
Hospital Processes and the Nurse-Patient Interaction in Breast Cancer Care. Findings from a Cross-Sectional Study

 , ,
, ,  and
and
Abstract
:1. Introduction
1.1. Importance of Social Support for Breast Cancer Patients
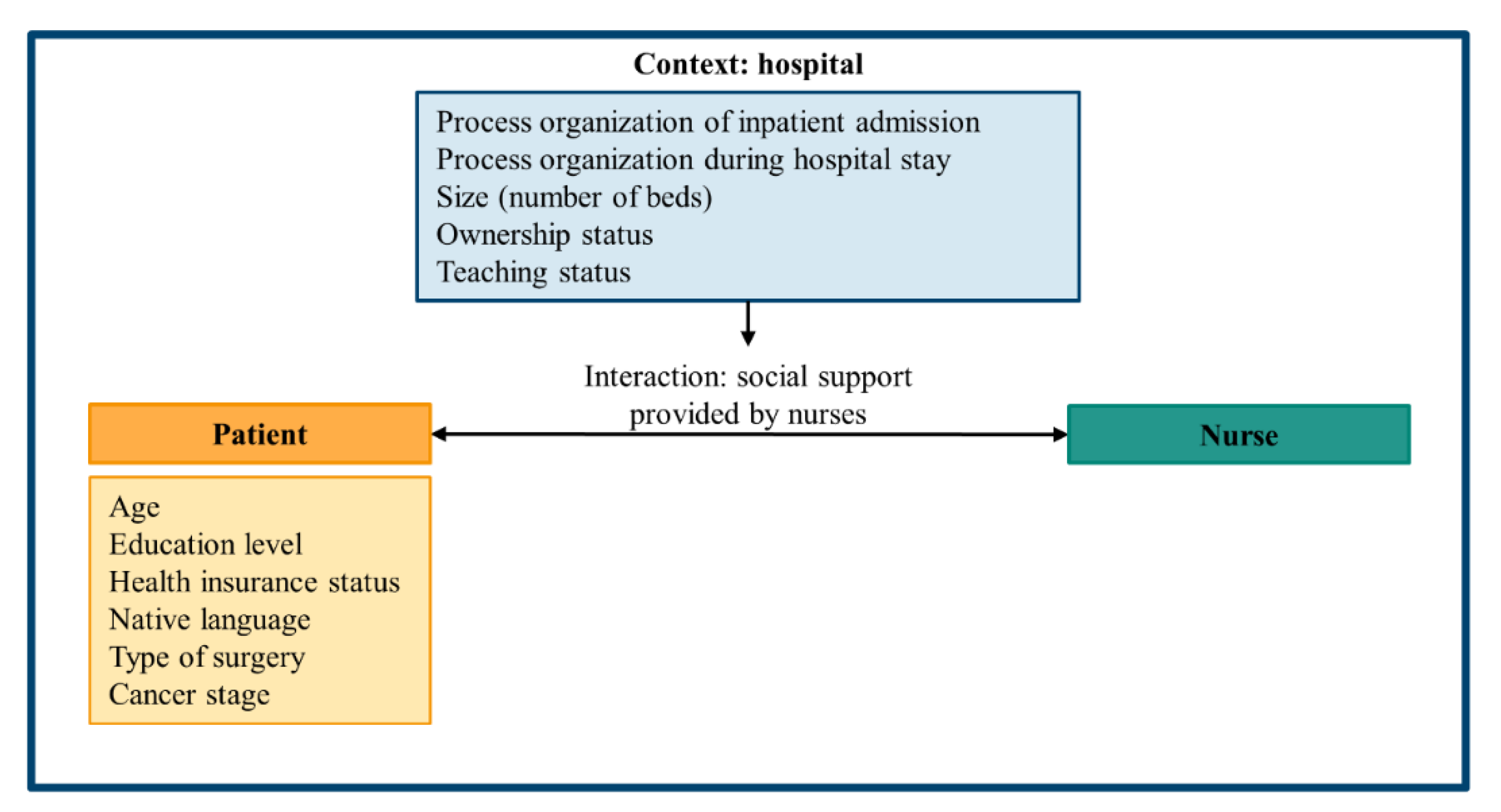
1.2. Association between Organizational Factors and Patient-Provider Interactions
2. Materials and Methods
2.1. Patient Survey
2.1.1. Data Collection
2.1.2. Sample
2.1.3. Instruments
2.2. Structured Quality Reports of the Hospitals
2.3. Data Analysis
2.4. Ethics and Other Permission
3. Results
3.1. Descriptive Results
3.2. Results of Multilevel Analysis
4. Discussion
4.1. Interpretation within the Context of the Wider Literature
4.2. Strengths and Limitations
4.3. Implications for Policy, Practice and Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Cancer: Breast Cancer. Available online: https://www.who.int/cancer/prevention/diagnosis-screening/breast-cancer/en/ (accessed on 27 February 2019).
- Bericht zum Krebsgeschehen in Deutschland 2016. Available online: https://edoc.rki.de/handle/176904/3264 (accessed on 3 August 2021).
- Brustkrebs im Frühen Stadium. Available online: https://www.krebshilfe.de/infomaterial/Patientenleitlinien/Brustkrebs-im-fruehen-Stadium_Patientenleitlinie_DeutscheKrebshilfe.pdf (accessed on 3 August 2021).
- Ansmann, L.; Kowalski, C.; Pfaff, H. Ten Years of Patient Surveys in Accredited Breast Centers in North Rhine-Westphalia. Geburtshilfe Frauenheilkd. 2016, 76, 37–45. [Google Scholar] [CrossRef] [Green Version]
- Mehnert, A.; Hartung, T.J.; Friedrich, M.; Vehling, S.; Brähler, E.; Härter, M.; Keller, M.; Schulz, H.; Wegscheider, K.; Weis, J.; et al. One in two cancer patients is significantly distressed: Prevalence and indicators of distress. Psychooncology 2018, 27, 75–82. [Google Scholar] [CrossRef]
- Mishra, V.S.; Saranath, D. Association between demographic features and perceived social support in the mental adjustment to breast cancer. Psychooncology 2019, 28, 629–634. [Google Scholar] [CrossRef]
- Gil-González, I.; Martín-Rodríguez, A.; Conrad, R.; Pérez-San-Gregorio, M.Á. Quality of life in adults with multiple sclerosis: A systematic review. BMJ Open 2020, 10, e041249. [Google Scholar] [CrossRef]
- Gariépy, G.; Honkaniemi, H.; Quesnel-Vallée, A. Social support and protection from depression: Systematic review of current findings in Western countries. Br. J. Psychiatry 2016, 209, 284–293. [Google Scholar] [CrossRef]
- Wang, H.-H.; Wu, S.-Z.; Liu, Y.-Y. Association Between Social Support and Health Outcomes: A Meta-analysis. Kaohsiung J. Med Sci. 2003, 19, 345–350. [Google Scholar] [CrossRef] [Green Version]
- Ho, P.J.; Gernaat, S.A.M.; Hartman, M.; Verkooijen, H.M. Health-related quality of life in Asian patients with breast cancer: A systematic review. BMJ Open 2018, 8, e02051. [Google Scholar] [CrossRef] [PubMed]
- Arora, N.K.; Finney Rutten, L.J.; Gustafson, D.H.; Moser, R.; Hawkins, R.P. Perceived helpfulness and impact of social support provided by family, friends, and health care providers to women newly diagnosed with breast cancer. Psychooncology 2007, 16, 474–486. [Google Scholar] [CrossRef] [PubMed]
- Luszczynska, A.; Pawlowska, I.; Cieslak, R.; Knoll, N.; Scholz, U. Social support and quality of life among lung cancer patients: A systematic review. Psychooncology 2013, 22, 2160–2168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caplan, G. Support Systems and Community Mental Health: Lectures on Concept Development; Behavioral Publications: Pasadena, CA, US, 1974. [Google Scholar]
- Kaplan, H.B. Health, disease, and the social structure. In Handbook of Medical Sociology; Freeman, H.E., Levine, S., Eds.; Prentice Hall: Englewood Cliffs, NJ, USA, 1989; pp. 46–68. [Google Scholar]
- Bultz, B.D. Cancer Care and the Role of Psychosocial Oncology: Where are We and Where are We Going? Asia Pac. J. Oncol. Nurs. 2016, 3, 118–120. [Google Scholar] [PubMed]
- Cook, O.; McIntyre, M.; Recoche, K.; Lee, S. Experiences of gynecological cancer patients receiving care from specialist nurses: A qualitative systematic review. JBI Database Syst. Rev. Implement. Rep. 2017, 15, 2087–2112. [Google Scholar] [CrossRef]
- Evans, E.C. Exploring the Nuances of Nurse-Patient Interaction through Concept Analysis: Impact on Patient Satisfaction. Nurs. Sci. Q. 2016, 29, 62–70. [Google Scholar] [CrossRef]
- Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century; Institute of Medicine: Washington, DC, USA, 2001; ISBN 0309072808. [Google Scholar]
- Engineer, L.D.; Winters, B.D.; Weston, C.M.; Zhang, A.; Sharma, R.; Bass, E.; Jones, D.; Rosen, A.; Yoon, F.B.; Borzecki, A.; et al. Hospital Characteristics and the Agency for Healthcare Research and Quality Inpatient Quality Indicators: A Systematic Review. J. Healthc. Qual. 2016, 38, 304–313. [Google Scholar] [CrossRef]
- Wiechula, R.; Conroy, T.; Kitson, A.L.; Marshall, R.J.; Whitaker, N.; Rasmussen, P. Umbrella review of the evidence: What factors influence the caring relationship between a nurse and patient? J. Adv. Nurs. 2016, 72, 723–734. [Google Scholar] [CrossRef]
- Olds, D.M.; Aiken, L.H.; Cimiotti, J.P.; Lake, E.T. Association of Nurse Work Environment and Safety Climate on Patient Mortality: A Cross-sectional Study. Int. J. Nurs. Stud. 2017, 74, 155–161. [Google Scholar] [CrossRef]
- Ansmann, L.; Kowalski, C.; Ernstmann, N.; Ommen, O.; Jung, J.; Visser, A.; Pfaff, H. Do breast cancer patients receive less support from physicians in German hospitals with high physician workload? A multilevel analysis. Patient Educ. Couns. 2013, 93, 327–334. [Google Scholar] [CrossRef]
- Ansmann, L.; Wirtz, M.; Kowalski, C.; Pfaff, H.; Visser, A.; Ernstmann, N. The impact of the hospital work environment on social support from physicians in breast cancer care. Patient Educ. Couns. 2014, 96, 352–360. [Google Scholar] [CrossRef]
- Ansmann, L.; Kowalski, C.; Ernstmann, N.; Ommen, O.; Pfaff, H. Patients’ perceived support from physicians and the role of hospital characteristics. Int. J. Qual. Health Care 2012, 24, 501–508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norouzinia, R.; Aghabarari, M.; Shiri, M.; Karimi, M.; Samami, E. Communication Barriers Perceived by Nurses and Patients. Glob. J. Health Sci. 2015, 8, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Dilworth, S.; Higgins, I.; Parker, V.; Kelly, B.; Turner, J. Patient and health professional’s perceived barriers to the delivery of psychosocial care to adults with cancer: A systematic review. Psychooncology 2014, 23, 601–612. [Google Scholar] [CrossRef] [PubMed]
- Bumb, M.; Keefe, J.; Miller, L.; Overcash, J. Breaking Bad News: An Evidence-Based Review of Communication Models for Oncology Nurses. Clin. J. Oncol. Nurs. 2017, 21, 573–580. [Google Scholar] [CrossRef] [PubMed]
- Feldman-Stewart, D.; Brundage, M.D.; Tishelman, C. A conceptual framework for patient-professional communication: An application to the cancer context. Psychooncology 2005, 14, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Dillman, D.A. Mail and telephone surveys: The total design method; Wiley: New York, NY, USA, 1978. [Google Scholar]
- MacCallum, R.C.; Zhang, S.; Preacher, K.J.; Rucker, D.D. On the practice of dichotomization of quantitative variables. Psychol. Methods 2002, 7, 19–40. [Google Scholar] [CrossRef] [PubMed]
- Hox, J.J.; Moerbeek, M.; Van de Schoot, R. Multilevel Analysis: Techniques and Applications, 3rd ed.; Routledge Taylor & Francis Group: New York, NY, USA; London, UK, 2018; ISBN 9781315650982. [Google Scholar]
- Lüdtke, O.; Marsh, H.W.; Robitzsch, A.; Trautwein, U.; Asparouhov, T.; Muthén, B. The multilevel latent covariate model: A new, more reliable approach to group-level effects in contextual studies. Psychol. Methods 2008, 13, 203–229. [Google Scholar] [CrossRef] [Green Version]
- Puts, M.T.E.; Papoutsis, A.; Springall, E.; Tourangeau, A.E. A systematic review of unmet needs of newly diagnosed older cancer patients undergoing active cancer treatment. Support. Care Cancer 2012, 20, 1377–1394. [Google Scholar] [CrossRef] [PubMed]
- Kowalski, C.; Diener, S.E.; Steffen, P.; Wuerstlein, R.; Harbeck, N.; Pfaff, H. Associations between hospital and patient characteristics and breast cancer patients’ satisfaction with nursing staff. Cancer Nurs. 2012, 35, 221–228. [Google Scholar] [CrossRef]
- Sen, S.; Soulos, P.R.; Herrin, J.; Roberts, K.B.; Yu, J.B.; Lesnikoski, B.-A.; Ross, J.S.; Krumholz, H.M.; Gross, C.P. For-profit hospital ownership status and use of brachytherapy after breast-conserving surgery. Surgery 2014, 155, 776–788. [Google Scholar] [CrossRef] [Green Version]
- Leyland, A.H.; Groenewegen, P.P. Multilevel Modelling for Public Health and Health Services Research: Health in Context, 1st ed.; Springer International Publishing: Cham, Switzerland, 2020; p. 286. [Google Scholar]
- Ben Charif, A.; Croteau, J.; Adekpedjou, R.; Zomahoun, H.T.V.; Adisso, E.L.; Légaré, F. Implementation Research on Shared Decision Making in Primary Care: Inventory of Intracluster Correlation Coefficients. Med. Decis. Making 2019, 39, 661–672. [Google Scholar] [CrossRef]
- Selby, J.V.; Schmittdiel, J.A.; Lee, J.; Fung, V.; Thomas, S.; Smider, N.; Crosson, F.J.; Hsu, J.; Fireman, B. Meaningful variation in performance: What does variation in quality tell us about improving quality? Med. Care 2010, 48, 133–139. [Google Scholar] [CrossRef]
- Manary, M.P.; Boulding, W.; Staelin, R.; Glickman, S.W. The patient experience and health outcomes. N. Engl. J. Med. 2013, 368, 201–203. [Google Scholar] [CrossRef] [Green Version]
- Nowak, M.; Swora, M.; Karbach, U.; Pfaff, H.; Ansmann, L. Associations between hospital structures, processes and patient experiences of preparation for discharge in breast cancer centers: A multilevel analysis. Health Care Manag. Rev. 2021, 46, 98–110. [Google Scholar] [CrossRef] [PubMed]
- Stab, N.; Hacker, W. Participatory redesign of work organisation in hospital nursing: A study of the implementation process. J. Nurs. Manag. 2018, 26, 382–392. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Response Options: Frequency (%) a (n = 2979) | |||||
|---|---|---|---|---|---|
| Item | Item Content | 1 | 2 | 3 | 4 |
| SuPP-N scale | |||||
| suppn1 | I could rely on the nurses when I had problems with my illness. | 15 (0.5) | 90 (3.0) | 625 (21.0) | 2249 (75.5) |
| suppn2 | The nurses supported me in a way that made it easier for me to deal with my illness. | 21 (0.7) | 125 (4.2) | 707 (23.7) | 2126 (71.4) |
| suppn3 | The nurses were willing to listen to my illness-related problems. | 38 (1.3) | 175 (5.9) | 787 (26.4) | 1979 (66.4) |
| Process Organization of Inpatient Admission | |||||
| 1 | The patient admission was easy to find. | 15 (0.5) | 75 (2.5) | 575 (19.3) | 2314 (77.7) |
| 2 | The waiting time at the admission was short. | 90 (3.0) | 281 (9.4) | 807 (27.1) | 1801 (60.5) |
| 3 | The admission forms were understandable. | 13 (0.4) | 54 (1.8) | 722 (24.2) | 2190 (73.5) |
| 4 | The admission process was quick. | 50 (1.7) | 159 (5.3) | 660 (22.2) | 2110 (70.8) |
| Process Organization during the Hospital Stay | |||||
| 1 | On the day of my admission there were organizational problems. | 2085 (70.0) | 516 (17.3) | 249 (8.4) | 129 (4.3) |
| 2 | Here at the hospital, the right hand sometimes didn’t know what the left hand was doing. | 2059 (69.1) | 661 (22.2) | 192 (6.4) | 67 (2.2) |
| 3 | There were often waiting times for the examinations or procedures. | 1385 (46.5) | 937 (31.5) | 516 (17.3) | 141 (4.7) |
| 4 | Examinations and procedures were sometimes rescheduled. | 1918 (64.4) | 690 (23.2) | 264 (8.9) | 107 (3.6) |
| 5 | I had the impression, that there were coordination difficulties between the ward and the diagnostical examination units. | 2032 (68.2) | 678 (22.8) | 194 (6.5) | 75 (2.5) |
| 6 | I had the impression that, there were coordination difficulties between doctors and nurses. | 2168 (72.8) | 651 (21.9) | 112 (3.8) | 48 (1.6) |
| Variable | Response Trait | n (%) |
|---|---|---|
| UICC Staging | 0 | 318 (10.7) |
| I | 1175 (39.4) | |
| II | 781 (26.2) | |
| III | 235 (7.9) | |
| IV | 99 (3.3) | |
| Missing | 371 (12.5) | |
| Neoadjuvant Chemotherapy | Yes | 330 (11.1) |
| No | 2619 (87.9) | |
| Missing | 30 (1.0) | |
| Type of surgery | Breast-conserving surgery | 2166 (72.7) |
| Mastectomy | 705 (23.6) | |
| Missing | 108 (3.6) | |
| ASA | 1 | 1434 (48.1) |
| 2 | 1105 (37.1) | |
| 3 and 4 | 249 (8.4) | |
| Missing | 191 (6.4) | |
| Age | 18–39 | 122 (4.1) |
| 40–49 | 547 (18.4) | |
| 50–59 | 932 (31.3) | |
| 60–69 | 810 (27.2) | |
| 70–79 | 452 (15.2) | |
| ≥80 | 101 (3.4) | |
| Missing | 15 (0.5) | |
| Highest educational level | Without lower secondary school education | 51 (1.7) |
| Lower secondary school education | 1148 (38.5) | |
| Intermediate secondary school education | 864 (29.0) | |
| university entrance qualification | 849 (28.5) | |
| Missing | 67 (2.2) | |
| Native language | German | 2795 (93.8) |
| Other | 184 (6.2) | |
| Missing | 32 (1.1) | |
| Health insurance status | Public | 2087 (70.1) |
| Public with additional private insurance | 489 (16.4) | |
| Private | 355 (11.9) | |
| Missing | 48 (1.6) | |
| Variable | Scale format | Mean (SD); min-max |
| Perceived social support | Scale from 1 to 4 | 3.65 (0.55); 1–4 |
| Process organization of inpatient admission | Scale from 1 to 4 | 3.63 (0.50); 1–4 |
| Process organization during hospital stay | Scale from 1 to 4 | 3.50 (0.59); 1–4 |
| Variable | Response Trait | n (%) |
|---|---|---|
| Teaching status | Non-teaching hospital | 14 (16.9) |
| Academic teaching hospital | 64 (77.1) | |
| University hospital | 5 (6.0) | |
| Hospital ownership status | For-profit ownership | 6 (7.2) |
| Public ownership | 17 (20.5) | |
| Charitable ownership | 60 (72.3) | |
| Minimum/Maximum | Mean (SD) | |
| Hospital size (number of beds) | 43/1422 | 526 (284) |
| Model 1 | Model 2 | Model 3 | ||
|---|---|---|---|---|
| Patient Level | OR (95%-CI) | OR (95%-CI) | OR (95%-CI) | |
| UICC Staging (ref. Stage 0) | Stage 1 | 1.05 (0.85; 1.30) | 1.05 (0.85; 1.29) | 1.02 (0.82; 1.28) |
| Stage 2 | 1.17 (0.94; 1.45) | 1.18 (0.95; 1.46) | 1.25 (0.98; 1.59) | |
| Stage 3 | 1.09 (0.75; 1.57) | 1.09 (0.76; 1.57) | 1.06 (0.73; 1.56) | |
| Stage 4 | 1.17 (0.72; 1.88) | 1.16 (0.72; 1.88) | 1.09 (0.69; 1.71) | |
| Age (ref. 50–59) | 18–39 | 1.24 (0.83; 1.86) | 1.25 (0.84; 1.87) | 1.44 (0.95; 2.20) |
| 40–49 | 1.07 (0.87; 1.32) | 1.07 (0.87; 1.32) | 1.10 (0.87; 1.36) | |
| 60–69 | 1.25 (1.02, 1.52) | 1.25 (1.03; 1.52) | 1.28 (1.03; 1.60) | |
| 70–79 | 0.96 (0.75; 1.22) | 0.96 (0.75; 1.23) | 0.88 (0.67; 1.16) | |
| Older than 79 | 1.27 (0.90; 1.81) | 1.28 (0.90; 1.82) | 1.27 (0.90; 1.79) | |
| Neoadjuvant chemotherapy (ref. no) | yes | 0.93 (0.75; 1.15) | 0.92 (0.75; 1.14) | 0.86 (0.69; 1.08) |
| Type of surgery (ref. mastectomy without reconstruction) | Mastectomy with reconstruction | 0.97 (0.74; 1.27) | 0.96 (0.73; 1.26) | 0.95 (0.70; 1.30) |
| Breast-conserving therapy | 1.05 (0.86; 1.29) | 1.05 (0.86; 1.28) | 1.05 (0.85; 1.31) | |
| ASA classification (ref. ASA 1) | ASA 2 | 1.08 (0.94; 1.25) | 1.08 (0.94; 1.24) | 1.10 (0.95; 1.27) |
| ASA 3 and 4 | 0.81 (0.59; 1.11) | 0.80 (0.59; 1.10) | 0.94 (0.65; 1.37) | |
| Highest educational level (ref. Lower secondary school education) | Without lower secondary school education | 0.59 (0.34; 1.00) | 0.58 (0.34; 1.00) | 0.64 (0.37; 1.13) |
| Intermediate secondary school education | 0.93 (0.70; 1.08) | 0.93 (0.79; 1.08) | 0.90 (0.75; 1.08) | |
| university entrance qualification | 0.85 (0.73; 0.99) | 0.86 (0.74; 1.00) | 0.82 (0.98; 1.15) | |
| Native language (ref. other) | German | 1.23 (0.96; 1.56) | 1.23 (0.96; 1.56) | 1.32 (1.01; 1.72) |
| Insurance status (ref. private) | Public | 1.22 (1.00; 1.51) | 1.22 (1.00; 1.51) | 1.29 (1.02; 1.62) |
| Public with additional private insurance | 1.06 (0.81; 1.40) | 1.07 (0.81; 1.40) | 0.99 (0.74; 1.32) | |
| Process organization of inpatient admission | 2.15 (1.79; 2.58) | |||
| Process organization during hospital stay | 2.81 (2.41; 3.29) | |||
| Hospital level | OR (95%-CI) | OR (95%-CI) | ||
| Hospital size (number of beds) | 1.00 (0.99; 1.00) | 1.00 (0.99; 1.00) | ||
| Teaching status (ref. non-teaching) | academic educational hospital | 1.21 (0.94; 1.56) | 1.01 (0.76; 1.34) | |
| university hospital | 0.60 (0.72; 2.80) | 1.41 (0.67; 2.97) | ||
| Hospital ownership (ref. public) | Charitable | 1.08 (0.84; 1.40) | 1.01 (0.79; 1.28) | |
| For-profit | 1.31 (0.96; 1.79) | 1.41 (1.02; 1.93) | ||
| Process organization of inpatient admission | 3.61 (1.67; 7.78) | |||
| Process organization during hospital stay | 2.11 (1.04; 4.29) | |||
| ICC (nullmodel = 0.021) | 0.021 | 0.018 | 0.009 | |
| R² Level 2 | 0.0% | 14.3% | 57.1% | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lubasch, J.S.; Lee, S.; Kowalski, C.; Beckmann, M.; Pfaff, H.; Ansmann, L. Hospital Processes and the Nurse-Patient Interaction in Breast Cancer Care. Findings from a Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 8224. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18158224
Lubasch JS, Lee S, Kowalski C, Beckmann M, Pfaff H, Ansmann L. Hospital Processes and the Nurse-Patient Interaction in Breast Cancer Care. Findings from a Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2021; 18(15):8224. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18158224
Chicago/Turabian StyleLubasch, Johanna Sophie, Susan Lee, Christoph Kowalski, Marina Beckmann, Holger Pfaff, and Lena Ansmann. 2021. "Hospital Processes and the Nurse-Patient Interaction in Breast Cancer Care. Findings from a Cross-Sectional Study" International Journal of Environmental Research and Public Health 18, no. 15: 8224. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18158224