1. Introduction
We practice self-medication (SM) every day as a part of self-care of our health [
1]. SM is an action practiced either personally or assisted by someone to manage unknown and less severe health conditions. The World Health Organization stated that the responsible practice of SM does pose the advantage of preventing and treating various mild health conditions that do not need initial medical consultation. Additionally, SM provides an affordable alternative for managing common illnesses [
2]. However, inappropriate SM can lead to health consequences such as lack of drug effectiveness, allergy to certain medications, hindrance of actual diagnosis, increased resistance to certain types of medication, severe medication side effects, interaction with other drugs and food supplements, drug toxicity, overdose and dependency, development of resistance to certain drugs, withdrawal symptoms, and countless other health problems [
3].
Although the objective of SM is clear, it is often practiced without proper scientific knowledge and background. In fact, SM practice could be forecasted in countries where healthcare expenses are met through people’s own pockets. Nevertheless, in Saudi Arabia, where healthcare expenses are supported by government and insurance companies, SM practice still prevails. Usually, the medications received from family or friends, leftover drugs from a previous prescription, and over-the-counter (OTC) drugs are self-administered to treat acute health conditions such as influenza, headache, coughs, and gastrointestinal disturbances [
4,
5]. SM is very common among the educated population, and the possible reasons for this rising tendency are the desire for self-care, kindheartedness towards family members in sickness [
6], time trouble, shortage of health services, financial limitations, ignorance, misconceptions [
7], and extensive advertisement and availability of drugs in non-drug shops [
8]. Inappropriate SM not only harms the patient in the form of medication-related problems, but also increases treatment cost and frequency of hospital admission. SM is generally prevalent in all age groups; however, its extent differs among individuals and regions. The students of the healthcare program are expected to be more knowledgeable regarding the rational use of medications as compared to the general public. Rational use of medicine and the outcomes of irrational use are highlighted to these students in their curriculum [
9]. SM among healthcare students would be because of their future medical preferences and knowledge about the drugs. Practicing SM, however, though seen by a lot of students as a time-managing, easy and successful process, does pose many hazards [
10].
Various national [
9,
10] (Mustafa and Rohra [
11]; Sultan MA et al. [
12]; Mustafa SS et al. [
13]) and international (Marwa AF et al. [
14]; Lukovic et al. [
15]; Helal RM and Abou-El Wafa HS [
16]; Regina FA et al. [
17]) studies have focused on SM behavior among college and university students, recognizing surge and widespread practice in this specific category, identifying key factors such as socio-demographic settings, lifestyle, easy accessibility and availability of medications, good knowledge, advertisement, and high level of education [
18].
Moreover, the SM market is now on the rise [
19]. During 2020, the OTC drugs market size was valued at more than
$151 billion and anticipated to grow at a compound annual growth rate (CAGR) of over 5.1% between 2021 and 2027 (
$209 billion). The COVID-19 outbreak has significantly affected the sales of OTC drugs with an increased focus on personal health during the pandemic. This has considerably amplified the use of cold and flu products, along with vitamins. The OTC products not only reduce treatment costs significantly, but also increase the affordability of treatment for all patient classes [
20]. Various other scientific research studies have been conducted among AlMaarefa University (UM) students, such as the prevalence of stress [
21], consumption of caffeine [
22], sleep and academic performance [
23], and COVID-19 related anxiety [
24].
2. Materials and Methods
2.1. Study Design and Population
This institution-based cross-sectional study was conducted to investigate the level of knowledge, attitude, and practice of SM among undergraduate students of UM, Riyadh, Kingdom of Saudi Arabia. This study was approved by the institutional review board of UM with the registration number (03-02032021) and conducted over a period of four months from February to May 2021. Undergraduate students from the College of Pharmacy, the College of Medicine, and the College of Applied Sciences of UM were included. Students of other universities and those who disagreed to participate were excluded from this study.
2.2. Study Tool
The study employed a pre-designed validated structured questionnaire to collect the data, which was developed after an extensive literature review. The questionnaire was categorized into segments such as demography, knowledge, attitude, practice and student’s viewpoint and opinion regarding SM. The bilingual questionnaire was made available online to the students of UM through the university message center and other platforms. A consent form was displayed at the beginning of the questionnaire explaining the purpose of the study and assuring their identity and confidentiality. The participants had an option either to accept or reject participation.
2.3. Validity and Reliability of Study Tool
The content validation of the questionnaire was done by expert professors in the field. The face validity was tested by conducting two pilot studies on 30 students with a gap of one week (10 students each from the colleges of Pharmacy, Medicine, and Applied Sciences). These participants were excluded from the final sample. Necessary modifications were made based on the pre-test feedback. Additionally, Cronbach’s alpha factor (0.75) was calculated to check the questionnaire reliability. Repeat responses were identified by tracking student university ID and were excluded from data analysis.
2.4. Sampling Method and Sample Size
The sample size was determined using the single population proportion formula by assuming a 95% confidence level, 5% margin of error, and precision level of 5%. The proportion of SM observed in the pilot study was 66%. The number of students registered at UM was 2327. The correction formula was applied to calculate the final sample (300) size [
25]. However, to ensure more representative data and anticipating a few incomplete and repeat responses, we collected a larger sample size of 399.
2.5. Data Collection
Participant’s knowledge about responsible SM was assessed using 7 questions with a 7-point scale. All 7 questions were given a score of 1 or 0 (each correct response had a value of 1 and incorrect or do not know was given a value of 0). Assessment of participant’s knowledge about SM consisted of responsibility towards SM, when to discontinue SM drugs, antibiotics for self-use, and class of drugs for self-use. The expected maximum cumulative score was 7 and the minimum was 0. Participant’s knowledge was categorized as good, moderate, and poor using the original Bloom’s cut-off points (Good, 80–100%; Moderate, 50–79%; and Poor, <50%). A score of 6–7 points was considered good, moderate if the score was 4–5, and poor for a score of ≤3. Likewise, attitude towards responsible SM was assessed by putting 4 statements on a Likert’s scale, from strongly agree (5), agree (4), neutral (3), disagree (2), to strongly disagree (1). The maximum expected score was 20 and the minimum was 4. The level of attitude was classified using modified Bloom’s cut off points, as positive if the score was between 16–20 (80–100%), neutral for a score of 12–16 (60–79%), and negative if a score was less than 12 (<60%).
Students’ practice towards SM was measured using 8 questions that consisted of SM practice during the last six months, type of drug consumed, the reason for and frequency of SM, source of drug information, place of obtaining the drug, and negative impact of irrational SM. Students shared their viewpoints and opinions to rationalize and improvise the responsible SM and to spread the awareness towards SM through various platforms.
2.6. Data Processing and Analysis
The online responses collected were subjected to tests for completeness and consistency before processing for analysis. Incomplete and repeat responses were excluded from the analysis. The descriptive statistics were summarized by measuring frequency, percentage, and standard deviation. Variation in the adequacy of knowledge and attitude was hypothesized among students of various colleges; cross-tabulation was performed applying the chi-square test. Multiple stepwise linear regressions were applied to find out the relationship between scores of knowledge and attitude with participant’s characteristics. The analyzed data was systematically organized and presented in tabular, graphical, and narrative forms. SPSS (version 27.0, IBM, New York, NY, USA) was used to perform all statistical analyses. A p-value of less than 0.05 was considered significant.
4. Discussion
Rational and responsible SM is key not only for better health outcome, but also to limit adverse drug events, dosage, treatment errors, and risk of addiction or abuse. This study was conducted in students of UM, considering that health science students have adequate knowledge about medicines; hence, they are more aware of the consequences of improper SM. The UM student’s perception about SM will be valuable in judging the characteristics of their future medication handling, promoting health, and reducing drug-related problems.
In the present study, students’ overall adequacy of knowledge and attitude towards SM were satisfactory. Although SM has many pros and cons, it depends on who uses it and how it is used for self-treatment [
26]. In our study, we noticed that 55% of UM students took SM drugs during the last six months, which is lower compared to studies of students of King Khalid University, Abha [
12] (98.7%), Al-Qassim University [
13] (86.6%), Jazan University [
10] (87%), Bangladeshi Undergraduate Pharmacy Students [
27] (88%), Zabol University of Medical Sciences, Iran [
28] (57%), Kasturba Medical College, India [
29] (78.6%) and higher compared to students of Imam Abdulrahman Bin Faisal University in Dammam [
9] (26%). Comparing the results with findings from Serbia [
15], where the prevalence of SM was dependent on age and gender, our study showed no significant difference. We observed the significant impact of college (Pharmacy), the presence of long-term disease, and family members working in health on low liability to indulge in SM practice. The common reason for the high prevalence of SM might be academic knowledge about drugs.
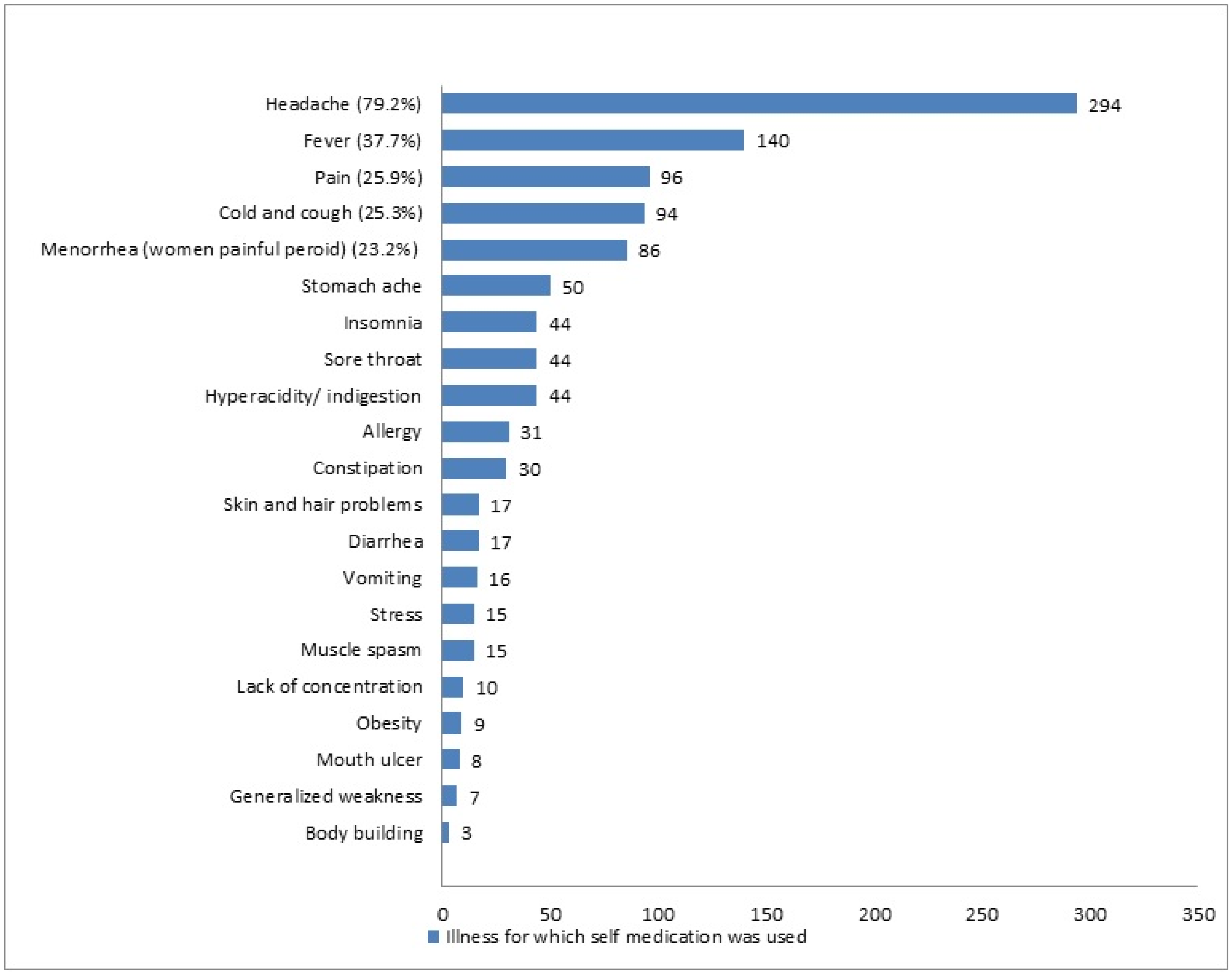
The study shows that 292 (78.7%) of the students are aware of responsible SM, similar to a previous study done in Kasturba Medical College, India [
29]. Like other previously published studies [
10,
13,
16,
27,
28,
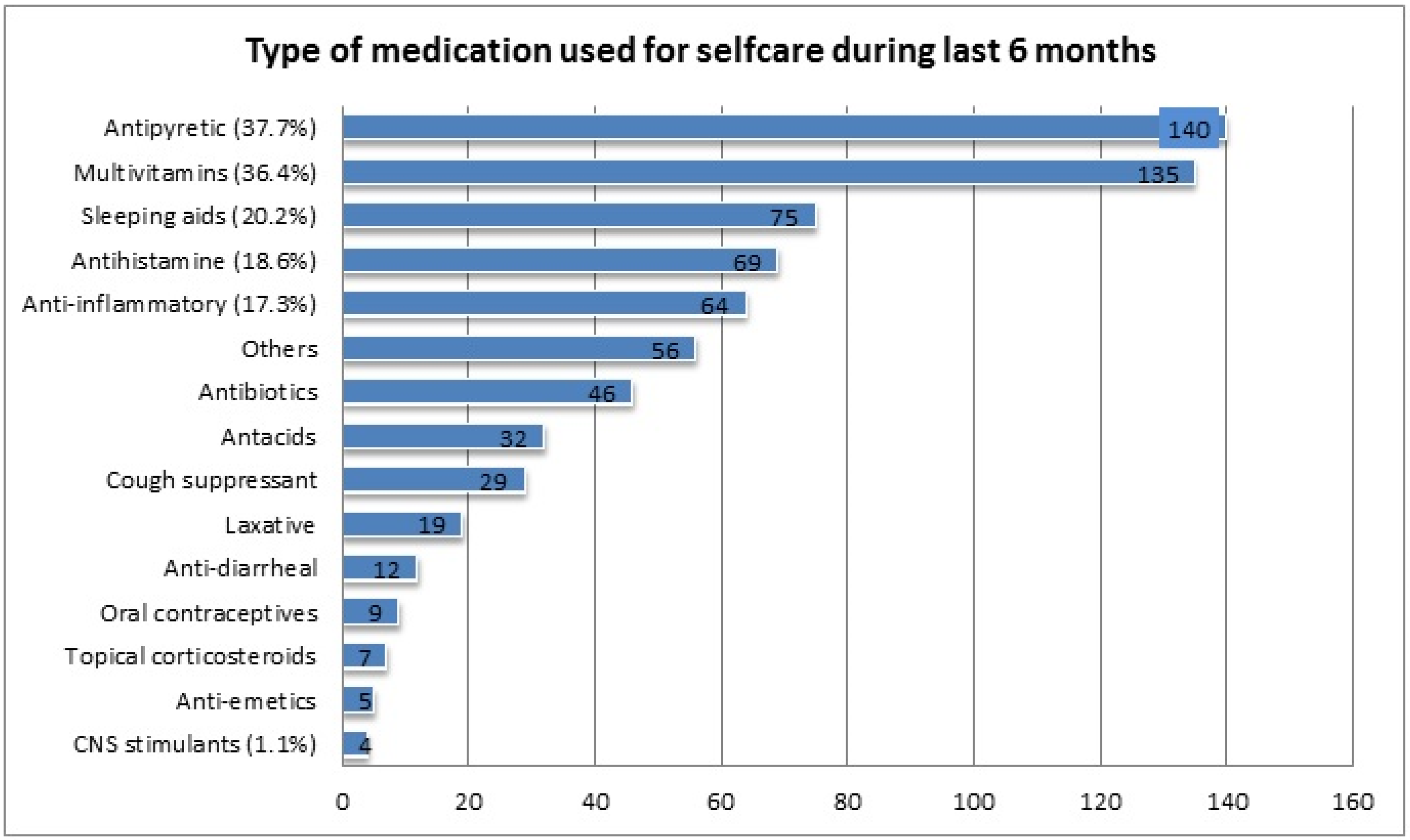
29], headache, fever, pain, cold, cough, and menorrhea were the most common illnesses for which SM was practiced. The most common type of medication preferred for self-use was antipyretic (37.7%), multivitamins (36.4%), antihistamines (18.6%), and anti-inflammatories (17.3%). Similar findings were reported in a study conducted on students of a Portuguese University [
17], and studies within Saudi Arabia [
9,
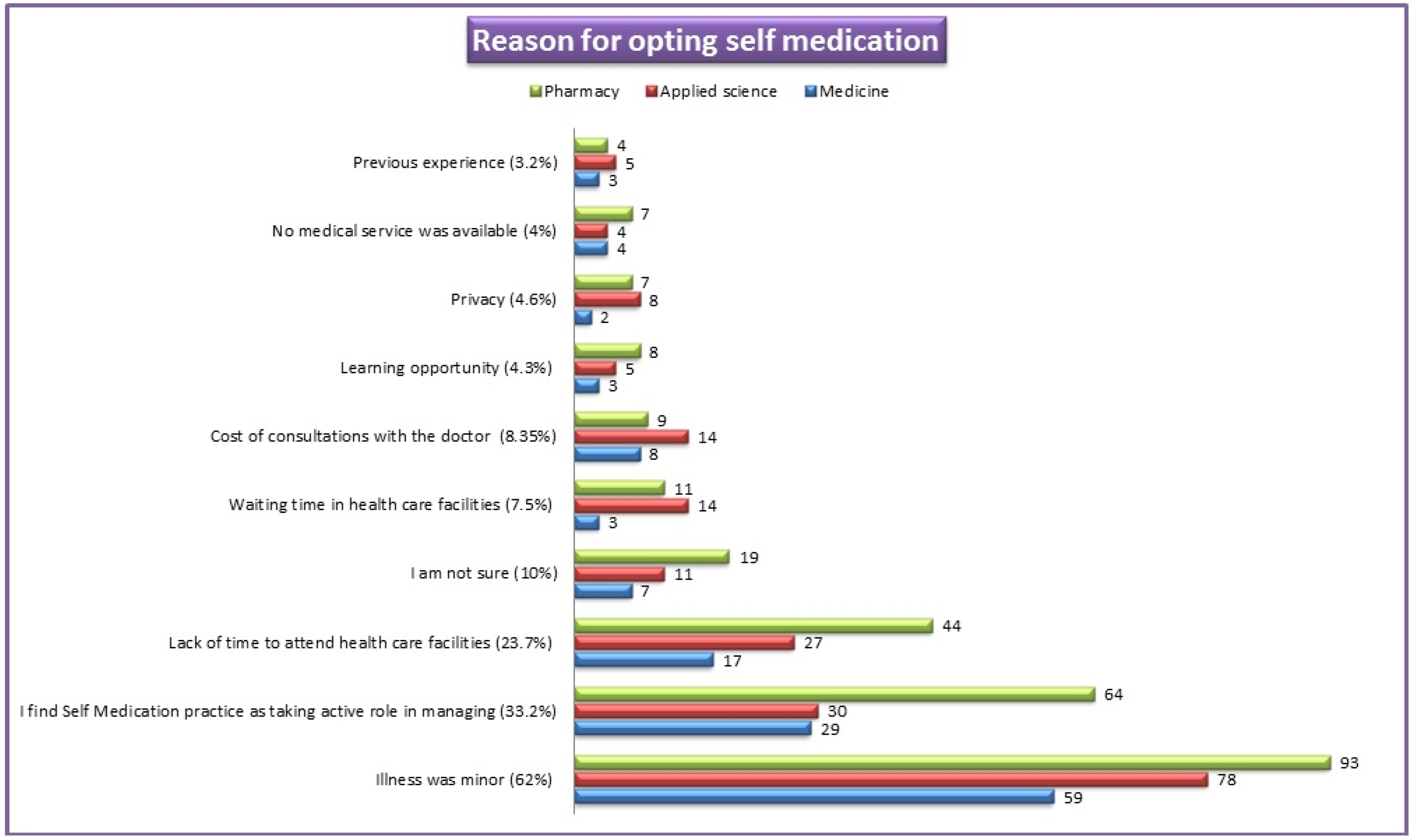
12]. The reasons mentioned by our students for opting for medication for self-care were minor illness (62%), previous experience (33.2%), and lack of time to attend the health care facility (23.7%). These findings are comparable with the outcomes reported by earlier studies [
9,
12,
16]. Improper SM practices may lead to the advancement of the disease, incorrect diagnosis, and promote serious health hazards. Easy availability of medicine, quick relief, and time-saving were the contributing factors for SM as reported by other studies [
29,
30]. Contrary to antipyretics and antihistamines, the use of antibiotics was much lower (12.4%). This practice indicates that students of UM have adequate knowledge about antimicrobial resistance and the consequences of irrational use of antibiotics. A similar finding has been quoted in a previous study [
27]. Our study has noticed that the pharmacy store was commonplace for obtaining a drug for SM. The key factor for SM practice was student’s adequate medication knowledge obtained during their course of study. These findings are similar to those reported in earlier studies [
12,
27,
28]. However, a study conducted on students of the city of Mansoura, Egypt [
16] quoted academic knowledge was the least important contributing factor. Our study noticed that the majority of respondents practiced SM once a month, which is comparable with the study conducted on students at Dammam University [
9]. The respondents of the present study have mentioned drug side effects, interaction, and resistance as major negative outcomes of irrational and unsupervised SM, which is contrary to the findings reported in the Zabol University of Medical Sciences, Iran [
28], where the highest number of respondents stated no negative impact of SM. Interestingly, students have shared their viewpoints and opinions regarding the rationalization and improvement of responsible SM and the conveying of awareness. A majority of respondents agree that creating awareness and education regarding the implication of self-medication would improvise and rationalize SM practice. This finding was comparable with the reports mentioned by students of Kasturba Medical College, India [
29]. The students have also mentioned the role of key platform such as the Ministry of Health and pharmaceutical companies in spreading the awareness regarding responsible SM.
The adequacy of knowledge among students of UM is satisfactory, unlike findings of King Khalid University [
12], where student’s knowledge about SM was poor. The student’s age, gender, study level, college of study, BMI, full/working student, and family member in the healthcare field had a significant impact on the level of knowledge. The level of knowledge increases dramatically as students progress to the higher study levels of the program. The study also showed that College of Pharmacy students (18.9%) had better knowledge regarding SM compared to students of the College of Medicine and Applied Sciences. Likewise, the respondent’s attitude towards responsible SM was greatly positive. In the present study, we observed the significant impact of gender, study level, full/working student, residential status, and marital status on attitude. As students progress to higher study levels of the program, a greater positive attitude towards SM has been observed. These observations are in line with studies conducted in other parts of Saudi Arabia [
9,
12]. In contrast, a study conducted on students of Taibah University [
31] observed a high level of negative attitudes towards SM. We observed a positive correlation between knowledge and attitude scores. An important finding in our study is that students of UM refer to books and academic knowledge to get medication information and retain a higher level of consciousness regarding the negative impact of irrational SM. Health professionals should play a predominant role in guiding self-medication behaviors in the general public.
4.1. Strengths and Limitations
A high response rate (399) was one of the strengths of this study. Students from all the study levels were accepted. Since the practice segment of the questionnaire was embedded with recall questions on drug use, the time period was restricted to the last six months to limit the recall bias. Considering the complexity of some survey questions, an online survey was set up bilingually (English and Arabic) to improve the understanding of questions. Since our study is cross-sectional, it is recommended to carry out prospective studies on student behavior regarding SM and determines factors influencing attitude and practice. Many respondents were busy with their exams, labs, and lectures during our study period and physical interaction was limited due to COVID-19 precautionary measures, hence data collection was strenuous. Although more than the required number of respondents completed the survey, many students still did not participate in our study.
4.2. Recommendations
Although students of UM reported having satisfactory and adequate perception regarding SM, it is suggested that offering an elective course highlighting the responsibility towards rational SM and the negative impact of irresponsible SM would be useful. Additionally, strategies to conduct small group work or workshops culminating in the impact of SM could be developed. We recommend the expansion of this study and encourage all the students of UM to complete the survey.







{kind=link}
{kind=link}
{kind=link}
{kind=link}