
Occupational Risk Factors and Hypertensive Disorders in Pregnancy: A Systematic Review


Abstract
:1. Introduction
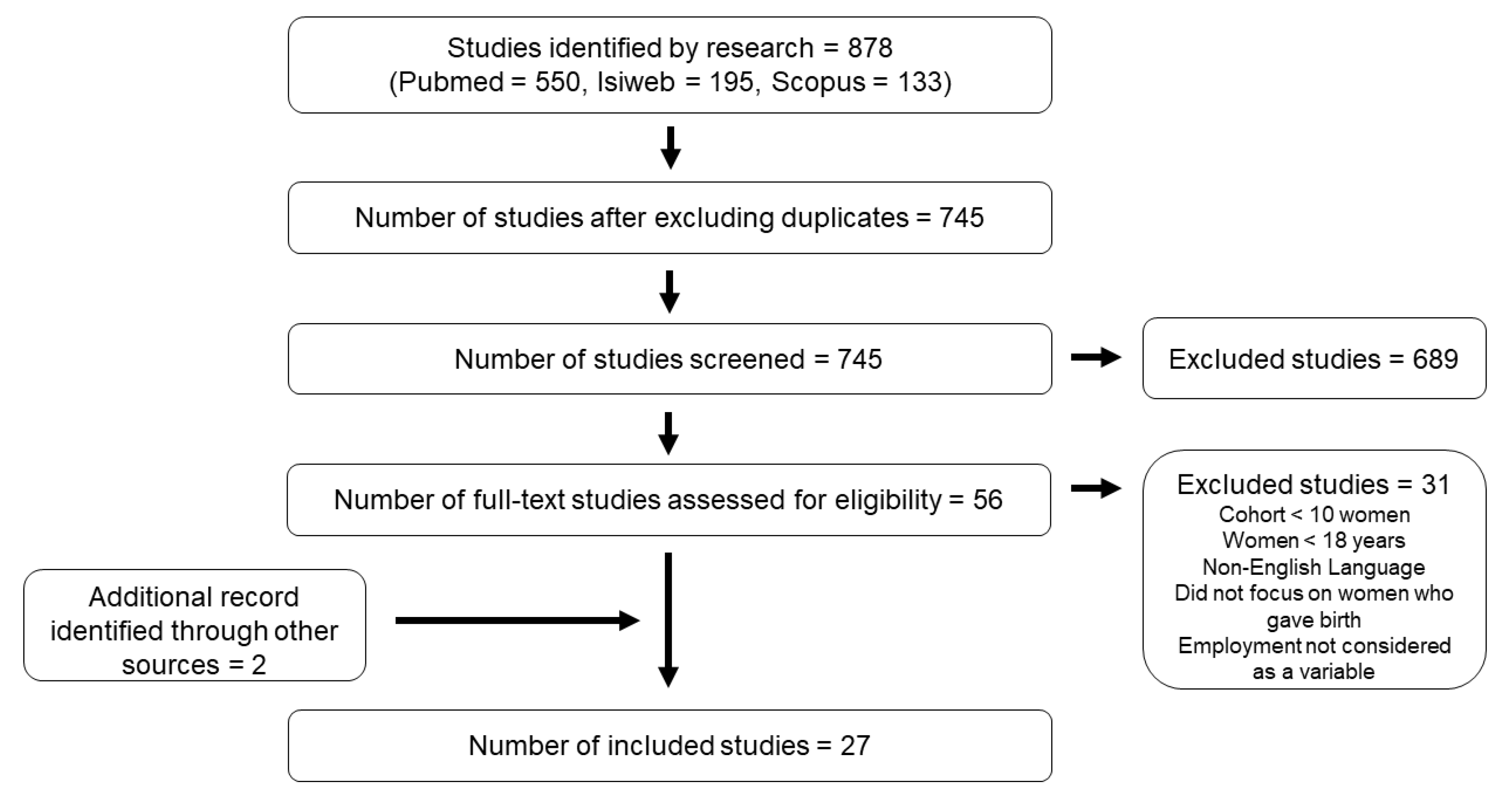
2. Materials and Methods
3. Results
3.1. Work during Pregnancy and HDP
3.2. Occupational Risk Factors and HDP
3.2.1. Biological Risk Factors
3.2.2. Chemical Risk Factors
3.2.3. Physical Risk Factors
3.2.4. Physical Workload
3.2.5. Shift and Night Shift Work
3.2.6. Job Related Stress
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Burton, G.J.; Redman, C.W.; Roberts, J.M.; Moffett, A. Pre-eclampsia: Pathophysiology and clinical implications. BMJ 2019, 366, l2381. [Google Scholar] [CrossRef] [Green Version]
- American College of Obstetricians and Gynecologists. Gestational Hypertension and Preeclampsia: ACOG Practice Bulletin, Number 222. Obstet Gynecol. 2020, 135, e237–e260. [Google Scholar] [CrossRef]
- Chappell, L.C.; Cluver, C.A.; Kingdom, J.; Tong, S. Pre-eclampsia. Lancet 2021, 398, 341–354. [Google Scholar] [CrossRef]
- Brown, M.A.; Magee, L.A.; Kenny, L.C.; Karumanchi, S.A.; McCarthy, F.P.; Saito, S.; Hall, D.R.; Warren, C.E.; Adoyi, G.; Ishaku, S.; et al. Hypertensive Disorders of Pregnancy: ISSHP Classification, Diagnosis, and Management Recommendations for International Practice. Hypertension 2018, 72, 24–43. [Google Scholar] [CrossRef] [Green Version]
- Rana, S.; Lemoine, E.; Granger, J.P.; Karumanchi, S.A. Preeclampsia: Pathophysiology, Challenges, and Perspectives. Circ. Res. 2019, 124, 1094–1112. [Google Scholar] [CrossRef]
- Kintiraki, E.; Papakatsika, S.; Kotronis, G.; Goulis, D.G.; Kotsis, V. Pregnancy-Induced hypertension. Hormones 2015, 14, 211–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO World Health Organization. WHO Recommendations for Prevention and Treatment of Pre-Eclampsia and Eclampsia; WHO: Geneva, Switzerland, 2011; p. 38. [Google Scholar]
- Sibai, B.; Dekker, G.; Kupferminc, M. Pre-eclampsia. Lancet 2005, 365, 785–799. [Google Scholar] [CrossRef]
- Roberts, J. Preeclampsia: A Two Stage Disorder; RCOG Press: London, UK, 2003; pp. 66–78. [Google Scholar]
- Villar, J.; Carroli, G.; Wojdyla, D.; Abalos, E.; Giordano, D.; Baaqeel, H.; Farnot, U.; Bergsjø, P.; Bakketeig, L.; Lumbiganon, P.; et al. Preeclampsia, gestational hypertension and intrauterine growth restriction, related or independent conditions? Am. J. Obstet. Gynecol. 2006, 194, 921–931. [Google Scholar] [CrossRef]
- Mongraw-Chaffin, M.L.; Cirillo, P.M.; Cohn, B.A. Preeclampsia and cardiovascular disease death: Prospective evidence from the child health and development studies cohort. Hypertension 2010, 56, 166–171. [Google Scholar] [CrossRef] [Green Version]
- Umesawa, M.; Kobashi, G. Epidemiology of hypertensive disorders in pregnancy: Prevalence, risk factors, predictors and prognosis. Hypertens. Res. 2017, 40, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Ying, W.; Catov, J.M.; Ouyang, P. Hypertensive Disorders of Pregnancy and Future Maternal Cardiovascular Risk. J. Am. Heart Assoc. 2018, 7, e009382. [Google Scholar] [CrossRef] [PubMed]
- Xiong, T.; Chen, P.; Mu, Y.; Li, X.; Di, B.; Li, J.; Qu, Y.; Tang, J.; Liang, J.; Mu, D. Association between ambient temperature and hypertensive disorders in pregnancy in China. Nat. Commun. 2020, 11, 2925. [Google Scholar] [CrossRef] [PubMed]
- Assibey-Mensah, V.; Glantz, J.C.; Hopke, P.K.; Jusko, T.A.; Thevenet-Morrison, K.; Chalupa, D.; Rich, D.Q. Wintertime Wood Smoke, Traffic Particle Pollution, and Preeclampsia. Hypertension 2020, 75, 851–858. [Google Scholar] [CrossRef]
- Su, X.; Zhao, Y.; Yang, Y.; Hua, J. Correlation between exposure to fine particulate matter and hypertensive disorders of pregnancy in Shanghai, China. Environ. Health 2020, 19, 101. [Google Scholar] [CrossRef]
- Wei, J.; Liu, C.-X.; Gong, T.-T.; Wu, Q.-J.; Wu, L. Cigarette smoking during pregnancy and preeclampsia risk: A systematic review and meta-analysis of prospective studies. Oncotarget 2015, 6, 43667–43678. [Google Scholar] [CrossRef] [PubMed]
- Kawashima, A.; Koide, K.; Hasegawa, J.; Arakaki, T.; Takenaka, S.; Maruyama, D.; Matsuoka, R.; Sekizawa, A. Maternal Smoking History Enhances the Expression of Placental Growth Factor in Invasive Trophoblasts at Early Gestation Despite Cessation of Smoking. PLoS ONE 2015, 10, e0134181. [Google Scholar] [CrossRef]
- López-Jaramillo, P. Calcium, nitric oxide, and preeclampsia. Semin. Perinatol. 2000, 24, 33–36. [Google Scholar] [CrossRef]
- Duvekot, E.J.; De Groot, C.J.; Bloemenkamp, K.W.; Oei, S. Pregnant women with a low milk intake have an increased risk of developing preeclampsia. Eur. J. Obstet. Gynecol. Reprod. Biol. 2002, 105, 11–14. [Google Scholar] [CrossRef]
- Rolfo, A.; Nuzzo, A.; De Amicis, R.; Moretti, L.; Bertoli, S.; Leone, A. Fetal–Maternal Exposure to Endocrine Disruptors: Correlation with Diet Intake and Pregnancy Outcomes. Nutrients 2020, 12, 1744. [Google Scholar] [CrossRef]
- Ye, Y.; Tang, Y.; Xiong, Y.; Feng, L.; Li, X. Bisphenol A exposure alters placentation and causes preeclampsia-like features in pregnant mice involved in reprogramming of DNA methylation ofWNT2. FASEB J. 2019, 33, 2732–2742. [Google Scholar] [CrossRef] [Green Version]
- Cai, C.; Vandermeer, B.; Khurana, R.; Nerenberg, K.; Featherstone, R.; Sebastianski, M.; Davenport, M.H. The impact of occupational shift work and working hours during pregnancy on health outcomes: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2019, 221, 563–576. [Google Scholar] [CrossRef]
- Agrawal, A.; Wenger, N.K. Hypertension during Pregnancy. Curr. Hypertens. Rep. 2020, 22, 64. [Google Scholar] [CrossRef]
- Johnson, T. Maternity Leave and Employment Patterns: 2001–2003; Current Population Report; US Census Bureau: Washington, DC, USA, 2007; pp. 70–113.
- Gabbe, S.G.; Turner, L. Reproductive hazards of the American lifestyle: Work during pregnancy. Am. J. Obstet. Gynecol. 1997, 176, 826–832. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landsbergis, P.A.; Hatch, M.C. Psychosocial work stress and pregnancy-induced hypertension. Epidemiology 1996, 7, 346–351. [Google Scholar] [CrossRef]
- Klonoff-Cohen, H.S.; Cross, J.L.; Pieper, C.F. Job stress and preeclampsia. Epidemiology 1996, 7, 245–249. [Google Scholar] [CrossRef]
- Higgins, J.R.; Walshe, J.J.; Conroy, R.M.; Darling, M.R. The relation between maternal work, ambulatory blood pressure, and pregnancy hypertension. J. Epidemiol. Community Health 2002, 56, 389–393. [Google Scholar] [CrossRef] [Green Version]
- Nugteren, J.J.; Snijder, C.A.; Hofman, A.; Jaddoe, V.W.; Steegers, E.A.; Burdorf, A. Work-related maternal risk factors and the risk of pregnancy induced hypertension and preeclampsia during pregnancy. The Generation R Study. PLoS ONE 2012, 7, e39263. [Google Scholar] [CrossRef]
- Spracklen, C.N.; Ryckman, K.K.; Triche, E.W.; Saftlas, A.F. Physical Activity During Pregnancy and Subsequent Risk of Preeclampsia and Gestational Hypertension: A Case Control Study. Matern. Child Health J. 2016, 20, 1193–1202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eiríksdóttir, V.H.; Valdimarsdóttir, U.A.; Ásgeirsdóttir, T.L.; Hauksdóttir, A.; Lund, S.H.; Bjarnadóttir, R.I.; Cnattingius, S.; Zoëga, H. Pregnancy-Induced Hypertensive Disorders before and after a National Economic Collapse: A Population Based Cohort Study. PLoS ONE 2015, 10, e0138534. [Google Scholar] [CrossRef] [PubMed]
- Haelterman, E.; Marcoux, S.; Croteau, A.; Dramaix, M. Population-based study on occupational risk factors for preeclampsia and gestational hypertension. Scand. J. Work. Environ. Health 2007, 33, 304–317. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saftlas, A.F.; Logsden-Sackett, N.; Wang, W.; Woolson, R.; Bracken, M.B. Work, Leisure-Time Physical Activity, and Risk of Preeclampsia and Gestational Hypertension. Am. J. Epidemiol. 2004, 160, 758–765. [Google Scholar] [CrossRef]
- Chang, P.-J.; Chu, L.-C.; Hsieh, W.-S.; Chuang, Y.-L.; Lin, S.-J.; Chen, P.-C. Working hours and risk of gestational hypertension and pre-eclampsia. Occup. Med. 2009, 60, 66–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bilhartz, T.D.; Bilhartz, P. Occupation as a Risk Factor for Hypertensive Disorders of Pregnancy. J. Women Health 2013, 22, 188a–188i. [Google Scholar] [CrossRef]
- Spinillo, A.; Capuzzo, E.; Colonna, L.; Piazzi, G.; Nicola, S.; Baltaro, F. The Effect of Work Activity in Pregnancy on the Risk of Severe Preeclampsia. Aust. N. Z. J. Obstet. Gynaecol. 1995, 35, 380–385. [Google Scholar] [CrossRef]
- Cerón-Mireles, P.; Harlow, S.; Sánchez-Carrillo, C.; Núñez, R. Risk factors for pre-eclampsia/eclampsia among working women in Mexico City. Paediatr. Perinat. Epidemiol. 2001, 15, 40–46. [Google Scholar] [CrossRef] [Green Version]
- Rustveld, L.O.; Kelsey, S.F.; Sharma, R. Association Between Maternal Infections and Preeclampsia: A Systematic Review of Epidemiologic Studies. Matern. Child Health J. 2007, 12, 223–242. [Google Scholar] [CrossRef]
- Üstün, Y.; Engin-Ustun, Y.; Ozkaplan, E.; Otlu, B.; Tekerekoglu, M.S. Association of Helicobacter pylori infection with systemic inflammation in preeclampsia. J. Matern. Neonatal Med. 2009, 23, 311–314. [Google Scholar] [CrossRef] [PubMed]
- Strand, K.; Odland, M.; Iversen, A.-C.; Nordbø, S.; Vik, T.; Austgulen, R. Cytomegalovirus antibody status at 17–18 weeks of gestation and pre-eclampsia: A case-control study of pregnant women in Norway. BJOG Int. J. Obstet. Gynaecol. 2012, 119, 1316–1323. [Google Scholar] [CrossRef] [PubMed]
- Sansone, M.; Sarno, L.; Saccone, G.; Berghella, V.; Maruotti, G.; Migliucci, A.; Capone, A.; Martinelli, P. Risk of Preeclampsia in Human Immunodeficiency Virus–Infected Pregnant Women. Obstet. Gynecol. 2016, 127, 1027–1032. [Google Scholar] [CrossRef]
- Eskenazi, B.; Bracken, M.B.; Holford, T.R.; Grady, J. Exposure to Organic Solvents and Hypertensive Disorders of Pregnancy. Am. J. Ind. Med. 1988, 14, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Ledda, C.; Fiore, M.; Santarelli, L.; Bracci, M.; Mascali, G.; D’Agati, M.G.; Busà, A.; Ferrante, M.; Rapisarda, V. Gestational Hypertension and Organophosphorus Pesticide Exposure: A Cross-Sectional Study. BioMed Res. Int. 2015, 2015, 280891. [Google Scholar] [CrossRef] [PubMed]
- Irwin, D.E.; Savitz, D.A.; André, K.A.S.; Hertz-Picciotto, I. Study of occupational risk factors for pregnancy-induced hypertension among active duty enlisted navy personnel. Am. J. Ind. Med. 1994, 25, 349–359. [Google Scholar] [CrossRef]
- Sears, C.G.; Braun, J.M.; Ryan, P.H.; Xu, Y.; Werner, E.F.; Lanphear, B.P.; Wellenius, G.A. The association of traffic-related air and noise pollution with maternal blood pressure and hypertensive disorders of pregnancy in the HOME study cohort. Environ. Int. 2018, 121, 574–581. [Google Scholar] [CrossRef] [PubMed]
- Bendokiene, I.; Grazuleviciene, R.; Dedele, A. Risk of hypertension related to road traffic noise among reproductive-age women. Noise Health 2011, 13, 371–377. [Google Scholar] [CrossRef]
- Lissåker, C.T.; Gustavsson, P.; Albin, M.; Ljungman, P.; Bodin, T.; Sjöström, M.; Selander, J. Occupational exposure to noise in relation to pregnancy-related hypertensive disorders and diabetes. Scand. J. Work Environ. Health 2021, 47, 33–41. [Google Scholar] [CrossRef]
- Wergeland, E.; Strand, K. Working conditions and prevalence of pre-eclampsia, Norway 1989. Int. J. Gynecol. Obstet. 1997, 58, 189–196. [Google Scholar] [CrossRef]
- Nurminen, T.; Kurppa, K. Occupational noise exposure and course of pregnancy. Scand. J. Work Environ. Health 1989, 15, 117–124. [Google Scholar] [CrossRef] [Green Version]
- Skröder, H.; Pettersson, H.; Albin, M.; Gustavsson, P.; Rylander, L.; Norlén, F.; Selander, J. Occupational exposure to whole-body vibrations and pregnancy complications: A nationwide cohort study in Sweden. Occup. Environ. Med. 2020, 77, 691–698. [Google Scholar] [CrossRef]
- European Agency for Safety Health and Work. Worplace Exposure to Vibration in Europe: An Expert Review. Available online: https://osha.europa.eu/en/publications/report-workplace-exposure-vibration-europe-expert-review (accessed on 21 May 2021).
- International Labour Office (ILO) Shift Work. Conditions of Work and Employment Programme. Information Sheet No. WT-8 2004. Available online: https://www.ilo.org/wcmsp5/groups/public/---ed_protect/---protrav/---travail/documents/publication/wcms_170713.pdf (accessed on 14 May 2021).
- Your Europe–European Union Working Hours. Available online: https://europa.eu/youreurope/business/human-resources/working-hours-holiday-leave/working-hours/index_en.htm#shortcut-5 (accessed on 14 May 2021).
- Bonzini, M.; Palmer, K.T.; Coggon, D.; Carugno, M.; Cromi, A.; Ferrario, M.M. Shift work and pregnancy outcomes: A systematic review with meta-analysis of currently available epidemiological studies. BJOG Int. J. Obstet. Gynaecol. 2011, 118, 1429–1437. [Google Scholar] [CrossRef] [Green Version]
- Hammer, P.; Flachs, E.; Specht, I.; Pinborg, A.; Petersen, S.; Larsen, A.; Hougaard, K.; Hansen, J.; Hansen, Å.; Kolstad, H.; et al. Night work and hypertensive disorders of pregnancy: A national register-based cohort study. Scand. J. Work Environ. Health 2018, 44, 403–413. [Google Scholar] [CrossRef]
- Suzumori, N.; Ebara, T.; Matsuki, T.; Yamada, Y.; Kato, S.; Omori, T.; Saitoh, S.; Kamijima, M.; Sugiura-Ogasawara, M. The Japan Environment & Children’s Study Group Effects of long working hours and shift work during pregnancy on obstetric and perinatal outcomes: A large prospective cohort study—Japan Environment and Children’s Study. Birth 2019, 47, 67–79. [Google Scholar]
- Davari, M.H.; Naghshineh, E.; Mostaghaci, M.; Mirmohammadi, S.J.; Bahaloo, M.; Jafari, A.; Mehrparvar, A.H. Shift Work Effects and Pregnancy Outcome: A Historical Cohort Study. J. Fam. Reprod. Health 2018, 12, 84–88. [Google Scholar]
- Nurminen, T. Shift work, fetal development and course of pregnancy. Scand. J. Work Environ. Health 1989, 15, 395–403. [Google Scholar] [CrossRef] [Green Version]
- Karasek, R.A., Jr. Job Demands, Job Decision Latitude, and Mental Strain: Implications for Job Redesign. Adm. Sci. Q. 1979, 24, 285–308. [Google Scholar] [CrossRef]
- Marcoux, S.; Bérubé, S.; Brisson, C.; Mondor, M. Job Strain and Pregnancy-Induced Hypertension. Epidemiology 1999, 10, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Anorlu, R.I.; Iwuala, N.C.; Odum, C.U. Risk factors for pre-eclampsia in Lagos, Nigeria. Aust. N. Z. J. Obstet. Gynaecol. 2005, 45, 278–282. [Google Scholar] [CrossRef]
- Vollebregt, K.C.; Van Der Wal, M.F.; Wolf, H.; Vrijkotte, T.G.M.; Boer, K.; Bonsel, G.J. Is psychosocial stress in first ongoing pregnancies associated with pre-eclampsia and gestational hypertension? BJOG Int. J. Obstet. Gynaecol. 2008, 115, 607–615. [Google Scholar] [CrossRef] [PubMed]
- Leeners, B.; Neumaier-Wagner, P.; Kuse, S.; Stiller, R.; Rath, W. Emotional stress and the risk to develop hypertensive diseases in pregnancy. Hypertens. Pregnancy 2007, 26, 211–226. [Google Scholar] [CrossRef] [PubMed]
- Eurostat. Employment and Activity by Sex and Age—Annual Data. Available online: http://ec.europa.eu/eurostat/web/products-datasets/-/lfsi_emp_a) (accessed on 25 May 2021).
- Santos, S.; Voerman, E.; Amiano, P.; Barros, H.; Beilin, L.J.; Bergström, A.; Charles, M.A.; Chatzi, L.; Chevrier, C.; Chrousos, G.P.; et al. Impact of maternal body mass index and gestational weight gain on pregnancy complications: An individual participant data meta-analysis of European, North American and Australian cohorts. BJOG 2019, 126, 984–995. [Google Scholar] [CrossRef]
- Liu, Q.; Shi, J.; Duan, P.; Liu, B.; Li, T.; Wang, C.; Li, H.; Yang, T.; Gan, Y.; Wang, X.; et al. Is shift work associated with a higher risk of overweight or obesity? A systematic review of observational studies with meta-analysis. Int. J. Epidemiol. 2018, 47, 1956–1971. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kongwattanakul, K.; Saksiriwuttho, P.; Chaiyarach, S.; Thepsuthammarat, K. Incidence, characteristics, maternal complications, and perinatal outcomes associated with preeclampsia with severe features and HELLP syndrome. Int. J. Womens Health 2018, 10, 371–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujiwara, K.; Tsukishima, E.; Kasai, S.; Masuchi, A.; Tsutsumi, A.; Kawakami, N.; Miyake, H.; Kishi, R. Urinary catecholamines and salivary cortisol on workdays and days off in relation to job strain among female health care providers. Scand. J. Work Environ. Health 2004, 30, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Katz, V.L.; Jenkins, T.; Haley, L.; Bowes, W.A., Jr. Catecholamine levels in pregnant physicians and nurses: A pilot study of stress and pregnancy. Obstet. Gynecol. 1991, 77, 338–342. [Google Scholar]
- van der Beek, A.J.; Meijman, T.F.; Frings-Dresen, M.H.; Kuiper, J.I.; Kuiper, S. Lorry drivers’ work stress evaluated by catecholamines excreted in urine. Occup. Environ. Med. 1995, 52, 464–469. [Google Scholar] [CrossRef] [Green Version]
- Young, W.F.; Landsberg, L. Catecholemines and the adrenal medulla. In Williams Textbook of Endocrinology; Saunders: Philadelphia, PA, USA, 1998. [Google Scholar]
- Khatun, S.; Kanayama, N.; Hossain, B.; El Maradny, E.; Kobayashi, T.; Jahan, S.; Bhuiyan, A.B.; Terao, T. Increased concentrations of plasma epinephrine and norepinephrine in patients with eclampsia. Eur. J. Obstet. Gynecol. Reprod. Biol. 1997, 74, 103–109. [Google Scholar] [CrossRef]
- Nakamura, H.; Ohsu, W.; Nagase, H.; Okazawa, T.; Yoshida, M.; Okada, A. Uterine circulatory dysfunction induced by whole-body vibration and its endocrine pathogenesis in the pregnant rat. Eur. J. Appl. Physiol. Occup. Physiol. 1996, 72, 292–296. [Google Scholar] [CrossRef]


{kind=link}
| Study Location (Analyzed Period) | Study Design | Population Investigated (Number) and Age | Occupational Risk Factors | Additional Information | Results | Overall Quality | Reference |
|---|---|---|---|---|---|---|---|
| Pennsylvania and New York, USA (1987–1989) | Prospective cohort | 717 women with singleton pregnancies | Employment status | - | Higher risk of GH: All cases among the group who worked during first semester vs. no cases in the unemployed group (lower bound of 95% CI for RR = 1.7). | Good | Landsbergis et al. [29] |
| North Carolina, USA (1984–1987) | Cross sectional | 110 cases of PE vs. 115 controls | Employment status | - | Higher risk of PE:
| Good | Klonoff-Cohen et al. [30] |
| Dublin, Ireland (not specified) | Prospective cohort | 933 primiparas with singleton pregnancies 289 unemployed vs. 245 employed | Employment status | - | Higher risk of PE:
| Good | Higgins et al. [31] |
| Netherlands (2002–2006) | Prospective cohort | 4465 women with singleton pregnancies | Employment status Working hours | Working hours per week: 1–24; 25–39: 40 or more. | Higher risk of GH and PE, although not statistically significant:
| Excellent | Nugteren et al. [32] |
| Iowa, USA (2002–2005) | Cross sectional | 258 primiparous women with PE and 233 primiparous women with GH vs. 182 primiparous normotensive women | Employment status Working hours | Women were asked to report whether or not they worked during pregnancy and the number of hours worked per week. | Lower risk of PE:
| Good | Spracklen et al. [33] |
| Iceland (2005–2012) | Retrospective cohort | 35,211 women with singleton pregnancies | Employment status | Employment status:
| Unemployment led to higher risk of:
| Good | Eiríksdóttir et al. [34] |
| Canada (1997–1999) | Retrospective cohort | 4729 women who delivered singleton births and worked since the first month of pregnancy | Employment status Work schedule | Information on work conditions at the onset of pregnancy was collected. | Higher risk of PE
| Good | Haelterman et al. [35] |
| Connecticut, USA (1988–1991) | Cross sectional | 142 PE and 172 GH vs. 2422 normotensive controls | Employment status Work activity | - | Lower risk of PE, although non-significant:
| Excellent | Saftlas et al. [36] |
| Taiwan (2005) | Retrospective cohort | 20,276 primiparous women with singleton pregnancies | Type of employment | Work schedules subgroups:
| No significant findings between non-employed and different work schedules or working hours in all or primiparous women. | Good | Chang et al. [37] |
| Texas, USA (2005) | Retrospective cohort | 385,537 women who gave birth | Type of work Education | Study limitations: Data obtained by the Texas Electronic Registrar Birth Registration, with self-reported information. | Higher risk of HDP:
| Good | Bilhartz et al. [38] |
| Italy (1990–1994) | Retrospective cohort | 160 women with severe PE vs. 320 normotensive women | Work type | - | Lower risk of PE: Clerical workers (OR 0.53, 95% CI 0.30–0.96) vs. unemployed women; Clerical workers (OR 0.2 95% CI 0.08–0.049) vs. not formally employed women. | Good | Spinillo et al. [39] |
| Mexico City, Mexico (1992) | Retrospective cohort | 2663 women with singleton pregnancies | Socio-economic status Work type Education | Socio-economic status:
| Higher risk of PE:
| Good | Cerón-Mireles et al. [40] |
| Study Location (Analyzed Period) | Study Design | Population Investigated | Occupational Chemical Agents | Additional Information | Results | Overall Quality | Reference |
|---|---|---|---|---|---|---|---|
| Netherlands (2002–2006) | Prospective cohort | 4465 women with singleton pregnancies | Occupational chemical compounds: polycyclic aromatic hydrocarbons (PAHs); pesticides; phthalates; organic solvents; bisphenol A; alkylphenolic compounds; flame retardants; Metals; miscellaneous agents | Job Exposure Matrix (JEM) scores:
| Higher risk of PE in women exposed to pesticides, although not statistically significant (3.15, 95% CI 0.38–25.94) vs. no exposure. | Excellent | Nugteren et al. [32] |
| New Haven, Connecticut, North America (1980–1982) | Prospective cohort | 270 women who delivered at Yale-New Haven Hospital: 90 occupational exposed vs. 180 controls | Solvents | Job Titles: Laboratory workers/technicians (n = 22); artist/art teachers (n = 16); assemblers (n = 13); machine operators/factory workers (n = 5); operating and recovery room personnel (n = 11); electrical and circuit-board workers (n = 5); science teachers (n = 3); chemist/chemical workers (n = 5); layout editors (n = 2). | Higher risk of:
| Good | Eskenazi et al. [45] |
| Sicily, Italy (2007–2013) | Prospective cohort | 2203 women who delivered during the period. 474 occupational exposed vs. 582 not exposed | Organophosphorus pesticides: diazinon; malathion; parathion; chlorpyrifos | Exposure in the first trimester of pregnancy:
| Higher risk of GH: Exposure to diazinon (aOR 1.09, 95% CI 1.03–1.16) and malathion (aOR 1.14, 95% CI 1.08–1.19) vs. no exposure. | Sufficient | Ledda et al. [46] |
| U.S. Navy Personnel (1987–1989) | Retrospective cohort | 5605 women with singleton pregnancies | Hazardous chemical exposure (e.g., organic, metals, etc.) | Exposure to chemical agents classified as:
| No increased risk of HDP due to hazardous chemical exposure in the workplace. | Good | Irwin et al. [47] |
| Study Location (Analyzed Period) | Study Design | Population Investigated | Occupational Risk Factors | Additional Information | Results | Overall Quality | Reference |
|---|---|---|---|---|---|---|---|
| Canada (1997–1999) | Retrospective cohort | 4729 women who delivered singleton births and worked since the first month of pregnancy | WBV Extreme temperatures Noise | WBV: Any exposure Extreme temperatures: always or frequently; rarely or never. Noise: an environment where a person could speak normally (not exposed); or had to speak loudly or shout (exposed) to be heard at 2 m. | WBV: no significantly higher risk of PE in exposed vs. unexposed women (1.2 aOR, 95% CI, 0.6–2.5). Extreme temperatures: higher risk of PE (1.6 aOR, 95% CI, 1.0- 2.6) and GH (1.3 aOR, 95% CI, 0.8–2.2), in women frequently or always exposed to extreme temperatures vs. those rarely or never exposed. Noise: no significant association. | Good | Haelterman et al. [35] |
| U.S. Navy Personnel (1987–1989) | Retrospective cohort | 5605 women with singleton pregnancies | Noise Extreme temperature/humidity | Intensity and duration of noise exposure during a typical working day: High: ≥84 dB(A)/8 h. Medium: >conversation levels. Low: rarely or never > conversation levels. | No association with noise exposure No association with extremes temperatures and humidity. | Good | Irwin et al. [47] |
| Sweden (1994–2014) | Prospective cohort | 1,109,516 working women with singleton pregnancies | Noise | Annual average 8 h occupational exposure levels: 70 dB(A); 70–74 dB(A); 75–80 dB(A); 80–85 dB(A); >85 dB(A). | Noise exposure 80–85 dB(A) both in part-time and full-time employment: Higher risk of HDP (aRR 1.10, 95% CI 1.06–1.44) and PE (aRR 1.11, 95% CI 1.07–1.16) vs. <70 dB(A). Noise exposure 80–85 dB(A) only in full-time employment: Higher risk of HDP (aRR 1.12, 95% CI 1.05–1.18) and PE (aRR 1.14, 95% CI 1.07–1.22) vs. <70 dB(A). No significant association for exposure >85 db(A). | Good | Lissaker et al. [50] |
| Norway (October–November 1989) | Retrospective cohort | 5388 women with singleton pregnancies | Noise | Any exposure. | No association. | Insufficient | Wergeland and Strand. [51] |
| Finland (1976–1985) | Case–control | 1475 mothers from the Finnish Register of Congenital Malformations between June 1976 and December 1985 vs. 1475 controls | Noise and night shift work | Any exposure. No exposure (less than 80 dB(A)). Low intensity (around 80 dB(A)). Moderate (around 85 dB(A)). High intensity (around 90 dB(A)). | Higher risk of GH in exposed mothers compared to unexposed (RR 1.8, 95% CI 1.0–1.3). | Sufficient | Nurminenand Kurppa [52] |
| Sweden (1994–2014) | Prospective cohort | 1,091,044 working women who gave birth between 1994 and 2014 | Whole Body Vibrations (WBV) | Average 8 h occupational exposure levels: High: ≥0.5 m/s2. Medium: 0.3–0.4 m/s2. Low: 0.1–0.2 m/s2. | Higher risk for full-time workers exposed to WBV at levels ≥0.5m/s2:
| Good | Skröder et al. [53] |
| Study Location (Analyzed Period) | Study Design | Population Investigated | Occupational Risk Factors | Additional Information | Results | Overall Quality | Reference |
|---|---|---|---|---|---|---|---|
| Pennsylvania and New York, USA (1987–1989 | Prospective cohort | 717 women with singleton pregnancies | First trimester physical work demands | Assessing Physical Workload score (range 0–980): sum of subjects’ responses to five items (climbing or balancing; lifting, carrying, pulling, or pushing objects; moving around a lot; exerting a lot of physical effort; sitting or standing in uncomfortable positions for long periods of time). | Physical work demands > 200: Lower risk of GH and PE although not statically significant (0.7 OR, 95% CI 0.2–2.5) vs. physical work demands < 200. | Good | Landsbergis et al. [29] |
| Ireland | Prospective cohort | 933 primiparas with singleton pregnancies 289 unemployed vs. 245 employed | Employment Work posture | Work type defined as:
| Higher risk of PE:
| Good | Higgins et al. [31] |
| Netherlands (2002–2006) | Prospective cohort | 4465 women with singleton pregnancies | Physical exertion | Occupational physical exertion:
1–24; 25–39: 40 or more | Higher risk of GH and PE, although not statistically significant:
| Excellent | Nugteren et al. [32] |
| Iowa, USA (2002–2005) | Cross selection | 258 primiparous women with PE and 233 primiparous women with GH vs. 182 primiparous normotensive women | Leisure Time Physical Activity (LTPA) Work schedule Occupational physical exertion Work posture | Occupational risk factor investigated:
| Lower risk of PE:
| Good | Spracklen et al. [33] |
| Canada (1997–1999) | Retrospective cohort | 4729 women who delivered singleton births and worked since the first month of pregnancy | Work posture Physical exertion | Work posture assessed as hours spent:
| Higher risk of PE:
| Good | Haelterman et al. [35] |
| Connecticut, USA (1988–1991) | Cross sectional | 142 PE and 172 GH vs. 2422 normotensive controls | Work schedule Work posture Leisure-Time Physical Activity (LTPA) |
| Lower risk of PE, although non-significant:
| Excellent | Saftlas et al. [36] |
| Italy (1990–1994) | Retrospective cohort | 160 women with severe PE vs. 320 normotensive women | Level of physical activity at work | Level of physical activity at work:
| Higher risk of PE: Moderate/high physical activity at work (OR 2.08, 95% CI 1.11–3.88) vs. mild activity. | Good | Spinillo et al. [39] |
| Mexico (1992) | Retrospective cohort | 2663 women with singleton pregnancies | Work posture Physical activity at work | Hours spent standing and whether the job required physical effort assessed by structured questionnaire. | No association with hour spent standing, having a job which required physical effort. | Good | Cerón-Mireles et al. [40] |
| U.S. Navy Personnel (1987–1989) | Retrospective cohort | 5605 women with singleton pregnancies | Physical job demands | Assessing Physical Workload:
| Higher risk of PE in parous women engaged in the following activities vs. administrative and support jobs:
| Good | Irwin et al. [47] |
| Norway (October–November 1989) | Retrospective cohort | 5388 women with singleton pregnancies | Work posture Physical job demands | Prolonged high physical work:
| Higher risk of PE:
| Insufficient | Wergeland and Strand [51] |
| Study Location (Analyzed Period) | Study Design | Population Investigated | Occupational Risk Factors | Additional Information | Results | Overall Quality | Reference |
|---|---|---|---|---|---|---|---|
| Netherlands (2002–2006) | Prospective cohort | 4465 women with singleton pregnancies | Work schedule | Night shift/month:
| No significant association. | Excellent | Nugteren et al. [32] |
| Canada (1997–1999) | Retrospective cohort | 4729 women who delivered singleton births and worked since the first month of pregnancy | Work schedule | Weekly night work hours (23:00–06:00):
| No significant association. | Good | Haelterman et al. [35] |
| Taiwan (2005) | Retrospective cohort | 20,276 primiparous women with singleton pregnancies | Work schedule Type of employment | Work schedules subgroups:
≤40; 41–48; 49–56; >56 h/week. | No significant findings between non employed and different work schedules or working hours in all or primiparous women. | Good | Chang et al. [37] |
| Norway (October–November 1989) | Retrospective cohort | 5388 women with singleton pregnancies | Work schedule | Not specified. | Higher risk of PE only in parous women (aOR 2.0, 95%CI 1.1–3.6) vs. non-shift workers. | Insufficient | Wergeland and Strand [51] |
| Denmark (2007–2013) | Retrospective cohort | 18,724 primiparous women with singleton pregnancies 11,193 night workers vs. 7531 day workers | Work schedule | Consecutive night shifts categories:
| Higher risk of HDP:
| Good | Hammer et al. [58] |
| Japan (2011–2014) | Prospective cohort | 99,744 women with singleton pregnancies | Work schedule | Workers without night shifts:
| Higher risk of HDP:
| Good | Suzumori et al. [59] |
| Iran (2017) | Retrospective cohort | 429 working women with singleton pregnancies 214 shift workers vs. 215 day workers | Work schedule | Job title:
| Higher risk of PE: Shift workers vs. morning workers (14.5% vs. 7.9%, p = 0.031). Non-significant higher risk of PE: Shift workers vs. morning workers (aOR 1.69, 95% CI 0.8–3.3). | Sufficient | Davari et al. [60] |
| Finland (1976–1985) | Case–control | 1475 mothers from the Finnish Register of Congenital Malformations vs. 1475 controls | Rotating shifts in noisy and noiseless environment |
| Higher risk for GH in shift work in a noisy environment compared to noiseless shift work (aRR 1.9, 95% CI 0.6–2.3) | Sufficient | Nurminen [61] |
| Study Location (Analyzed Period) | Study Design | Population Investigated | Job Related Stress Variables | Additional Information | Results | Overall Quality | Reference |
|---|---|---|---|---|---|---|---|
| Pennsylvania and New York, USA (1987–1989) | Prospective cohort | 717 women with singleton pregnancies | Working hours Job strain Job complexity | Job pressures/low job controls:
| In women with lower-status jobs:
| Good | Landsbergis et al. [29] |
| North Carolina, USA (1984–1987) | Cross sectional | 110 cases of PE vs. 115 controls | Job strain | Job strain categories, by psychological demand and decision latitude:
| Higher risk of PE:
| Good | Klonoff-Cohen et al. [30] |
| Canada (1997–1999) | Retrospective cohort | 4729 women who delivered singleton births and worked since the first month of pregnancy | Job strain Work pace | Forced pace, piece work or assembly-line work Job strain:
| No association to job strain and work pace. | Good | Haelterman et al. [35] |
| Norway (October–November 1989) | Retrospective cohort | 5388 women with singleton pregnancies | Work pace | Work pace:
| Higher risk of PE: Hectic work pace (aOR 1.4, 95% CI 1.0–2.0) vs. no hectic work pace. Lower risk of PE: Influence on work pace (aOR 0.7, 95% CI 1.0–2.0) vs. no influence. | Insufficient | Wergeland and Strand [51] |
| Quebec, Canada (1984–1986) | Cross sectional | 128 PE cases, 201 GH cases vs. 401 normotensive women | Job strain Working hours | Job strain categories, by psychological demand and decision latitude:
| Higher risk of PE:
High psychological demand (aOR 2.1, 95% CI 1.1–3.8) vs. low demand. High job strain (aOR 1.3; 95% CI 0.8–2.2) vs. low job strain. | Good | Marcoux et al. [63] |
| Lagos, Nigeria (2001–2002) | Case–control study | 128 women who delivered during the period and who had PE Vs. 240 controls | Working during pregnancy Stressful work environment | Five-levels activity score based on:
| Higher risk of PE: Women with a stressful work environment during pregnancy (aOR 2.10; 95% CI 1.20–3.71) vs. unexposed controls. No association between working during pregnancy and PE. | Sufficient | Anorlu et al. [64] |
| Amsterdam, Netherlands (2003–2004) | Prospective cohort | 3679 primiparas with singleton pregnancies (128 PE, 161 GH, Vs 3390 controls) | Working Hours Workload Work control Job strain | Weekly working hours: <32, >32 h. Workload: Low: <50th percentile; Moderate: 50th–90th percentile; High > 90th percentile. Work control: High: >50th percentile; Moderate: 10th–50th percentile); Low: <10th percentile. Job strain: Highest: high workload, low work control; High: high workload, low-moderate work control; Low: low workload, high-moderate work control. | No significant association. | Sufficient | Vollebregt et al. [65] |
| Germany (2004–2006) | Cross sectional | 725 cases vs. 880 controls | Emotional stress | Reasons for acute emotional stress, related to job:
| Causes for emotional stress:
| Sufficient | Leeners et al. [66] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Spadarella, E.; Leso, V.; Fontana, L.; Giordano, A.; Iavicoli, I. Occupational Risk Factors and Hypertensive Disorders in Pregnancy: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 8277. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168277
Spadarella E, Leso V, Fontana L, Giordano A, Iavicoli I. Occupational Risk Factors and Hypertensive Disorders in Pregnancy: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(16):8277. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168277
Chicago/Turabian StyleSpadarella, Emanuela, Veruscka Leso, Luca Fontana, Angela Giordano, and Ivo Iavicoli. 2021. "Occupational Risk Factors and Hypertensive Disorders in Pregnancy: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 16: 8277. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168277