
Instrumental Validity of the Motion Detection Accuracy of a Smartphone-Based Training Game

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
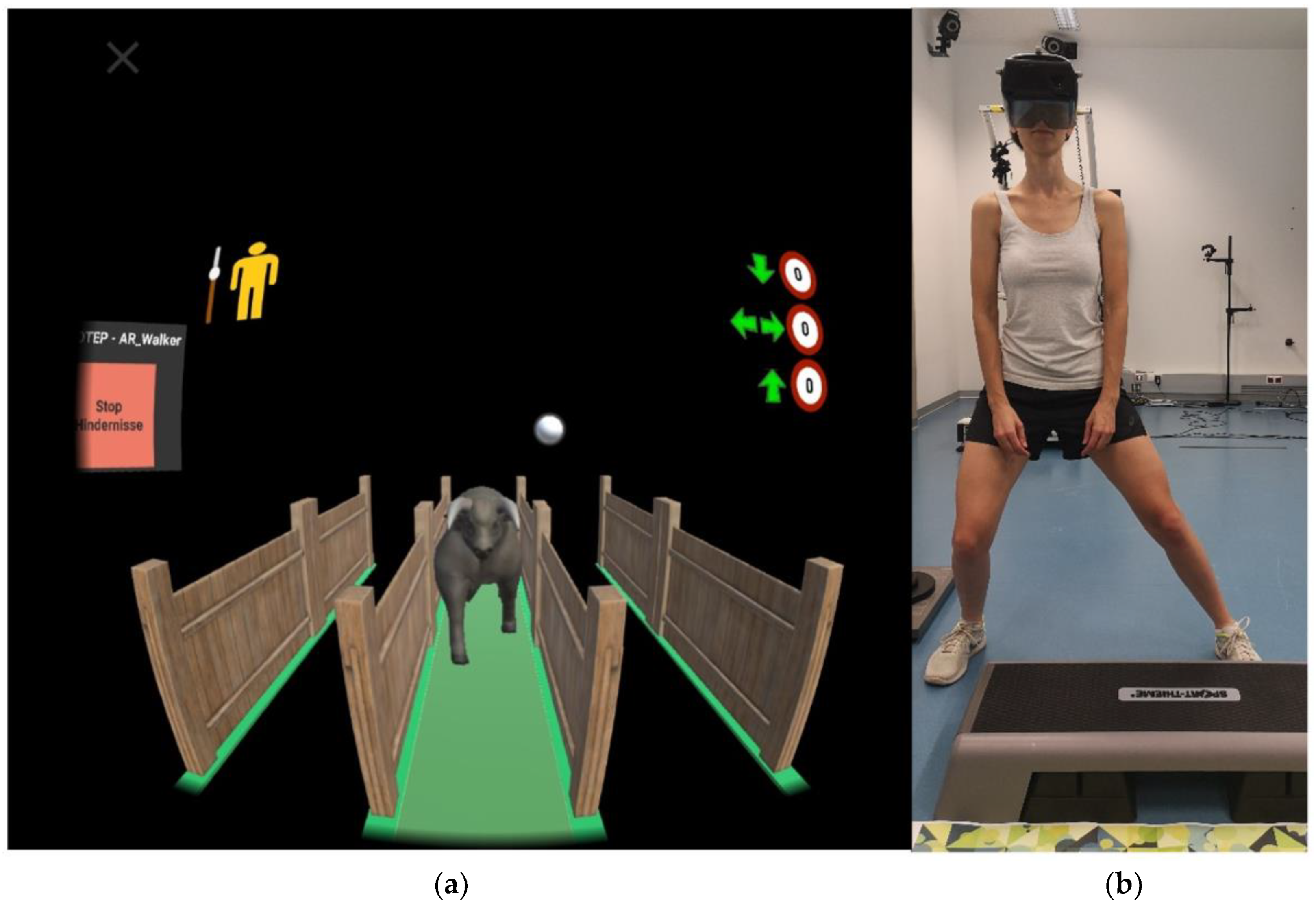
2.2. Exer-Game
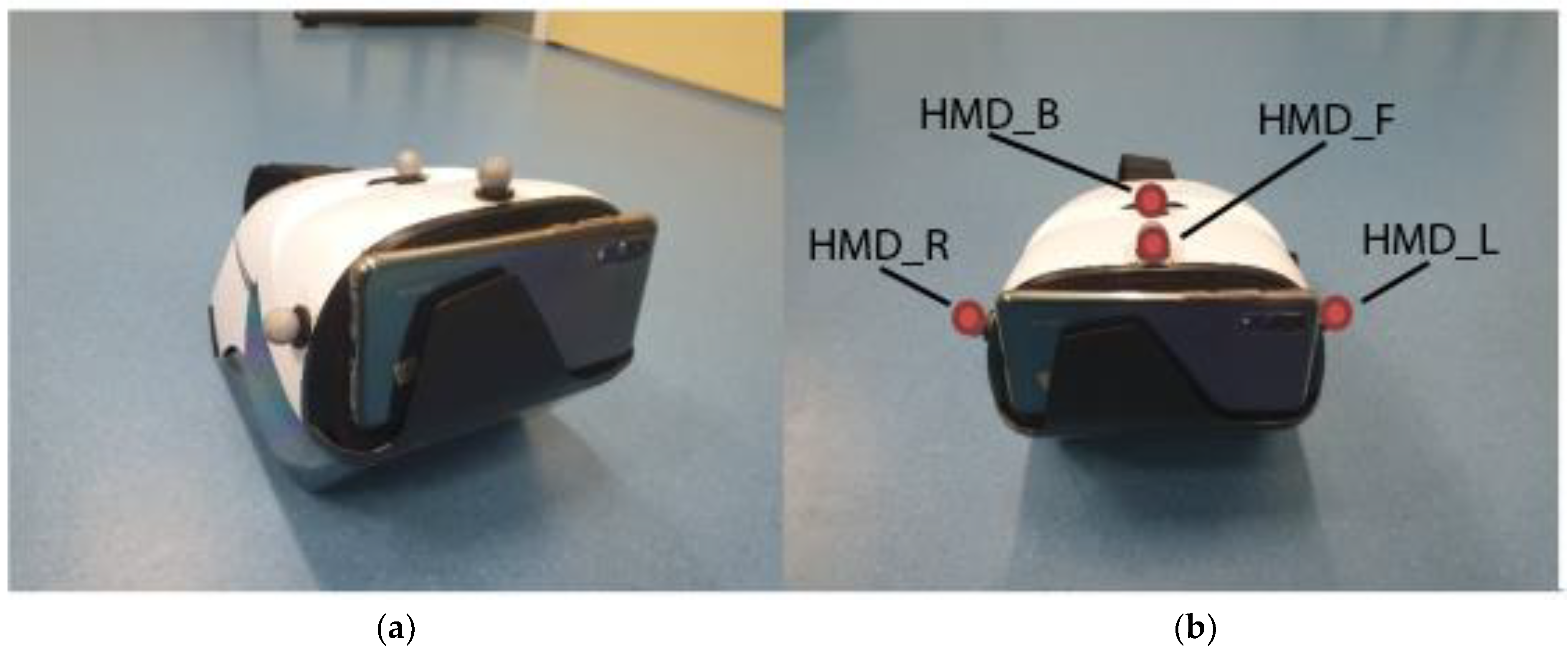
2.3. Reference System
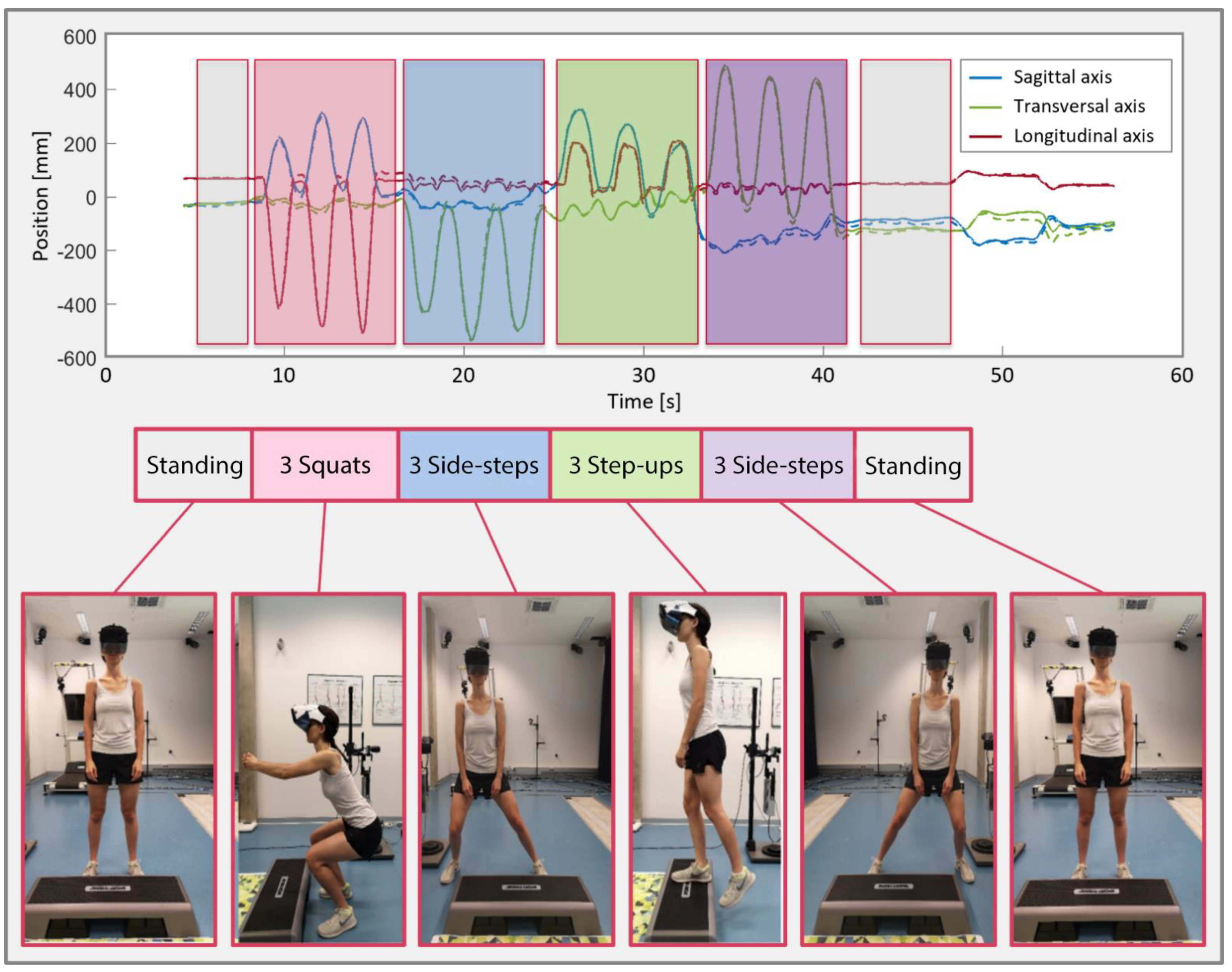
2.4. Measurement Protocol
2.5. Analysis and Statistics
3. Results
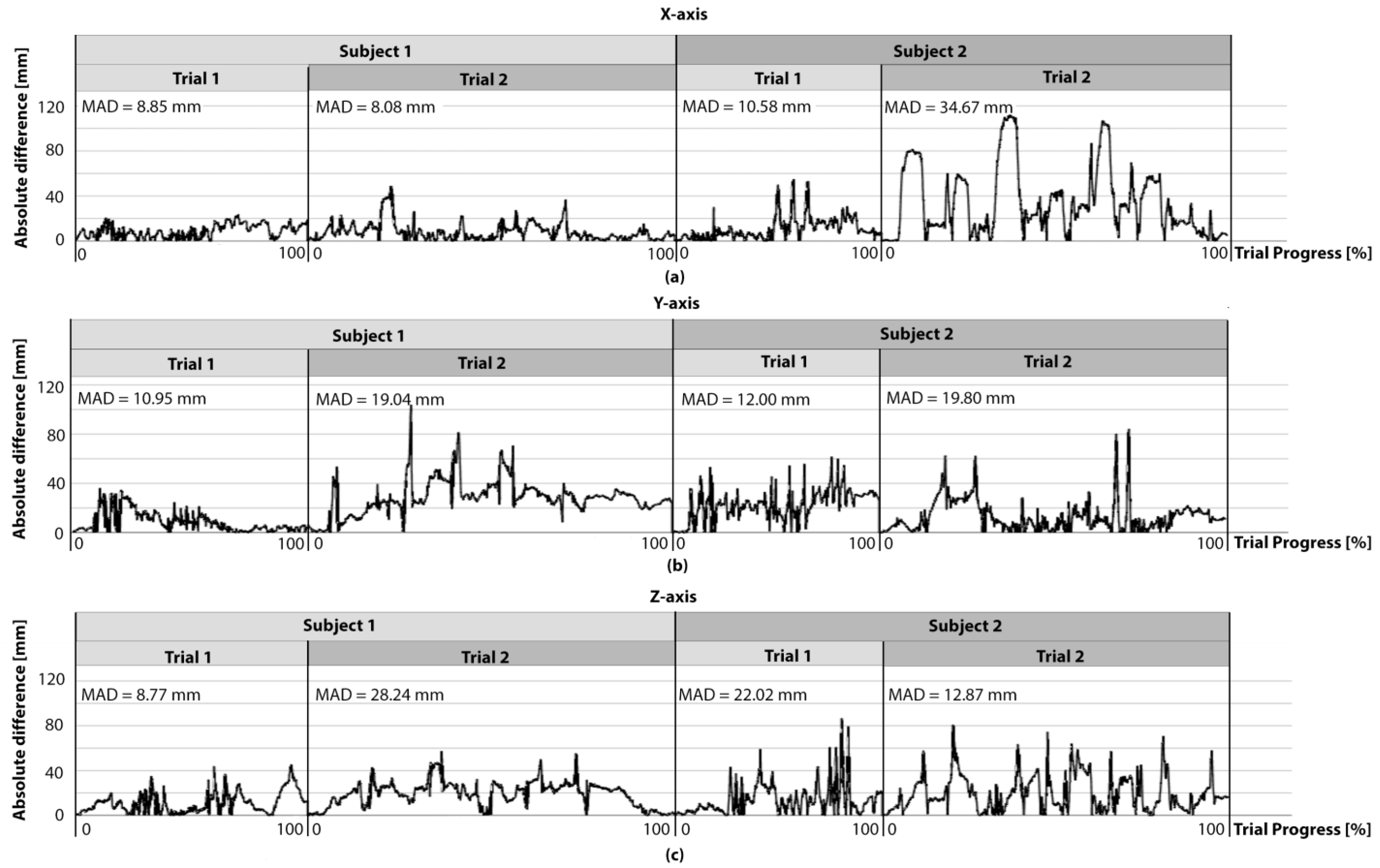
3.1. Position Trajectories
3.2. Rotational Trajectories
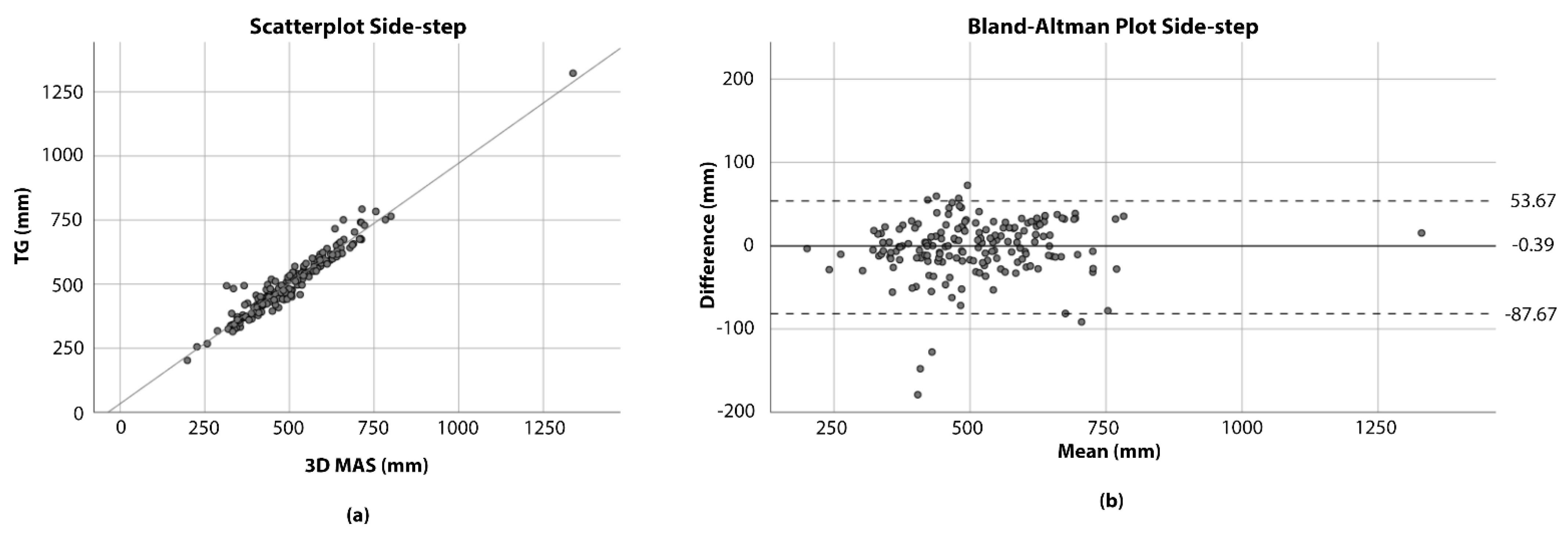
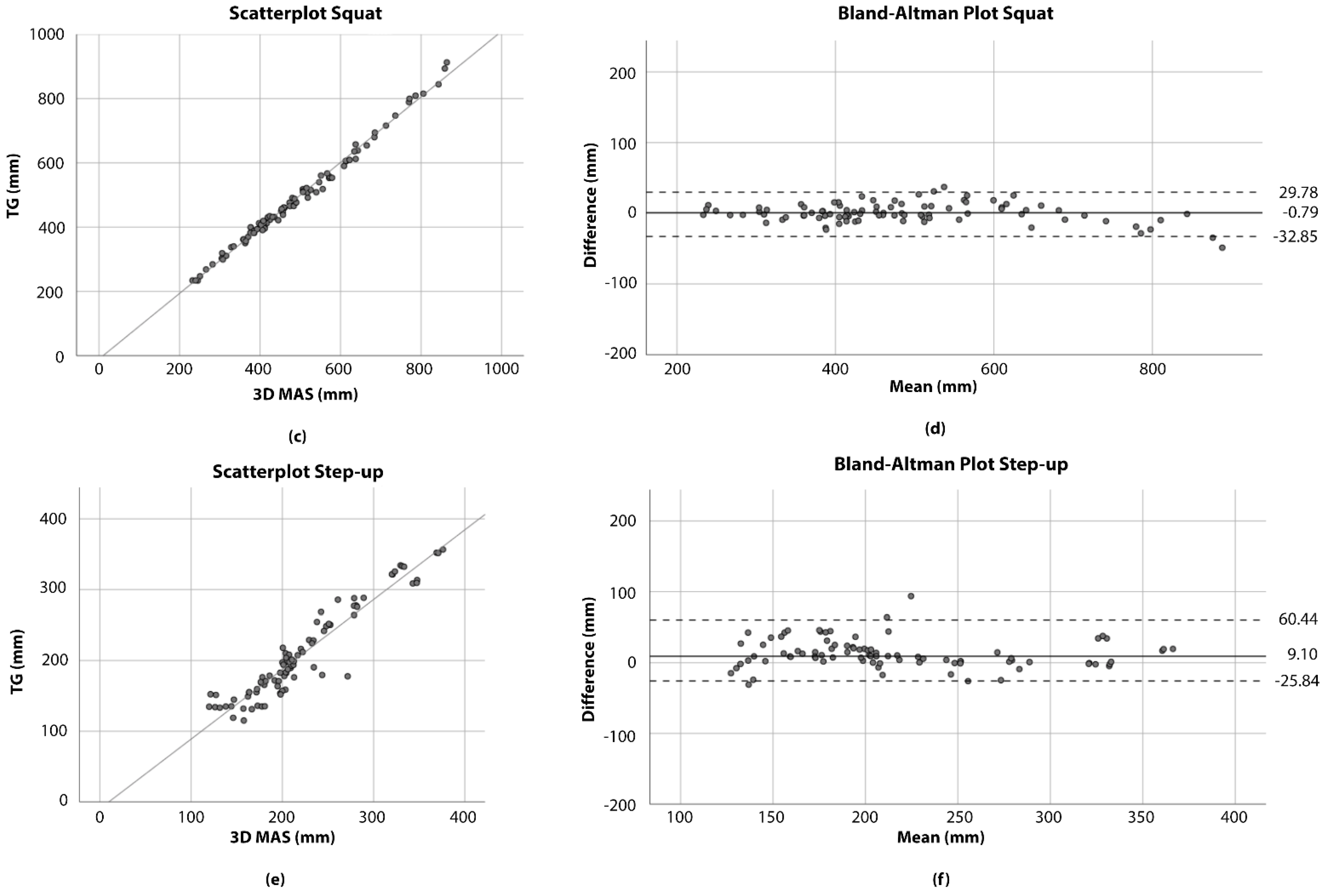
3.3. Exercise Amplitudes
4. Discussion
4.1. Limitations
4.2. Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hazra, N.C.; Gulliford, M.C.; Rudisill, C. ‘Fair innings’ in the face of ageing and demographic change. Health Econ. Policy Law 2017, 13, 209–217. [Google Scholar] [CrossRef] [Green Version]
- Wolf, D.A.; Amirkhanyan, A.A. Demographic Change and Its Public Sector Consequences. Public Adm. Rev. 2010, 70, s12–s23. [Google Scholar] [CrossRef]
- Singh, J.A.; Yu, S.; Chen, L.; Cleveland, J.D. Rates of Total Joint Replacement in the United States: Future Projections to 2020–2040 Using the National Inpatient Sample. J. Rheumatol. 2019, 46, 1134–1140. [Google Scholar] [CrossRef]
- Pabinger, C.; Lothaller, H.; Portner, N.; Geissler, A. Projections of hip arthroplasty in OECD countries up to 2050. HIP Int. 2018, 28, 498–506. [Google Scholar] [CrossRef]
- Bahl, J.S.; Nelson, M.J.; Taylor, M.; Solomon, L.B.; Arnold, J.B.; Thewlis, D. Biomechanical changes and recovery of gait function after total hip arthroplasty for osteoarthritis: A systematic review and meta-analysis. Osteoarthr. Cartil. 2018, 26, 847–863. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beaulieu, M.L.; Lamontagne, M.; Beaulé, P.E. Lower limb biomechanics during gait do not return to normal following total hip arthroplasty. Gait Posture 2010, 32, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Queen, R.M.; Appleton, J.S.; Butler, R.J.; Newman, E.T.; Kelley, S.S.; Attarian, D.E.; Bolognesi, M.P. Total Hip Arthroplasty Surgical Approach Does Not Alter Postoperative Gait Mechanics One Year After Surgery. PM R 2014, 6, 221–226. [Google Scholar] [CrossRef] [Green Version]
- Korn, O.; Buchweitz, L.; Rees, A.; Bieber, G.; Werner, C.; Hauer, K. Using Augmented Reality and Gamification to Empower Rehabilitation Activities and Elderly Persons. A Study Applying Design Thinking. In Advances in Artificial Intelligence, Software and Systems Engineering; Ahram, T.Z., Ed.; Advances in Intelligent Systems and Computing; Springer International Publishing: Cham, Switzerland, 2019; Volume 787, pp. 219–229. ISBN 978-3-319-94228-5. [Google Scholar]
- Kern, F.; Winter, C.; Gall, D.; Kathner, I.; Pauli, P.; Latoschik, M.E. Immersive Virtual Reality and Gamification Within Procedurally Generated Environments to Increase Motivation During Gait Rehabilitation. In Proceedings of the 2019 IEEE Conference on Virtual Reality and 3D User Interfaces (VR), Osaka, Japan, 23–27 March 2019; pp. 500–509. [Google Scholar] [CrossRef]
- Tuah, N.M.; Ahmedy, F.; Gani, A.; Yong, L.N. A Survey on Gamification for Health Rehabilitation Care: Applications, Opportunities, and Open Challenges. Information 2021, 12, 91. [Google Scholar] [CrossRef]
- Street, T.D.; Lacey, S.J.; Langdon, R.R. Gaming Your Way to Health: A Systematic Review of Exergaming Programs to Increase Health and Exercise Behaviors in Adults. Games Health J. 2017, 6, 136–146. [Google Scholar] [CrossRef]
- Muñoz-Saavedra, L.; Miró-Amarante, L.; Domínguez-Morales, M. Augmented and Virtual Reality Evolution and Future Tendency. Appl. Sci. 2020, 10, 322. [Google Scholar] [CrossRef] [Green Version]
- Viglialoro, R.M.; Condino, S.; Turini, G.; Carbone, M.; Ferrari, V.; Gesi, M. Review of the Augmented Reality Systems for Shoulder Rehabilitation. Information 2019, 10, 154. [Google Scholar] [CrossRef] [Green Version]
- Luque-Moreno, C.; Ferragut-Garcías, A.; Rodríguez-Blanco, C.; Heredia-Rizo, A.M.; Oliva-Pascual-Vaca, J.; Kiper, P.; Pascual-Vaca, Á. A Decade of Progress Using Virtual Reality for Poststroke Lower Extremity Rehabilitation: Systematic Review of the Intervention Methods. BioMed Res. Int. 2015, 2015, 342529. [Google Scholar] [CrossRef] [Green Version]
- TRIMOTEP Trainingsstützung Im Alltag Nach Rehabilitation Hüft-TEP. Available online: https://projekte.ffg.at/projekt/2812174 (accessed on 24 July 2021).
- TRIMOTEP Project Homepage. Available online: https://trimotep.fh-joanneum.at/ (accessed on 24 July 2021).
- Reiter, D.; Fülöp, G.; Pochobradsky, E.; Röthlin, F.; Stoppacher, A. Rehabilitationsplan 2020; Gesundheit Österreich: Vienna, Austria, 2020. [Google Scholar]
- Niedermüller, S. Bewegungserkennung Für Physiotherapeutische Übungen Mit Augmented-, Virtual- Und Mixed Reality Devices. Master’s Thesis, FH JOANNEUM-University of Applied Sciences, Graz, Austria, 2018. [Google Scholar]
- Dunn, J.; Yeo, E.; Moghaddampour, P.; Chau, B.; Humbert, S. Virtual and augmented reality in the treatment of phantom limb pain: A literature review. NeuroRehabilitation 2017, 40, 595–601. [Google Scholar] [CrossRef]
- Gorman, C.; Gustafsson, L. The use of augmented reality for rehabilitation after stroke: A narrative review. Disabil. Rehabil. Assist. Technol. 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Vidal-Balea, A.; Blanco-Novoa, Ó.; Fraga-Lamas, P.; Fernández-Caramés, T.M. Developing the Next Generation of Augmented Reality Games for Pediatric Healthcare: An Open-Source Collaborative Framework Based on ARCore for Implementing Teaching, Training and Monitoring Applications. Sensors 2021, 21, 1865. [Google Scholar] [CrossRef] [PubMed]
- McCauley, M.E.; Sharkey, T.J. Cybersickness: Perception of Self-Motion in Virtual Environments. Presence Teleoperators Virtual Environ. 1992, 1, 311–318. [Google Scholar] [CrossRef]
- Bolink, S.A.A.N.; Naisas, H.; Senden, R.; Essers, H.; Heyligers, I.C.; Meijer, K.; Grimm, B. Validity of an inertial measurement unit to assess pelvic orientation angles during gait, sit–stand transfers and step-up transfers: Comparison with an optoelectronic motion capture system. Med. Eng. Phys. 2016, 38, 225–231. [Google Scholar] [CrossRef]
- Wirth, M.A.; Fischer, G.; Verdú, J.; Reissner, L.; Balocco, S.; Calcagni, M. Comparison of a New Inertial Sensor Based System with an Optoelectronic Motion Capture System for Motion Analysis of Healthy Human Wrist Joints. Sensors 2019, 19, 5297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feuvrier, F.; Sijobert, B.; Azevedo, C.; Griffiths, K.; Alonso, S.; Dupeyron, A.; Laffont, I.; Froger, J. Inertial measurement unit compared to an optical motion capturing system in post-stroke individuals with foot-drop syndrome. Ann. Phys. Rehabil. Med. 2020, 63, 195–201. [Google Scholar] [CrossRef]
- Seel, T.; Werner, C.; Schauer, T. The adaptive drop foot stimulator–Multivariable learning control of foot pitch and roll motion in paretic gait. Med. Eng. Phys. 2016, 38, 1205–1213. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Madara, K.C.; Marmon, A.; Aljehani, M.; Hunter-Giordano, A.; Zen, J.; Raisis, L. Progressive rehabilitation after total hip arthroplasty: A pilot and feasibility study. Int. J. Sports Phys. Ther. 2019, 14, 564–581. [Google Scholar] [CrossRef] [Green Version]
- Oufqir, Z.; El Abderrahmani, A.; Satori, K. ARKit and ARCore in serve to augmented reality. In Proceedings of the 2020 International Conference on Intelligent Systems and Computer Vision (ISCV), Fez, Morocco, 9–11 June 2020; pp. 1–7. [Google Scholar] [CrossRef]
- Cimolin, V.; Galli, M. Summary measures for clinical gait analysis: A literature review. Gait Posture 2014, 39, 1005–1010. [Google Scholar] [CrossRef]
- Salchow-Hömmen, C.; Callies, L.; Laidig, D.; Valtin, M.; Schauer, T.; Seel, T. A Tangible Solution for Hand Motion Tracking in Clinical Applications. Sensors 2019, 19, 208. [Google Scholar] [CrossRef] [Green Version]
- Richards, J.G. The measurement of human motion: A comparison of commercially available systems. Hum. Mov. Sci. 1999, 18, 589–602. [Google Scholar] [CrossRef]
- Abhayasinghe, N.; Murray, I.; Sharif Bidabadi, S. Validation of Thigh Angle Estimation Using Inertial Measurement Unit Data against Optical Motion Capture Systems. Sensors 2019, 19, 596. [Google Scholar] [CrossRef] [Green Version]
- Ceseracciu, E.; Sawacha, Z.; Cobelli, C. Comparison of Markerless and Marker-Based Motion Capture Technologies through Simultaneous Data Collection during Gait: Proof of Concept. PLoS ONE 2014, 9, e87640. [Google Scholar] [CrossRef] [PubMed]
- Schmitz, A.; Ye, M.; Shapiro, R.; Yang, R.; Noehren, B. Accuracy and repeatability of joint angles measured using a single camera markerless motion capture system. J. Biomech. 2014, 47, 587–591. [Google Scholar] [CrossRef]
- Kuttner, T.; Rohnen, A. Springer Fachmedien Wiesbaden GmbH Praxis der Schwingungsmessung: Messtechnik und Schwingungsanalyse mit MATLAB; Springer: Berlin/Heidelberg, Germany, 2019; ISBN 978-3-658-25047-8. [Google Scholar]
- Noujaim, S.E.; Horwitz, D.; Sharma, M.; Marhoul, J. Accuracy Requirements for a Hypoglycemia Detector: An Analytical Model to Evaluate the Effects of Bias, Precision, and Rate of Glucose Change. J. Diabetes Sci. Technol. 2007, 1, 652–668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koch, R.; Spörl, E. Statistische Verfahren zum Vergleich zweier Messmethoden und zur Kalibrierung: Konkordanz-, Korrelations- und Regressionsanalyse am Beispiel der Augeninnendruckmessung. Klin. Mon. Augenheilkd. 2007, 224, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Giavarina, D. Understanding Bland Altman analysis. Biochem. Med. 2015, 25, 141–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, X.; Chen, K.B.; Lin, J.-H.; Radwin, R.G. The accuracy of the Oculus Rift virtual reality head-mounted display during cervical spine mobility measurement. J. Biomech. 2015, 48, 721–724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Obdrzalek, S.; Kurillo, G.; Ofli, F.; Bajcsy, R.; Seto, E.; Jimison, H.; Pavel, M. Accuracy and robustness of Kinect pose estimation in the context of coaching of elderly population. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012; pp. 1188–1193. [Google Scholar] [CrossRef]
- Xu, X.; McGorry, R.W. The validity of the first and second generation Microsoft Kinect™ for identifying joint center locations during static postures. Appl. Ergon. 2015, 49, 47–54. [Google Scholar] [CrossRef]
- Yuan, Q.; Chen, I.-M. Localization and velocity tracking of human via 3 IMU sensors. Sens. Actuators A Phys. 2014, 212, 25–33. [Google Scholar] [CrossRef]
- Poulose, A.; Eyobu, O.S.; Han, D.S. An Indoor Position-Estimation Algorithm Using Smartphone IMU Sensor Data. IEEE Access 2019, 7, 11165–11177. [Google Scholar] [CrossRef]
- LaValle, S.M.; Yershova, A.; Katsev, M.; Antonov, M. Head Tracking for the Oculus Rift. In Proceedings of the International Conference on Robotics and Automation, Hongkong, China, 5–7 June 2014; pp. 187–194. [Google Scholar] [CrossRef]
- Narasimhappa, M.; Mahindrakar, A.D.; Guizilini, V.C.; Terra, M.H.; Sabat, S.L. MEMS-Based IMU Drift Minimization: Sage Husa Adaptive Robust Kalman Filtering. IEEE Sens. J. 2020, 20, 250–260. [Google Scholar] [CrossRef]
- Reimer, L.M.; Weigel, S.; Ehrenstorfer, F.; Adikari, M.; Birkle, W.; Jonas, S. Mobile Motion Tracking for Disease Prevention and Rehabilitation Using Apple ARKit. In Studies in Health Technology and Informatics; Hayn, D., Schreier, G., Baumgartner, M., Eds.; IOS Press: Amsterdam, The Netherlands, 2021; ISBN 978-1-64368-180-1. [Google Scholar]
- Bielecki, J.E.; Tadi, P. Therapeutic Exercise; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | N = 30 |
|---|---|
| Age in Years, N (SD) | 32.0 (±10.1) |
| Gender, N (%) | |
| Female, absolute (%) | 15 (50) |
| Male, absolute (%) | 15 (50) |
| Height in cm, mean (SD) | 175 (±10) |
| Previous experience with AR/VR applications, N (%) | 16 (53.3) |
| Previous experience with squat exercise, N (%) | 30 (100) |
| Squat exercise already performed once, N (%) | 30 (100) |
| Previous experience with the exercise side-step, N (%) | 29 (96.7) |
| Side-step exercise already performed once, N (%) | 30 (100) |
| Previous experience with the exercise step-up, N (%) | 30 (100) |
| Step-up exercise already performed once, N (%) | 30 (100) |
| Trial 1 | Trial 2 |
|---|---|
| Starting the training game | Starting the training game |
| Performing synchronization movement | Performing synchronization movement |
| 3 squats | Playing the training game for approximately one minute |
| 3 Side-steps to the right side and back | |
| 3 Step-ups | |
| 3 Side-steps to the left side and back | |
| Closing the training game | Closing the training game |
| Axis | MAD | RMSE |
|---|---|---|
| Sagittal, mm | 18.68 ± 29.7 | 35.08 |
| Transversal, mm | 24.98 ± 26.73 | 36.59 |
| Longitudinal, mm | 18.03 ± 17.66 | 25.24 |
| Rotational Trajectory | MAD | RMSE |
|---|---|---|
| Flexion, ° | 0.48 ± 0.46 | 0.66 |
| Lateral flexion, ° | 0.47 ± 0.88 | 1.00 |
| Rotation, ° | 0.73 ± 0.96 | 1.20 |
| Parameter | Squat | Side-Step | Step-Up |
|---|---|---|---|
| MAD ± SD, mm | 10.13 ± 9.4 | 24.59 ± 24.33 | 17.31 ± 16.65 |
| RMSE, mm | 13.79 | 34.54 | 23.96 |
| MARD | 0.02 | 0.05 | 0.08 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guggenberger, B.; Jocham, A.J.; Jocham, B.; Nischelwitzer, A.; Ritschl, H. Instrumental Validity of the Motion Detection Accuracy of a Smartphone-Based Training Game. Int. J. Environ. Res. Public Health 2021, 18, 8410. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168410
Guggenberger B, Jocham AJ, Jocham B, Nischelwitzer A, Ritschl H. Instrumental Validity of the Motion Detection Accuracy of a Smartphone-Based Training Game. International Journal of Environmental Research and Public Health. 2021; 18(16):8410. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168410
Chicago/Turabian StyleGuggenberger, Bernhard, Andreas J. Jocham, Birgit Jocham, Alexander Nischelwitzer, and Helmut Ritschl. 2021. "Instrumental Validity of the Motion Detection Accuracy of a Smartphone-Based Training Game" International Journal of Environmental Research and Public Health 18, no. 16: 8410. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168410