
Applying the Social Vulnerability Index as a Leading Indicator to Protect Fire-Based Emergency Medical Service Responders’ Health


Abstract
:1. Introduction
1.1. Total Worker Health® Approach to Mitigating Fire-Based EMS Responders’ Risks
1.1.1. Health Leading Indicators
1.1.2. SVI as a TWH® Leading Indicator
1.2. Research Questions
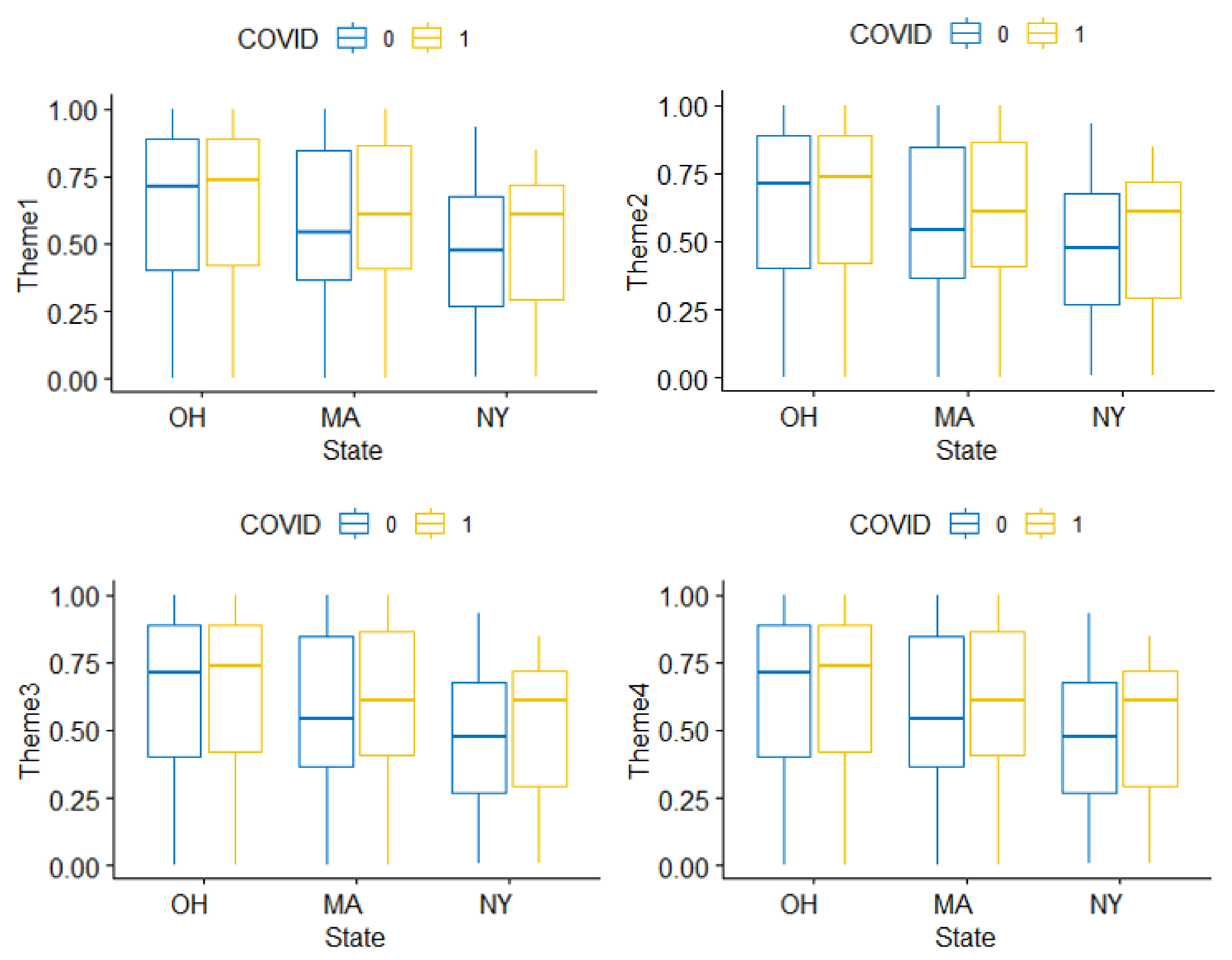
- RQ1: Do the four SVI themes predict fire-based EMS responders’ potential exposure to SARS-CoV-2 during response calls?
- RQ2: Do the four SVI themes predict the types of calls to which fire-based EMS responders are deployed (i.e., EMS, fire, and other)?
2. Materials and Methods
- (1)
- Computer-aided dispatch (CAD) module. The CAD extracts fire department operations information that is automated within municipality reporting systems. These data elements include the type of call, duration of call, exposures during the call, and specific resources deployed to the call (e.g., ladder truck, ambulance).
- (2)
- Individual exposure module (i.e., career diary). A worker’s career diary is manually filled in by a worker after a completed response using either a smart phone or desktop. Within this application, workers input information about potential exposures (e.g., fire, hazmat, chemical, or biological) and personal protective equipment (PPE) worn during the incident (e.g., turnout gear, disposable face shield, or respirator).
2.1. NFORS Data Variables
2.1.1. NFORS Self-Reported Potential Exposure to SARS-CoV-2
2.1.2. NFORS Call Type
2.2. Other Imported Data Variables
2.2.1. Monthly Average of COVID-19 New Cases
2.2.2. Social Vulnerability Index
2.3. Sample
2.4. Analysis
- COVID-19 new cases: New cases of COVID-19 were controlled for in the analysis because the prevalence of COVID-19 infections in an area might affect the call type (i.e., higher rates of EMS calls) and subsequent potential exposure to SARS-CoV-2.
- Fire department/state: Knowing infection rates could be different by state, based on the time of the study, researchers aimed to capture regional effects (by state/department) by creating fire department dummies for use in the analyses.
- Month: Knowing infection rates could vary over time, researchers aimed to capture seasonal effects (by month) by creating time dummy variables.
- Population: If a fire department covers an area with a larger population, fire-based EMS responders may be more likely to be exposed to SARS-CoV-2, as well as receive certain types of calls, in comparison to departments who serve smaller populations, making population an important control variable.
2.4.1. SVI and Exposure to SARS-CoV-2
2.4.2. SVI and Types of Calls
- β10: intercept;
- β11: A one-unit increase in the variable Theme1 is associated with the change in the log odds of having FIRE call vs. EMS call in the amount of β11;
- β21: A one-unit increase in the variable Theme1 is associated with the change in the log odds of having OTHER call vs. EMS call in the amount of β21;
- β17: The log odds of having FIRE call vs. EMS call is associated with a change by β17 if moving from department MA to NY;
- β28: The log odds of having OTHER call vs. EMS call is associated with a change by β28 if moving from department MA to OH.
3. Results
3.1. Descriptive Statistics
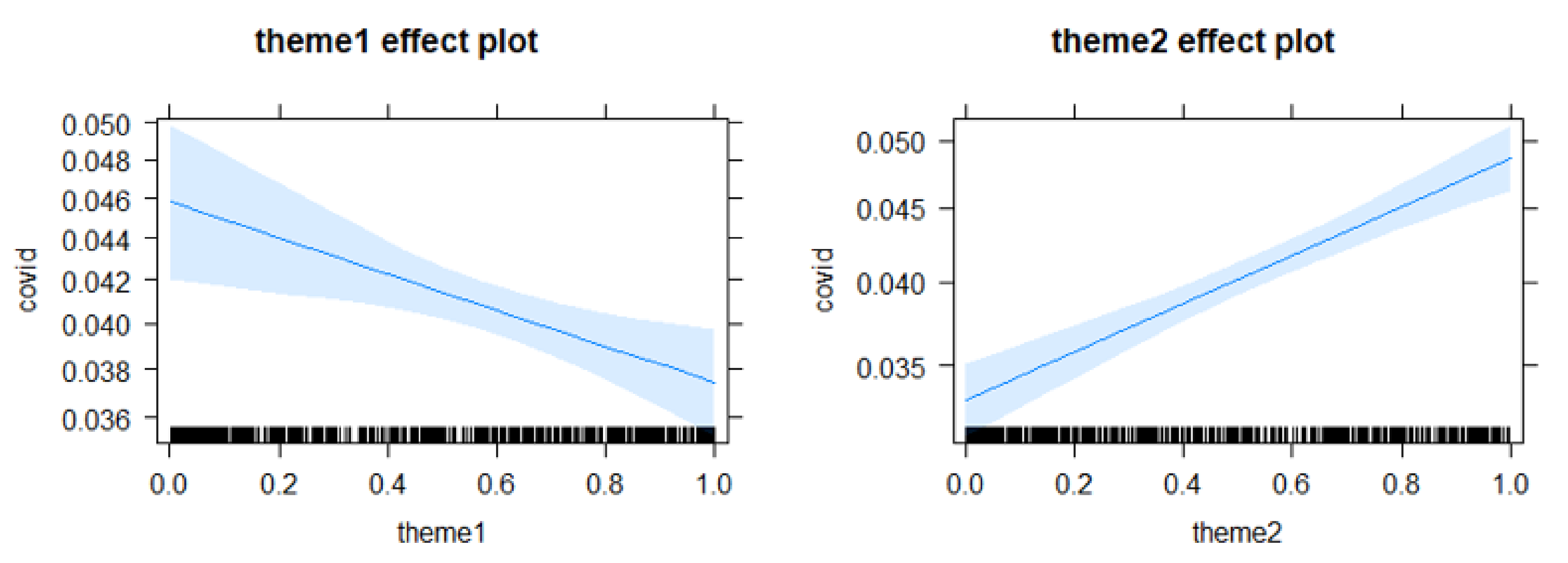
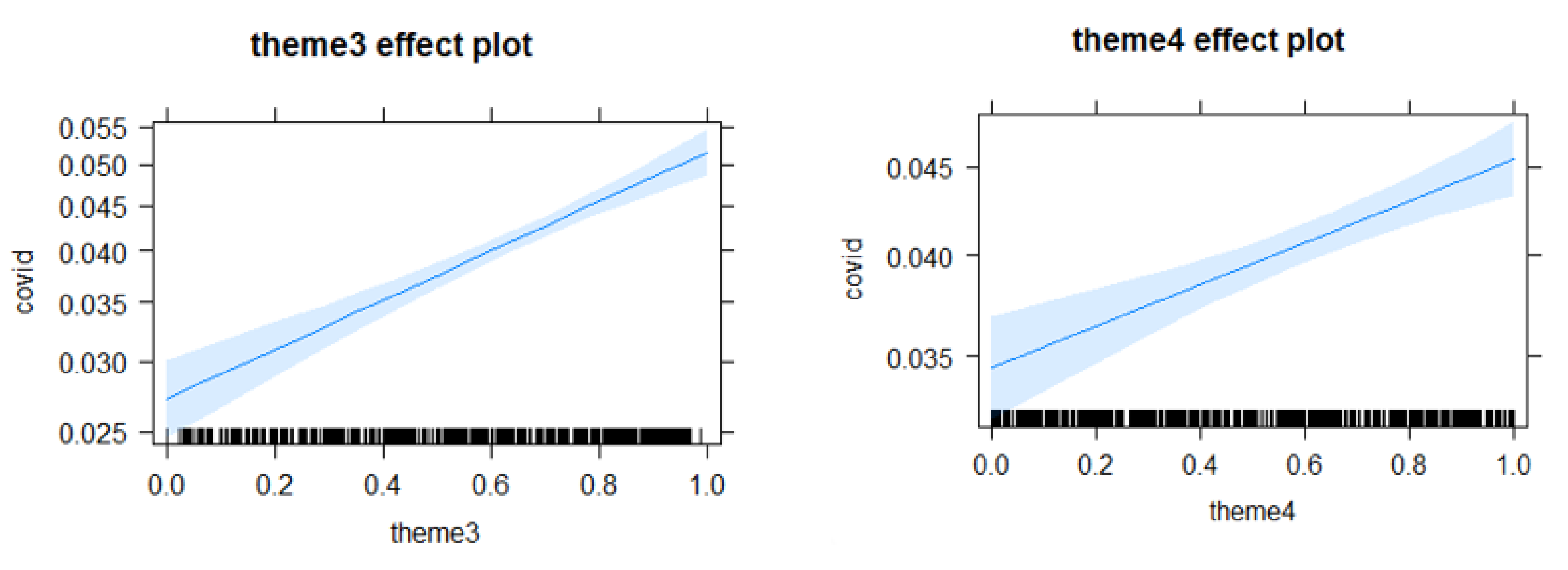
3.2. RQ1 Logit Regression for SVI and SARS-CoV-2 Exposure
- Theme 2—household composition increased the odds of exposure to SARS-CoV-2 by 49.3%;
- Theme 3—racial/ethnic minority/language increased the odds of exposure to SARS-CoV-2 by 94.4%;
- Theme 4—housing/transportation increased the odds of exposure to SARS-CoV-2 by 33.6%.
3.3. RQ2: Multiple Logistic Regression for SVI and Call Type
4. Discussion
4.1. Health Promotion Interventions That Engage Workers on and off the Job
- Incorporate and update SVI as a health leading indicator into safety and health programs around hazard recognition and risk assessment (for examples of such indicators, see [33,34,38]). As previously mentioned, some fire departments have made this addition to their risk assessment programs already e.g., [49]. This mindful addition will allow SVI to be included and acknowledged in organizational audits of fire departments’ safety and health management systems.
- Develop and include educational training materials to maintain safety and health when responding to areas with higher social vulnerability. For example, fire departments can work with their public health departments to develop and provide plain-language, culturally sensitive, and relevant public health messaging tailored to community needs. Regarding COVID-19 specifically, educational materials could be multi-lingual and contain known risk factors for adverse outcomes [71]. Fire-based EMS responders can have these resources with them during emergency response calls to help educate the community and minimize communication gaps with community residents during good intent or other nonlife-threatening calls.
4.2. Improvement of Data Surveillance at the Organizational and Policy Levels
4.2.1. Emergency Call Surveillance Data for Machine Learning
4.2.2. Response Planning and Resource Allocation
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Disclaimer
Appendix A

Appendix B


References
- Reichard, A.A.; Jackson, L.L. Occupational injuries among emergency responders. Am. J. Ind. Med. 2009, 53, 1–11. [Google Scholar] [CrossRef]
- EMS as an Essential Public Safety Service. Ann. Emerg. Med. 2017, 70, 942. [CrossRef] [PubMed]
- NHTSA Office of EMS. What Is EMS? Available online: https://www.ems.gov/whatisems.html (accessed on 21 April 2021).
- ILO (International Labour Organization). CHAPTER V: Substantive Provisions of Labour Legislation. Available online: https://www.ilo.org/legacy/english/dialogue/ifpdial/llg/noframes/ch5.htm#6 (accessed on 14 December 2020).
- NFPA. National Fire Protection Association. Fire Department Calls. Available online: https://www.nfpa.org/News-and-Research/Data-research-and-tools/Emergency-Responders/Fire-department-calls (accessed on 17 April 2021).
- Keisling, P. Why We Need to Take the ‘Fire’ out of ‘Fire Department’. Available online: https://www.governing.com/archive/col-fire-departments-rethink-delivery-emergency-medical-services.html (accessed on 15 April 2021).
- Maguire, B.J.; O’Neill, B.J.; Phelps, S.; Maniscalo, P.M.; Gerard, D.R.; Handal, K.A. COVID-19 Fatalities among EMS Clinicians. EMS. 2020. Available online: https://www.ems1.com/ems-products/personal-protective-equipment-ppe/articles/covid-19-fatalities-among-ems-clinicians-BMzHbuegIn1xNLrP/ (accessed on 15 April 2021).
- Murphy, D.L.; Barnard, L.M.; Drucker, C.J.; Yang, B.; Emert, J.M.; Schwarcz, L.; Counts, C.; Jacinto, T.Y.; McCoy, A.M.; Morgan, A.T.; et al. Occupational exposures and programmatic response to COVID-19 pandemic: An emergency medical services experience. Emerg. Med. J. 2020, 37, 707–713. [Google Scholar] [CrossRef] [PubMed]
- Harrison, R.; Shusterman, D.; Kurtz, T.; Grant, M.; Brokaw, J.; Phelps, S.; Nunez, A. SFFD COVID-19 Antibody Study: Prelim-Inary Information. Available online: https://sffd19.ucsf.edu/sites/g/files/tkssra5726/f/wysiwyg/SFFD%20COVID19%20Seroprev%20Summary%20wo%20.pdf (accessed on 4 July 2021).
- Weiden, M.D.; Zeig-Owens, R.; Singh, A.; Schwartz, T.; Liu, Y.; Vaeth, B.; Nolan, A.; Cleven, K.L.; Hurwitz, K.; Beecher, S.; et al. Pre-COVID-19 lung function and other risk factors for severe COVID-19 in first responders. ERJ Open Res. 2021, 7, 1–4. [Google Scholar] [CrossRef]
- Jamieson, A. What Happens as More Police, Firefighters, and Paramedics Get Sick with COVID-19? Available online: https://www.healthline.com/health-news/what-do-we-do-if-our-police-firefighters-and-paramedics-all-get-sick-with-covid-19 (accessed on 3 July 2021).
- CDC (Centers for Disease Control and Prevention). What Firefighters and EMS Providers Need to Know about COVID-19. 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/community/organizations/firefighter-EMS.html (accessed on 18 April 2021).
- Butler, C.; Marsh, S.; Domitrovich, J.W.; Helmkamp, J. Wildland firefighter deaths in the United States: A comparison of existing surveillance systems. J. Occup. Environ. Hyg. 2017, 14, 258–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Estes, C.R.; Marsh, S.M.; Castillo, D.N. Surveillance of traumatic firefighter fatalities: An assessment of four systems. Public Health Rep. 2011, 126, 540–551. [Google Scholar] [CrossRef] [PubMed]
- Poplin, G.S.; Pollack, K.M.; Griffin, S.; Day-Nash, V.; Peate, W.F.; Nied, E.; Gulotta, J.; Burgess, J.L. Establishing a proactive safety and health risk management system in the fire service. BMC Public Health 2015, 15, 407. [Google Scholar] [CrossRef] [Green Version]
- Walton, S.M.; Conrad, K.M.; Furner, S.E.; Samo, D.G. Cause, type, and workers’ compensation costs of injury to fire fighters. Am. J. Ind. Med. 2003, 43, 454–458. [Google Scholar] [CrossRef] [PubMed]
- Marsh, S.M.; Gwilliam, M.; Konda, S.; Tiesman, H.M.; Fahy, R. Nonfatal injuries to firefighters treated in U.S. emergency departments, 2003–2014. Am. J. Prev. Med. 2018, 55, 353–360. [Google Scholar] [CrossRef]
- Lee, D.J.; Fleming, L.E.; Gomez-Marín, O.; Leblanc, W. Risk of hospitalization among firefighters: The national health interview survey, 1986–1994. Am. J. Public Health 2004, 94, 1938–1939. [Google Scholar] [CrossRef]
- Smith, T.D.; DeJoy, D.M.; Dyal, M.-A.; Pu, Y.; Dickinson, S. Multi-level safety climate associations with safety behaviors in the fire service. J. Saf. Res. 2019, 69, 53–60. [Google Scholar] [CrossRef]
- Smith, T.; Hughes, K.; DeJoy, D.M.; Dyal, M.-A. Assessment of relationships between work stress, work-family conflict, burnout and firefighter safety behavior outcomes. Saf. Sci. 2018, 103, 287–292. [Google Scholar] [CrossRef]
- Tiesman, H.M.; Gwilliam, M.; Konda, S.; Rojek, J.; Marsh, S. Nonfatal injuries to law enforcement officers: A rise in assaults. Am. J. Prev. Med. 2018, 54, 503–509. [Google Scholar] [CrossRef]
- El Sayed, S.A.; Sanford, S.M.; Kerley, K.R. Understanding workplace stress among federal law enforcement officers. Am. J. Crim. Justice 2019, 44, 409–429. [Google Scholar] [CrossRef]
- CDC (Centers for Disease Control and Prevention). Planning for an Emergency: Strategies for Identifying and Engaging at-Risk Groups. A Guidance Document for Emergency Managers, 1st ed.; CDC: Atlanta, GA, USA, 2015. Available online: https://www.cdc.gov/nceh/hsb/disaster/atriskguidance.pdf (accessed on 3 July 2021).
- Smith, T.D.; Mullins-Jaime, C.; Dyal, M.-A.; DeJoy, D.M. Stress, burnout and diminished safety behaviors: An argument for Total Worker Health® approaches in the fire service. J. Saf. Res. 2020, 75, 189–195. [Google Scholar] [CrossRef]
- NIOSH (National Institute for Occupational Safety and Health). What Is Total Worker Health? Available online: https://www.cdc.gov/niosh/twh/totalhealth.html (accessed on 12 April 2021).
- NIOSH (National Institute for Occupational Safety and Health). The NIOSH Future of Work Initiative. 2020. Available online: https://www.cdc.gov/niosh/topics/future-of-work/default.html (accessed on 8 April 2021).
- NIOSH (National Institute for Occupational Safety and Health). Fundamentals of Total Worker Health Approaches: Essential Elements for Advancing Worker Safety, Health, and Well-Being; Publication No. 2017-112; Lee, M.P., Hudson, H., Richards, R., Chang, C.C., Chosewood, L.C., Schill, A.L., Eds.; NIOSH: Cincinnati, OH, USA, 2016.
- Tamers, S.L.; Chosewood, L.C.; Childress, A.; Hudson, H.; Nigam, J.; Chang, C.C. Total Worker Health® 2014–2018: The novel approach to worker safety, health, and well-being evolves. Int. J. Environ. Res. Public Health 2019, 16, 321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ASSP (American Society of Safety Professionals). ASSP/ISO TR-45005-2021 Occupational Health and Safety Management—Safe Working During the COVID-19 pandemic—General Guidelines for Organizations; A technical report prepared by ASSP and registered with ANSI; American Society of Safety Professionals: Park Ridge, IL, USA, 2021. [Google Scholar]
- Sinclair, R.R.; Allen, T.; Barber, L.; Bergman, M.; Britt, T.; Butler, A.; Ford, M.; Hammer, L.; Kath, L.; Probst, T.; et al. Occupational health science in the time of COVID-19: Now more than ever. Occup. Health Sci. 2020, 4, 1–22. [Google Scholar] [CrossRef] [PubMed]
- ADPC (Asian Disaster Preparedness Center). Integrating Disaster Risk Management into the Development Process. Disaster Risk Management Practitioner’s Handbook Series, Bangkok. 2013. Available online: https://www.adpc.net/igo/category/ID407/doc/2013-pKb4FR-ADPC-ADPC_DRM_Practitioners_Handbook_-_The_Development_Process.pdf (accessed on 17 April 2021).
- Tveiten, C.K.; Albrechtsen, E.; Wærø, I.; Wahl, A.M. Building resilience into emergency management. Saf. Sci. 2012, 50, 1960–1966. [Google Scholar] [CrossRef] [Green Version]
- NSC, National Safety Council, Campbell Institute. Elevating EHS Leading Indicators: From Defining to Designing. 2017. Available online: https://www.thecampbellinstitute.org/wp-content/uploads/2017/05/Campbell-Institute-Elevating-EHS-Leading-Indicators-From-Defining-to-Designing-WP.pdf (accessed on 17 April 2021).
- NSC, National Safety Council, Campbell Institute. Transforming EHS Performance Measurement through Leading Indicators. 2017. Available online: https://www.thecampbellinstitute.org/wp-content/uploads/2017/07/Campbell-Institute-Transforming-EHS-through-Leading-Indicators-WP.pdf (accessed on 17 April 2021).
- NSC, National Safety Council, Campbell Institute. An Implementation Guide to Leading Indicators. 2019. Available online: https://www.thecampbellinstitute.org/wp-content/uploads/2019/08/Campbell-Institute-An-Implementation-Guide-to-Leading-Indicators.pdf (accessed on 17 April 2021).
- NASEM. Leading Health Indicators 2030: Advancing Health, Equity, and Well-Being; National Academies of Sciences, Engineering, and Medicine: Washington, DC, USA, 2020. [Google Scholar]
- IOM (Institute of Medicine). Leading health indicators for health people 2020: Letter report; The National Academies Press: Washington, DC, USA, 2011. [Google Scholar] [CrossRef]
- AIHA (American Industrial Hygiene Association). Best Practice Guide for Leading Health Metrics in Occupational Health and Safety Programs. 2020. Available online: https://aiha-assets.sfo2.digitaloceanspaces.com/AIHA/resources/Guidance-Documents/Best-Practice-Guide-for-Leading-Health-Metrics-in-Occupational-Health-and-Safety-Programs-Guidance-Document.pdf (accessed on 15 April 2021).
- Morrow, B.H. Identifying and Mapping Community Vulnerability. Disasters 1999, 23, 1–18. [Google Scholar] [CrossRef]
- O’Brien, G.; O’Keefe, P.; Rose, J.; Wisner, B. Climate change and disaster management. Disasters 2006, 30, 64–80. [Google Scholar] [CrossRef]
- Phillips, B.D.; Thomas, D.S.; Fothergill, A.; Blinn-Pike, L. Social Vulnerability to Disasters; CRC Press: Boca Raton, FL, USA, 2010. [Google Scholar]
- Cutter, S.L.; Burton, C.G.; Emrich, C.T. Disaster resilience indicators for benchmarking baseline conditions. J. Homel. Secur. Emerg. Manag. 2010, 7, 1–22. [Google Scholar]
- Cutter, S.L. GI science, disasters, and emergency management. Trans GIS 2003, 7, 439–446. [Google Scholar] [CrossRef]
- Cutter, S.L.; Mitchell, J.T.; Scott, M.S. Revealing the vulnerability of people and places: A case study of Georgetown County, South Carolina. Ann. Assoc. Am. Geogr. 2000, 90, 713–737. [Google Scholar] [CrossRef]
- Flanagan, B.E.; Gregory, E.W.; Hallisey, E.J.; Heitgerd, J.L.; Lewis, B. A social vulnerability index for disaster management. J. Homel. Secur. Emerg. Manag. 2011, 8, 1–22. [Google Scholar] [CrossRef]
- CDC (Centers for Disease Control and Prevention). Health Equity Considerations and Racial and Ethnic Minority Groups. 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/community/health-equity/race-ethnicity.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fcoronavirus%2F2019-ncov%2Fneed-extra-precautions%2Fracial-ethnic-minorities.html (accessed on 21 April 2021).
- ATSDR (Agency for Toxic Substances and Disease Registry). Social Vulnerability Index. 2021. Available online: https://www.atsdr.cdc.gov/placeandhealth/svi/index.html (accessed on 18 April 2021).
- Dasgupta, S.; Bowen, V.B.; Leidner, A.; Fletcher, K.; Musial, T.; Rose, C.; Cha, A.; Kang, G.; Dirlikov, E.; Pevzner, E.; et al. Association between social vulnerability and a county’s risk for becoming a COVID-19 hotspot—United States, June 1–July 25, 2020. Morb. Mortal Wkly. Rep. 2020, 69, 1535. [Google Scholar] [CrossRef] [PubMed]
- City of Columbus. Columbus Fire and EMS Standards of Cover/Community Risk Assessment. 2020. Available online: https://www.columbusga.gov/Portals/FireEMS/StandardsOfCover2020.pdf?ver=BQu8fFyIs1WfBj3beL4ZaQ%3D%3D (accessed on 8 July 2021).
- Tamers, S.L.; Streit, J.; Pana-Cryan, R.; Ray, T.; Syron, L.; Flynn, M.A.; Castillo, D.; Roth, G.; Geraci, C.; Guerin, R.; et al. Envisioning the future of work to safeguard the safety, health, and well-being of the workforce: A perspective from the CDC’s National Institute for Occupational Safety and Health. Am. J. Ind. Med. 2020, 63, 1065–1084. [Google Scholar] [CrossRef]
- OSHA (Occupational Safety and Health Administration). Part 1910.1030—Bloodborne Pathogens. Available online: https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.1030 (accessed on 18 April 2021).
- IPSDI (International Public Safety Data Institute). NFORS Changes Everything. Available online: https://i-psdi.org/nfors-overview.html (accessed on 20 April 2021).
- Kinsey, K.; Ahrens, M. NFIRS Incident Types: Why Aren’t They Telling a Clearer Story? National Fire Protection Association: Quincy, MA, USA, 2016; Available online: https://www.nfpa.org/-/media/Files/News-and-Research/Fire-statistics-and-reports/Emergency-responders/osNFIRSIncidentType.ashx?la=en (accessed on 10 April 2021).
- GitHub. NY Times COVID-19 Data. Available online: https://github.com/nytimes/covid-19-data (accessed on 10 April 2021).
- ATSDR (Agency for Toxic Substances and Disease Registry). Geospatial Research, Analysis, and Service Program. Social Vulnerability Index. Available online: https://svi.cdc.gov/data-and-tools-download.html (accessed on 1 February 2021).
- Tonidandel, S.; LeBreton, J.M. Relative importance analysis: A useful supplement to regression analysis. J. Bus. Psychol. 2011, 26, 1–9. [Google Scholar] [CrossRef]
- Tonidandel, S.; Lebreton, J.M.; Johnson, J.W. Determining the statistical significance of relative weights. Psychol. Methods 2009, 14, 387–399. [Google Scholar] [CrossRef]
- Millett, G.A.; Jones, A.T.; Benkeser, D.; Baral, S.; Mercer, L.; Beyrer, C.; Honermann, B.; Lankiewicz, E.; Mena, L.; Crowley, J.S.; et al. Assessing differential impacts of COVID-19 on black communities. Ann. Epidemiol. 2020, 47, 37–44. [Google Scholar] [CrossRef]
- Kaiser Family Foundation. Low-Income and Communities of Color at Higher Risk of Serious Illness If Infected with Coronavirus. Available online: https://www.kff.org/coronavirus-covid-19/issue-brief/low-income-and-communities-of-color-at-higher-risk-of-serious-illness-if-infected-with-coronavirus/ (accessed on 15 April 2021).
- Rodriguez-Diaz, C.E.; Guilamo-Ramos, V.; Mena, L.; Hall, E.; Honermann, B.; Crowley, J.S.; Baral, S.; Prado, G.J.; Marzan-Rodriguez, M.; Beyrer, C.; et al. Risk for COVID-19 infection and death among Latinos in the United States: Examining heterogeneity in transmission dynamics. Ann. Epidemiol. 2020, 52, 46–53.e2. [Google Scholar] [CrossRef]
- Karaye, I.M.; Horney, J.A. The Impact of social vulnerability on COVID-19 in the U.S.: An analysis of spatially varying relationships. Am. J. Prev. Med. 2020, 59, 317–325. [Google Scholar] [CrossRef]
- Punnett, L.; Cavallari, J.M.; Henning, R.A.; Nobrega, S.; Dugan, A.G.; Cherniack, M.G. Defining ‘integration for Total Worker Health®: A new proposal. Ann. Work. Expo. Health 2020, 64, 223–235. [Google Scholar] [CrossRef] [Green Version]
- Schill, A.L. Advancing well-being through Total Worker Health®. Work. Health Saf. 2017, 65, 158–163. [Google Scholar] [CrossRef]
- Maguire, B.J.; Smith, S. Injuries and fatalities among emergency medical technicians and paramedics in the United States. Prehosp. Disaster Med. 2013, 28, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Henning, R.; Warren, N.; Robertson, M.; Faghri, P.; Cherniack, M. The CPH-NEW research team workplace health protection and promotion through participatory ergonomics: An integrated approach. Public Health Rep. 2009, 124, 26–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Punnett, L.; Cherniack, M.; Henning, R.; Morse, T.; Faghri, P. The CPH-NEW Research Team A conceptual framework for integrating workplace health promotion and occupational ergonomics programs. Public Health Rep. 2009, 124, 16–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Punnett, L.; Warren, N.; Henning, R.; Nobrega, S.; Cherniack, M. Participatory ergonomics as a model for integrated programs to prevent chronic disease. J. Occup. Environ. Med. 2013, 55, S19–S24. [Google Scholar] [CrossRef]
- Cherniack, M.; Dussetschleger, J.; Dugan, A.; Farr, D.; Namazi, S.; El Ghaziri, M.; Henning, R. Participatory action research in corrections: The HITEC 2 program. Appl. Ergon. 2016, 53, 169–180. [Google Scholar] [CrossRef]
- CDC (Centers for Disease Control and Prevention). The CDC Worksite Health ScoreCard. Available online: https://www.cdc.gov/dhdsp/pubs/docs/HSC_Manual.pdf (accessed on 15 April 2021).
- CDC (Centers for Disease Control and Prevention). Introduction to the “New and Improved” CDC Worksite Health ScoreCard. Available online: www.cdc.gov/workplacehealthpromotion/initiatives/healthscorecard/pdf/CDC-Scorecard-Update-Webinar-Final-508.pdf (accessed on 15 April 2021).
- Cromer, S.J.; Lakhani, C.M.; Wexler, D.J.; Burnett-Bowie, S.A.M.; Udler, M.; Patel, C.J. Geospatial Analysis of Individual and Community-Level Socioeconomic Factors Impacting SARS-CoV-2 Prevalence and Outcomes. Available online: https://www.medrxiv.org/content/10.1101/2020.09.30.20201830v1 (accessed on 17 April 2021).
- Chau, P.H.; Gusmano, M.K.; Cheng, J.O.Y.; Cheung, S.H.; Woo, J. Social vulnerability index for the older people—Hong Kong and New York City as examples. J. Hered. 2014, 91, 1048–1064. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Institute for Occupational Safety and Health and American Society of Safety Professionals. Overlapping Vulnerabilities: The Occupational Safety and Health of Young Immigrant Workers in Small Construction Firms; Publication No. 2015-178; NIOSH: Cincinnati, OH, USA, 2015.
- Jørgensen, M.B.; Villadsen, E.; Burr, H.; Punnett, L.; Holtermann, A. Does employee participation in workplace health promotion depend on the working environment? A cross-sectional study of Danish workers. BMJ Open 2016, 6, e010516. [Google Scholar] [CrossRef] [Green Version]
- CDC (Centers for Disease Control and Prevention). Public Health Surveillance: Preparing for the Future. 2021. Available online: https://www.cdc.gov/surveillance/pdfs/Surveillance-Series-Bookleth.pdf (accessed on 5 May 2021).
- EENA (European Emergency Number Association). Artificial Intelligence and Machine Learning in Public Safety; EENA: Brussels, Belgium, 2019; Available online: https://eena.org/knowledge-hub/documents/artificial-intelligence-machine-learning-in-public-safety/ (accessed on 5 May 2021).
- Cannuscio, C.C.; Davis, A.L.; Kermis, A.D.; Khan, Y.; Dupuis, R.; Taylor, J.A. A Strained 9-1-1 system and threats to public health. J. Community Health 2016, 41, 658–666. [Google Scholar] [CrossRef] [Green Version]
- Nethercott, K. Security. Defense mechanisms. Health Serv. J. 1997, 107, 30–31. [Google Scholar]
- Bigham, B.L.; Kennedy, S.M.; Drennan, I.; Morrison, L.J. Expanding paramedic scope of practice in the community: A systematic review of the literature. Prehosp. Emerg. Care 2013, 17, 361–372. [Google Scholar] [CrossRef]
- Lahav, O.; Mastronarde, N.; van der Schaar, M. What is interpretable? Using machine learning to design interpretable decision-support systems machine learning for health (ML4H). In Proceedings of the 32nd Conference on Neural Information Processing Systems, Workshop at NeurIPS 2018, Montreal, QC, Canada, 8 December 2018. [Google Scholar]
- Ferenchik, M. Columbus Pilot Program Determines First Responder or Social Worker Response for 911 Calls. The Columbus Dispatch. 18 May. Available online: https://www.firefighternation.com/leadership/columbus-pilot-program-determines-first-responder-or-social-worker-response-for-911-calls/#gref (accessed on 4 July 2021).
- Wolkin, A.; Patterson, J.R.; Harris, S.; Soler, E.; Burrer, S.; McGeehin, M.; Greene, S. Reducing public health risk during disasters: Identifying social vulnerabilities. J. Homel. Secur. Emerg. Manag. 2015, 12, 809–822. [Google Scholar] [CrossRef] [Green Version]
- Murray, R.M.; Allen, J.A.; Davis, A.L.; Taylor, J.A. Meeting science meets public health: Results from the “Stress and Violence in fire-based EMS Responders (SAVER)” systems checklist consensus conference (SC3). J. Saf. Res. 2020, 74, 249–261. [Google Scholar] [CrossRef]
- Taylor, J.A.; Murray, R.M.; Davis, A.L.; Shepler, L.J.; Harrison, C.K.; Novinger, N.A.; Allen, J.A. Creation of a systems-level checklist to address stress and violence in fire-based emergency medical services responders. Occup. Health Sci. 2019, 3, 265–295. [Google Scholar] [CrossRef] [Green Version]
- Mendes, J.M.D.O. Social vulnerability indexes as planning tools: Beyond the preparedness paradigm. J. Risk Res. 2009, 12, 43–58. [Google Scholar] [CrossRef]
- Dennerlein, J.T.; Burke, L.; Sabbath, E.L.; Williams, J.A.R.; Peters, S.; Wallace, L.; Karapanos, M.; Sorensen, G. An integrative total worker health framework for keeping workers safe and healthy during the COVID-19 pandemic. Hum. Factors J. Hum. Factors Ergon. Soc. 2020, 62, 689–696. [Google Scholar] [CrossRef] [PubMed]
- Haas, E.J.; Yorio, P.L. Exploring the differences in safety climate among mining sectors. Min. Met. Explor. 2021, 38, 655–668. [Google Scholar] [CrossRef]
- McLellan, D.L.; Cabán-Martinez, A.J.; Nelson, C.C.; Pronk, N.P.; Katz, J.N.; Allen, J.D.; Sorensen, G. Organizational characteristics influence implementation of worksite health protection and promotion programs: Evidence from smaller businesses. J. Occup. Environ. Med. 2015, 57, 1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NIOSH (National Institute for Occupational Safety and Health). Productive Aging and Work: Safety and Health Outcomes. 2015. Available online: https://www.cdc.gov/niosh/topics/productiveaging/safetyandhealth.html (accessed on 16 April 2021).

{kind=link}
{kind=link}
{kind=link}
| SVI Theme | SVI Subthemes | Negative Impact |
|---|---|---|
| Theme 1: Socioeconomic status (SES) | Percentage of persons below poverty estimate, percentage unemployed estimate, per capita income estimate, and percentage with no high school diploma estimate | Often lack resources needed to comply with emergency preparedness instructions |
| Theme 2: Household composition/disability | Percentage of people ≥65 and ≤17 years old, percentage with a disability, and percentage of single-parent households | Issues with communication and comprehension of an emergency, subsequent barriers to mobility, and more likely to need financial support |
| Theme 3: Minority status/language | Percentage in racial/ethnic minority groups and the percentage who speak English less than well | Trouble understanding public health directives, culturally insensitive messaging |
| Theme 4: Housing/transportation | Percentage multiunit structures, percentage mobile homes, percentage crowding, percentage no vehicle, and percentage group quarters | Live in multi-unit structures or mobile homes in group quarters, lack vehicle |
| Variables | ||||
|---|---|---|---|---|
| Continuous variables | N | Mean | SD | Description |
| Theme 1 (SES) | 156,983 | 0.6086 | 0.3016 | Percentile ranking of SES |
| Theme 2 (household/disability) | 156,983 | 0.5220 | 0.3474 | Percentile ranking of household composition/disability |
| Theme 3 (minority status/language) | 156,983 | 0.6201 | 0.2287 | Percentile ranking of minority status/language |
| Theme 4 (housing/transportation) | 156,983 | 0.5843 | 0.2717 | Percentile ranking of housing/transportation |
| Population | 156,983 | 4504 | 2416 | Total population of the geographic area |
| COVID-19 new cases | 156,983 | 131 | 91.52 | Monthly averaged COVID new cases of the specified geographic area (i.e., FIPS) |
| Categorical variables | N | percentage | ||
| Potential SARS-CoV-2 Exposure | ||||
| 156,983 | ||||
| Yes | 8143 | 5.2% | ||
| No | 148,840 | 94.8% | ||
| Department | 156,983 | |||
| Massachusetts | 41,917 | 26.7% | ||
| New York | 5692 | 3.6% | ||
| Ohio | 109,374 | 69.7% | ||
| Call Type | 156,983 | |||
| EMS | 99,297 | 63.3% | ||
| Fire | 47,729 | 30.4% | ||
| Other | 9957 | 6.3% |
| Theme 1 SES | Theme 2 Household/ Disability | Theme 3 Minority Status/Language | Theme 4 Housing/ Transportation | |||||
|---|---|---|---|---|---|---|---|---|
| Potential SARS-CoV-2 exposure | Mean | SD | Mean | SD | Mean | SD | Mean | SD |
| Yes | 0.6122 | 0.2793 | 0.5195 | 0.3329 | 0.7032 | 0.2191 | 0.6605 | 0.2557 |
| No | 0.6084 | 0.3028 | 0.5221 | 0.3481 | 0.6156 | 0.2283 | 0.5802 | 0.2719 |
| Call Type | Mean | SD | Mean | SD | Mean | SD | Mean | SD |
| EMS | 0.6382 | 0.2933 | 0.5732 | 0.3326 | 0.6015 | 0.2223 | 0.5581 | 0.2724 |
| Fire | 0.5566 | 0.3103 | 0.4401 | 0.3554 | 0.6439 | 0.2362 | 0.6185 | 0.2644 |
| Other | 0.5631 | 0.3019 | 0.4038 | 0.3489 | 0.6917 | 0.2298 | 0.6825 | 0.2570 |
| Massachusetts | New York | Ohio | ||||
|---|---|---|---|---|---|---|
| Yes potential exposure | 3212 | 7.7% | 1338 | 23.5% | 3593 | 3.3% |
| No potential exposure | 38,705 | 92.3% | 4354 | 76.5% | 105,781 | 96.7% |
| Total | 41,917 | 5692 | 109,374 | |||
| Vulnerability | Mean | SD | Mean | SD | Mean | SD |
| Theme 1 | 0.5524 | 0.2978 | 0.4650 | 0.2687 | 0.6377 | 0.2995 |
| Theme 2 | 0.3778 | 0.3579 | 0.3662 | 0.2344 | 0.5854 | 0.3286 |
| Theme 3 | 0.7555 | 0.2070 | 0.7434 | 0.2027 | 0.5618 | 0.2128 |
| Theme 4 | 0.7370 | 0.1967 | 0.7074 | 0.2855 | 0.5194 | 0.2700 |
| Est. | Std.Err | Pr (>|z|) | Odds Ratio | 95% Confidence Interval | ||
|---|---|---|---|---|---|---|
| (2.5%) | (97.5%) | |||||
| (intercept) | −4.020 * | 0.063 | 0.000 | 0.018 | 0.016 | 0.0203 |
| Theme 1 (SES) | −0.210 * | 0.072 | 0.004 | 0.810 | 0.703 | 0.934 |
| Theme 2 (household/disability) | 0.401 * | 0.052 | 0.000 | 1.493 | 1.349 | 1.653 |
| Theme 3 (minority status/language) | 0.665 * | 0.080 | 0.000 | 1.944 | 1.663 | 2.274 |
| Theme 4 (housing/transportation) | 0.289 * | 0.056 | 0.000 | 1.336 | 1.197 | 1.491 |
| Department | ||||||
| NY | 0.869 * | 0.042 | 0.000 | 2.383 | 2.196 | 2.585 |
| OH | −0.807 * | 0.033 | 0.000 | 0.446 | 0.418 | 0.476 |
| Population | 0.000 * | 0.000 | 0.000 | 1.000 | 1.000 | 1.000 |
| COVID-19 Cases | 0.005 * | 0.000 | 0.000 | 1.005 | 1.005 | 1.005 |
| FIRE | OTHER | |||||
|---|---|---|---|---|---|---|
| Coefficient | RRR | 95% CI | Coefficient | RRR | 95% CI | |
| (Intercept) | 1.222 * | 3.3931 | 3.3706–3.4157 | −0.385 * | 0.6803 | 0.6797–0.6809 |
| SVI themes | ||||||
| Theme 1 | −0.254 * | 0.7754 | 0.7697–0.7811 | −0.062 * | 0.9403 | 0.9395–0.9412 |
| Theme 2 | −0.368 * | 0.6919 | 0.6873–0.6964 | −0.637 * | 0.5287 | 0.5283–0.5291 |
| Theme 3 | −0.281 * | 0.7550 | 0.7511–0.7589 | −0.048 * | 0.9529 | 0.9522–0.9537 |
| Theme 4 | −0.036 * | 0.9644 | 0.9593–0.9694 | 0.312 * | 1.3668 | 1.3658–1.3678 |
| Department | ||||||
| NY | −1.656 * | 0.1909 | 0.1908–0.1910 | −1.362 * | 0.2561 | 0.2561–0.2562 |
| OH | −1.959 * | 0.14106 | 0.1403–0.1418 | −2.520 * | 0.08043 | 0.0804–0.0805 |
| Total population | −0.00000 | 1 | 1.0000–1.0000 | −0.00002 * | 1 | 1.0000–1.0000 |
| COVID-19 cases | −0.0002 ** | 0.9998 | 0.9997–1.0000 | −0.0003 * | 0.9997 | 0.9995–0.9998 |
| Residual deviance | 227314 | |||||
| AIC | 227350 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haas, E.J.; Furek, A.; Casey, M.; Yoon, K.N.; Moore, S.M. Applying the Social Vulnerability Index as a Leading Indicator to Protect Fire-Based Emergency Medical Service Responders’ Health. Int. J. Environ. Res. Public Health 2021, 18, 8049. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18158049
Haas EJ, Furek A, Casey M, Yoon KN, Moore SM. Applying the Social Vulnerability Index as a Leading Indicator to Protect Fire-Based Emergency Medical Service Responders’ Health. International Journal of Environmental Research and Public Health. 2021; 18(15):8049. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18158049
Chicago/Turabian StyleHaas, Emily J., Alexa Furek, Megan Casey, Katherine N. Yoon, and Susan M. Moore. 2021. "Applying the Social Vulnerability Index as a Leading Indicator to Protect Fire-Based Emergency Medical Service Responders’ Health" International Journal of Environmental Research and Public Health 18, no. 15: 8049. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18158049