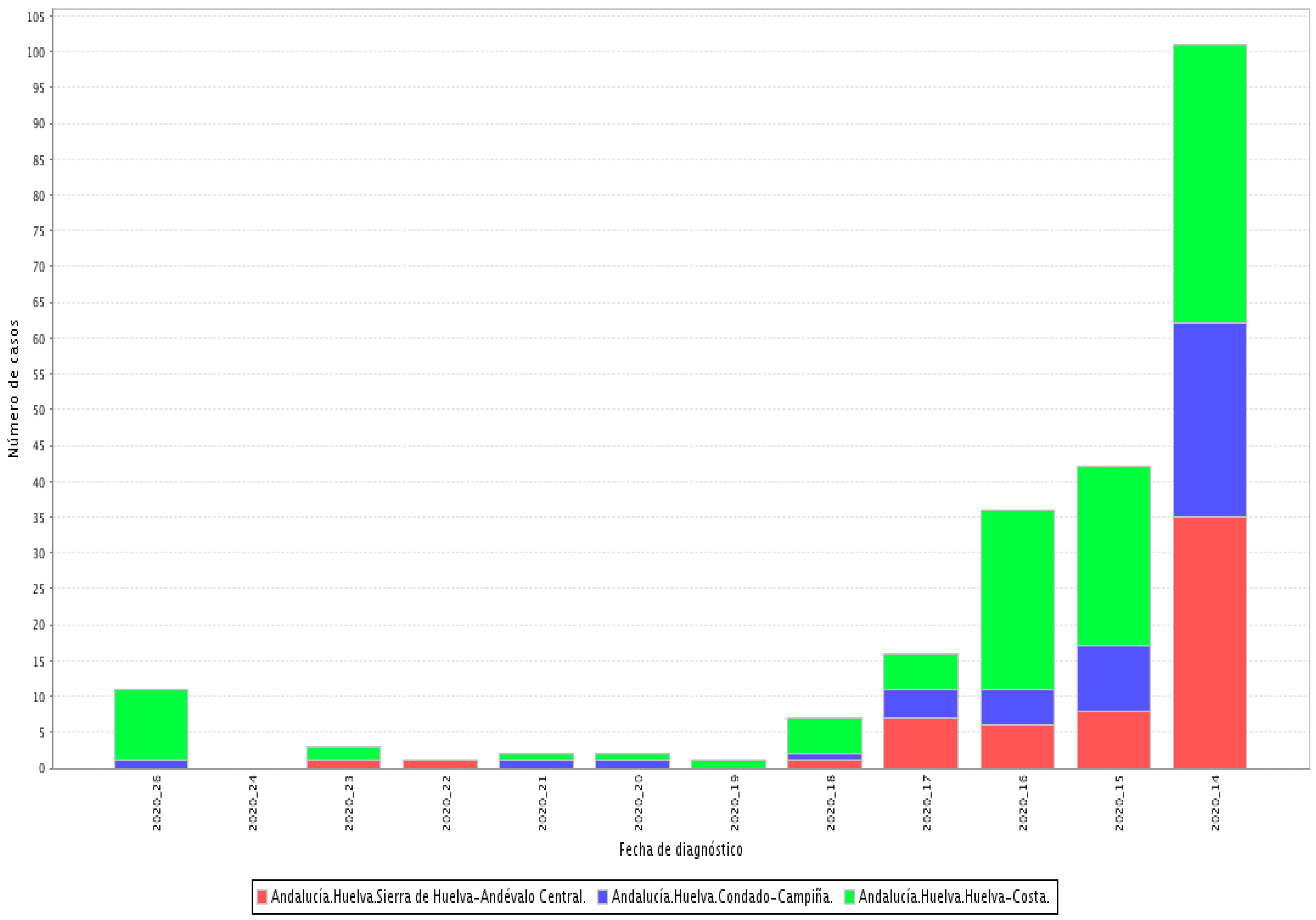
3.2. Prevalence of Emotional Exhaustion and Depersonalization as a Function of the Work Center
3.3. Differences in Emotional Exhaustion and Depersonalization According as a Function of Age, Marital Status, and Parental Status
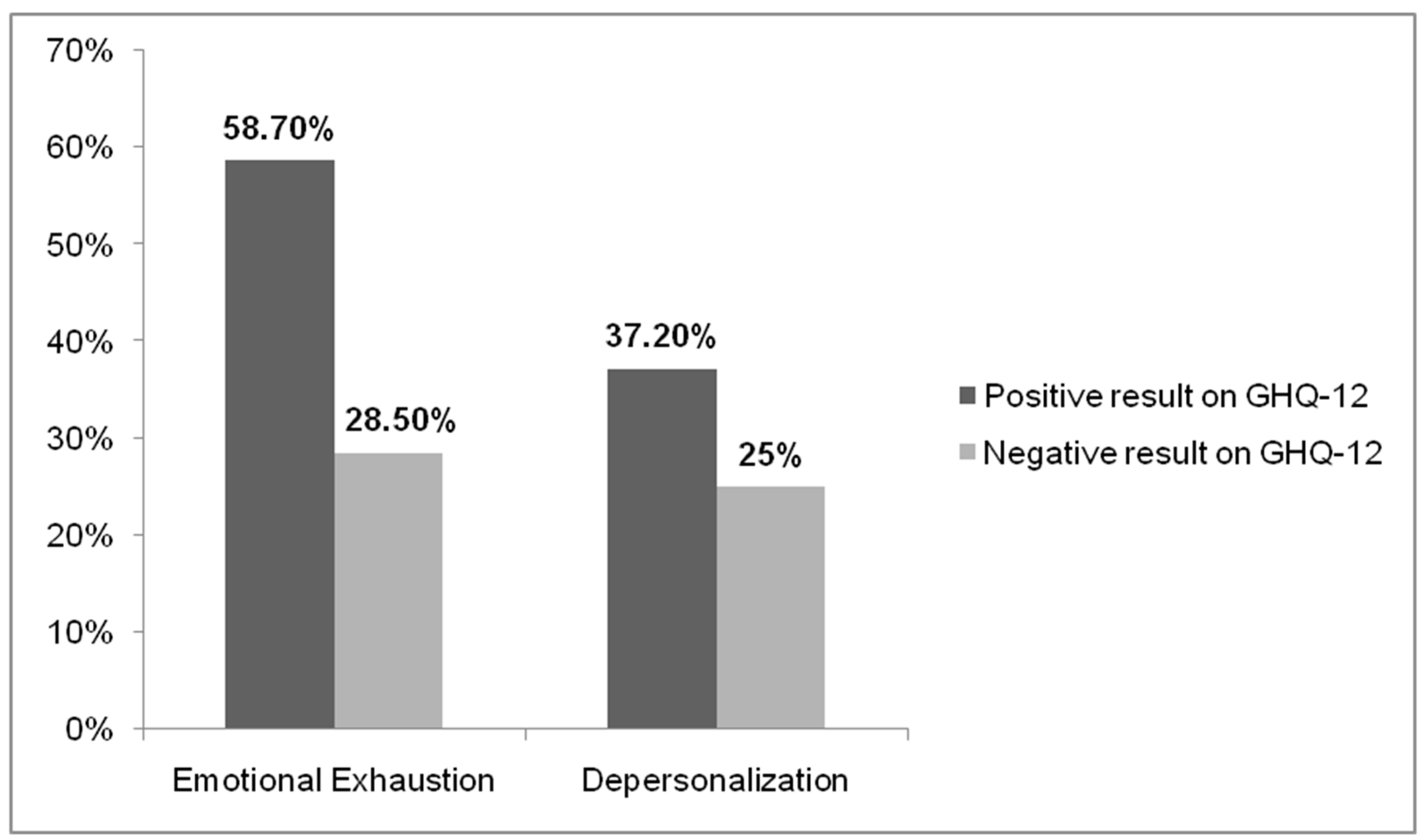
3.4. Relationship between the Variables of Emotional Exhaustion and Depersonalization and Contact with SARS-CoV-2 in the Work Environment and GHQ-12 Score
3.5. Relationship between the Possible Presence of Non-Psychotic Psychiatric Pathology (Positive GHQ-12) and Gender, Age, Marital Status, and Parental Status
3.6. Relationship between Probable Non-Psychotic Psychiatric Disorder and Contact with SARS-CoV-2 in the Work Environment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Gil-Monte, P.R. The Burnout Syndrome: An Occupational Disease in the Welfare Society; Pirámide: Madrid, Spain, 2005. [Google Scholar]
- García-Campayo, J.; Puebla-Guedea, M.; Herrera-Mercadal, P.; Daudén, E. Burnout Syndrome and Demotivation among Health Care Personnel. Managing Stressful Situations: The Importance of Teamwork. Actas Dermosifiliogr. 2016, 107, 400–406. [Google Scholar] [CrossRef] [PubMed]
- Santamaría, M.D.; Etxebarria, N.O.; Rodriguez, I.R.; Albondiga-Mayor, J.J.; Gorrochategui, M.P. Psychological impact of COVID-19 in a sample of Spanish healthcare professionals. Rev. Psychiatr. Salud Ment. 2020. [Google Scholar] [CrossRef]
- Bai, Y.; Lin, C.-C.; Lin, C.-Y.; Chen, J.-Y.; Chue, C.-M.; Chou, P. Survey of stress reactions among health care workers involved with the SARS outbreak. Psychiatr. Serv. 2004, 55, 1055–1057. [Google Scholar] [CrossRef] [PubMed]
- Maunder, R.; Hunter, J.; Vincent, L.; Bennett, J.; Peladeau, N.; Leszcz, M.; Sadavoy, J.; Verhaeghe, L.M.; Steinberg, R.; Mazzulli, T. The immediate psychological and occupational impact of the 2003 SARS outbreak in a teaching hospital. CMAJ 2003, 168, 1245–1251. [Google Scholar]
- Lee, S.M.; Kang, W.S.; Cho, A.R.; Kim, T.; Park, J.K. Psychological impact of the 2015 MERS outbreak on hospital workers and quarantined hemodialysis patients. Compr. Psychiatry 2018, 87, 123–127. [Google Scholar] [CrossRef]
- Chen, Q.; Liang, M.; Li, Y.; Guo, J.; Fei, D.; Wang, L.; He, L.; Sheng, C.; Cai, Y.; Li, X.; et al. Mental health care for medical staff in china during the COVID-19 outbreak. Lancet Psychiatry 2020, 7, e15–e16. [Google Scholar] [CrossRef]
- Li, Z.; Ge, J.; Yang, M.; Feng, J.; Qiao, M.; Jiang, R.; Bi, J.; Zhan, G.; Xu, X.; Wang, L.; et al. Vicarious traumatization in the general public, members, and non-members of medical teams aiding in COVID-19 control. Brain Behav. Immun. 2020, 88, 916–919. [Google Scholar] [CrossRef]
- Tifner, S.; Martín, P.; Albanesi-De-Nasetta, S.; De-Bortoli, M. Burnout in the teaching profession. Burnout and Teaching. STVDIVM. J. Humanit. 2006, 12, 279–291. [Google Scholar]
- Ng, Q.X.; De Deyn, M.L.Z.Q.; Lim, D.Y.; Chan, H.W.; Yeo, W.S. The wounded healer: A narrative review of the mental health effects of the COVID-19 pandemic on healthcare workers. Asian J. Psychiatr. 2020, 54, 102258. [Google Scholar] [CrossRef] [PubMed]
- Peterson, U.; Demerouti, E.; Bergström, G.; Samuelsson, M.; Asberg, M.; Nygren, A. Burnout and physical and mental health among Swedish healthcare workers. J. Adv. Nurs. 2008, 62, 84–95. [Google Scholar] [CrossRef]
- Lee, R.T.; Ashforth, B.E. Un examen meta-analítico de la correlación de las tresdimensiones del Burnout. Diario de Psicología Aplicada 1996, 81, 123–133. [Google Scholar]
- Kristensen, T.S.; Borritz, M.; Villadsen, E.; Christensen, K.B. The Copenhagen Burnout Inventory: A new tool for the assessment of burnout. Work Stress 2005, 19, 192–207. [Google Scholar] [CrossRef]
- Schutte, N.; Toppinnen, S.; Kalimo, R.; Schaufeli, W.B. The factorial validity of the Maslach Burnout Inventory-General Survey (MBI-GS) across ations and occupations. J. Occup. Organ. Psychol. 2000, 73, 53–66. [Google Scholar] [CrossRef]
- Consejería de Salud y Familias de la Junta de Andalucía. Informe COVID-19 en Andalucía. Dirección General de Salud Pública y Ordenación Farmacéutica. Sistema de Vigilancia Epidemiológica de Andalucía. Available online: http://www.juntadeandalucia.es/institutodeestadisticaycartografia/salud/COVID19.html (accessed on 28 June 2021).
- Maslach, C.; Jackson, S.E. Maslach Burnout Inventory Manual, 3rd ed.; Consulting Psychologists Press: Palo Alto, CA, USA, 1982. [Google Scholar]
- Maslach, C.; Schaufeli, W.B.; Leiter, M.P. Professional burnout. Annu. Rev. Psychol. 2001, 52, 397–422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maslach, C.; Jackson, S.E. The measurement of experienced burnout. J. Organ. Behav. 1998, 2, 99–113. [Google Scholar] [CrossRef]
- Goldberg, D.; Williams, P. User’s Guide to the General Health Questionnaire; NFER-Nelson: Berkshire, UK, 1988. [Google Scholar]
- Muñoz, P.E.; Vázquez, J.L.; Insausti, F.R.; Pastrana, E.; Varo, J. Spanish adaptation of the General Health Questionnaire (GHQ) of Goldberg. Arch. Neurobiol. 1979, 42, 139–158. [Google Scholar]
- Sánchez-López, M.P.; Dresch, V. The 12-Item General Health Questionnaire (GHQ-12): Reliability, external validity and factor structure in the Spanish population. Psicothema 2008, 20, 839–843. [Google Scholar]
- Gispert, R.; Rajmil, L.; Schiaffino, A.; Herdman, M. Sociodemographic and health-related correlates of psychiatric distress in a general population. Soc. Psychiatry Psychiatr. Epidemiol. 2003, 38, 677–683. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, F.J.; García-Beltrán, D.M.; Suárez-Falcón, J.C. General Health Questionnaire-12 validity in Colombia and factorial equivalence between clinical and non clinical participants. Psychiatry Res. 2017, 256, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Burrone, M.S.; Abeldaño, A.; Lucchese, M.; Susser, L.; Enders, J.E.; Alvarado, R.; Valencia, E.; Fernández, A.R. Psychometric evaluation and reliability study of the general health questionnaire (GHQ-12) in adult patients at the first level of care in Córdoba—Argentina. J. Fac. Med. Sci. Córdoba 2015, 72, 236–242. [Google Scholar]
- Adriaenssens, J.; De-Gucht, V.; Maes, S. Determinants and prevalence of burnout in emergency nurses: A systematic review of 25 years of research. BMC Nurs. 2015, 52, 649–661. [Google Scholar] [CrossRef]
- Tziner, A.; Rabenu, E.; Radomski, R.; Belkin, A. Work stress and turnover intentions among hospital physicians: The mediating role of burnout and work satisfaction. J. Work Organ. Psychol. 2015, 31, 207–213. [Google Scholar] [CrossRef] [Green Version]
- Ogińska-Bulik, N. Job stress and its consequences in healthcare professionals: The role of personality type D. Rev. Int. Med. Trab. Sal. Amb. 2016, 19, 113–122. [Google Scholar]
- Piñeiro, I.; Rodríguez, S.; Albite, A.; Freire, C.; Ferradás, M.M. Overload and perceived health in informal caregivers of patients with mental illness. Eur. J. Health Res. 2017, 3, 185–196. [Google Scholar] [CrossRef]
- Mamani-Encalada, A.; Obando-Zegarra, R.; Uribe-Malca, A.M.; Vivanco-Tello, M. Factors that trigger stress and its consequences in emergency work performance. Rev. Peru. Obst. Enferm. 2009, 3, 50–57. Available online: http://www.aulavirtualusmp.pe/ojs/index.php/rpoe/article/viewFile/543/415 (accessed on 3 February 2021).
- Schaufeli, W.B.; Leiter, M.P.; Maslach, C. Burnout: 35 years of research and practice. Career Dev. Int. 2009, 14, 204–220. [Google Scholar] [CrossRef] [Green Version]
- Cabrera, J.H.; Elvira, J.A. Stress and burnout in teachers. Int. J. Clin. Health Psychol. 2004, 4, 597–621. [Google Scholar]
- Carlotto, M.S. Análise da produçãocientíficasobre a Síndrome de Burnout no Brasil. Psico 2008, 39, 152–158. [Google Scholar]
- Leiter, M.P.; Maslach, C. The impact of interpersonal environment on burnout and organizational commitment. J. Organ. Behav. 2008, 9, 297–308. [Google Scholar] [CrossRef]
- Muñoz-del-Carpio, A.; Arias, L.; Caycho-Rodríguez, T. Burnout syndrome in medicine men from Arequipa city (Peru). Rev. Chil. Neuro-Psiquiat. 2019, 57, 139–148. [Google Scholar] [CrossRef] [Green Version]
- Ballester-Arnal, R.; Gómez-Martínez, S.; Gil, J.B.; Ferrandiz-Sellés, M.; Collado-Boira, E. Burnout and stressors in healthcare professionals in intensive care units. Rev. Psicopatol. Psicol. Clín. 2016, 21, 129–136. [Google Scholar] [CrossRef] [Green Version]
- Quevedo, H.C. Personal Fulfillment and Creativity of the Architectural Design I Student of the César Vallejo University of Trujillo in the 2016-II Cycle. Master’s Thesis, Universidad César Vallejo, Trujillo, Peru, 2016. [Google Scholar]
- Rodríguez-Contreras, P.; Santos-Iglesias, P. Relationship between perceived health status and health indicators in the Spanish population. Int. J. Clin. Health Psychol. 2007, 7, 883–898. [Google Scholar]
- Marenco-Escuderos, A.D.; Ávila-Toscano, J.H. Dimensions of social support associated with burnout syndrome in academic middle school teachers. Pensamiento Psicológico 2016, 14, 7–18. [Google Scholar] [CrossRef] [Green Version]
- Hunter, E.C.M.; Sierra, M.; David, A.S. The epidemiology of depersonalization and derealization: A systematic review. Soc. Psychiatry Psychiatr. Epidemiol. 2004, 39, 9–18. Available online: https://pubmed.ncbi.nlm.nih.gov/15022041/ (accessed on 3 February 2021). [PubMed]
- Ng, Q.X.; Lim, D.Y.; Chee, K.T. Reimagining the spectrum of affective disorders. Bipolar Disord. 2020, 22, 638–639. [Google Scholar] [CrossRef] [PubMed]
- Erquicia, J.; Valls, L.; Barja, A.; Gil, S.; Miquel, J.; Leal-Blanquet, J.; Schmidt, C.; Checa, J.; Vega, D. Emotional impact of the Covid-19 pandemic on healthcare workers in one of the most important foci of contagion in Europe. Med. Clin. 2020, 155, 434–440. [Google Scholar] [CrossRef]
- Pérez-Ortega, S.; Mesa, R.; Fernández, C.; Valverde, J. Situation of the cardiology nurse during the COVID-19 pandemic. Enferm Cardiol. 2020, 27, 82–89. [Google Scholar]
- Zhang, J.; Deng, X.; Liu, H.; Xu, X.; Fang, R. Evaluation of the mental health status of community healthcare workers during the COVID-19 outbreak. Medicine 2021, 100, e24739. [Google Scholar] [CrossRef] [PubMed]
- Trumello, C.; Bramanti, S.M.; Ballarotto, G.; Candelori, C.; Cerniglia, L.; Cimino, S.; Crudele, M.; Lombardi, L.; Pignataro, S.; Viceconti, M.L.; et al. Psychological Adjustment of Healthcare Workers in Italy during the COVID-19 Pandemic: Differences in Stress, Anxiety, Depression, Burnout, Secondary Trauma, and Compassion Satisfaction between Frontline and Non-Frontline Professionals. Int. J. Environ. Res. Public Health 2020, 17, 8358. [Google Scholar] [CrossRef]
- Cañadas-De la Fuente, G.A.; Ortega, E.; Ramirez-Baena, L.; De la Fuente-Solana, E.I.; Vargas, C.; Gómez-Urquiza, J.L. Gender, Marital Status, and Children as Risk Factors for Burnout in Nurses: A Meta-Analytic Study. Int. J. Environ. Res. Public Health 2018, 15, 2102. [Google Scholar] [CrossRef] [Green Version]
- Rusca, K.; Setyowatia. Prevalence of burnout síndrome among nurses in general hospitals in provincial East Java: Cross-sectional study. Enferm. Clin. 2019, 29, 362–366. [Google Scholar] [CrossRef] [PubMed]
- Molina-Praena, J.; Ramirez-Baena, L.; Gómez-Urquiza, J.L.; Cañadas, G.R.; De la Fuente, E.I.; Cañadas-De la Fuente, G.A. Levels of Burnout and Risk Factors in Medical Area Nurses: A Meta-Analytic Study. Int. J. Environ. Res. Public Health 2018, 15, 2800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ng, Q.X.; Chee, K.T.; De Deyn, M.L.Z.Q.; Chua, Z. Staying connected during the COVID-19 pandemic. Int. J. Soc. Psychiatry 2020, 66, 519–520. [Google Scholar] [CrossRef] [PubMed]
- González-Jiménez, A.J.; López-Martínez, M.J.; Zapata-Boluda, R.M.; Cala, V.; Dalouh, R. Educational Research and Cross-Cultural Health in Multicultural Contexts; Editorial Universidad de Almería: Almería, Spain, 2016. [Google Scholar]
- Webb Hooper, M.; Nápoles, A.M.; Pérez-Stable, E.J. COVID-19 and Racial/Ethnic Disparities. JAMA 2020, 323, 2466–2467. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Spearman’s Rho | Age | Emotional Exhaustion | Depersonalization | |
|---|---|---|---|---|
| Age | Correlation coefficient | 1.000 | 0.157 ** | 0.035 |
| Sig. (bilateral) | 0.0 | 0.000 | 0.266 | |
| N | 318 | 318 | 318 | |
| Emotional exhaustion | Correlation coefficient | 0.157 ** | 1.000 | 0.363 ** |
| Sig. (bilateral) | 0.000 | 0.0 | 0.000 | |
| N | 318 | 318 | 318 | |
| Depersonalization | Correlation coefficient | 0.035 | 0.363 ** | 1.000 |
| Sig. (bilateral) | 0.266 | 0.000 | 0.0 | |
| N | 318 | 318 | 318 | |
| Variables | Emotional Exhaustion | Depersonalization |
|---|---|---|
| Marital status | ||
| Pearson’s chi-square | 67.688 | 60.043 |
| Asymptotic significance (bilateral) | 0.000 * | 0.000 * |
| Independent Variables | Possible Presence of Non-Psychotic Psychiatric Pathology | Pearson’s Chi-Square | Asymptotic Significance (Bilateral) | ||
|---|---|---|---|---|---|
| Yes (%) | No (%) | ||||
| Sex | Man | 48.6% | 51.4% | 0.076 | 0.782 * |
| Woman | 47.6% | 52.4% | |||
| Marital status | Married | 52.6% | 47.4% | 23.588 | 0.000 * |
| Single | 48.1% | 51.9% | |||
| Divorced | 39.2% | 60.8% | |||
| Widower | 64.3% | 35.7% | |||
| With a partner | 32.0% | 68.0% | |||
| People with children | Yes | 46.2% | 53.8% | 1.909 | 0.167 * |
| No | 50.7% | 49.3% | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gago-Valiente, F.-J.; Mendoza-Sierra, M.-I.; Moreno-Sánchez, E.; Arbinaga, F.; Segura-Camacho, A. Emotional Exhaustion, Depersonalization, and Mental Health in Nurses from Huelva: A Cross-Cutting Study during the SARS-CoV-2 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 7860. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18157860
Gago-Valiente F-J, Mendoza-Sierra M-I, Moreno-Sánchez E, Arbinaga F, Segura-Camacho A. Emotional Exhaustion, Depersonalization, and Mental Health in Nurses from Huelva: A Cross-Cutting Study during the SARS-CoV-2 Pandemic. International Journal of Environmental Research and Public Health. 2021; 18(15):7860. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18157860
Chicago/Turabian StyleGago-Valiente, Francisco-Javier, María-Isabel Mendoza-Sierra, Emilia Moreno-Sánchez, Félix Arbinaga, and Adrián Segura-Camacho. 2021. "Emotional Exhaustion, Depersonalization, and Mental Health in Nurses from Huelva: A Cross-Cutting Study during the SARS-CoV-2 Pandemic" International Journal of Environmental Research and Public Health 18, no. 15: 7860. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18157860