
Effects of a Midwife-Coordinated Maternity Care Intervention (ChroPreg) vs. Standard Care in Pregnant Women with Chronic Medical Conditions: Results from a Randomized Controlled Trial

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Setting and Participants
2.3. Randomization and Blinding
2.4. Standard Care
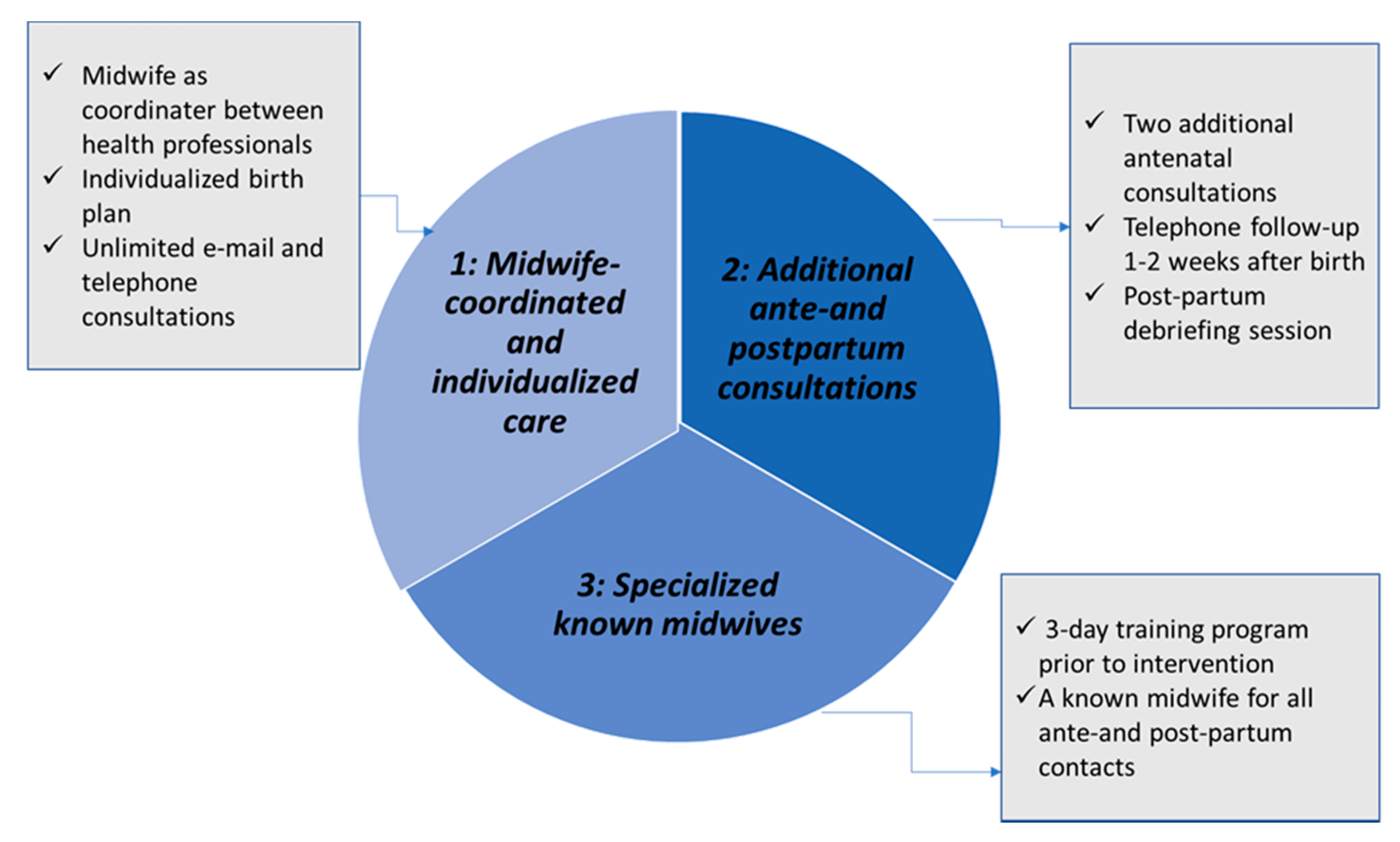
2.5. ChroPreg Intervention in Addition to Standard Care
2.6. Prespecified Outcomes
2.6.1. Primary Outcome
2.6.2. Secondary Outcomes
2.7. Statistical Analysis
2.8. Changes Due to COVID-19
3. Results
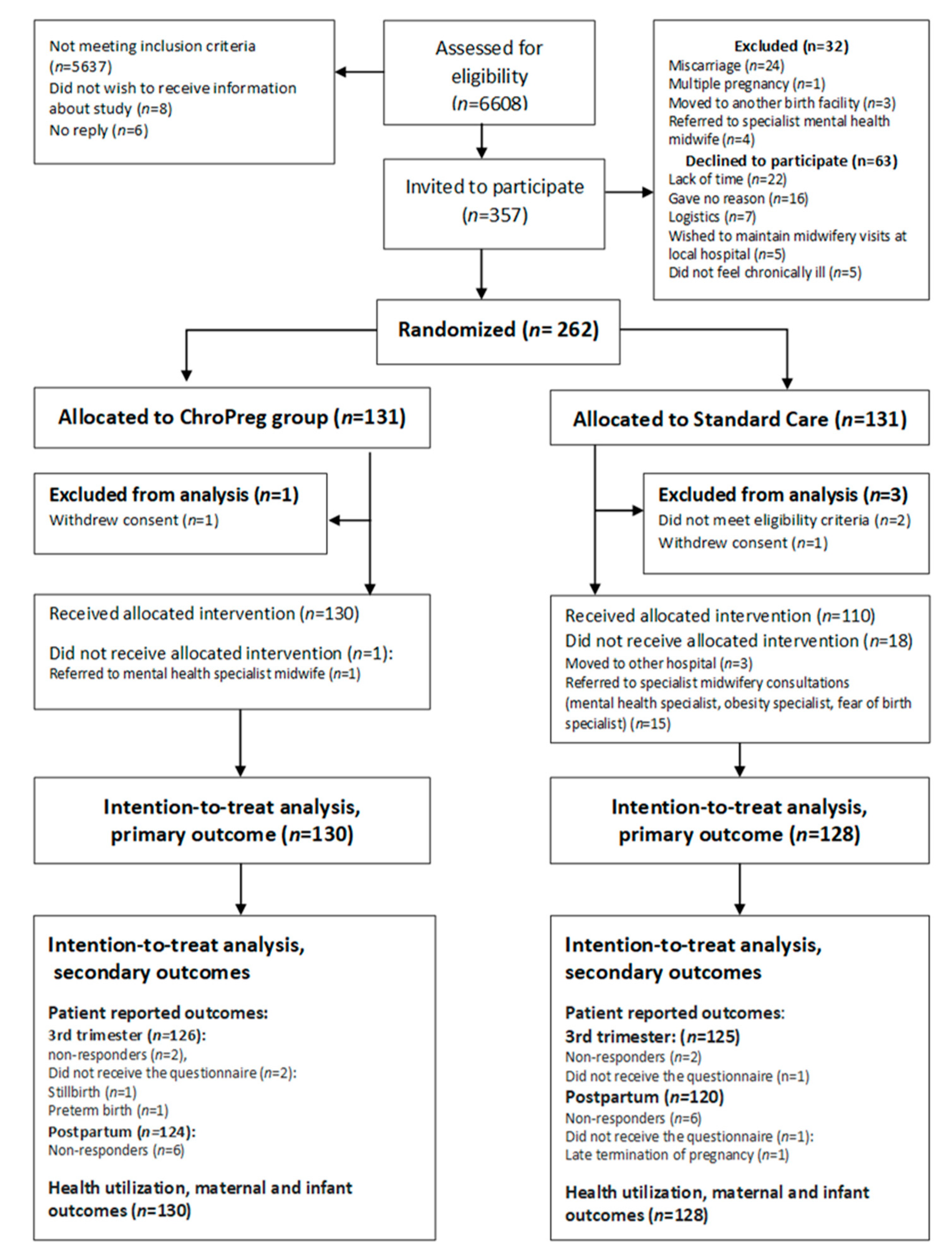
3.1. Study Population
3.2. Primary Outcome
3.3. Secondary Outcomes
4. Discussion
4.1. Main Results
4.2. Interpretation of Results
4.3. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kersten, I.; Lange, A.E.; Haas, J.P.; Fusch, C.; Lode, H.; Hoffmann, W.; Thyrian, J.R. Chronic Diseases in Pregnant Women: Prevalence and Birth Outcomes Based on the SNiP-Study. BMC Pregnancy Childbirth 2014, 14, 75. [Google Scholar] [CrossRef] [Green Version]
- Jolving, L.R.; Nielsen, J.; Kesmodel, U.S.; Nielsen, R.G.; Beck-Nielsen, S.S.; Norgard, B.M. Prevalence of Maternal Chronic Diseases during Pregnancy—A Nationwide Population Based Study from 1989 to 2013. Acta Obstet. Et Gynecol. Scand. 2016, 95, 1295–1304. [Google Scholar] [CrossRef]
- Hayes, D.K.; Robbins, C.L.; Ko, J.Y. Trends in Selected Chronic Conditions and Related Risk Factors Among Women of Reproductive Age: Behavioral Risk Factor Surveillance System, 2011–2017. J. Womens Health 2002 2020, 29, 1576–1585. [Google Scholar] [CrossRef] [PubMed]
- Wolff, M.G.D.; Johansen, M.; Rom, A.L.; Midtgaard, J.; Tabor, A.; Hegaard, H.K. Degree of Pregnancy Planning and Recommended Pregnancy Planning Behavior among Women with and without Chronic Medical Conditions—A Large Hospital-Based Cross-Sectional Study. Acta Obstet. Et Gynecol. Scand. 2021, 100, 1051–1060. [Google Scholar] [CrossRef]
- Wallenius, M.; Salvesen, K.Å.; Daltveit, A.K.; Skomsvoll, J.F. Reproductive Trends in Females with Inflammatory Joint Disease. BMC Pregnancy Childbirth 2016, 16, 123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Admon, L.K.; Winkelman, T.N.A.; Moniz, M.H.; Davis, M.M.; Heisler, M.; Dalton, V.K. Disparities in Chronic Conditions Among Women Hospitalized for Delivery in the United States, 2005–2014. Obstet. Gynecol. 2017, 130, 1319–1326. [Google Scholar] [CrossRef] [PubMed]
- Bramham, K.; Parnell, B.; Nelson-Piercy, C.; Seed, P.T.; Poston, L.; Chappell, L.C. Chronic Hypertension and Pregnancy Outcomes: Systematic Review and Meta-Analysis. BMJ 2014, 348, g2301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jara, L.J.; Medina, G.; Cruz-Dominguez, P.; Navarro, C.; Vera-Lastra, O.; Saavedra, M.A. Risk Factors of Systemic Lupus Erythematosus Flares during Pregnancy. Immunol. Res. 2014, 60, 184–192. [Google Scholar] [CrossRef] [PubMed]
- De Man, Y.A.; Dolhain, R.J.; Hazes, J.M. Disease Activity or Remission of Rheumatoid Arthritis before, during and Following Pregnancy. Curr. Opin. Rheumatol. 2014, 26, 329–333. [Google Scholar] [CrossRef]
- Brown, H.K.; Wilton, A.S.; Ray, J.G.; Dennis, C.-L.; Guttmann, A.; Vigod, S.N. Chronic Physical Conditions and Risk for Perinatal Mental Illness: A Population-Based Retrospective Cohort Study. PLoS Med. 2019, 16. [Google Scholar] [CrossRef]
- De Wolff, M.G.; Rom, A.L.; Johansen, M.; Broberg, L.; Midtgaard, J.; Tabor, A.; Hegaard, H.K. Worries among Pregnant Danish Women with Chronic Medical Conditions—A Cross Sectional Study with Data from the Copenhagen Pregnancy Cohort. Sex. Reprod. Healthc. Off. J. Swed. Assoc. Midwives 2021, 29, 100623. [Google Scholar] [CrossRef] [PubMed]
- The National Health Board National recommendations for Maternity Care. 2013. [In Danish]. Available online: https://www.sst.dk/-/media/Udgivelser/2015/Anbefalinger-svangreomsorgen/Anbefalinger-for-svangreomsorgen.ashx?la=da&hash=757F1953C4B437A70A44024B32D7DD2E1B0A9F5B (accessed on 24 July 2021).
- Narayan, B.; Nelson-Piercy, C. Medical Problems in Pregnancy. Clin. Med. 2017, 17, 251–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, C.; McCance, D.R.; Chappell, L.; Nelson-Piercy, C.; Thorne, S.A.; Ismail, K.M.K.; Green, J.S.A.; Bick, D. Implementation of Guidelines for Multidisciplinary Team Management of Pregnancy in Women with Pre-Existing Diabetes or Cardiac Conditions: Results from a UK National Survey. BMC Pregnancy Childbirth 2017, 17, 434. [Google Scholar] [CrossRef] [Green Version]
- Bick, D.; Beake, S.; Chappell, L.; Ismail, K.M.; McCance, D.R.; Green, J.S.A.; Taylor, C. Management of Pregnant and Postnatal Women with Pre-Existing Diabetes or Cardiac Disease Using Multi-Disciplinary Team Models of Care: A Systematic Review. BMC Pregnancy Childbirth 2014, 14, 428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lange, U.; Schnepp, W.; Zu Sayn-Wittgenstein, F. The experiences of chronically ill women in the time of pregnancy, birth and postnatal period—A review of qualitative studies. Z. Für Geburtshilfe und Neonatol. 2015, 219, 161–169. [Google Scholar] [CrossRef] [Green Version]
- Sandall, J.; Soltani, H.; Gates, S.; Shennan, A.; Devane, D. Midwife-Led Continuity Models versus Other Models of Care for Childbearing Women. Cochrane Database Syst. Rev. 2016, Cd004667. [Google Scholar] [CrossRef] [Green Version]
- Forster, D.A.; McLachlan, H.L.; Davey, M.-A.; Biro, M.A.; Farrell, T.; Gold, L.; Flood, M.; Shafiei, T.; Waldenström, U. Continuity of Care by a Primary Midwife (Caseload Midwifery) Increases Women’s Satisfaction with Antenatal, Intrapartum and Postpartum Care: Results from the COSMOS Randomised Controlled Trial. BMC Pregnancy Childbirth 2016, 16, 28. [Google Scholar] [CrossRef] [Green Version]
- Tracy, S.K.; Hartz, D.L.; Tracy, M.B.; Allen, J.; Forti, A.; Hall, B.; White, J.; Lainchbury, A.; Stapleton, H.; Beckmann, M.; et al. Caseload Midwifery Care versus Standard Maternity Care for Women of Any Risk: M@NGO, a Randomised Controlled Trial. Lancet 2013, 382, 1723–1732. [Google Scholar] [CrossRef]
- Cordasco, K.M.; Katzburg, J.R.; Katon, J.G.; Zephyrin, L.C.; Chrystal, J.G.; Yano, E.M. Care Coordination for Pregnant Veterans: VA’s Maternity Care Coordinator Telephone Care Program. Transl. Behav. Med. 2018, 8, 419–428. [Google Scholar] [CrossRef]
- Kroll-Desrosiers, A.R.; Crawford, S.L.; Moore Simas, T.A.; Rosen, A.K.; Mattocks, K.M. Improving Pregnancy Outcomes through Maternity Care Coordination: A Systematic Review. Womens Health Issues 2016, 26, 87–99. [Google Scholar] [CrossRef]
- Schmied, V.; Mills, A.; Kruske, S.; Kemp, L.; Fowler, C.; Homer, C. The Nature and Impact of Collaboration and Integrated Service Delivery for Pregnant Women, Children and Families. J. Clin. Nurs. 2010, 19, 3516–3526. [Google Scholar] [CrossRef]
- Lavender, T.; Richens, Y.; Milan, S.J.; Smyth, R.M.; Dowswell, T. Telephone Support for Women during Pregnancy and the First Six Weeks Postpartum. Cochrane Database Syst. Rev. 2013, Cd009338. [Google Scholar] [CrossRef]
- Mattocks, K.M.; Kuzdeba, J.; Baldor, R.; Casares, J.; Lombardini, L.; Gerber, M.R. Implementing and Evaluating a Telephone-Based Centralized Maternity Care Coordination Program for Pregnant Veterans in the Department of Veterans Affairs. Womens Health Issues Off. Publ. Jacobs Inst. Womens Health 2017, 27, 579–585. [Google Scholar] [CrossRef]
- De Wolff, M.G.; Johansen, M.; Ersbøll, A.S.; Rosthøj, S.; Brunsgaard, A.; Midtgaard, J.; Tabor, A.; Hegaard, H.K. Efficacy of a Midwife-Coordinated, Individualized, and Specialized Maternity Care Intervention (ChroPreg) in Addition to Standard Care in Pregnant Women with Chronic Disease: Protocol for a Parallel Randomized Controlled Trial. Trials 2019, 20, 291. [Google Scholar] [CrossRef] [Green Version]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 Statement: Updated Guidelines for Reporting Parallel Group Randomised Trials. Int. J. Surg. 2011, 9, 672–677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danish Health Authorities, I.J.S. (Ed.) Kronisk Sygdom. Patient, Sundhedsvæsen Og Samfund. Chronic Disease. Patient, Healthcare System and Society. Copenhagen: Danish Health and Medicines Authority; Danish Health Authorities: Copenhagen, Denmark, 2005. [Google Scholar]
- Chronic Condition Indicator (CCI) for ICD-10-CM (Beta Version). Available online: https://www.hcup-us.ahrq.gov/toolssoftware/chronic_icd10/chronic_icd10.jsp (accessed on 2 September 2020).
- Fødte og Fødsler (1997–). Available online: https://www.esundhed.dk/Registre/Det-medicinske-foedselsregister/Foedte-og-foedsler-1997-og-frem#tabpanel61119A72216248AC86DB508579760DED (accessed on 8 February 2021).
- Sundheds-og Ældreministeriet Sundhedsloven. Available online: https://www.retsinformation.dk/eli/lta/2019/903 (accessed on 21 April 2021).
- Rodriguez, C.; des Rivieres-Pigeon, C. A Literature Review on Integrated Perinatal Care. Int. J. Integr. Care 2007, 7, e28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bastos, M.H.; Furuta, M.; Small, R.; McKenzie-McHarg, K.; Bick, D. Debriefing Interventions for the Prevention of Psychological Trauma in Women Following Childbirth. Cochrane Database Syst. Rev. 2015, CD007194. [Google Scholar] [CrossRef] [PubMed]
- Plusquin, C.; Uvin, V.; Drakopoulos, P.; De Brucker, P.; Rosetti, J.; Francotte, J.; De Brucker, M. Reduction of Hospital Stay at Maternity Unit: An Evaluation of the Impact on Maternal and Neonatal Readmission. J. Obstet. Gynaecol. 2020, 40, 46–52. [Google Scholar] [CrossRef]
- Campbell, O.M.; Cegolon, L.; Macleod, D.; Benova, L. Length of Stay After Childbirth in 92 Countries and Associated Factors in 30 Low- and Middle-Income Countries: Compilation of Reported Data and a Cross-Sectional Analysis from Nationally Representative Surveys. PLoS Med. 2016, 13, e1001972. [Google Scholar] [CrossRef] [Green Version]
- Topp, C.W.; Ostergaard, S.D.; Sondergaard, S.; Bech, P. The WHO-5 Well-Being Index: A Systematic Review of the Literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef]
- Smith-Nielsen, J.; Matthey, S.; Lange, T.; Væver, M.S. Validation of the Edinburgh Postnatal Depression Scale against Both DSM-5 and ICD-10 Diagnostic Criteria for Depression. BMC Psychiatry 2018, 18, 393. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, J.M.; Kafetsios, K.; Statham, H.E.; Snowdon, C.M. Factor Structure, Validity and Reliability of the Cambridge Worry Scale in a Pregnant Population. J. Health Psychol. 2003, 8, 753–764. [Google Scholar] [CrossRef] [PubMed]
- Loosman, W.L.; Hoekstra, T.; van Dijk, S.; Terwee, C.B.; Honig, A.; Siegert, C.E.; Dekker, F.W. Short-Form 12 or Short-Form 36 to Measure Quality-of-Life Changes in Dialysis Patients? Nephrol. Dial. Transpl. 2015, 30, 1170–1176. [Google Scholar] [CrossRef] [Green Version]
- Truijens, S.E.; Pommer, A.M.; van Runnard Heimel, P.J.; Verhoeven, C.J.; Oei, S.G.; Pop, V.J. Development of the Pregnancy and Childbirth Questionnaire (PCQ): Evaluating Quality of Care as Perceived by Women Who Recently Gave Birth. Eur. J. Obstet. Gynecol. Reprod. Biol. 2014, 174, 35–40. [Google Scholar] [CrossRef]
- Coffman, C.J.; Edelman, D.; Woolson, R.F. To Condition or Not Condition? Analysing “change” in Longitudinal Randomised Controlled Trials. BMJ Open 2016, 6, e013096. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO Announces COVID-19 Outbreak a Pandemic. Available online: https://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/news/news/2020/3/who-announces-covid-19-outbreak-a-pandemic (accessed on 23 March 2021).
- Press Conference about COVID-19 11 March 2020 [In Danish]. Available online: https://www.stm.dk/presse/pressemoedearkiv/pressemoede-om-covid-19-den-11-marts-2020/ (accessed on 23 March 2021).
- OECD Statistics. Available online: https://stats.oecd.org/ (accessed on 28 January 2021).
- Statistikbanken. Available online: https://www.statistikbanken.dk/IND04 (accessed on 1 February 2021).
- Van Otterloo, L.; Connelly, C.; Gould, J.; Abreo, A.; Main, E. Mothers at Risk: Factors Affecting Maternal Postpartum Length of Stay. J. Perinat. Neonatal Nurs. 2018, 32, 303–314. [Google Scholar] [CrossRef] [PubMed]
- Bendix, J.; Hegaard, H.K.; Langhoff-Roos, J.; Bergholt, T. Changing Prevalence and the Risk Factors for Antenatal Obstetric Hospitalizations in Denmark 2003-2012. Clin. Epidemiol. 2016, 8, 165–175. [Google Scholar] [CrossRef] [Green Version]
- Goodwin, L.; Taylor, B.; Kokab, F.; Kenyon, S. Postnatal Care in the Context of Decreasing Length of Stay in Hospital after Birth: The Perspectives of Community Midwives. Midwifery 2018, 60, 36–40. [Google Scholar] [CrossRef]
- Department of Obstetrics, Rigshospitalet—Copenhagen University Hospital (In Danish) Clinical Guideline for Early Postpartum Discharge, Rigshospitalet-Copenhagen University Hospital. Available online: https://vip.regionh.dk/VIP/Admin/GUI.nsf/Desktop.html?open&openlink=http://vip.regionh.dk/VIP/Slutbruger/Portal.nsf/Main.html?open&unid=XF625AC1D656571B7C125791500783DCF&level=1301XJ&dbpath=/VIP/Redaktoer/1301XJ.nsf/&windowwidth=1100&windowheight=600&windowtitle=S%F8g (accessed on 8 March 2021).
- Floris, L.; Irion, O.; Bonnet, J.; Politis Mercier, M.-P.; de Labrusse, C. Comprehensive Maternity Support and Shared Care in Switzerland: Comparison of Levels of Satisfaction. Women Birth J. Aust. Coll. Midwives 2018, 31, 124–133. [Google Scholar] [CrossRef]
- Turienzo, C.F.; Silverio, S.A.; Coxon, K.; Brigante, L.; Seed, P.T.; Shennan, A.H.; Sandall, J.; On behalf of the POPPIE Collaborative Group. Experiences of Maternity Care among Women at Increased Risk of Preterm Birth Receiving Midwifery Continuity of Care Compared to Women Receiving Standard Care: Results from the POPPIE Pilot Trial. PLoS ONE 2021, 16, e0248588. [Google Scholar] [CrossRef]
- World Health Organization (Ed.) WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience; World Health Organization: Geneva, Switzerland, 2016; ISBN 978-92-4-154991-2. [Google Scholar]
- Perriman, N.; Davis, D.L.; Ferguson, S. What Women Value in the Midwifery Continuity of Care Model: A Systematic Review with Meta-Synthesis. Midwifery 2018, 62, 220–229. [Google Scholar] [CrossRef] [PubMed]
- Doyle, C.; Lennox, L.; Bell, D. A Systematic Review of Evidence on the Links between Patient Experience and Clinical Safety and Effectiveness. BMJ Open 2013, 3, e001570. [Google Scholar] [CrossRef] [PubMed]
- Macpherson, I. A Systematic Review of the Relationship Factor between Women and Health Professionals within the Multivariant Analysis of Maternal Satisfaction. Midwifery 2016, 41, 68–78. [Google Scholar] [CrossRef]
- Fernandez Turienzo, C.; Bick, D.; Briley, A.L.; Bollard, M.; Coxon, K.; Cross, P.; Silverio, S.A.; Singh, C.; Seed, P.T.; Tribe, R.M.; et al. Midwifery Continuity of Care versus Standard Maternity Care for Women at Increased Risk of Preterm Birth: A Hybrid Implementation-Effectiveness, Randomised Controlled Pilot Trial in the UK. PLoS Med. 2020, 17, e1003350. [Google Scholar] [CrossRef]
- Dharni, N.; Essex, H.; Bryant, M.J.; Cronin de Chavez, A.; Willan, K.; Farrar, D.; Bywater, T.; Dickerson, J.; on behalf of the Better Start Bradford Innovation Hub. The Key Components of a Successful Model of Midwifery-Led Continuity of Carer, without Continuity at Birth: Findings from a Qualitative Implementation Evaluation. BMC Pregnancy Childbirth 2021, 21, 205. [Google Scholar] [CrossRef] [PubMed]
- Mercieca-Bebber, R.; King, M.T.; Calvert, M.J.; Stockler, M.R.; Friedlander, M. The Importance of Patient-Reported Outcomes in Clinical Trials and Strategies for Future Optimization. Patient Relat. Outcome Meas. 2018, 9, 353–367. [Google Scholar] [CrossRef] [Green Version]
- Nilver, H.; Begley, C.; Berg, M. Measuring Women’s Childbirth Experiences: A Systematic Review for Identification and Analysis of Validated Instruments. BMC Pregnancy Childbirth 2017, 17, 203. [Google Scholar] [CrossRef] [PubMed]
- Knight, M.; Bunch, K.; Tuffnell, D.; Shakespeare, J.; Kotnis, R.; Kenyon, S.; Kurinczuk, J.J.; on behalf of MBRRACE-UK (Eds.) Saving Lives, Improving Mothers’ Care-Lessons Learned to Inform Maternity Care from the UK and Ireland Confidential Enquiries into Maternal Deaths and Morbidity 2016-18; National Perinatal Epidemiology Unit, University of Oxford: Oxford, UK, 2020. [Google Scholar]
- Altman, M.R.; Murphy, S.M.; Fitzgerald, C.E.; Andersen, H.F.; Daratha, K.B. The Cost of Nurse-Midwifery Care: Use of Interventions, Resources, and Associated Costs in the Hospital Setting. Womens Health Issues Off. Publ. Jacobs Inst. Womens Health 2017, 27, 434–440. [Google Scholar] [CrossRef]
- Donnellan-Fernandez, R.E.; Creedy, D.K.; Callander, E.J. Cost-Effectiveness of Continuity of Midwifery Care for Women with Complex Pregnancy: A Structured Review of the Literature. Health Econ. Rev. 2018, 8. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| ChroPreg Group (n = 130) | Standard Care Group (n = 128) | |
|---|---|---|
| n (%) | n (%) | |
| Maternal Age (years) | ||
| <25 | 2 (1.5) | 4 (3.1) |
| 25–29 | 25 (19.2) | 32 (25.0) |
| 30–34 | 64 (49.2) | 48 (37.5) |
| 35–39 | 29 (22.3) | 32 (25.0) |
| ≥40 | 10 (7.7) | 12 (9.4) |
| Mean (SD) | 33.2 (4.2) | 33.2 (4.9) |
| Parity | ||
| Nulliparous | 66 (50.8) | 76 (59.4) |
| Multiparous | 64 (49.2) | 52 (40.6) |
| Mode of conception | ||
| Spontaneous | 106 (81.5) | 104 (81.2) |
| ART | 24 (18.5) | 24 (18.8) |
| Smoking before pregnancy | ||
| Yes | 16 (12.3) | 15 (11.7) |
| No | 114 (87.7) | 113 (88.3) |
| Smoking now | ||
| Yes | 3 (2.3) | 0 (0.0) |
| No | 127 (97.7) | 128 (100) |
| Cohabitation | ||
| Yes | 124 (95.4) | 118 (92.2) |
| No | 6 (4.6) | 10 (7.8) |
| Body Mass Index (kg/m2) | ||
| <18.5 | 5 (3.8) | 8 (6.3) |
| 18.5–24.9 | 95 (73.1) | 95 (74.2) |
| 25–29.9 | 16 (12.3) | 17 (13.3) |
| ≥30 | 14 (10.8) | 8 (6.3) |
| Mean (SD) | 23.9 (4.7) | 22.7 (3.9) |
| Education | ||
| Compulsory | 9 (6.9) | 8 (6.3) |
| Skilled | 4 (3.1) | 5 (3.9) |
| Tertiary education (1–2 years) | 9 (6.9) | 8 (6.3) |
| Bachelor or equivalent (3–4 years) | 36 (27.7) | 43 (33.5) |
| Master or equivalent | 72 (55.4) | 64 (50.0) |
| Occupation | ||
| Employed | 101 (77.7) | 103 (80.5) |
| Unemployed | 6 (4.6) | 8 (6.3) |
| Student | 15 (11.5) | 12 (9.4) |
| Other * | 8 (6.2) | 5 (3.9) |
| Medication before pregnancy | ||
| No medication | 29 (22.3) | 25 (19.5) |
| 1–2 medications | 68 (52.3) | 76 (59.4) |
| 3–5 medications | 33 (25.4) | 27 (21.1) |
| Current medication | ||
| No medication | 43 (33.1) | 40 (31.3) |
| 1–2 medications | 64 (49.2) | 63 (49.2) |
| 3–5 medications | 23 (17.7) | 25 (19.5) |
| Degree of pregnancy planning | ||
| Highly planned | 70 (53.8) | 71 (55.5) |
| Fairly planned | 24 (18.5) | 24 (18.8) |
| Neither planned nor unplanned | 22 (16.9) | 25 (19.5) |
| Fairly unplanned | 6 (4.6) | 4 (3.1) |
| Highly unplanned | 8 (6.2) | 4 (3.1) |
| Number of CMCs | ||
| One | 99 (76.2) | 92 (71.9) |
| Two | 20 (15.4) | 29 (22.7) |
| Three | 10 (7.7) | 6 (4.7) |
| Four | 1 (0.8) | 1 (0.8) |
| Types of CMC: | ||
| Endocrinological disease a | 34 (19.7) | 32 (18.6) |
| Neurological disease b | 41 (23.7) | 34 (19.8) |
| Rheumatological disease c | 30 (17.3) | 36 (20.9) |
| Hematological disease d | 10 (5.8) | 15 (8.7) |
| Bowel disease e | 25 (14.4) | 18 (10.5) |
| Hypertension | 9 (5.2) | 8 (4.7) |
| Lung disease f | 8 (4.6) | 8 (4.7) |
| Kidney disease | 3 (1.7) | 7 (4.1) |
| Liver disease | 1 (0.6) | 1 (0.6) |
| Psychiatric disease | 1 (0.6) | 1 (0.6) |
| Endometriosis | 2 (1.2) | 5 (2.9) |
| Other CMCs ** | 9 (5.2) | 7 (4.1) |
| Component in Intervention | |
|---|---|
| Antenatal midwife consultations (median/range) | 6 (2–10) |
| Postpartum follow-up by telephone (n/%) * | 117 (90) |
| Postpartum debriefing session (n/%) * | 110 (85) |
| E-mail consultation ** (n/%) | 43 (33) |
| Weekly telephone hours ** (n/%) | 35 (27) |
| Allocation | n | Median | IQR | Range | LOS ≤ 3 Days |
|---|---|---|---|---|---|
| n (%) | |||||
| ChroPreg group | 130 | 3 | 2–4.75 | 1–35 | 84 (65) |
| Standard Care group | 128 | 3 | 2–4.0 | 1–23 | 75 (59) |
| ChroPreg Group | Standard Care Group | |||||
|---|---|---|---|---|---|---|
| WHO Five-Item Well-Being Index | n | Mean | Mean | Mean Difference | 95% CI | p-Value |
| Total scale score 33–37 weeks | 250 | 57.6 | 58.3 | −0.7 | −4.2–2.8 | 0.70 |
| (missing CPG = 4, SCG = 4) | ||||||
| Total scale score Two months postpartum | 240 | 67.5 | 65.5 | 2.0 | −1.6–5.6 | 0.27 |
| (missing CPG = 8, SCG = 10) | ||||||
| Edinburgh Postnatal Depression Scale (EPDS) | n | n (%) | n (%) | p-Value | ||
| EPDS ≥ 10 33–37 weeks | 249 | 27 (21) | 21 (17) | 0.38 | ||
| (missing = 4, SCG = 5) | ||||||
| EPDS ≥ 10 Two months postpartum | 239 | 25 (21) | 19 (16) | 0.36 | ||
| (missing = IG = 9, SCG = 10) | ||||||
| Cambridge Worry Scale | n | Mean | Mean | Mean Difference | 95% CI | p-Value |
| Total scale score 33–37 weeks | 250 | 16.5 | 15.52 | 1.0 | −0.8–2.8 | 0.27 |
| (missing CPG = 4, SCG = 4) | ||||||
| SF-12 | n | Mean | Mean | Mean Difference | 95% CI | p-Value |
| Physical Component Summary week 33–37 | 250 | 38.9 | 40.2 | −1.3 | −3.5–0.8 | 0.23 |
| (missing = CPG = 4, SCG = 4) | ||||||
| Physical Component Summary Two months postpartum | 242 | 49.3 | 47.7 | −0.5 | −2.7–1.7 | 0.66 |
| (missing = CPG = 7, SCG = 9) | ||||||
| Mental component summary week 33–37 | 250 | 51.1 | 51.4 | −0.3 | −2.4–1.8 | 0.76 |
| (missing = CPG = 4, SCG = 4) | ||||||
| Mental component summary Two months postpartum | 242 | 49.1 | 49.7 | −0.6 | −2.8–1.5 | 0.55 |
| (missing = CPG = 7, SCG = 9) | ||||||
| Pregnancy and Childbirth Questionnaire | n | Mean | Mean | Mean Difference | 95% CI | p-Value |
| Total scale score 8 weeks postpartum | 241 | 104.5 | 98.2 | 6.3 | 3.0–10.0 | 0.001 |
| (missing CPG = 8, SCG = 9) | ||||||
| Pregnancy subscale—Personal treatment Two months postpartum | 241 | 48.8 | 45.5 | 3.3 | 2.0–5.0 | <0.0001 |
| (missing CPG = 8, SCG = 9) | ||||||
| Pregnancy subscale—Information and education Two months postpartum (missing CPG = 8, SCG = 9) | 241 | 25.8 | 23.8 | 2.0 | 1.0–3.0 | 0.003 |
| Delivery subscale–Personal treatment Two months postpartum (missing CPG = 8, SCG = 11) | 239 | 29.9 | 29.4 | 0.5 | −1.0–2.0 | 0.51 |
| ChroPreg Group | Standard Care Group | ||||
|---|---|---|---|---|---|
| n | % | n | % | p-Value | |
| Pregnancy complications a | 19 | 15 | 20 | 16 | 0.82 |
| Antenatal outpatient telemonitoring | 3 | 2 | 4 | 3 | 0.72 ** |
| Intention to breastfeed (yes) (Assessed 33–37 weeks) | 121 | 96 | 118 | 95 | 0.73 |
| Labor onset b | 0.60 | ||||
| Spontaneous | 67 | 60 | 58 | 56 | |
| Induced | 45 | 40 | 45 | 44 | |
| Mode of birth | |||||
| Vaginal | 98 | 75 | 84 | 66 | 0.10 * |
| Cesarean section | 32 | 25 | 44 | 34 | |
| Preterm delivery | 11 | 8 | 8 | 6 | 0.60 |
| Use of epidural analgesia | 52 | 40 | 44 | 34.4 | 0.35 |
| Apgar Score ≤ 7 at 5 min | 1 | 1 | 1 | 1 | N/A |
| Breastfeeding (yes) (Assessed 8 weeks postpartum) | 106 | 87 | 98 | 83 | 0.41 |
| Median | IQR | Median | IQR | p-Value * | |
| Gestational age at birth (days) | 276 | 269–284 | 278 | 268–283 | 0.84 |
| Birth weight (kilograms) | 3.3 | 3.1–3.8 | 3.4 | 3.0–3.7 | 0.35 |
| Intended length of breastfeeding (months) | 9 | 6–12 | 8 | 6–12 | 0.16 |
| (Assessed eight weeks postpartum) | |||||
| ChroPreg Group | Standard Care Group | ||||
|---|---|---|---|---|---|
| Median | IQR | Median | IQR | p-Value * | |
| Number of planned visits with a midwife Antenatally | 6 | 5–7 | 4 | 3.25–5 | <0.0001 |
| Number of planned visits with an obstetrician Antenatally | 3 | 1.25–4 | 3 | 2–5 | 0.21 |
| Total number of planned visits with midwife or obstetrician whole study period ** | 11 | 9–13 | 9 | 8–12 | 0.0004 |
| Total number of unscheduled visits whole study period | 1 | 0–2 | 1 | 0–2 | 0.63 |
| Total number of planned telephone consultations whole study period | 4 | 3–5 | 2 | 1–4 | <0.0001 |
| Total number of unscheduled telephone consultation whole study period | 2 | 1–3 | 2 | 1–3 | 0.69 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Wolff, M.G.; Midtgaard, J.; Johansen, M.; Rom, A.L.; Rosthøj, S.; Tabor, A.; Hegaard, H.K. Effects of a Midwife-Coordinated Maternity Care Intervention (ChroPreg) vs. Standard Care in Pregnant Women with Chronic Medical Conditions: Results from a Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 7875. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18157875
de Wolff MG, Midtgaard J, Johansen M, Rom AL, Rosthøj S, Tabor A, Hegaard HK. Effects of a Midwife-Coordinated Maternity Care Intervention (ChroPreg) vs. Standard Care in Pregnant Women with Chronic Medical Conditions: Results from a Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2021; 18(15):7875. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18157875
Chicago/Turabian Stylede Wolff, Mie G., Julie Midtgaard, Marianne Johansen, Ane L. Rom, Susanne Rosthøj, Ann Tabor, and Hanne K. Hegaard. 2021. "Effects of a Midwife-Coordinated Maternity Care Intervention (ChroPreg) vs. Standard Care in Pregnant Women with Chronic Medical Conditions: Results from a Randomized Controlled Trial" International Journal of Environmental Research and Public Health 18, no. 15: 7875. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18157875