
Mouthwash Use and the Risk of Oral, Pharyngeal, and Laryngeal Cancer. A Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Method
2.2. Selection Criteria
2.3. Data Collection and Analysis
2.4. Quality Assessment and Risk of Bias
2.5. Statistical Analysis
3. Results
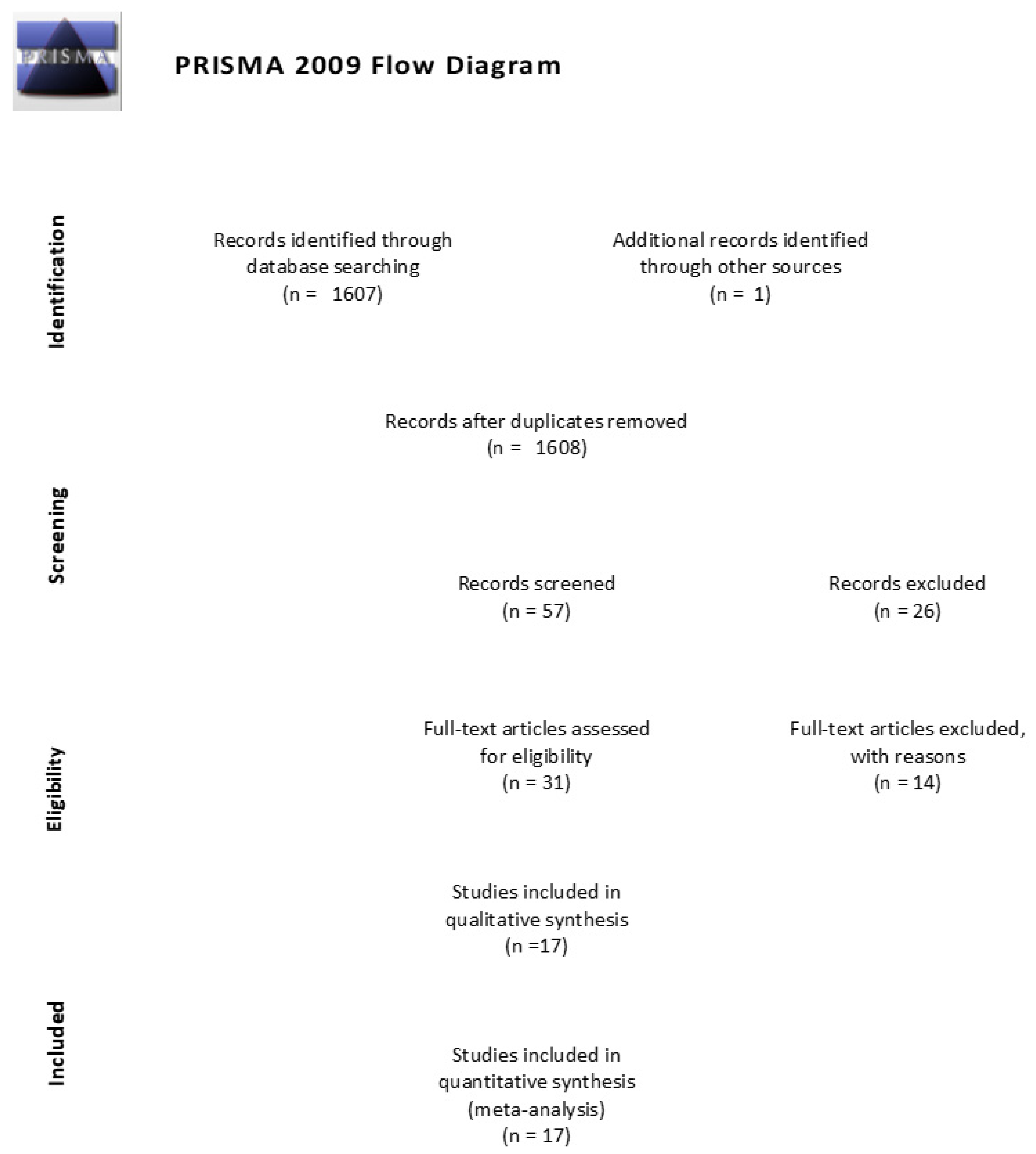
3.1. Search Synthesis
3.2. Quality Assessment
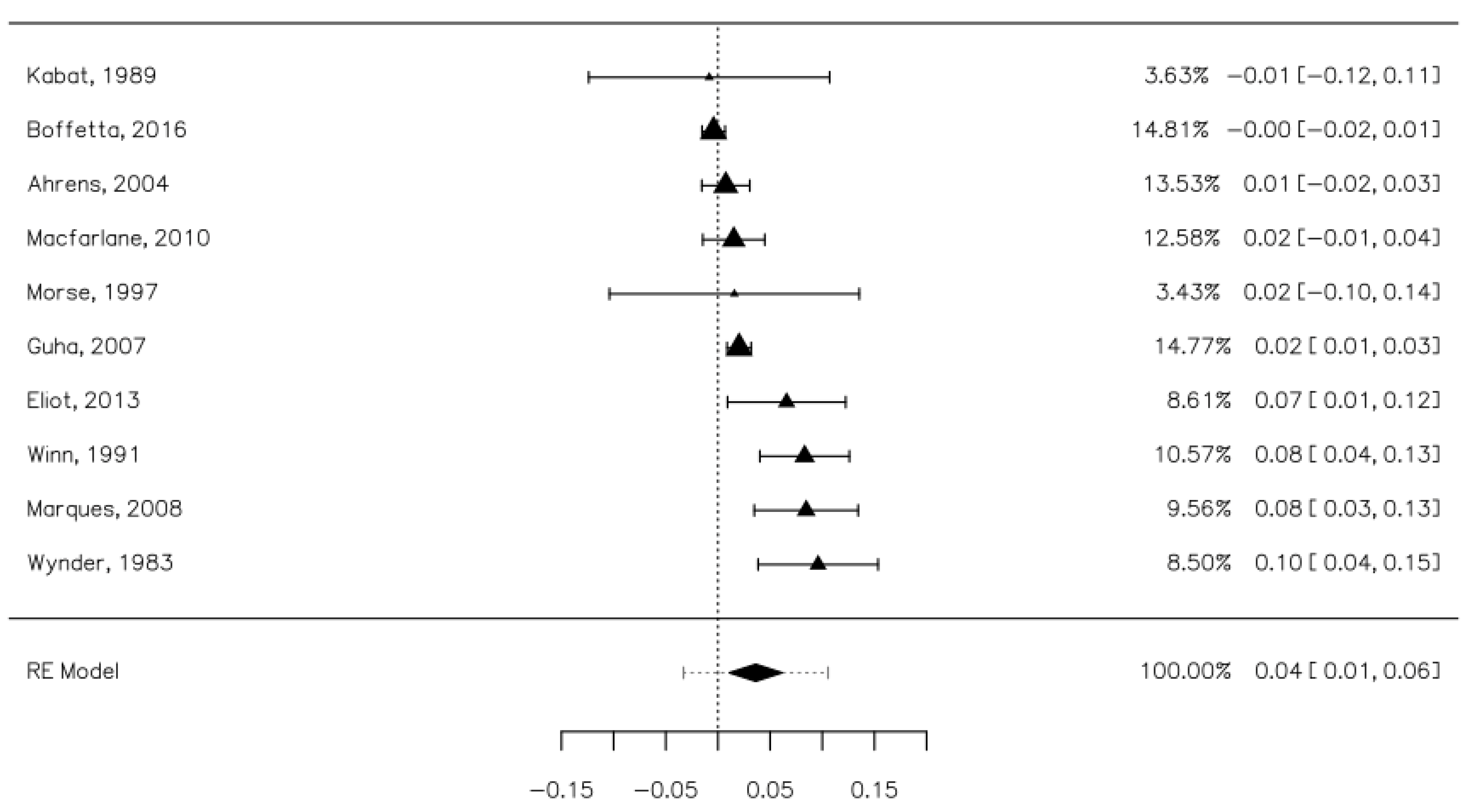
3.3. The Overall Risk of Upper Aerodigestive Tract Cancers Associated with Mouthwash Use
3.4. The Risk of Upper Aerodigestive Tract Cancers Associated with Mouthwash Depending on the Alcohol Content
3.5. The Risk of Upper Aerodigestive Tract Cancers Associated with Mouthwash Depending on the Frequency and Duration of Use
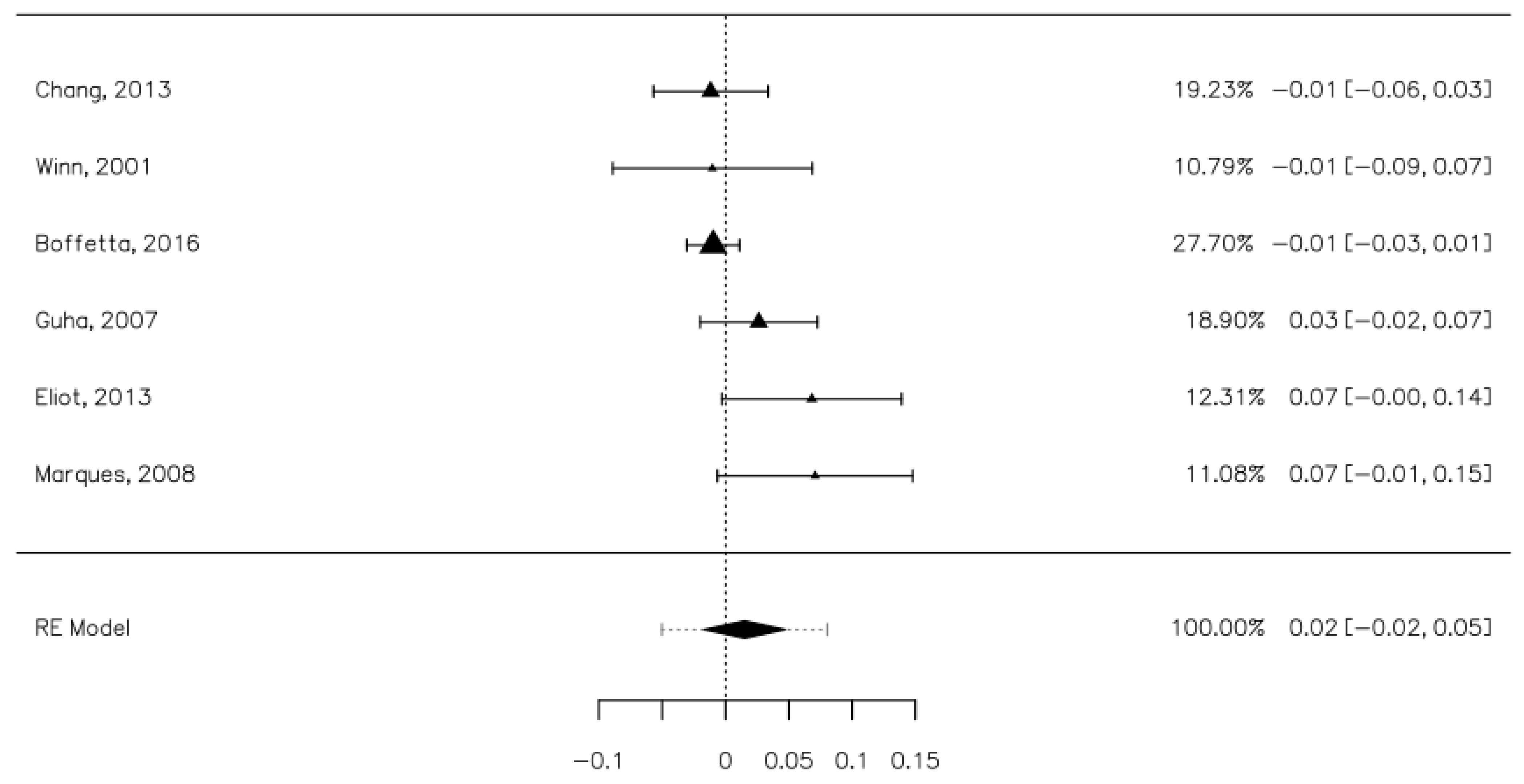
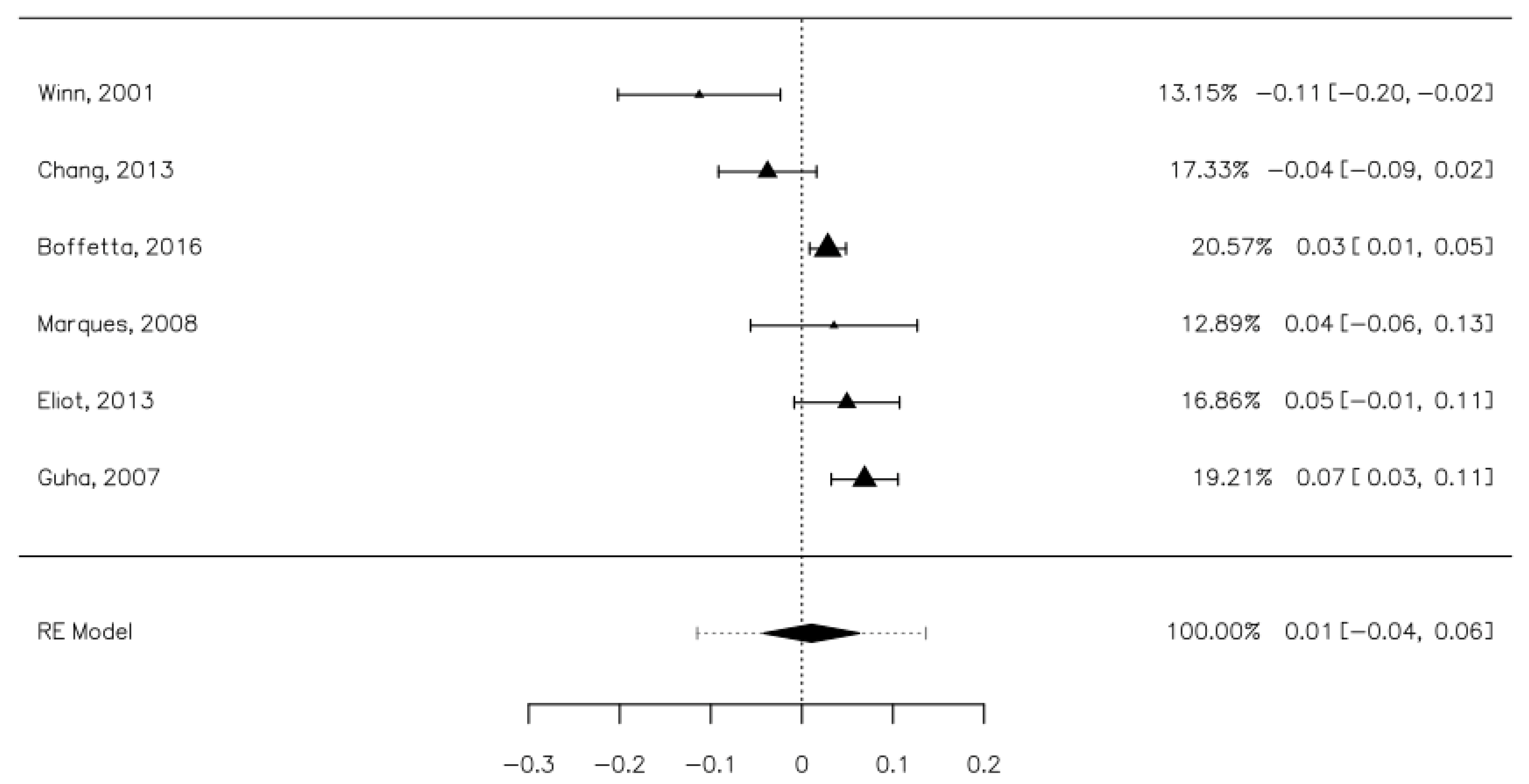
3.6. The Risk of Oral, Pharyngeal, and Laryngeal Cancer Associated with Mouthwash Use
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Petti, S.; Masood, M.; Scully, C. The magnitude of tobacco smoking-betel quid chewing-alcohol drinking interaction effect on oral cancer in South-East Asia. A meta-analysis of observational studies. PLoS ONE 2013, 8, e78999. [Google Scholar] [CrossRef]
- Quadri, M.F.A.; Tadakamadla, S.K.; John, T. Smokeless tobacco and oral cancer in the Middle East and North Africa: A systematic review and meta-analysis. Tob. Induc. Dis. 2019, 17, 56. [Google Scholar] [CrossRef] [PubMed]
- Sand, L.; Jalouli, J. Viruses and oral cancer. Is there a link? Microbes Infect. 2014, 16, 371–378. [Google Scholar] [CrossRef]
- Aupérin, A. Epidemiology of head and neck cancers: An update. Curr. Opin. Oncol. 2020, 32, 178–186. [Google Scholar] [CrossRef]
- Gall, F.; Colella, G.; Di Onofrio, V.; Rossiello, R.; Angelillo, I.F.; Liguori, G. Candida spp. in oral cancer and oral precancerous lesions. New Microbiol. 2013, 36, 283–288. [Google Scholar]
- Shimakage, M.; Horii, K.; Tempaku, A.; Kakudo, K.; Shirasaka, T.; Sasagawa, T. Association of Epstein-Barr virus with oral cancers. Hum. Pathol. 2002, 33, 608–614. [Google Scholar] [CrossRef] [PubMed]
- Scully, C. Oral cancer aetiopathogenesis; past, present and future aspects. Med. Oral Patol. Oral Cir. Bucal 2011, 16, e306-11. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.S.; Lo, H.I.; Wong, T.Y.; Huang, C.C.; Lee, W.T.; Tsai, S.T.; Chen, K.C.; Yen, C.J.; Wu, Y.H.; Hsueh, W.T.; et al. Investigating the association between oral hygiene and head and neck cancer. Oral Oncol. 2013, 49, 1010–1017. [Google Scholar] [CrossRef]
- Lachenmeier, D.W.; Monakhova, Y.B.; Markova, M.; Kuballa, T.; Rehm, J. What happens if people start drinking mouthwash as surrogate alcohol? A quantitative risk assessment. Food Chem. Toxicol. 2013, 51, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Vlachojannis, C.; Winsauer, H.; Chrubasik, S. Effectiveness and safety of a mouthwash containing essential oil ingredients. Phytother. Res. 2013, 27, 685–691. [Google Scholar] [CrossRef]
- Homann, N.; Tillonen, J.; Meurman, J.H.; Rintamäki, H.; Lindqvist, C.; Rautio, M.; Jousimies-Somer, H.; Salaspuro, M. Increased salivary acetaldehyde levels in heavy drinkers and smokers: A microbiological approach to oral cavity cancer. Carcinogenesis 2000, 21, 663–668. [Google Scholar] [CrossRef]
- Seitz, H.K.; Stickel, F. Molecular mechanisms of alcohol-mediated carcinogenesis. Nat. Rev. Cancer 2007, 7, 599–612. [Google Scholar] [CrossRef] [PubMed]
- Cook, R.T. Alcohol abuse, alcoholism, and damage to the immune system—A review. Alcohol. Clin. Exp. Res. 1998, 22, 1927–1942. [Google Scholar] [CrossRef]
- Ko, Y.C.; Huang, Y.L.; Lee, C.H.; Chen, M.J.; Lin, L.M.; Tsai, C.C. Betel quid chewing, cigarette smoking and alcohol consumption related to oral cancer in Taiwan. J. Oral Pathol. Med. 1995, 24, 450–453. [Google Scholar] [CrossRef] [PubMed]
- Aceves Argemí, R.; González Navarro, B.; Ochoa García-Seisdedos, P.; Estrugo Devesa, A.; López-López, J. Mouthwash With Alcohol and Oral Carcinogenesis: Systematic Review and Meta-analysis. J. Evid. Based. Dent. Pract. 2020, 20, 101407. [Google Scholar] [CrossRef] [PubMed]
- Weaver, A.; Fleming, S.M.; Smith, D.B. Mouthwash and oral cancer: Carcinogen or coincidence? J. Oral Surg. 1979, 37, 250–253. [Google Scholar] [PubMed]
- Gandini, S.; Negri, E.; Boffetta, P.; La Vecchia, C.; Boyle, P. Mouthwash and oral cancer risk—Quantitative meta-analysis of epidemiologic studies. Ann. Agric. Environ. Med. 2012, 19, 173–180. [Google Scholar]
- Appendix 2: MOOSE Guidelines. In Systematic Reviews in the Social Sciences; Blackwell Publishing Ltd: Oxford, UK, 2008; pp. 288–290. ISBN 9780470754887.
- Moher, D.; Altman, D.G.; Liberati, A.; Tetzlaff, J. PRISMA statement. Epidemiology 2011, 22, 128. [Google Scholar] [CrossRef] [Green Version]
- Luchini, C.; Stubbs, B.; Solmi, M.; Veronese, N. Assessing the quality of studies in meta-analyses: Advantages and limitations of the Newcastle Ottawa Scale. World J. Metaanal. 2017, 5, 80. [Google Scholar] [CrossRef]
- Sidik, K.; Jonkman, J.N. A comparison of heterogeneity variance estimators in combining results of studies. Stat. Med. 2007, 26, 1964–1981. [Google Scholar] [CrossRef]
- Borenstein, M.; Hedges, P.L.V.; Higgins, D.J.; Rothstein, H.R.; Borenstein, D.M.; Higgins, J.P. Introduction to Meta-Analysis; Wiley: Hoboken, NJ, USA, 2009; ISBN 9781282123434. [Google Scholar]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [Green Version]
- Ahrens, W.; Pohlabeln, H.; Foraita, R.; Nelis, M.; Lagiou, P.; Lagiou, A.; Bouchardy, C.; Slamova, A.; Schejbalova, M.; Merletti, F.; et al. Oral health, dental care and mouthwash associated with upper aerodigestive tract cancer risk in Europe: The ARCAGE study. Oral Oncol. 2014, 50, 616–625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blot, W.J.; Winn, D.M.; Fraumeni, J.F., Jr. Oral cancer and mouthwash. J. Natl. Cancer Inst. 1983, 70, 251–253. [Google Scholar]
- Boffetta, P.; Hayes, R.; Sartori, S.; Lee, Y.-C.; Muscat, J.; Olshan, A.; Winn, D.; Zhang, X.C.-F.; Morgenstern, H.; Chen, C.; et al. Mouthwash use and cancer of the head and neck: A pooled analysis from the International Head and Neck Cancer Epidemiology Consortium. Eur. J. Cancer Prev. 2016, 25, 344–348. [Google Scholar] [CrossRef] [Green Version]
- D’Souza, G.; Kreimer, A.R.; Viscidi, R.; Pawlita, M.; Fakhry, C.; Koch, W.M.; Westra, W.H.; Gillison, M.L. Case–Control Study of Human Papillomavirus and Oropharyngeal Cancer. N. Engl. J. Med. 2007, 356, 1944–1956. [Google Scholar] [CrossRef] [Green Version]
- Eliot, M.N.; Michaud, D.S.; Langevin, S.M.; McClean, M.D.; Kelsey, K.T. Periodontal disease and mouthwash use are risk factors for head and neck squamous cell carcinoma. Cancer Causes Control 2013, 24, 1315–1322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garrote, L.F.; Herrero, R.; Reyes, R.M.; Vaccarella, S.; Anta, J.L.; Ferbeye, L.; Muñoz, N.; Franceschi, S. Risk factors for cancer of the oral cavity and oro-pharynx in Cuba. Br. J. Cancer 2001, 85, 46–54. [Google Scholar] [CrossRef] [Green Version]
- Guha, N.; Boffetta, P.; Wünsch Filho, V.; Eluf Neto, J.; Shangina, O.; Zaridze, D.; Curado, M.P.; Koifman, S.; Matos, E.; Menezes, A.; et al. Oral health and risk of squamous cell carcinoma of the head and neck and esophagus: Results of two multicentric case-control studies. Am. J. Epidemiol. 2007, 166, 1159–1173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kabat, G.C.; Hebert, J.R.; Wynder, E.L. Risk factors for oral cancer in women. Cancer Res. 1989, 49, 2803–2806. [Google Scholar]
- Macfarlane, T.V.; Macfarlane, G.J.; Oliver, R.J.; Benhamou, S.; Bouchardy, C.; Ahrens, W.; Pohlabeln, H.; Lagiou, P.; Lagiou, A.; Castellsague, X.; et al. The aetiology of upper aerodigestive tract cancers among young adults in Europe: The ARCAGE study. Cancer Causes Control 2010, 21, 2213–2221. [Google Scholar] [CrossRef]
- Marques, L.A.; Eluf-Neto, J.; Figueiredo, R.A.O.; de Góis-Filho, J.F.; Kowalski, L.P.; de Carvalho, M.B.; Abrahão, M.; Wünsch-Filho, V. Oral health, hygiene practices and oral cancer. Rev. Saude Publica 2008, 42, 471–479. [Google Scholar] [CrossRef] [Green Version]
- Mashberg, A.; Barsa, P.; Grossman, M.L. A study of the relationship between mouthwash use and oral and pharyngeal cancer. J. Am. Dent. Assoc. 1985, 110, 731–734. [Google Scholar] [CrossRef] [PubMed]
- Morse, D.E.; Katz, R.V.; Pendrys, D.G.; Holford, T.R.; Krutchkoff, D.J.; Eisenberg, E.; Kosis, D.L.; Kerpel, S.; Freedman, P.; Mayne, S.T. Mouthwash use and dentures in relation to oral epithelial dysplasia. Oral Oncol. 1997, 33, 338–343. [Google Scholar] [CrossRef]
- Talamini, R.; Vaccarella, S.; Barbone, F.; Tavani, A.; La Vecchia, C.; Herrero, R.; Muñoz, N.; Franceschi, S. Oral hygiene, dentition, sexual habits and risk of oral cancer. Br. J. Cancer 2000, 83, 1238–1242. [Google Scholar] [CrossRef] [PubMed]
- Winn, D.M.; Blot, W.J.; McLaughlin, J.K.; Austin, D.F.; Greenberg, R.S.; Preston-Martin, S.; Schoenberg, J.B.; Fraumeni, J.F., Jr. Mouthwash use and oral conditions in the risk of oral and pharyngeal cancer. Cancer Res. 1991, 51, 3044–3047. [Google Scholar]
- Winn, D.M.; Diehl, S.R.; Brown, L.M.; Harty, L.C.; Bravo-Otero, E.; Fraumeni, J.F., Jr.; Kleinman, D.V.; Hayes, R.B. Mouthwash in the etiology of oral cancer in Puerto Rico. Cancer Causes Control 2001, 12, 419–429. [Google Scholar] [CrossRef] [PubMed]
- Wynder, E.L.; Kabat, G.; Rosenberg, S.; Levenstein, M. Oral Cancer and Mouthwash Use. JNCI 1983, 70, 255–260. [Google Scholar]
- Young, T.B.; Ford, C.N.; Brandenburg, J.H. An epidemiologic study of oral cancer in a statewide network. Am. J. Otolaryngol. 1986, 7, 200–208. [Google Scholar] [CrossRef]
- López de Blanc, S.A.; Baruzzi, A.M. Mouthrinses containing alcohol and oral cancer: Revision of epidemiological studies. Braz. Oral Res. 2007, 21, 16–22. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study (Year) | Country | Study Type | Timeframe | Cancer Type | Quality Score | Gender |
|---|---|---|---|---|---|---|
| Ahrens, 2014 [24] | Nine EU countries | Case-control | 2002–2005 | Oral, pharyngeal, laryngeal | 6 | Both |
| Blot, 1983 [25] | US | Case-control | 1975–1978 | Oral, pharyngeal | 6 | Female |
| Boffeta, 2016 [26] | Multiples sites | Case-control | Unspecified | Head and neck, oral cavity, pharyngeal, laryngeal | 4 | Both |
| Chang, 2013 [8] | Taiwan | Case-control | 2010–2012 | Oral, oropharynx, hypopharynx, larynx | 8 | Both |
| D’Souza, 2007 [27] | US | Case-control | 2000–2005 | Oral, pharyngeal | 7 | Both |
| Eliot, 2013 [28] | US | Case-control | 2006–2011 | Head and neck | 7 | Both |
| Garrote, 200 [29] | Cuba | Case-control | 1996–1999 | Oral, oropharynx | 6 | Both |
| Guha, 2007 [30] | Latin America, Eastern Europe | Case-control | 1998–2003 | Oral, pharyngeal | 4 | Both |
| Kabat, 1989 [31] | US | Case-control | 1983–1987 | Oral, pharyngeal | 4 | Female |
| Macfarlane, 2010 [32] | Europe | Case-control | Unspecified | Upper aerodigestive tract | 7 | Both |
| Marques, 2008 [33] | Brazil | Case-control | 1998–2002 | Oral, pharyngeal | 7 | Both |
| Mashberg, 1985 [34] | US | Case-control | 1981–1983 | Oral, pharyngeal | 8 | Both |
| Morse, 1997 [35] | US | Case-control | 1990–1993 | Oral epithelial dysplasia | 6 | Both |
| Talamini, 2000 [36] | Italy | Case-control | 1996–1999 | Oral, pharyngeal | 3 | Both |
| Winn, 1991 [37] | US | Case-control | 1984–1985 | Oral, pharyngeal | 8 | Both |
| Winn, 2001 [38] | US | Case-control | 1992–1995 | Oral, pharyngeal | 8 | Both |
| Wynder, 1983 [39] | US | Case-control | 1977–1980 | Oral, pharyngeal | 7 | Both |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hostiuc, S.; Ionescu, I.V.; Drima, E. Mouthwash Use and the Risk of Oral, Pharyngeal, and Laryngeal Cancer. A Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 8215. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18158215
Hostiuc S, Ionescu IV, Drima E. Mouthwash Use and the Risk of Oral, Pharyngeal, and Laryngeal Cancer. A Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(15):8215. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18158215
Chicago/Turabian StyleHostiuc, Sorin, Ioana Victoria Ionescu, and Eduard Drima. 2021. "Mouthwash Use and the Risk of Oral, Pharyngeal, and Laryngeal Cancer. A Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 15: 8215. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18158215