
Understanding the Life, Pain, and Barriers to Physical Activity in Korean Patients with Panic Disorder: Photovoice Inquiry

 ,
, 
Abstract
:1. Introduction
2. Method
2.1. Study Design
2.2. Participant Selection
2.3. Research Team and Reflexivity
2.4. Measurement
2.5. Data Analysis
2.6. Authenticity and Trustworthiness
2.7. Compliance with Ethical Standards
3. Results
3.1. The Life and Pain of Patients with PD
3.1.1. Fear of Confined or Large Places
Especially in the elevator… outside, in the park … I feel anxious regardless of where I am…I am worried that the elevator won’t open … Sometime in the past, I don’t know if the elevator was new or not, but it was too quiet. I thought that it broke down. Panic came instantly …(C)
3.1.2. Anxiety about Somatization Symptoms and Avoidance
I’m afraid to go to supermarkets or coffee shops, the crowded places, so I order a lot of things online. It was so hard to go to the supermarkets… I went to a large market once, but it was so hard …(G)
I have a precursor before the panic attack comes… When the precursor comes, it’s okay if I take medicine as soon as possible… It gets a lot harder when I cannot do that … I always prepare for the precursor … for everything… Especially if the precursor comes out while driving… it’s very dangerous … so I try not to drive as much as possible… and not to go so far… my spouse usually drives a lot.(A)
3.1.3. Thoughts of Death and Fear
The doctors in the hospital always say everyday … that I’ll never die with this disease… But in my everyday life, this disease is always connected to death… Anxiety starts to come …for example, it’s called a panic attack, when I run into it, I just think I will die. I am always afraid of the fear of death… I feel I am going to die.(A)
3.1.4. Limitations of Living and Longing
Now coffee… it contains caffeine. So now, when I talked with the doctor, he told me to avoid having caffeine as well as stress, in my first visit to him… It’s been more than 5 years since I stopped having coffee. But although there are many coffee shops around, I don’t go there… I envy those who go to the coffee shop, and sometimes I want to have a cup of coffee there.(D)
3.1.5. Side Effects of Medication
I have the side effects that I want to do nothing and I just want to sleep… These are psychotropic…When I joined an online community for panic disorder and worked, I saw many people talk the same just as me. If I take medicine, I become lethargic, have little vitality, and go limp.(G)
I feel comfortable when I take medicine in the hospital… If I don’t have it, I feel anxious. People with panic disorder probably feel like me…
3.1.6. Longing That No One Knows
This photo was taken with the meaning that I was alone… there is loneliness in my mind. Because other people don’t know and I’m the only one who knows about the disease … When the arms are broken, they can be seen to others, but this disease cannot be seen, so if I don’t explain … I don’t make the opportunities to meet people as much as possible, so I don’t meet people and I feel a bit lonely and a little isolated.(E)
3.2. Difficulties of Physical Activity Perceived by Patients with Panic Disorder
3.2.1. Avoidance Due to Panic Attacks or Anticipatory Anxiety Experienced during Physical Activity
I don’t want to think about it, but if I do, I went to the emergency room because I thought I would die from hyperventilation while playing soccer… That’s why I don’t play soccer anymore…(E)
I played badminton… I was playing badminton, but my heart suddenly seemed to be beating fast and I couldn’t breathe well… I stopped playing and got help from others … I have been to the emergency room by calling 119.(B)
I haven’t exercised, but sometimes I’ve tried … Whenever I exercised … I felt like I was breathing with this straw in my mouth. This means that I am out of breath. Now I cannot overcome this, so it’s very difficult to exercise.(G)
3.2.2. Happy Memories, but Now I Can’t …
I took a picture of a tennis racket … It’s been a while since I had panic disorder … before that, I really liked playing sports. So, the happiest time for me is when I exercise, and I miss those times a little … and … I haven’t used the racket since I had panic disorder although I have it in my car … So, whenever I open the truck and look at the racket, I think it was really good time in the past, but why is it like this now?(F)
3.2.3. Anticipatory Anxiety about Places of Physical Activity
This is a photo of a shower room … After exercising, I must take a shower. Because it is hard for me to enter such a narrow place … I won’t do it… when I exercise, because I have to take a shower again, I have to go into a narrow space … that is continuously connected, to me …(B)
3.2.4. Lack of Desire to Exercise
It seems that not only the desire for exercise but also the desire for diverse lifestyle often disappears. I feel like I am drowsy and thoughtless …(D)
3.2.5. Nevertheless, Physical Activity Is a Challenge
I bought a smart watch … because the heart rate can be checked with it … because I keep looking at the heart rate. Now I check the watch when I feel a little breathless and anxious … if my heart rate is normal, I think I feel relieved. I have a habit of always wearing the watch and checking it whenever I move.(C)
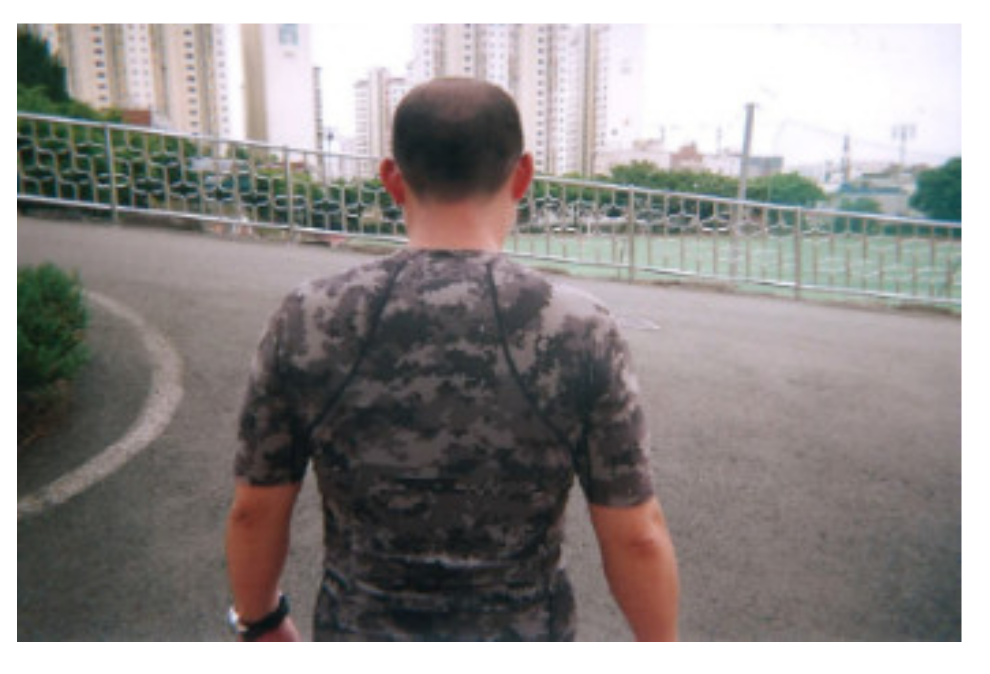
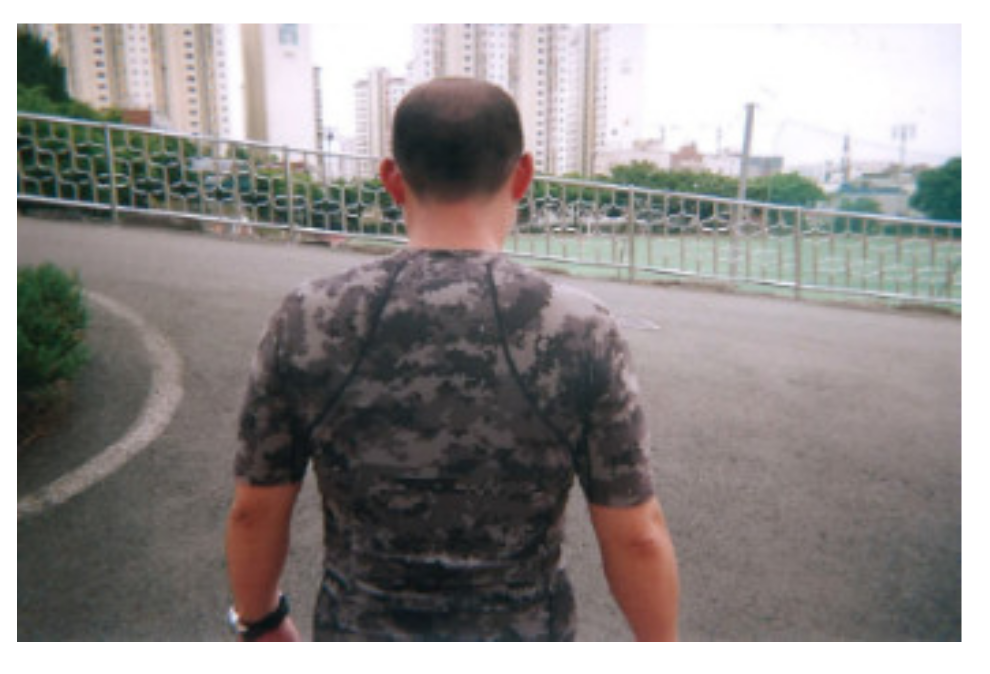
When I exercise, there must always be a lot of people … if there is no one, I don’t exercise. I need a partner for any other reason… well… I need people around me … if I’m in an emergency, they can take me to the emergency room or treat me … and yes … so actually I cannot exercise often.(F)
It means that I check a location of a hospital in order to go there quickly when I have a panic attack. Of course, I know the hospital on the way I always go, and if I go a different route for the first time, I always check the nearby hospital first before I start to go. It is the same with exercise. Even if I cannot participate in sports sometimes, if I go with my friends, I think that I can do it because I like playing sports and I am good at it … I check the location of a hospital that I can get to as soon as possible and then I go to watch the sports.(A)
4. Discussion
4.1. To See the World through Their Eyes
4.2. Patients with PD and Barriers to Physical Activity
4.3. Phyical Activity for Patients with Panice Disorder
4.4. Symptoms in People with Panic Disorder Vary Widely, Making It Very Difficult for Doctors to Recommend Certain Physical Activities. I. Neuropsychiatrist
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Suh, H.-S.; Lee, J.-H.; Gim, M.-S.; Kim, M.-K. Korean guidelines for the treatment of panic disorder. J. Korean Med. Assoc. 2018, 61, 493–499. [Google Scholar] [CrossRef]
- Zhou, T.H.; Hu, G.L.; Wang, L. Psychological Disorder Identifying Method Based on Emotion Perception over Social Networks. Int. J. Environ. Res. Public Health 2019, 16, 953. [Google Scholar] [CrossRef] [Green Version]
- Pattyn, T.; Eede, F.V.D.; Lamers, F.; Veltman, D.; Sabbe, B.G.; Penninx, B.W. Identifying Panic Disorder Subtypes Using Factor Mixture Modeling. Depress. Anxiety 2015, 32, 509–517. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Kim, Y.S.; Yoo, S.W. Quality of Life in Patients with Panic Disorder. J. Korean Neuropsychiatr Assoc. 2001, 40, 407–415. [Google Scholar]
- Roy-Byrne, P.P. Panic Disorder in Adults: Epidemiology, Pathogenesis, Clinical Manifestations, Course, Assessment, and Diagnosis; Up To Date: Waltham, MA, USA, 2016. [Google Scholar]
- Park, S.H. Evidence-Based Treatment of Panic Disorder. Korean J. Clin. Psychol. 2017, 36, 458–469. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.M.; Kim, M.K.; Lee, S.H. Neurobiological Basis of Anxiety Related Disorders. Korean J. Biol. Psychiatry 2018, 21, 128–140. [Google Scholar]
- Yue, G.H.; Eun-Young, S.; Hyun-Joo, K. Cognitive Behavioral Therapy for Panic Disorder: Domestic Research Trends. Korean J. Rehabil. Psychol. 2017, 24, 637–654. [Google Scholar]
- Quagliato, L.A.; Cosci, F.; Shader, R.I.; Silberman, E.K.; Starcevic, V.; Balon, R.; Dubovsky, S.L.; Salzman, C.; Krystal, J.H.; Weintraub, S.J.; et al. Selective serotonin reuptake inhibitors and benzodiazepines in panic disorder: A meta-analysis of common side effects in acute treatment. J. Psychopharmacol. 2019, 33, 1340–1351. [Google Scholar] [CrossRef] [PubMed]
- Gautam, S.; Jain, A.; Gautam, M.; Vahia, V.N.; Gautam, A. Clinical Practice Guidelines for the Management of Generalised Anxiety Disorder (GAD) and Panic Disorder (PD). Indian J. Psychiatry 2017, 59, 67–S73. [Google Scholar] [CrossRef]
- Christensen, A.B.; Wahrén, S.; Reinholt, N.; Poulsen, S.; Hvenegaard, M.; Simonsen, E.; Arnfred, S. “Despite the Differences, We Were All the Same”. Group Cohesion in Diagnosis-Specific and Transdiagnostic CBT Groups for Anxiety and Depression: A Qualitative Study. Int. J. Environ. Res. Public Health 2021, 18, 5324. [Google Scholar] [CrossRef]
- Horst, F.; Oudsten, B.D.; Zijlstra, W.; de Jongh, A.; Lobbestael, J.; de Vries, J. Cognitive Behavioral Therapy vs. Eye Movement Desensitization and Reprocessing for Treating Panic Disorder: A Randomized Controlled Trial. Front. Psychol. 2017, 8, 1409. [Google Scholar] [CrossRef] [Green Version]
- Choi, Y.H.; Lee, J.H. Cognitive-behavioral Therapy for Panic Disorder. J. Korean Neuropsychiatr Assoc. 1998, 37, 603–619. [Google Scholar]
- Caldirola, D.; Alciati, A.; Riva, A.; Perna, G. Are there advances in pharmacotherapy for panic disorder? A systematic review of the past five years. Expert Opin. Pharmacother. 2018, 19, 1357–1368. [Google Scholar] [CrossRef]
- Stubbs, B.; Koyanagi, A.; Hallgren, M.; Firth, J.; Richards, J.; Schuch, F.; Rosenbaum, S.; Mugisha, J.; Veronese, N.; Lahti, J.; et al. Physical activity and anxiety: A perspective from the World Health Survey. J. Affect. Disord. 2017, 208, 545–552. [Google Scholar] [CrossRef] [Green Version]
- Mochcovitch, M.D.; Deslandes, A.; Freire, R.; Garcia, R.; Nardi, A.E. The effects of regular physical activity on anxiety symptoms in healthy older adults: A systematic review. Rev. Bras. de Psiquiatr. 2016, 38, 255–261. [Google Scholar] [CrossRef] [Green Version]
- Powers, M.; Asmundson, G.J.G.; Smits, J. Exercise for Mood and Anxiety Disorders: The State-of-the Science. Cogn. Behav. Ther. 2015, 44, 237–239. [Google Scholar] [CrossRef] [Green Version]
- Fetzner, M.G.; Asmundson, G.J. Aerobic Exercise Reduces Symptoms of Posttraumatic Stress Disorder: A Randomized Controlled Trial. Cogn. Behav. Ther. 2015, 44, 301–313. [Google Scholar] [CrossRef] [PubMed]
- Kim, I.-H. Effects of Relaxation Therapy and Exercise Therapy on the ACTH and Cortisol Hormone Level in Workers. J. Korean Acad. Fundam. Nurs. 2001, 8, 293–301. [Google Scholar]
- Yang, Y.-J. Exercise and Stress. Korean Soc. Stress Med. 2005, 13, 165–169. [Google Scholar]
- Bin Lim, Y.; Kim, J.W.; Hong, S.-B.; Kim, J.-W. Association between BDNF and Antidepressant Effects of Exercise in Youth: A Preliminary Study. J. Korean Acad. Child Adolesc. Psychiatry 2016, 27, 72–81. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.H.; Yang, J.C.; Kim, J.B.; Lim, K.Y.; Lee, S.Y.; Yu, B.H. A Validation Study of Korean Albany Panic and Phobia Questionnaire (APPQ). J. Korean Neuropsychiatr. Assoc. 2004, 43, 329–336. [Google Scholar]
- Onwuegbuzie, A.J.; Leech, N.L. A Call for Qualitative Power Analyses. Qual. Quant. 2007, 41, 105–121. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Creswell, J.W.; Poth, C.N. Qualitative Inquiry and Research Design: Choosing among Five Approaches; Sage Publications: Thousand Oaks, CA, USA, 2016. [Google Scholar]
- Baker, T.A.; Wang, C.C. Photovoice: Use of a Participatory Action Research Method to Explore the Chronic Pain Experience in Older Adults. Qual. Health Res. 2006, 16, 1405–1413. [Google Scholar] [CrossRef]
- Kim, K.-O. Socio-ecological Meaning, Concern, and Improvement Plan Associated with Physical Activity in Older Population in Rural Area: A Mixed Method Inquiry. Korean J. Phys. Educ.-Humanit. Soc. Sci. 2015, 54, 41–57. [Google Scholar]
- Maxwell, J.A. Qualitative Research Design: An Interactive Approach; Sage: Thousand Oaks, CA, USA, 2005. [Google Scholar]
- Denzin, N.K. Qualitative Inquiry under Fire: Toward a New Paradigm Dialogue; Left Coast Press: Walnut Creek, CA, USA, 2009. [Google Scholar]
- Asami, T.; Nakamura, R.; Takaishi, M.; Yoshida, H.; Yoshimi, A.; Whitford, T.J.; Hirayasu, Y. Smaller volumes in the lateral and basal nuclei of the amygdala in patients with panic disorder. PLoS ONE 2018, 13, e0207163. [Google Scholar] [CrossRef] [Green Version]
- Starcevic, V. Will the RANZCP clinical practice guidelines for the treatment of anxiety disorders assist in making adequate treatment decisions for panic disorder? Aust. N. Z. J. Psychiatry 2018, 53, 362–363. [Google Scholar] [CrossRef]
- Hoehn, T.; Braune, S.; Scheibe, G.; Albus, M. Physiological, biochemical and subjective parameters in anxiety patients with panic disorder during stress exposure as compared with healthy controls. Eur. Arch. Psychiatry Clin. Neurosci. 1997, 247, 264–274. [Google Scholar] [CrossRef] [PubMed]
- Fleury, M.-J.; Ngui, A.N.; Bamvita, J.-M.; Grenier, G.; Caron, J. Predictors of healthcare service utilization for mental health reasons. Int. J. Environ. Res. Public Health 2014, 11, 10559–10586. [Google Scholar] [CrossRef] [Green Version]
- Held-Poschardt, D.; Sterzer, P.; Schlagenhauf, F.; Pehrs, C.; Wittmann, A.; Stoy, M.; Hägele, C.; Knutson, B.; Heinz, A.; Ströhle, A. Reward and loss anticipation in panic disorder: An fMRI study. Psychiatry Res. Neuroimaging 2018, 271, 111–117. [Google Scholar] [CrossRef]
- Kandola, A.; Vancampfort, D.; Herring, M.; Rebar, A.; Hallgren, M.; Firth, J.; Stubbs, B. Moving to Beat Anxiety: Epidemiology and Therapeutic Issues with Physical Activity for Anxiety. Curr. Psychiatry Rep. 2018, 20, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKinzie, A.E. Scared to Death: Reflections on Panic and Anxiety in the Field. Symb. Interact. 2017, 40, 483–497. [Google Scholar] [CrossRef]
- Carrera, M.; Herrán, A.; Ayuso-Mateos, J.L.; Sierra-Biddle, D.; Ramírez, M.L.; Ayestarán, A.; Hoyuela, F.; Rodríguez-Cabo, B.; Vázquez-Barquero, J.L. Quality of life in early phases of panic disorder: Predictive factors. J. Affect. Disord. 2006, 94, 127–134. [Google Scholar] [CrossRef]
- Nayar, N.; Deshpande, M.; Mudgal, S.; Pandey, R. Depression, anxiety, perceived loneliness among school-going adolescents. A comparative study between hostellers and day boarders. J. Med. Sci. Clin. Res. 2018, 6, 344–348. [Google Scholar] [CrossRef]
- Tretiakov, A.; Malakhova, A.; Naumova, E.; Rudko, O.; Klimov, E. Genetic Biomarkers of Panic Disorder: A Systematic Review. Genes 2020, 11, 1310. [Google Scholar] [CrossRef]
- Angehrn, A.; Teale Sapach, M.J.; Ricciardelli, R.; MacPhee, R.S.; Anderson, G.S.; Carleton, R.N. Sleep quality and mental disorder symptoms among Canadian public safety personnel. Int. J. Environ. Res. Public Health 2020, 17, 2708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kinchin, D. Post Traumatic Stress Disorder: The Invisible Injury; Success Unlimited: Montgomery, AL, USA, 2004. [Google Scholar]
- Silva, L.R.B.; Seguro, C.S.; de Oliveira, C.G.A.; Santos, P.O.S.; de Oliveira, J.C.M.; Filho, L.F.M.D.S.; Júnior, C.A.D.P.; Gentil, P.; Rebelo, A.C.S. Physical Inactivity Is Associated with Increased Levels of Anxiety, Depression, and Stress in Brazilians During the COVID-19 Pandemic: A Cross-Sectional Study. Front. Psychiatry 2020, 11, 565291. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, P.J.; Herring, M.; McDowell, C.P.; Dishman, R.K. Physical activity is indirectly associated with pain in college women through associations with somatization and panic disorder symptoms: A cross-sectional study. Ann. Epidemiol. 2019, 33, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Nardi, A.E.; Freire, R.C.; Zin, W.A. Panic disorder and control of breathing. Respir. Physiol. Neurobiol. 2009, 167, 133–143. [Google Scholar] [CrossRef]
- McDowell, C.P.; Dishman, R.K.; Gordon, B.R.; Herring, M.P. Physical Activity and Anxiety: A Systematic Review and Meta-analysis of Prospective Cohort Studies. Am. J. Prev. Med. 2019, 57, 545–556. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Yoon, K.L. Emotional response to autobiographical memories in depression: Less happiness to positive and more sadness to negative memories. Cogn. Behav. Ther. 2020, 49, 475–485. [Google Scholar] [CrossRef]
- Ogawa, S.; Kondo, M.; Okazaki, J.; Imai, R.; Ino, K.; A Furukawa, T.; Akechi, T. The relationships between symptoms and quality of life over the course of cognitive-behavioral therapy for panic disorder in Japan. Asia-Pac. Psychiatry 2016, 9, e12249. [Google Scholar] [CrossRef]
- Perna, G.; Caldirola, D. Is panic disorder a disorder of physical fitness? A heuristic proposal. F1000Research 2018, 7, 294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quagliato, L.A.; Freire, R.C.; Nardi, A.E. Risks and benefits of medications for panic disorder: A comparison of SSRIs and benzodiazepines. Expert Opin. Drug Saf. 2018, 17, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Maremmani, A.G.; Cerniglia, L.; Cimino, S.; Bacciardi, S.; Rovai, L.; Pallucchini, A.; Spera, V.; Perugi, G.; Maremmani, I. Further Evidence of a Specific Psychopathology of Addiction. Differentiation from Other Psychiatric Psychopathological Dimensions (Such as Obesity). Int. J. Environ. Res. Public Health 2017, 14, 943. [Google Scholar] [CrossRef] [Green Version]
- Smits, J.A.J.; Zvolensky, M.J. Emotional vulnerability as a function of physical activity among individuals with panic disorder. Depress. Anxiety 2006, 23, 102–106. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant | Gender | Age | Marital Status | Family/ Inmate | Monthly Income (USD) | Education Level | Regular PA Participation | Remarks |
|---|---|---|---|---|---|---|---|---|
| A | Male | 52 | Single | Alone | 1500 or over | College graduation | NO | |
| B | Male | 42 | Married | Children | 1500 or over | College graduation | NO | |
| C | Male | 54 | Married | Spouse | 1500 or over | High school graduation | NO | |
| D | Female | 38 | Single | Relative | 500 or over | Grad school graduation | NO | |
| E | Male | 42 | Married | Spouse | 1500 or over | College graduation | NO | |
| F | Male | 46 | Married | Spouse | 1500 or over | College graduation | NO | |
| G | Female | 42 | Married | Spouse | 1500 or over | College graduation | NO | |
| H | Female | 34 | Married | Single | 500 or over | High school graduation | NO | Drop-out |
| I | Male | 47 | Married | - | - | Neuropsychiatrist | - | Medical Advice |
| Stage | Details | Operator |
|---|---|---|
| 1 | Finding significant statements with photographs | All researchers |
| 2 | Integration, organizing and collecting significant statements with photographs | Kim, Buttler, Gritzmacher |
| 3 | Classifying categories (e.g., pain and physical activity) through the classification of important statements | Kim, Buttler, Gritzmacher |
| 4 | Finding main themes and sub-themes in separated categories | All researchers |
| 5 | a) Repeated discussion and reflection of the research team to determine the final theme b) Holistic analysis based on overall statement, descrption, theme, and interpretation c) Sharing data with research participants for theme confirmation | All researchers & participants |
| 6 | Creating report | Kim |
| Main Theme | Sub-Themes | Title of Photos |
|---|---|---|
| The life and pain of patients with PD |
|
|
|
| |
|
| |
|
| |
|
| |
| Longing that no one knows |
| |
| Difficulties of physical activity perceived by patients with panic disorder |
|
|
|
| |
|
| |
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, K.-O.; Ryu, J.-H.; Chung, H.-R.; Butler, M.K.; Gritzmacher, D. Understanding the Life, Pain, and Barriers to Physical Activity in Korean Patients with Panic Disorder: Photovoice Inquiry. Int. J. Environ. Res. Public Health 2021, 18, 8140. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18158140
Kim K-O, Ryu J-H, Chung H-R, Butler MK, Gritzmacher D. Understanding the Life, Pain, and Barriers to Physical Activity in Korean Patients with Panic Disorder: Photovoice Inquiry. International Journal of Environmental Research and Public Health. 2021; 18(15):8140. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18158140
Chicago/Turabian StyleKim, Kyung-O, Jae-Hyeong Ryu, Hae-Ryong Chung, Marcia K. Butler, and Deborah Gritzmacher. 2021. "Understanding the Life, Pain, and Barriers to Physical Activity in Korean Patients with Panic Disorder: Photovoice Inquiry" International Journal of Environmental Research and Public Health 18, no. 15: 8140. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18158140