3.1. Survey Results
The final sample achieved for the study was 108. The demographic information of the participants is presented in
Table 1. Among the total participants, 58.3% were male (63/108), and 41.7% were female (45/108). Considering the age groups, 43.5% were aged between 35 and 44 years (47/108), followed by 30.6% between 25 and 34 years (114/479), 12% between 18 and 24 years (13/108), 12% between 45 and 54 years (13/108), and 1.9% participants aged 55 or more than 55 years (2/108). Focusing on the education of the participants, 38.9% were bachelor’s degree graduates (42/108), followed by 30.6% master’s graduates (33/108), 15.7% high school graduates or diploma graduates (17/108), and 14.8% doctorates (16/108). Demographics of the participants reflected good participation levels by both genders. Moreover, the majority of the participants were aged between 25 and 44 years, reflecting the population who is better equipped with the skills of using health information technologies [
40,
41,
42], and has good education levels.
All the participants were having an experience of using both Telehealth and mHealth approaches. In relation to the experience of using Telehealth (via telephone/mobile), 65.7% of the participants had 2 or less than 2 years of experience (71/108), followed by 17.6% having 2 to 5 years of experience (19/108), 9.3% having 10 or more years of experience (10/108), and 7.4% having 5 to 10 years of experience (8/108). In relation to the experience of using mHealth (via mobile application/smart sensors), 63.9% of the participants had 2 or less than 2 years of experience (69/108), followed by 25.9% having 2 to 5 years of experience (28/108), 6.5% having 10 or more years of experience (7/108), and 3.7% having 5 to 10 years of experience (4/108). The experience levels of the participants in relation to mHealth and Telehealth reflected almost similar statistics, with the majority of them having 2 years or less and 2 to 5 years of experience.
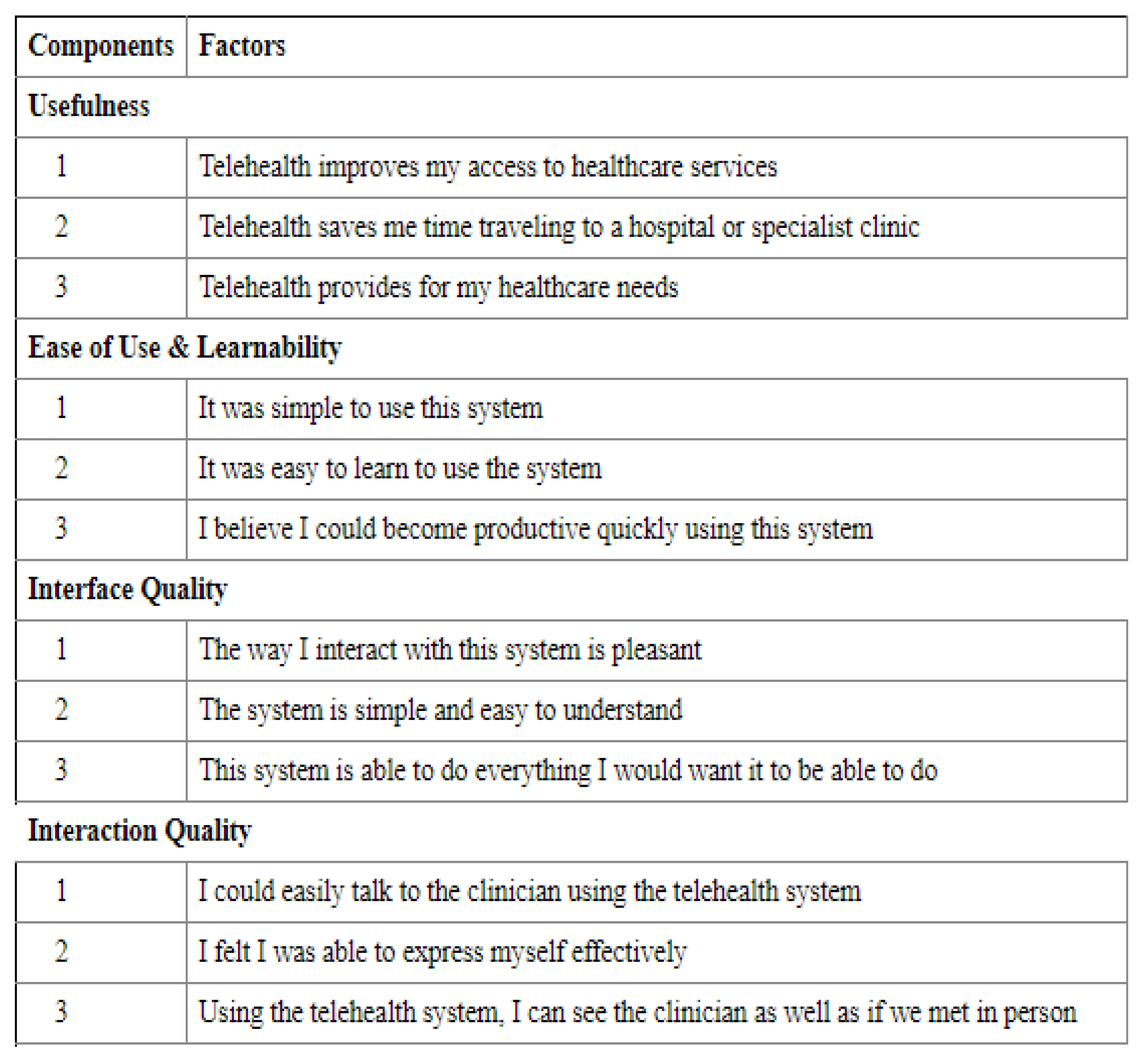
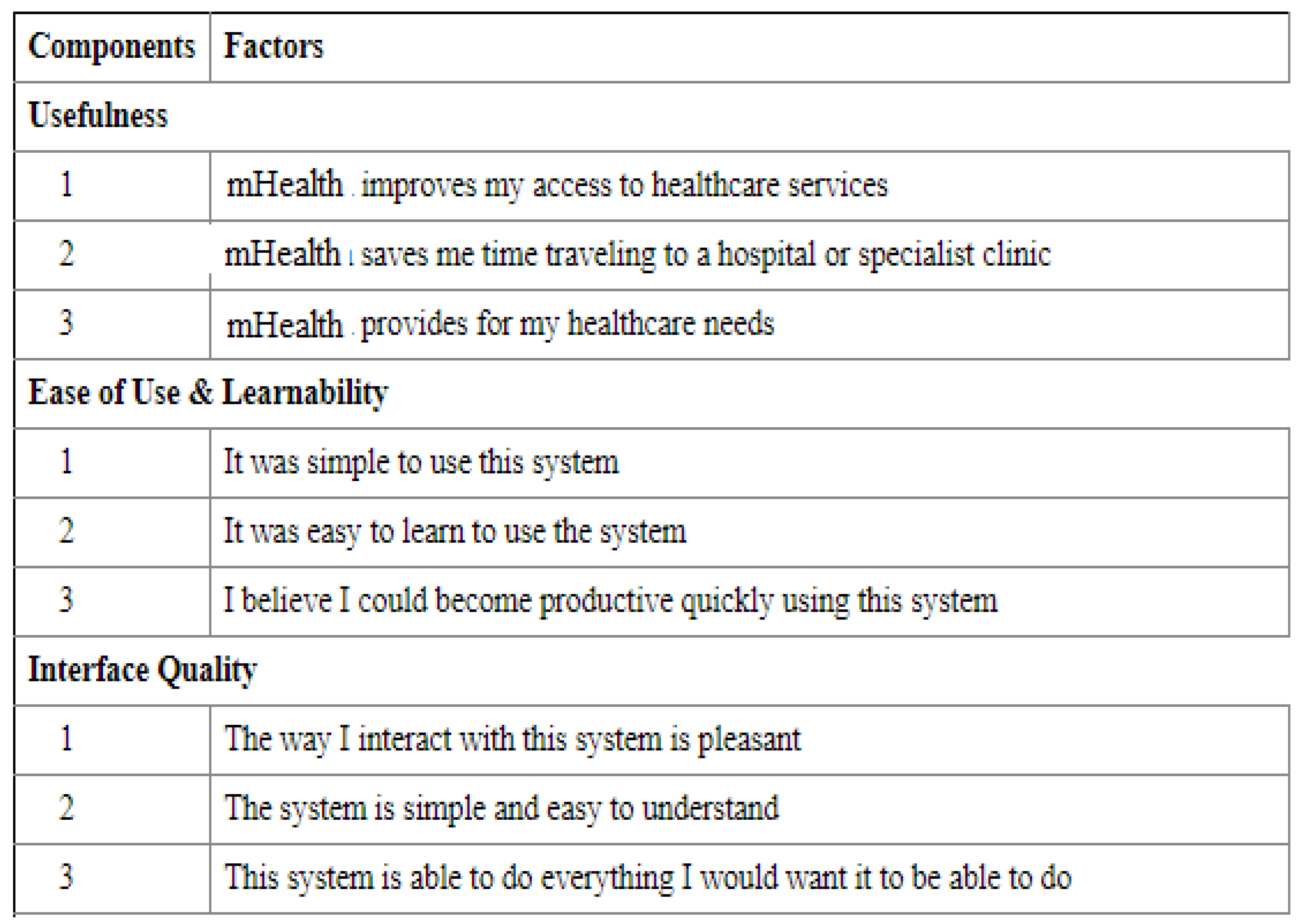
Participants’ opinions on the usefulness of both mHealth and Telehealth are presented in
Table 2. Improved access to healthcare was identified to be a highly rated factor related to usefulness, followed by the time-saving factor, and approaches meeting the healthcare needs of the users. Both approaches were identified to be similarly rated by the participants in relation to the usefulness parameter.
Furthermore, to identify the differences of opinions in relation to mHealth and Telehealth, a
t-test was conducted, as shown in
Table 3. The mean scores of mHealth (Mean = 3.64, SD = 1.12) and Telehealth (Mean = 3.61, SD = 1.08), identified in the analysis, reflected that participants found that both mHealth and Telehealth approaches to be effective in terms of usefulness.
t-value, as shown in
Table 3, was found to be (
t = 0.2004) at 0.05 confidence interval, and was identified as not statistically significant (
p > 0.05). Therefore, no significant differences of opinions in relation to the usefulness of mHealth and Telehealth can be observed. The findings are similar to [
32], reflecting the usefulness of both approaches. As both approaches are aimed at improving access to healthcare and save time in accessing healthcare needs, it is possible that both approaches are identified to be useful by the participants.
Participants’ opinions on the ease of use and learnability parameters are presented in
Table 4. It can be observed that simple to use and easy to learn factors of mHealth are slightly greater than that of Telehealth; no major differences were identified in relation to the ability of the approach for enhancing productivity. While the mHealth application is mobile-based, and easy to use, Telehealth completely relies on calls in providing care and monitoring health information. Therefore, slight differences in terms of ease of use and learnability factors can be expected.
Furthermore, to identify the differences of opinions in relation to mHealth and Telehealth, a
t-test was conducted, as shown in
Table 5. The mean scores of mHealth (Mean = 3.72, SD = 1.12) and Telehealth (Mean = 3.69, SD = 1.1), identified in the analysis, reflected that participants found that both mHealth and Telehealth approaches to be effective in terms of ease of use and learnability.
t-value, as shown in
Table 5, was found to be (
t = 0.1986) at 0.05 confidence interval, and was identified as not statistically significant (
p > 0.05). Therefore, no significant differences of opinions in relation to ease of use and learnability parameters of mHealth and Telehealth can be observed. These findings can be related to [
33], in which ease of use and learnability were rated to be effective by the majority of the participants.
While mHealth applications have a mobile interface, Telehealth does not have any physical interface, but the quality of the interface can be identified from the communication between patients and healthcare practitioners over telephone or mobiles. In relation to the interface quality, both mHealth and Telehealth approaches were rated slightly above average (Mean = 2.5), as shown in
Table 6. It is interesting to note that only 50.9% of the participants either strongly agreed or agreed that the Telehealth approach meets their healthcare needs, and only 52.7% of the participants either strongly agreed or agreed that the mHealth approach meets their healthcare needs, reflecting that there is a considerable number of participants who are not happy with interface quality in both approaches.
Furthermore, to identify the differences of opinions in relation to mHealth and Telehealth, a
t-test was conducted, as shown in
Table 7. The mean scores of mHealth (Mean = 3.42, SD = 1.05) and Telehealth (Mean = 3.43, SD = 1.06), identified in the analysis, reflected that participants found that both mHealth and Telehealth approaches to be effective in terms of interface quality.
t-value, as shown in
Table 7, was found to be (
t = 0.0697) at 0.05 confidence interval, and was identified as not statistically significant (
p > 0.05). Therefore, no significant differences of opinions in relation to interface quality parameters of mHealth and Telehealth can be observed. These findings related to mHealth are similar to [
34], indicating good interface quality of mHealth applications.
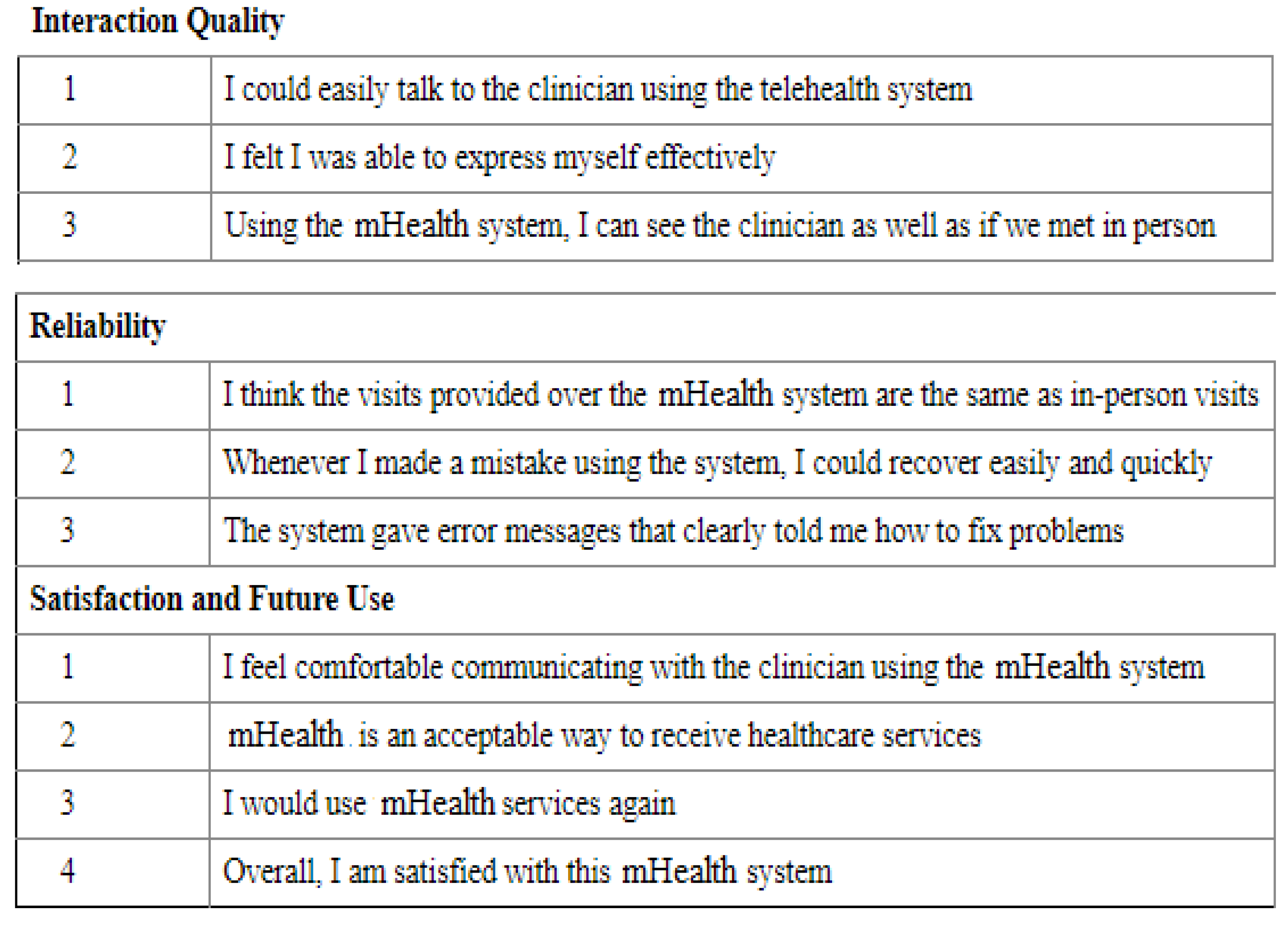
In relation to interaction quality, no significant differences were identified between mHealth and Telehealth, as identified from
Table 8. In relation to the ability of the approaches reflecting in similar to personal interactions, less than 50% of the participants reflected the opinion that these approaches are similar to personal interactions. Moreover, more than 50% of the participants stated that they are not able to express their opinions effectively on mHealth and Telehealth applications.
Furthermore, to identify the differences of opinions in relation to mHealth and Telehealth, a
t-test was conducted, as shown in
Table 9. The mean scores of mHealth (Mean = 3.41, SD = 1.05) and Telehealth (Mean = 3.40, SD = 0.99), identified in the analysis, reflected that participants found that both mHealth and Telehealth approaches to be effective in terms of interaction quality.
t-value, as shown in
Table 9, was found to be (
t = 0.0720) at 0.05 confidence interval, and was identified as not statistically significant (
p > 0.05). Therefore, no significant differences of opinions in relation to interface quality parameters of mHealth and Telehealth can be observed. These findings related to mHealth are similar to [
33,
34], indicating average interaction quality of mHealth and Telehealth approaches.
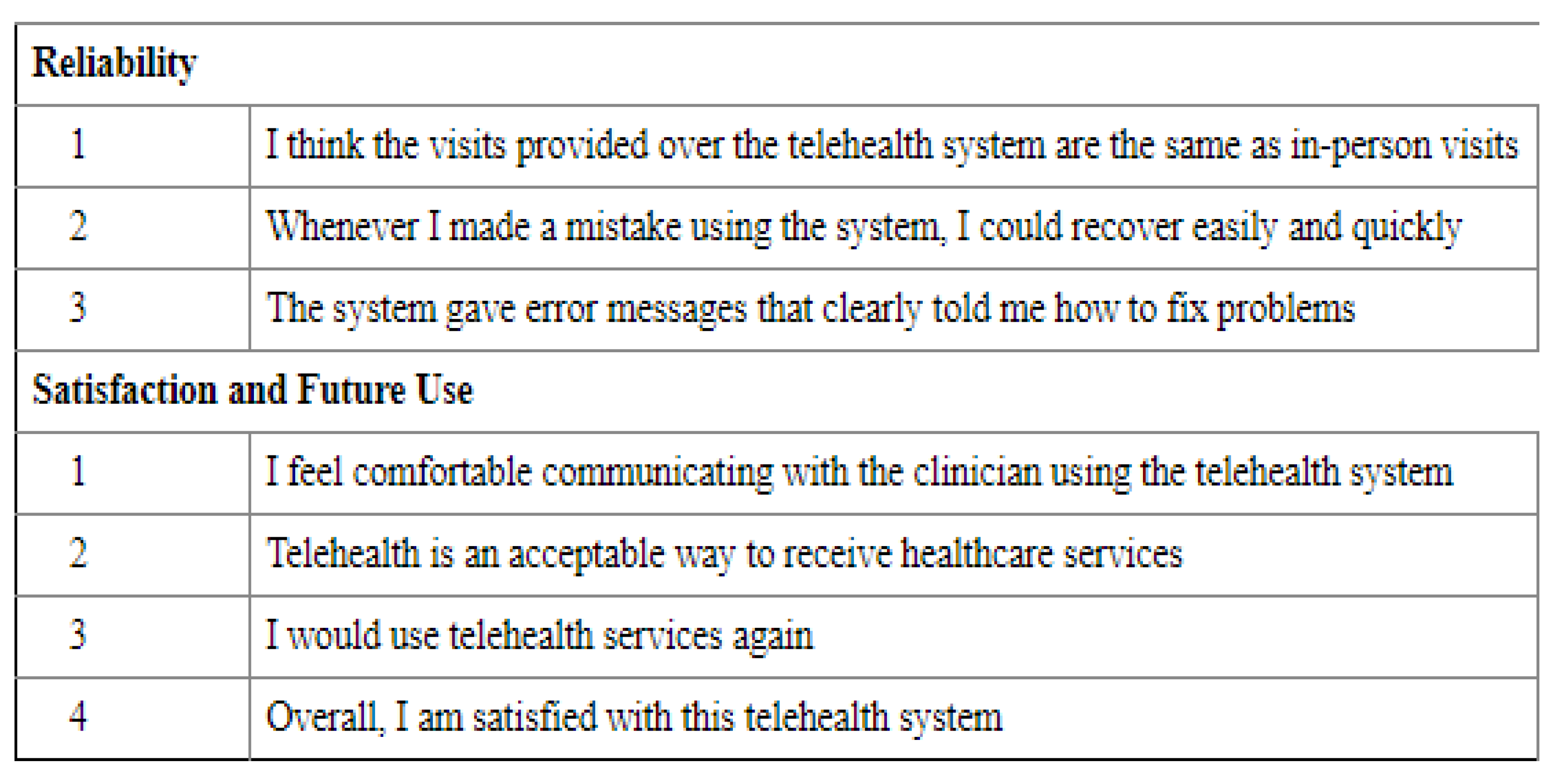
In relation to reliability (
Table 10), the mHealth approach was rated as slightly better than the Telehealth approach, stating that the approach was similar to hospital visits in delivering the care, and also in the ability to fix issues by receiving messages through the application (in comparison to messages received through calls). The majority of the participants (>50%) were identified to be neutral (neither agree nor disagree) in relation to all the factors listed in the reliability parameter.
Furthermore, to identify the differences of opinions in relation to mHealth and Telehealth, a
t-test was conducted, as shown in
Table 11. The mean scores of mHealth (Mean = 3.27, SD = 1.03) and Telehealth (Mean = 3.08, SD = 1.05), identified in the analysis, reflected that participants found that both mHealth and Telehealth approaches to be effective in terms of reliability.
t-value, as shown in
Table 11, was found to be (
t = 1.3424) at 0.05 confidence interval, and was identified as not statistically significant (
p > 0.05). Therefore, no significant differences of opinions in relation to the reliability parameter of mHealth and Telehealth can be observed. Considering the less acceptance of eHealth in Saudi Arabia, due to various factors of influence, it may be possible that low responses were identified in relation to reliability factor, which can be compared to the findings in [
43].
In relation to satisfaction (
Table 12), it can be identified that participants were slightly more satisfied with mHealth compared to Telehealth across all the factors related to satisfaction and future use. Considering the overall satisfaction, there is no difference of opinions expressed in relation to both approaches. However, while 60% of the participants agreed that they would use mHealth in the future, 64% of the participants stated they would use Telehealth in the future, indicating a slightly more preference towards Telehealth over mHealth.
Furthermore, to identify the differences of opinions in relation to mHealth and Telehealth, a
t-test was conducted, as shown in
Table 11. The mean scores of mHealth (Mean = 3.63, SD = 1.06) and Telehealth (Mean = 3.53, SD = 1.04), identified in the analysis, reflected that participants found that both mHealth and Telehealth approaches to be effective in terms of satisfaction and future use.
t-value, as shown in
Table 13, was found to be (
t = 0.6998) at 0.05 confidence interval, and was identified as not statistically significant (
p > 0.05). Therefore, no significant differences of opinions in relation to the reliability parameter of mHealth and Telehealth can be observed.
These findings may be compared to [
31,
32,
40] in relation to satisfaction levels. Moreover, preference over these approaches may be influenced by the recent COVID-19 outbreak, which has led to increased adoption of eHealth approaches due to the surge in COVID-19 cases and preventive measures such as lockdowns and curfews. However, lack of reliability as identified in [
43] can be one of the reasons for leaning more towards Telehealth rather than mHealth.
3.2. Interview Results
A total of seven healthcare practitioners were interviewed, and all of them were males. Among them, three participants belonged to the age group of 35–44 years; another three in 45–54 years; and one participant in 25–34 years. Four participants were general physicians, one participant was a dentist, one was a surgery specialist, and another was a medical specialist. Three participants had experience of 2 or less years in using mHealth and Telehealth approaches, two had an experience of 2 to 5 years, and another two had an experience of 5 to 10 years. The participants’ experience levels and roles reflect a good sample for collecting the information about mHealth and Telehealth.
Focusing on the opinions expressed in relation to Telehealth, all the participants identified good usefulness levels for Telehealth. One of the interviewees identified it to be an easier approach to reach patients without any difficulty or requirement to learn new technologies, reflecting the edge over mHealth. Another interviewee identified Telehealth to be an effective approach in providing distant care. In relation to mHealth, only one participant identified its usefulness to be poor, while the rest of them indicated good levels of usefulness. One of the interviewees identified it to be very useful, providing real-time information at any time. The findings in relation to usefulness indicated that the majority of the participants identified both approaches to be of good usefulness. However, Telehealth was identified to be slightly more useful compared to mHealth.
In relation to ease of use, all the interviewees mentioned Telehealth to be very easy to use and learn. However, one of the interviewees mentioned that additional training relating to compliances and standards is required in using Telehealth. One of the interviewees mentioned that Telehealth may not be easy to learn in the beginning, but as handling of it improves, one can learn effectively. Similarly, all the interviewees identified mHealth to be easy to use, with little knowledge of computers and technology. However, one of the interviewees mentioned that experience is required in using mHealth, and another interviewee mentioned that mHealth is hard to use. Another interviewee mentioned that mHealth may be effective for learning for only those who use mobiles more frequently, and have experience of using applications. The overall analysis of responses indicated that Telehealth was rated slightly more than mHealth in terms of ease of use and learnability.
In relation to interface and interaction quality, all the interviewees reflected Telehealth to be good. Similarly, in relation to mHealth, only one interviewee identified it with poor interface and interaction quality. Using Telehealth was identified to be effective because interaction using Telehealth takes comparatively less time than visits, which can save time; while using mHealth, it was indicated that a lot of time could be saved as it is one-way messaging. Both approaches indicated time-saving as an outcome of effective interface and interaction quality. However, Telehealth was slightly rated more than mHealth.
Focusing on the reliability parameter, all the interviewees indicated Telehealth to be reliable but extended their statement that reliability may depend on many factors, including the physician and patient and the technology used to connect them. While Telehealth mainly relies on calls, it is sometimes possible that internet technologies such as voice over internet protocol or applications such as skype or zoom may be used, which may raise concerns over security and privacy. However, in relation to mHealth, five interviewees stated it to be reliable. One of the interviewees stated that more research is needed to assess its reliability, while others raised privacy and security concerns over mHealth.
Findings relating to usefulness, ease of use, learnability, interface and interaction quality, and reliability from interviewees’ perspectives reflected a slightly greater preference towards Telehealth compared to mHealth in contrast to patients’ perspectives. The differences of opinions among the participants may be related to their experience and understanding of these approaches, and also the features and design of the applications they have been using, which can influence their perspectives [
44,
45,
46].
In relation to the satisfaction parameter, all the interviewees reflected good satisfaction levels about the Telehealth approach. However, focusing on the mHealth approach, one interviewee stated moderate satisfaction and another interviewee stated poor satisfaction. Findings reflected that the interviewees are slightly more satisfied with Telehealth compared to mHealth. These results regarding satisfaction contrasted with survey results, where participants identified with being slightly more satisfied with mHealth compared to Telehealth, supporting findings from [
47,
48,
49,
50]. Furthermore, in relation to future use prospects, Telehealth was identified to be a promising approach in reducing clinical visits, improving quality healthcare. Similarly, mHealth was also identified to be having a promising future where electronic health records can be integrated with daily monitoring systems, providing 24 × 7 remote healthcare services which can significantly improve effectiveness and efficiency of care. The results have indicated that both mHealth and Telehealth would be increasingly adopted in the future, similar to survey results.







{kind=link}
{kind=link}
{kind=link}
{kind=link}