
Effects of Functional Fitness Enhancement through Taekwondo Training on Physical Characteristics and Risk Factors of Dementia in Elderly Women with Depression †


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Methods
2.2.1. Physical Examination
2.2.2. Functional Fitness
2.2.3. Geriatric Depression Scale-Korea
2.2.4. Korean Dementia Screening Questionnaire
2.2.5. Taekwondo Training Program
2.3. Blood Sample Analysis
2.4. Statistical Analysis
3. Results
3.1. Functional Fitness
3.2. Physical Characteristics
3.3. Dementia Risk Factors
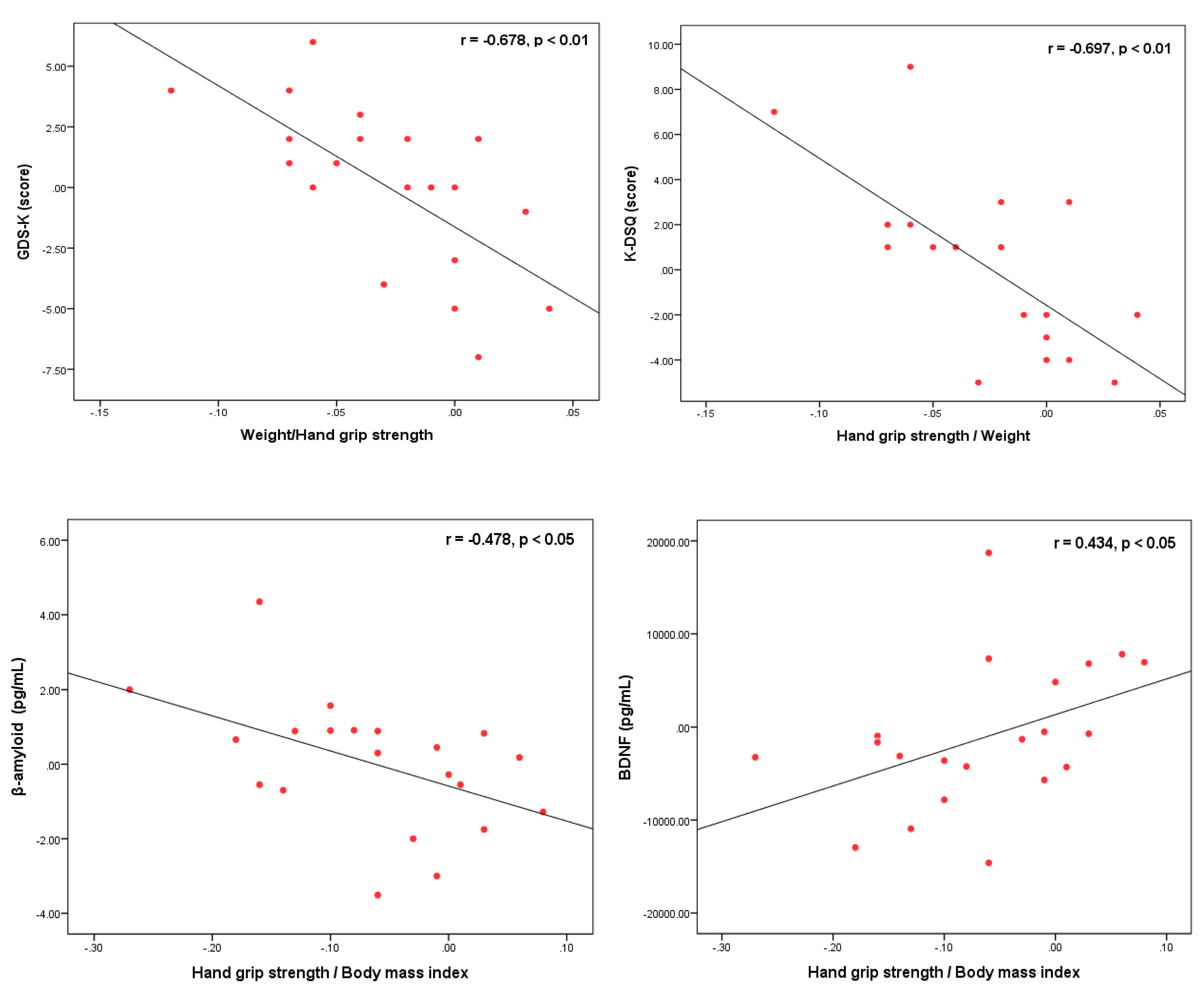
3.4. Correlations among Hand Grip Strength/Weight, Depression and Dementia Risk Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Statistics Korea. Survey on Dementia Prevalence; Nationwide Study on the Prevalence of Dementia in Korean Elders 2017; Ministry of Health & Welfare: Sejong, Korea, 2017.
- Lee, D.W.; Seong, S.J. The national dementia plan: From the 1st to the 3rd. J. Korean Med. Assoc. 2018, 61, 298–303. [Google Scholar] [CrossRef]
- Kerpershoek, L.; De Vugt, M.; Wolfs, C.; Woods, B.; Jelley, H.; Orrell, M.; Stephan, A.; Bieber, A.; Meyer, G.; Selbaek, G.; et al. Needs and quality of life of people with middle-stage dementia and their family carers from the European Actifcare study. When informal care alone may not suffice. Aging Ment. Health 2017, 22, 897–902. [Google Scholar] [CrossRef] [PubMed]
- Duncombe, J.; Kitamura, A.; Hase, Y.; Ihara, M.; Kalaria, R.N.; Horsburgh, K. Chronic cerebral hypoperfusion: A key mechanism leading to vascular cognitive impairment and dementia. Closing the translational gap between rodent models and human vascular cognitive impairment and dementia. Clin. Sci. 2017, 131, 2451–2468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stephen, R.; Hongisto, K.; Solomon, A.; Lönnroos, E. Physical Activity and Alzheimer’s Disease: A Systematic Review. Journals Gerontol. Ser. A Boil. Sci. Med. Sci. 2017, 72, 733–739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guitar, N.A.; Connelly, D.M.; Nagamatsu, L.S.; Orange, J.B.; Muir-Hunter, S.W. The effects of physical exercise on executive function in community-dwelling older adults living with Alzheimer’s-type dementia: A systematic review. Ageing Res. Rev. 2018, 47, 159–167. [Google Scholar] [CrossRef]
- Selkoe, D.J.; Hardy, J. The amyloid hypothesis of Alzheimer’s disease at 25 years. EMBO Mol. Med. 2016, 8, 595–608. [Google Scholar] [CrossRef]
- Bostrom, P.; Wu, J.; Jedrychowski, M.P.; Korde, A.; Ye, L.; Lo, J.C.; Kajimura, S. A PGC1-α-dependent myokine that drives brown-fat-like development of white fat and thermogenesis. Nature 2012, 481, 463. [Google Scholar] [CrossRef]
- Jin, Y.; Sumsuzzman, D.M.; Choi, J.; Kang, H.; Lee, S.R.; Hong, Y. Molecular and Functional Interaction of the Myokine Irisin with Physical Exercise and Alzheimer’s Disease. Molecules 2018, 23, 3229. [Google Scholar] [CrossRef] [Green Version]
- Scheper, V.; Schwieger, J.; Hamm, A.; Lenarz, T.; Hoffmann, A. BDNF—Overexpressing human mesenchymal stem cells mediate increased neuronal protection in vitro. J. Neurosci. Res. 2019, 97, 1414–1429. [Google Scholar] [CrossRef]
- Rikli, R.E.; Jones, C.J. Development and validation of criterion-referenced clinically relevant fitness standards for maintaining physical independence in later years. Gerontologist 2013, 53, 255–267. [Google Scholar] [CrossRef]
- Lawman, H.G.; Troiano, R.; Perna, F.M.; Wang, C.-Y.; Fryar, C.D.; Ogden, C.L. Associations of Relative Handgrip Strength and Cardiovascular Disease Biomarkers in U.S. Adults, 2011–2012. Am. J. Prev. Med. 2016, 50, 677–683. [Google Scholar] [CrossRef] [PubMed]
- Rolland, Y.; Lauwers-Cances, V.; Pahor, M.; Fillaux, J.; Grandjean, H.; Vellas, B. Muscle strength in obese elderly women: Effect of recreational physical activity in a cross-sectional study. Am. J. Clin. Nutr. 2004, 79, 552–557. [Google Scholar] [CrossRef] [Green Version]
- Cetinus, E.; Buyukbese, M.A.; Üzel, M.; Ekerbicer, H.; Karaoguz, A. Hand grip strength in patients with type 2 diabetes mellitus. Diabetes Res. Clin. Pract. 2005, 70, 278–286. [Google Scholar] [CrossRef] [PubMed]
- Kuh, D.; Bassey, E.J.; Butterworth, S.; Hardy, R.; Wadsworth, M.E.J.; The Musculoskeletal Study Team. Grip Strength, Postural Control, and Functional Leg Power in a Representative Cohort of British Men and Women: Associations With Physical Activity, Health Status, and Socioeconomic Conditions. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2005, 60, 224–231. [Google Scholar] [CrossRef] [Green Version]
- Sayer, A.A.; Syddall, H.; Dennison, E.; Martin, H.; Phillips, D.; Cooper, C.; Byrne, C.D. Grip strength and the metabolic syndrome: Findings from the Hertfordshire Cohort Study. QJM Int. J. Med. 2007, 100, 707–713. [Google Scholar] [CrossRef] [Green Version]
- Ruiz, J.R.; Sui, X.; Lobelo, F.; Morrow, J.R.; Jackson, A.W.; Sjöström, M.; Blair, S.N. Association between muscular strength and mortality in men: Prospective cohort study. BMJ 2008, 337, a439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Izawa, K.P.; Watanabe, S.; Osada, N.; Kasahara, Y.; Yokoyama, H.; Hiraki, K.; Omiya, K. Handgrip strength as a predictor of prognosis in Japanese patients with congestive heart failure. Eur. J. Cardiov. Prev. R. 2009, 16, 21–27. [Google Scholar] [CrossRef]
- Norman, K.; Stobäus, N.; Gonzalez, M.C.; Schulzke, J.-D.; Pirlich, M. Hand grip strength: Outcome predictor and marker of nutritional status. Clin. Nutr. 2011, 30, 135–142. [Google Scholar] [CrossRef]
- Almeida, O.P.; Hankey, G.; Yeap, B.B.; Golledge, J.; Flicker, L. Depression as a modifiable factor to decrease the risk of dementia. Transl. Psychiatry 2017, 7, e1117. [Google Scholar] [CrossRef] [Green Version]
- Valkanova, V.; Ebmeier, K.P.; Allan, C. Depression is linked to dementia in older adults. Practitioner 2017, 261, 11–15. [Google Scholar] [PubMed]
- Dudas, R.; Malouf, R.; Mccleery, J.; Dening, T. Antidepressants for treating depression in dementia. Cochrane Database Syst. Rev. 2018, 8, CD003944. [Google Scholar] [CrossRef]
- Loprinzi, P.D.; Blough, J.; Ryu, S.; Kang, M. Experimental effects of exercise on memory function among mild cognitive impairment: Systematic review and meta-analysis. Physician Sportsmed. 2018, 47, 21–26. [Google Scholar] [CrossRef]
- Nascimento, C.M.C.; Pereira, J.R.; De Andrade, L.P.; Garuffi, M.; Ayan, C.; Kerr, D.S.; Talib, L.L.; Cominetti, M.R.; Stella, F. Physical Exercise Improves Peripheral BDNF Levels and Cognitive Functions in Mild Cognitive Impairment Elderly with Different BDNF Val66Met Genotypes. J. Alzheimer’s Dis. 2014, 43, 81–91. [Google Scholar] [CrossRef]
- Baek, S.H. The Effect of Taekwondo and Cognitive Task Program on Muscular Dystrophy and Dementia Risk Factors in Elderly Women. Ph.D. Thesis, Dong-A University Graduate School, Busan, Korea, 2020. [Google Scholar]
- Lee, Y.C. A study of the relationship between depression symptom and physical performance in elderly women. J. Exerc. Rehabil. 2015, 11, 367–371. [Google Scholar] [CrossRef]
- Damirchi, A.; Hosseini, F.; Babaei, P. Mental Training Enhances Cognitive Function and BDNF More Than Either Physical or Combined Training in Elderly Women With MCI: A Small-Scale Study. Am. J. Alzheimer’s Dis. Other Dementiasr 2017, 33, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H. The Effect of Taekwondo Training on CT-Based Thigh Muscle Area and Insulin Resistance in Diabetes Elderly Women. Ph.D. Thesis, Dong-A University Graduate School, Busan, Korea, 2020. [Google Scholar]
- Lee, S.H.; Scott, S.D.; Pekas, E.J.; Lee, S.; Lee, S.H.; Park, S.Y. Taekwondo training reduces blood catecholamine levels and arterial stiffness in postmenopausal women with stage-2 hypertension: Randomized clinical trial. Clin. Exp. Hypertens. 2019, 41, 675–681. [Google Scholar] [CrossRef]
- Korea Sports Promotion Foundation. Development of National Fitness Evaluation Criteria for the Elderly. 2011. Available online: http://nfa.kspo.or.kr/ (accessed on 27 July 2021).
- Jung, I.K.; Kwak, D.I.; Cho, S.H.; Lee, H.S. A preliminary study on standardization of Korean form of geriatric depression Scale (KGDS). J. Korean Neuropsychiatr. Assoc. 1998, 37, 340–351. [Google Scholar]
- Yesavage, J.A.; Brink, T.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.; Leirer, V.O. Development and validation of a geriatric depression screening scale: A preliminary report. J. Psychiatr. Res. 1983, 17, 37–49. [Google Scholar] [CrossRef]
- Yang, D.W.; Chey, J.Y.; Kim, S.Y.; Kim, B.S. The development and validation of Korean dementia screening questionnaire (KDSQ). J. Korean Neurol. Assoc. 2002, 20, 135–141. [Google Scholar]
- Kukkiwon. Taekwondo Technical Glossary. 2010. Available online: www.kukkiwon.or.kr (accessed on 27 July 2021).
- Borg, G. Borg’s Perceived Exertion and Pain Scales. Human Kinetics. 1998. Available online: https://psycnet.apa.org/record/1998-07179-000 (accessed on 27 July 2021).
- McGrath, R.P.; Kraemer, W.J.; Al Snih, S.; Peterson, M. Handgrip Strength and Health in Aging Adults. Sports Med. 2018, 48, 1993–2000. [Google Scholar] [CrossRef]
- Oxley, J.; O’Hern, S.; Burtt, D.; Rossiter, B. Falling while walking: A hidden contributor to pedestrian injury. Accid. Anal. Prev. 2018, 114, 77–82. [Google Scholar] [CrossRef]
- Kim, Y.H.; Jeong, M.K.; Park, H.; Park, S.K. Effects of Regular Taekwondo Intervention on Health-Related Physical Fitness, Cardiovascular Disease Risk Factors and Epicardial Adipose Tissue in Elderly Women with Hypertension. Int. J. Environ. Res. Public Health 2021, 18, 2935. [Google Scholar] [CrossRef] [PubMed]
- Bridge, C.A.; da Silva Santos, J.F.; Chaabene, H.; Pieter, W.; Franchini, E. Physical and physiological profiles of taekwondo athletes. Sports Med. 2014, 44, 713–733. [Google Scholar] [CrossRef]
- Toskovic, N.N.; Blessing, D.; Williford, H.N. Physiologic profile of recreational male and female novice and experienced Tae Kwon Do practitioners. J. Sports Med. Phys. Fit. 2004, 44, 164. [Google Scholar]
- Kim, J.-H. Association between body mass index and cognition function and all-cause mortality in Korean elderly people. Obes. Med. 2020, 17, 100174. [Google Scholar] [CrossRef]
- Ishii, H.; Makizako, H.; Doi, T.; Tsutsumimoto, K.; Shimada, H. Associations of Skeletal Muscle Mass, Lower-Extremity Functioning, and Cognitive Impairment in Community-Dwelling Older People in Japan. J. Nutr. Health Aging 2018, 23, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.-J.; Wu, G.-H.; Yang, Y.-L.; Wu, Y.-H.; Zhang, L.; Wang, M.-H.; Mo, L.-Y.; Xue, G.; Wang, C.-Z.; Weng, X.-F. Nutrition, Physical Exercise, and the Prevalence of Sarcopenia in Elderly Residents in Nursing Homes in China. Med. Sci. Monit. 2019, 25, 4390–4399. [Google Scholar] [CrossRef]
- Brudnak, M.A.; Dundero, D.; Van Hecke, F.M. Are thehard’martial arts, such as the Korean martial art, TaeKwon-Do, of benefit to senior citizens? Med. Hypotheses 2002, 59, 485–491. [Google Scholar] [CrossRef]
- Bartels, C.; Wagner, M.; Wolfsgruber, S.; Ehrenreich, H.; Schneider, A. Alzheimer’s Disease Neuroimaging Initiative. Impact of SSRI therapy on risk of conversion from mild cognitive impairment to Alzheimer’s dementia in individuals with previous depression. Am. J. Psychiatry 2018, 175, 232–241. [Google Scholar] [CrossRef]
- Erickson, K.I.; Miller, D.L.; Roecklein, K.A. The aging hippocampus: Interactions between exercise, depression, and BDNF. Neuroscientist 2012, 18, 82–97. [Google Scholar] [CrossRef]
- Nigam, S.M.; Xu, S.; Kritikou, J.S.; Marosi, K.; Brodin, L.; Mattson, M.P. Exercise and BDNF reduce Aβ production by enhancing α—Secretase processing of APP. J. Neurochem. 2017, 142, 286–296. [Google Scholar] [CrossRef] [PubMed]
- Jørgensen, M.L.K.; Kjølhede, T.; Dalgas, U.; Hvid, L.G. Plasma brain-derived neurotrophic factor (BDNF) and sphingosine-1-phosphat (S1P) are NOT the main mediators of neuroprotection induced by resistance training in persons with multiple sclerosis—A randomized controlled trial. Mult. Scler. Relat. Disorders 2019, 31, 106–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marinus, N.; Hansen, D.; Feys, P.; Meesen, R.; Timmermans, A.; Spildooren, J. The impact of different types of exercise training on peripheral blood brain-derived neurotrophic factor concentrations in older adults: A meta-analysis. Sports Med. 2019, 49, 1529–1546. [Google Scholar] [CrossRef] [PubMed]
- Zsuga, J.; Tajti, G.; Papp, C.; Juhasz, B.; Gesztelyi, R. FNDC5/irisin, a molecular target for boosting reward-related learning and motivation. Med. Hypotheses 2016, 90, 23–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tofighi, A.; Alizadeh, R.; Tolouei Azar, J. The effect of eight weeks high intensity interval raining (HIIT) on serum amounts of FGF21 and irisin in sedentary obese women. J. Urmia Univ. Med. Sci. 2017, 28, 453–466. [Google Scholar]
- Batitucci, G.; Brandao, C.F.C.; De Carvalho, F.G.; Marchini, J.S.; Pfrimer, K.; Ferrioli, E.; da Silva, A.S.R. Taurine supplementation increases irisin levels after high intensity physical training in obese women. Cytokine 2019, 123, 154741. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Taekwondo (n = 10) | Control (n = 10) | p-Value |
|---|---|---|---|
| Age (years) | 72.55 ± 5.45 | 72.40 ± 3.81 | 0.918 |
| Body height (m) | 1.50 ± 0.03 | 1.50 ± 0.05 | 0.645 |
| Body weight (kg) | 55.95 ± 4,94 | 54.12 ± 3.26 | 0.756 |
| Body mass index (kg/m2) | 24.72 ± 2.10 | 24.20 ± 1.98 | 0.809 |
| Percent fat (%) | 42.41 ± 3.78 | 42.17 ± 5.26 | 0.973 |
| Systolic blood pressure (mmHg) | 148.82 ± 9.93 | 148.20 ± 14.03 | 0.863 |
| Diastolic blood pressure (mmHg) | 86.91 ± 8.22 | 83.30 ± 8.72 | 0.349 |
| ASMI (kg/m2) | 5.34 ± 0.30 | 5.55 ± 0.14 | 0.051 |
| GDS-K (score) | 15.64 ± 1.75 | 16.00 ± 1.76 | 0.809 |
| K-DSQ (score) | 5.73 ± 2.87 | 5.90 ± 2.88 | 0.918 |
| Item | Contents | Time (min) |
|---|---|---|
| Warm-up exercises | Walking at the gym with pairs Memory recollecting and word chaining with pairs Stretching (sit down, spread legs lightly and bend down) | 10 |
| Taekwondo training program | 1∼6 week’s RPE 1; 10∼11 | 40 |
| Seogi—Juchumseogi, Apseogi, Apgubi, Dwitgubi, Moaseogi, Naranhiseogi, Hakdariseogi (10 min) Jireugi—Momtongjireugi, Ulgooljireugi, Naeryeojireugi, Yeopjireugi, Jeocheojireugi, Chetdarijireugi, Pyojeokjireugi (10 min) Makgi—Naeryeomakgi, Momtongmakgi, Ollyeomakgi, Momtonganmakgi, Momtongbakkanmakgi, Geumgangmakgi, Santeulmakgi (10 min) Chagi—Ap-chagi (Front, Dollyeo-chagi, Naeryeo-chag. Yeopchagi, Dwichagi, Dwidollyeochagi (10 min) | ||
| 7∼12 week’s RPE; 12∼13 | ||
| Seogi—Juchumseogi, Apseogi, Apgubi, Dwitgubi, Moaseogi, Naranhiseogi, Hakdariseogi (5 min) Jireugi—Momtongjireugi, Ulgooljireugi, Naeryeojireugi, Yeopjireugi, Jeocheojireugi, Chetdarijireugi, Pyojeokjireugi (5 min) Makgi—Naeryeomakgi, Momtongmakgi, Ollyeomakgi, Momtonganmakgi, Momtongbakkanmakgi, Geumgangmakgi, Santeulmakgi (5 min) Chagi—Ap-chagi (Front, Dollyeo-chagi, Naeryeo-chag. Yeopchagi, Dwichagi, Dwidollyeochagi (5 min) Taeguek 1 Jang (separated once, once without a verbal order) (10 min) Taekwon Aerobics (separation action once, once in tune with the music) (10 min) | ||
| Cool-down exercises | Walking at the gym with pairs Memory recollecting and word chaining with pairs Stretching (rolling shoulder and neck to lie down) | 10 |
| Variable | Group | Baseline | 12 Weeks | Source | p-Value |
|---|---|---|---|---|---|
| Hand grip strength (kg) | Taekwondo | 16.55 ± 1.40 | 19.09 ± 1.43 | Group | 0.227 |
| Time | 0.002 ** | ||||
| Control | 17.07 ± 1.49 | 16.97 ± 1.39 | Group × Time | 0.008 ** | |
| Hand grip strength/weight | Taekwondo | 0.30 ± 0.04 | 0.35 ± 0.04 | Group | 0.729 |
| Time | 0.000 *** | ||||
| Control | 0.32 ± 0.03 | 0.32 ± 0.03 | Group × Time | 0.006 ** | |
| 4-m gait speed (m/s) | Taekwondo | 0.75 ± 0.05 | 0.85 ± 0.06 | Group | 0.011 * |
| Time | 0.004 ** | ||||
| Control | 0.76 ± 0.03 | 0.73 ± 0.03 | Group × Time | 0.000 *** | |
| 3-m timed up and go (sec) | Taekwondo | 7.00 ± 0.47 | 6.46 ± 0.70 | Group | 0.250 |
| Time | 0.274 | ||||
| Control | 7.03 ± 1.09 | 7.23 ± 1.17 | Group × Time | 0.013 * | |
| Figure-of-eight track (sec) | Taekwondo | 31.08 ± 3.58 | 26.53 ± 1.95 | Group | 0.080 |
| Time | 0.003 ** | ||||
| Control | 31.96 ± 4.22 | 32.01 ± 4.01 | Group × Time | 0.011 * | |
| 30 s chair stand (frequency) | Taekwondo | 19.00 ± 3.85 | 20.64 ± 3.17 | Group | 0.871 |
| Time | 0.137 | ||||
| Control | 20.10 ± 4.93 | 20.22 ± 4.10 | Group × Time | 0.347 | |
| Sit-and-reach (cm) | Taekwondo | 11.82 ± 7.64 | 12.91 ± 6.73 | Group | 0.545 |
| Time | 0.658 | ||||
| Control | 9.05 ± 7.21 | 9.13 ± 6.77 | Group × Time | 0.066 |
| Variable | Group | Baseline | 12 Weeks | Source | p-Value |
|---|---|---|---|---|---|
| Body weight (kg) | Taekwondo | 55.95 ± 4.94 | 54.65 ± 4.38 | Group | 0.496 |
| Time | 0.068 | ||||
| Control | 54.12 ± 3.26 | 53.83 ± 2.77 | Group × Time | 0.212 | |
| Body mass index (kg/m2) | Taekwondo | 24.72 ± 2.10 | 24.14 ± 1.79 | Group | 0.073 |
| Time | 0.108 | ||||
| Control | 24.20 ± 1.98 | 24.08 ± 1.83 | Group × Time | 0.220 | |
| Percent fat (%) | Taekwondo | 42.41 ± 3.78 | 40.07 ± 3.69 | Group | 0.403 |
| Time | 0.012 * | ||||
| Control | 42.17 ± 5.26 | 43.46 ± 5.64 | Group × Time | 0.012 * | |
| ASMI (kg/m2) | Taekwondo | 5.34 ± 0.30 | 5.66 ± 0.40 | Group | 0.540 |
| Time | 0.863 | ||||
| Control | 5.55 ± 0.14 | 5.26 ± 0.46 | Group × Time | 0.003 ** | |
| Systolic blood pressure (mmHg) | Taekwondo | 148.82 ± 9.93 | 136.27 ± 8.04 | Group | 0.124 |
| Time | 0.092 | ||||
| Control | 148.20 ± 14.03 | 151.01 ± 12.40 | Group × Time | 0.007 ** | |
| Diastolic blood pressure (mmHg) | Taekwondo | 86.91 ± 8.22 | 76.27 ± 9.41 | Group | 0.607 |
| Time | 0.000 *** | ||||
| Control | 83.30 ± 8.72 | 83.54 ± 7.59 | Group × Time | 0.001 ** | |
| GDS-K (score) | Taekwondo | 15.64 ± 1.75 | 13.18 ± 2.14 | Group | 0.003 ** |
| Time | 0.689 | ||||
| Control | 16.00 ± 1.76 | 18.80 ± 2.10 | Group × Time | 0.000 *** | |
| Positive items (score) | Taekwondo | 8.73 ± 2.15 | 7.09 ± 2.59 | Group | 0.262 |
| Time | 0.814 | ||||
| Control | 8.20 ± 1.75 | 10.00 ± 1.94 | Group × Time | 0.020 * | |
| Negative (score) | Taekwondo | 6.91 ± 2.02 | 6.09 ± 2.47 | Group | 0.116 |
| Time | 0.945 | ||||
| Control | 7.80 ± 2.62 | 8.80 ± 2.15 | Group × Time | 0.184 |
| Variable | Group | Baseline | 12 Weeks | Source | p-Value |
|---|---|---|---|---|---|
| TC (mg/dL) | Taekwondo | 198.09 ± 26.44 | 165.00 ± 23.71 | Group | 0.070 |
| Time | 0.173 | ||||
| Control | 199.20 ± 37.29 | 216.44 ± 32.59 | Group × Time | 0.000 *** | |
| TG (mg/dL) | Taekwondo | 156.09 ± 25.01 | 108.91 ± 25.95 | Group | 0.033 |
| Time | 0.003 ** | ||||
| Control | 155.70 ± 19.52 | 156.57 ± 24.26 | Group × Time | 0.001 ** | |
| LDL-C (mg/dL) | Taekwondo | 127.09 ± 23.52 | 101.91 ± 15.66 | Group | 0.099 |
| Time | 0.067 | ||||
| Control | 127.77 ± 25.44 | 134.10 ± 19.33 | Group × Time | 0.001 ** | |
| HDL-C (mg/dL) | Taekwondo | 53.64 ± 9.48 | 60.91 ± 8.83 | Group | 0.467 |
| Time | 0.947 | ||||
| Control | 58.50 ± 16.83 | 48.79 ± 12.12 | Group × Time | 0.001 ** | |
| FFA (μEq/L) | Taekwondo | 644.91 ± 313.95 | 535.18 ± 257.62 | Group | 0.016 * |
| Time | 0.929 | ||||
| Control | 724.50 ± 295.14 | 852.82 ± 242.15 | Group × Time | 0.012 * | |
| Adiponectin (μg/mL) | Taekwondo | 7.85 ± 2.18 | 9.99 ± 2.21 | Group | 0.026 * |
| Time | 0.956 | ||||
| Control | 8.29 ± 2.24 | 6.10 ± 6.36 | Group × Time | 0.002 ** | |
| Arteriosclerosis index | Taekwondo | 2.79 ± 0.75 | 1.75 ± 0.46 | Group | 0.033 |
| Time | 0.862 | ||||
| Control | 2.66 ± 1.16 | 3.71 ± 1.57 | Group × Time | 0.001 ** | |
| K-DSQ (score) | Taekwondo | 5.73 ± 2.87 | 3.00 ± 1.67 | Group | 0.018 * |
| Time | 0.780 | ||||
| Control | 5.90 ± 2.88 | 8.50 ± 3.66 | Group × Time | 0.002 ** | |
| Irisin (μg/mL) | Taekwondo | 8.14 ± 1.17 | 7.55 ± 1.47 | Group | 0.898 |
| Time | 0.053 | ||||
| Control | 9.97 ± 3.82 | 7.20 ± 1.68 | Group × Time | 0.238 | |
| β-amyloid (pg/mL) | Taekwondo | 3.69 ± 2.08 | 2.63 ± 0.86 | Group | 0.258 |
| Time | 0.938 | ||||
| Control | 3.22 ± 0.85 | 4.36 ± 8.29 | Group × Time | 0.002 ** | |
| BDNF (pg/mL) | Taekwondo | 24,134.67 ± 3889.04 | 29,933.33 ± 2626.50 | Group | 0.039 |
| Time | 0.448 | ||||
| Control | 24,769.75 ± 7945.22 | 20,705.83 ± 3126.01 | Group × Time | 0.012 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Baek, S.-H.; Hong, G.-R.; Min, D.-K.; Kim, E.-H.; Park, S.-K. Effects of Functional Fitness Enhancement through Taekwondo Training on Physical Characteristics and Risk Factors of Dementia in Elderly Women with Depression. Int. J. Environ. Res. Public Health 2021, 18, 7961. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18157961
Baek S-H, Hong G-R, Min D-K, Kim E-H, Park S-K. Effects of Functional Fitness Enhancement through Taekwondo Training on Physical Characteristics and Risk Factors of Dementia in Elderly Women with Depression. International Journal of Environmental Research and Public Health. 2021; 18(15):7961. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18157961
Chicago/Turabian StyleBaek, Sun-Hong, Ga-Ram Hong, Do-Kyum Min, Eun-Hee Kim, and Sang-Kab Park. 2021. "Effects of Functional Fitness Enhancement through Taekwondo Training on Physical Characteristics and Risk Factors of Dementia in Elderly Women with Depression" International Journal of Environmental Research and Public Health 18, no. 15: 7961. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18157961