
Uganda Mountain Community Health System—Perspectives and Capacities towards Emerging Infectious Disease Surveillance



Abstract
:1. Introduction
2. Materials and Methods
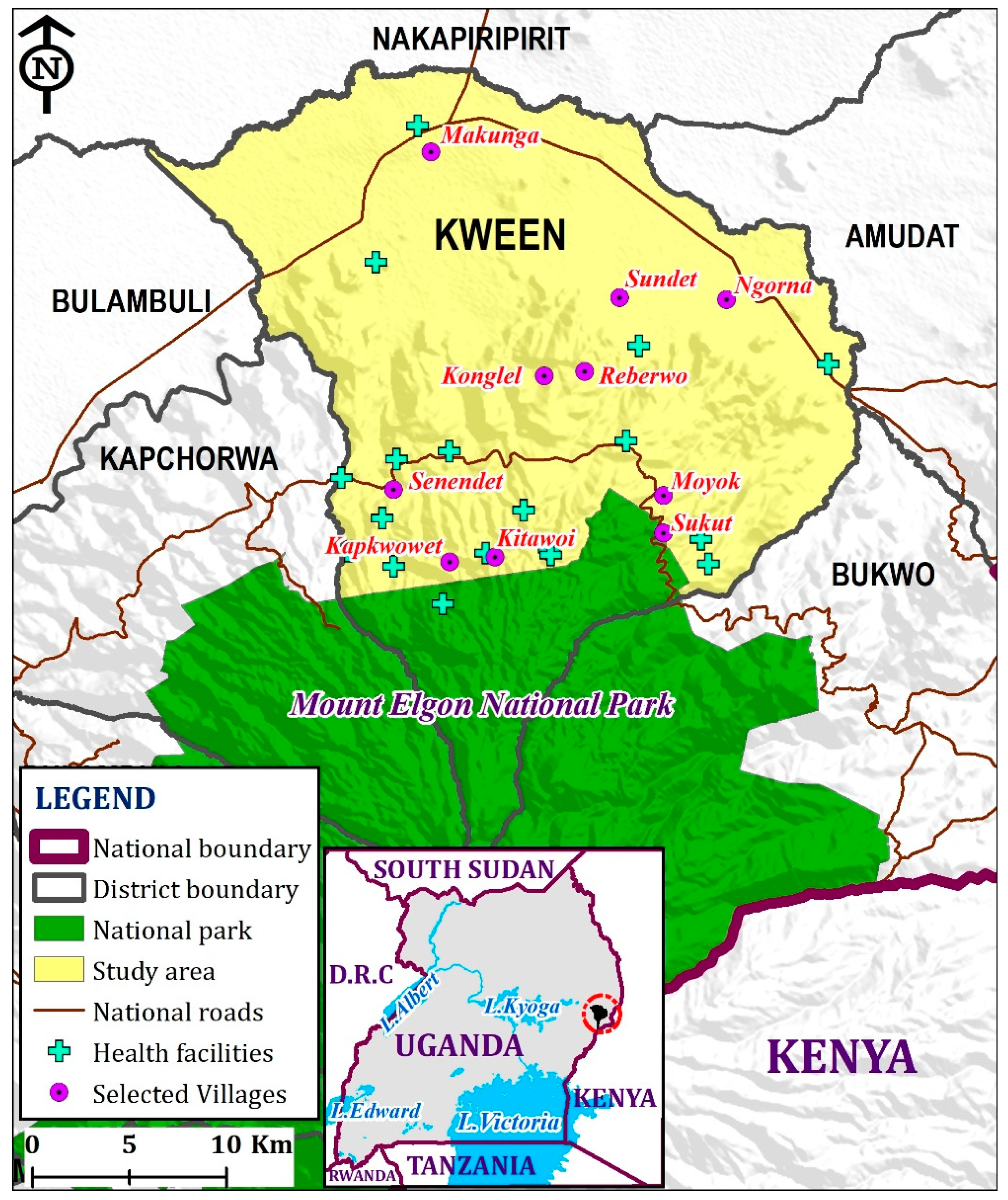
2.1. Study Site, Study Population, and Sampling Strategy
2.2. Data Collection
2.3. Scoring of Perceptions
2.4. Data Analysis
3. Results
3.1. Sociodemographic Characteristics
3.2. Perceptions on Climate Change and Impacts on Public Health
3.2.1. Rainfall and Temperature
“These days, the rainfall has greatly changed. Sometimes we receive abnormally large quantities of rainfall and sometimes it gets extremely low. The onset and cessation of these rains have greatly changed and hard to predict”. Noted by a VHT member.
“Temperature sometimes gets so high that even our water wells dry up. This is common now unlike in the past”. Noted by a VHT member.
3.2.2. Climate Change Events
“These days, floods are more common and especially in the flat areas of Greek, Ngenge and Sundet. This was not the case in the past because these rains at times come when they are too much”. Noted by a VHT member.
3.2.3. Climate Change Impacts on Health
“The malaria cases are now common in cold areas near Mt. Elgon national park and yet they were not there in the past. The mosquitoes are moving to these areas and it is because of the warming temperature there”. Noted by a VHT member.
“New diseases are now common that affect humans and livestock. These diseases include foot and mouth disease, Marburg, anthrax, and cholera. These diseases are coming up because of the changing climate associated with floods and high temperature”. Noted by a VHT member.
“We experience many environmental events like mud sliding, flooding of the rivers and yet this would cause diseases and also destroy our crops”. Noted by a VHT member.
3.3. Surveillance Capacities
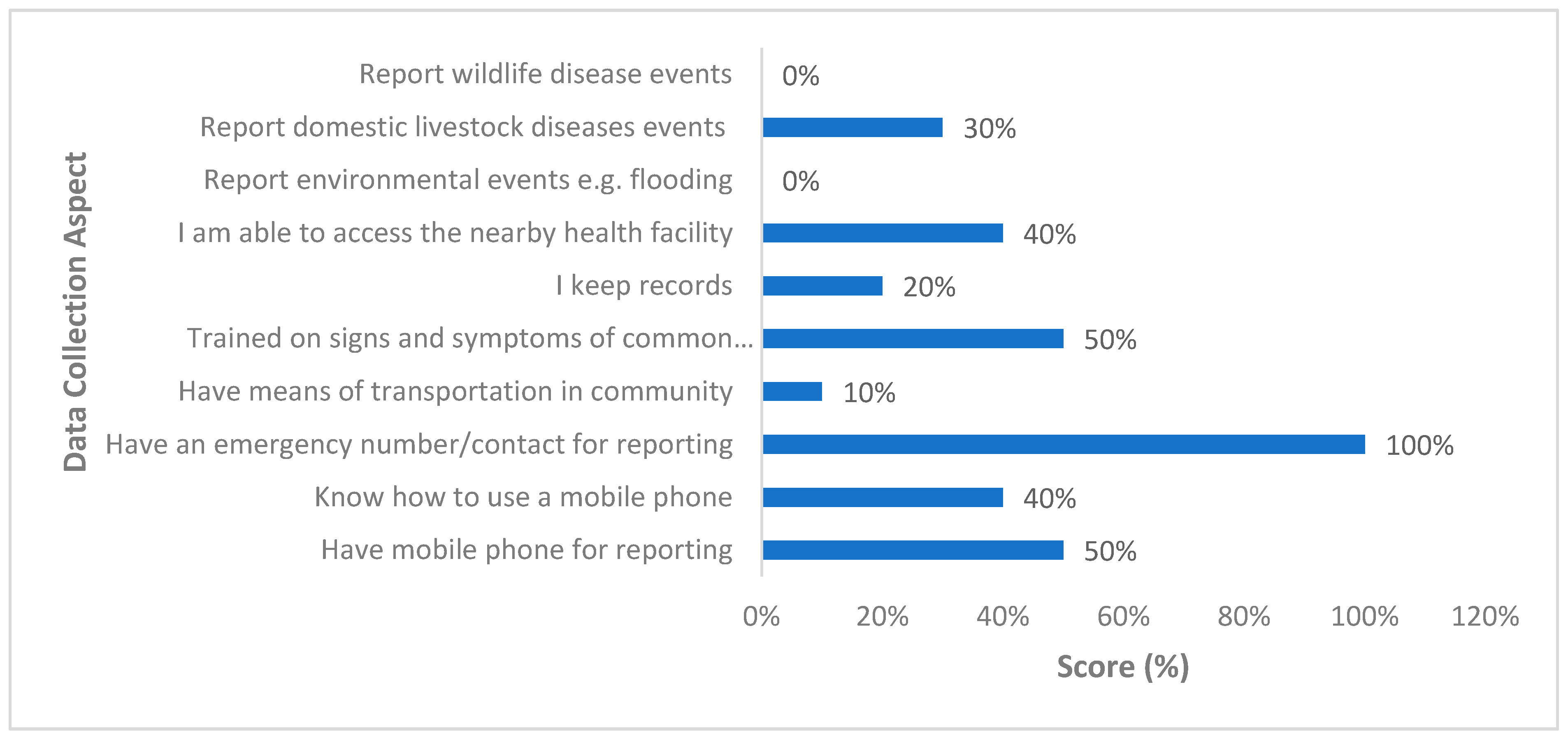
3.3.1. Data Collection
“I have a mobile phone but I am not well-versed with typing messages. I sometimes just give a friend/my child to type and send the message. But it is too much work because I have to explain to the person helping me to type and yet there is no payment for the service”. Noted by a VHT member.
3.3.2. Data Analysis
“We have been taught several times about the signs and symptoms of common diseases that’s why we are able to identify such patients in the community” Noted by a VHT member.
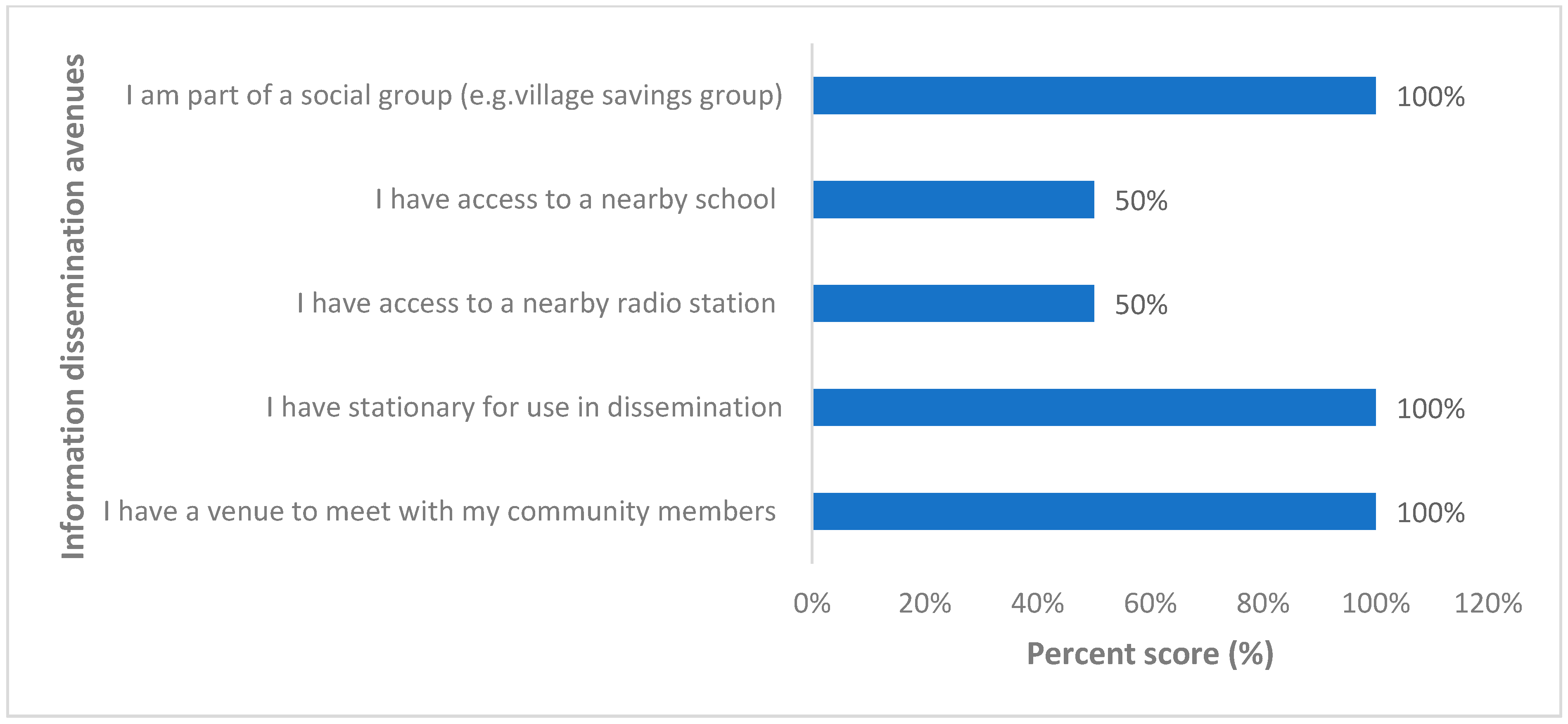
3.3.3. Information Dissemination
“I do community walks sometimes and meet with my community members. I can pass on the message on public health events while paying them a visit”. Noted by a VHT member. “I am part of the village savings team and sometimes I disseminate health-related messages to my teammates whenever we meet. I would reach out to the broader community but it is hard to reach out to all areas as it needs a transport means”. Noted by a VHT member.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cucinotta, D.; Vanelli, M. WHO Declares COVID-19 a Pandemic. Acta Biomed. Atenei. Parm. 2020, 91, 157–160. [Google Scholar] [CrossRef]
- Gupta, A.; Zhu, H.; Doan, M.K.; Michuda, A.; Majumder, B. Economic Impacts of the COVID−19 Lockdown in a Remittance-Dependent Region. Am. J. Agric. Econ. 2021, 103, 466–485. [Google Scholar] [CrossRef]
- WHO. WHO Coronavirus Disease. WHO. Int. 2021. Available online: https://covid19.who.int/table (accessed on 23 March 2021).
- Wang, L.-F.; Crameri, G. Emerging zoonotic viral diseases. Rev. Sci. Tech. l’OIE 2014, 33, 569–581. [Google Scholar] [CrossRef]
- Jones, K.; Patel, N.; Levy, M.; Storeygard, A.; Balk, D.; Gittleman, J.L.; Daszak, P. Global trends in emerging infectious diseases. Nat. Cell Biol. 2008, 451, 990–993. [Google Scholar] [CrossRef] [PubMed]
- Pisarski, K. The Global Burden of Disease of Zoonotic Parasitic Diseases: Top 5 Contenders for Priority Consideration. Trop. Med. Infect. Dis. 2019, 4, 44. [Google Scholar] [CrossRef] [Green Version]
- Nava, A.; Shimabukuro, J.S.; Chmura, A.A.; Luz, S.L.B. The Impact of Global Environmental Changes on Infectious Disease Emergence with a Focus on Risks for Brazil. ILAR J. 2017, 58, 393–400. [Google Scholar] [CrossRef] [Green Version]
- Woolhouse, M.; Gaunt, E. Ecological Origins of Novel Human Pathogens. Crit. Rev. Microbiol. 2007, 33, 231–242. [Google Scholar] [CrossRef]
- The World Bank. People, Pathogens and Our Planet; The World Bank: Washington, DC, USA, 2012. [Google Scholar]
- Gottwalt, A. Impact of deforestation on vector-borne disease incidence. J. Glob. Health 2013, 3, 16–19. [Google Scholar]
- Rulli, M.C.; Santini, M.; Hayman, D.T.S.; D’Odorico, P. The nexus between forest fragmentation in Africa and Ebola virus disease outbreaks. Sci. Rep. 2017, 7, srep41613. [Google Scholar] [CrossRef] [Green Version]
- Hahn, M.B.; Gurley, E.S.; Epstein, J.H.; Islam, M.S.; Patz, J.A.; Daszak, P.; Luby, S.P. The Role of Landscape Composition and Configuration on Pteropus giganteus Roosting Ecology and Nipah Virus Spillover Risk in Bangladesh. Am. J. Trop. Med. Hyg. 2014, 90, 247–255. [Google Scholar] [CrossRef] [Green Version]
- Food and Agricultural Organization of the United Nations (FAO). The Water-Energy-Food Nexus—A New Approach in Support of Food Security and Sustainable Agriculture; Food and Agriculture Organization of the United Nations: Rome, Italy, 2014; pp. 1–11. Available online: http://www.fao.org/3/a-bl496e.pdf (accessed on 23 March 2021).
- United Nations. World Urbanization Prospects: The 2014 Revision, Highlights (ST/ESA/SER.A/352); United Nations: New York, NY, USA, 2014. [Google Scholar]
- Wang, J.; Dong, K. What drives environmental degradation? Evidence from 14 Sub-Saharan African countries. Sci. Total Environ. 2019, 656, 165–173. [Google Scholar] [CrossRef]
- Fischer, T.; Byerlee, D.; Edmeades, G. Crop yields and global food security. Aust. Cent. Int. Agric. Res. 2014, 660, 8–11. [Google Scholar]
- Van Ittersum, M.K.; van Bussel, L.G.J.; Wolf, J.; Grassini, P.; van Wart, J.; Guilpart, N.; Claessens, L.; de Groot, H.; Wiebe, K.; Mason-D’Croz, D.; et al. Can sub-Saharan Africa feed itself? Proc. Natl. Acad. Sci. USA 2016, 113, 14964–14969. [Google Scholar] [CrossRef] [Green Version]
- Patz, J.A. Global climate change and emerging infectious diseases. JAMA 1996, 275, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Brooks, D.R.; Boeger, W. Climate change and emerging infectious diseases: Evolutionary complexity in action. Curr. Opin. Syst. Biol. 2019, 13, 75–81. [Google Scholar] [CrossRef]
- Carlson, C.J.; Albery, G.F.; Merow, C.; Trisos, C.H.; Zipfel, C.M.; Eskew, E.A.; Olival, K.; Ross, N.; Bansal, S. Climate change will drive novel cross-species viral transmission. BioRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Thurlow, J. COVID-19 lockdowns have imposed substantial economic costs on countries in Africa. COVID-19 Glob. Food Secur. 2020, 23–25. [Google Scholar]
- Resnick, D. COVID-19 lockdowns threaten Africa’s vital informal urban food trade. In COVID-19 Lockdowns Threaten Africa’s Vital Informal Urban Food Trade; International Food Policy Research Institute: Washington, DC, USA, 2020. [Google Scholar]
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, M.; Agha, R. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int. J. Surg. 2020, 78, 185–193. [Google Scholar] [CrossRef]
- Kohler, T.; Giger, M.; Hurni, H.; Ott, C.; Wiesmann, U.; Von Dach, S.W.; Maselli, D. Mountains and Climate Change: A Global Concern. Mt. Res. Dev. 2010, 30, 53–55. [Google Scholar] [CrossRef] [Green Version]
- Afrane, Y.A.; Githeko, A.K.; Yan, G. The ecology of Anopheles mosquitoes under climate change: Case studies from the effects of deforestation in East African highlands. Ann. N. Y. Acad. Sci. 2012, 1249, 204–210. [Google Scholar] [CrossRef]
- Githeko, A.; Ototo, E.; Guiyun, Y. Progress towards understanding the ecology and epidemiology of malaria in the western Kenya highlands: Opportunities and challenges for control under climate change risk. Acta Trop. 2012, 121, 19–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siya, A.; Kalule, B.J.; Ssentongo, B.; Lukwa, A.; Egeru, A. Malaria patterns across altitudinal zones of Mount Elgon following intensified control and prevention programs in Uganda. BMC Infect. Dis. 2020, 20, 1–16. [Google Scholar] [CrossRef]
- Ding, Y.; Peng, J. Impacts of Urbanization of Mountainous Areas on Resources and Environment: Based on Ecological Footprint Model. Sustainability 2018, 10, 765. [Google Scholar] [CrossRef] [Green Version]
- Gorokhovich, Y.; Doocy, S.; Walyawula, F.; Muwanga, A.; Nardi, F. Landslides in Bududa, Eastern Uganda: Preliminary Assessment and Proposed Solutions. In Landslide Science and Practice; Springer Science and Business Media LLC: Berlin, Germany, 2013; Volume 4, pp. 145–149. [Google Scholar]
- Mbonye, A.K.; Wamala, J.F.; Nanyunja, M.; Opio, A.; Makumbi, I.; Aceng, J.R. Ebola Viral Hemorrhagic Disease Outbreak in West Africa- Lessons from Uganda. Afr. Health Sci. 2014, 14, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Kwagonza, L.; Masiira, B.; Kyobe-Bosa, H.; Kadobera, D.; Atuheire, E.B.; Lubwama, B.; Kagirita, A.; Katushabe, E.; Kayiwa, J.T.; Lutwama, J.J.; et al. Outbreak of yellow fever in central and southwestern Uganda, February–May 2016. BMC Infect. Dis. 2018, 18, 548. [Google Scholar] [CrossRef]
- Okethwangu, D.; Birungi, D.; Biribawa, C.; Kwesiga, B.; Turyahabwe, S.; Ario, A.R.; Zhu, B. Multidrug-resistant tuberculosis outbreak associated with poor treatment adherence and delayed treatment: Arua District, Uganda, 2013–2017. BMC Infect. Dis. 2019, 19, 387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biribawa, C.; Atuhairwe, J.A.; Bulage, L.; Okethwangu, D.O.; Kwesiga, B.; Ario, A.R.; Zhu, B. Measles outbreak amplified in a pediatric ward: Lyantonde District, Uganda, August 2017. BMC Infect. Dis. 2020, 20, 398. [Google Scholar] [CrossRef]
- Ario, A.R.; Nsubuga, F.; Bulage, L.; Zhu, B. Investigating an outbreak of measles in Kamwenge District, Uganda, July 2015. Pan. Afr. Med. J. 2018, 30, 9. [Google Scholar] [CrossRef]
- Amanya, G.; Kizito, S.; Nabukenya, I.; Kalyango, J.; Atuheire, C.; Nansumba, H.; Abwoye, S.A.; Opio, D.N.; Kibuuka, E.; Karamagi, C. Risk factors, person, place and time characteristics associated with Hepatitis E Virus outbreak in Napak District, Uganda. BMC Infect. Dis. 2017, 17, 451. [Google Scholar] [CrossRef] [Green Version]
- Shoemaker, T.R.; Nyakarahuka, L.; Balinandi, S.; Ojwang, J.; Tumusiime, A.; Mulei, S.; Kyondo, J.; Lubwama, B.; Sekamatte, M.; Namutebi, A.; et al. First Laboratory-Confirmed Outbreak of Human and Animal Rift Valley Fever Virus in Uganda in 48 Years. Am. J. Trop. Med. Hyg. 2019, 100, 659–671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mbonye, A.K.; Sekamatte, M. Disease outbreaks and reporting in Uganda. Lancet 2018, 392, 2347–2348. [Google Scholar] [CrossRef] [Green Version]
- Kisaakye, E.; Ario, A.R.; Bainomugisha, K.; Cossaboom, C.M.; Lowe, D.; Bulage, L.; Kadobera, D.; Sekamatte, M.; Lubwama, B.; Tumusiime, D.; et al. Outbreak of Anthrax Associated with Handling and Eating Meat from a Cow, Uganda, 2018. Emerg. Infect. Dis. 2020, 26, 2799–2806. [Google Scholar] [CrossRef] [PubMed]
- Nanteza, M.B.; Bakamutumaho, B.; Kisakye, A.; Namuwulya, P.; Bukenya, H.; Katushabe, E.; Bwogi, J.; Byabamazima, C.R.; Williams, R.; Gumede, N. The detection of 3 ambiguous type 2 vaccine-derived polioviruses (VDPV2s) in Uganda. Virol. J. 2018, 15, 77. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Weekly Bulletin on Outbreaks and Other Emergencies; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- Nyakarahuka, L.; Skjerve, E.; Nabadda, D.; Sitali, D.C.; Mumba, C.; Mwiine, F.N.; Lutwama, J.J.; Balinandi, S.; Shoemaker, T.; Kankya, C. Knowledge and attitude towards Ebola and Marburg virus diseases in Uganda using quantitative and participatory epidemiology techniques. PLoS Negl. Trop. Dis. 2017, 11, e0005907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nyakarahuka, L.; Shoemaker, T.R.; Balinandi, S.; Chemos, G.; Kwesiga, B.; Mulei, S.; Kyondo, J.; Tumusiime, A.; Kofman, A.; Masiira, B.; et al. Marburg virus disease outbreak in Kween District Uganda, 2017: Epidemiological and laboratory findings. PLoS Negl. Trop. Dis. 2019, 13, e0007257. [Google Scholar] [CrossRef] [PubMed]
- Bomuhangi, A.; Nabanoga, G.; Namaalwa, J.J.; Jacobson, M.G. Local communities’ perceptions of climate variability in the Mt. Elgon region, eastern Uganda. Cogent Environ. Sci. 2016, 2, 1–16. [Google Scholar] [CrossRef]
- Tiyo, C.E.; Orach-Meza, F.L.; Edroma, E.L. Understanding Small-Scale Farmers’ Perception and Adaption Strategies to Climate Change Impacts: Evidence from Two Agro-Ecological Zones Bordering National Parks of Uganda. J. Agric. Sci. 2015, 7, 253. [Google Scholar] [CrossRef] [Green Version]
- Mulinde, C.; Majaliwa, J.; Twinomuhangi, R.; Mfitumukiza, D.; Komutunga, E.; Ampaire, E.; Asiimwe, J.; Van Asten, P.; Jassogne, L. Perceived climate risks and adaptation drivers in diverse coffee landscapes of Uganda. NJAS Wagening. J. Life Sci. 2019, 88, 31–44. [Google Scholar] [CrossRef]
- Jiang, B.; Bamutaze, Y.; Pilesjö, P. Climate change and land degradation in Africa: A case study in the Mount Elgon region, Uganda. Geo Spatial Inf. Sci. 2014, 17, 39–53. [Google Scholar] [CrossRef] [Green Version]
- Egeru, A. Climate risk management information, sources and responses in a pastoral region in East Africa. Clim. Risk Manag. 2016, 11, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Egeru, A. Role of indigenous knowledge in climate change adaptation: A case study of the Teso sub-region, Eastern Uganda. Indian J. Tradit. Knowl. 2012, 11, 217–224. [Google Scholar]
- Makame, M.O.; Shackleton, S. Perceptions of climate variability and change in relation to observed data among two east coast communities in Zanzibar, East Africa. Clim. Dev. 2020, 12, 801–813. [Google Scholar] [CrossRef]
- Cuni-Sanchez, A.; Omeny, P.; Pfeifer, M.; Olaka, L.; Mamo, M.B.; Marchant, R.; Burgess, N.D. Climate change and pastoralists: Perceptions and adaptation in montane Kenya. Clim. Dev. 2019, 11, 513–524. [Google Scholar] [CrossRef] [Green Version]
- Yvonne, M.; Ouma, G.; Olago, D.; Opondo, M. Trends in Climate Variables (Temperature and Rainfall) and Local Perceptions of Climate Change In Lamu, Kenya. Geogr. Environ. Sustain. 2020, 13, 102–109. [Google Scholar] [CrossRef]
- Kimbugwe, G.; Mshilla, M.; Oluka, D.; Nalikka, O.; Kyangwa, J.; Zalwango, S.; Kilizza, U.; Turyasiima, M.; Ntambazi, L.; Walugembe, F.; et al. Challenges Faced by Village Health Teams (VHTs) in Amuru, Gulu and Pader Districts in Northern Uganda. Open J. Prev. Med. 2014, 4, 740–750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brunie, A.; Wamala-Mucheri, P.; Otterness, C.; Akol, A.; Chen, M.; Bufumbo, L.; Weaver, M. Keeping community health workers in Uganda motivated: Key challenges, facilitators, and preferred program inputs. Glob. Health Sci. Pract. 2014, 2, 103–116. [Google Scholar] [CrossRef]
- Mays, D.C.; O’Neil, E.J.; Mworozi, E.A.; Lough, B.J.; Tabb, Z.J.; Whitlock, A.E.; Mutimba, E.M.; Talib, Z.M. Supporting and retaining Village Health Teams: An assessment of a community health worker program in two Ugandan districts. Int. J. Equity Health 2017, 16, 129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Donovan, J.; Hamala, R.; Namanda, A.S.; Musoke, D.; Ssemugabo, C.; Winters, N. ‘We are the people whose opinions don’t matter’. A photovoice study exploring challenges faced by community health workers in Uganda. Glob. Public Health 2020, 15, 384–401. [Google Scholar] [CrossRef]
- Perry, S.; Fair, C.D.; Burrowes, S.; Holcombe, S.J.; Kalyesubula, R. Outsiders, insiders, and intermediaries: Village health teams’ negotiation of roles to provide high quality sexual, reproductive and HIV care in Nakaseke, Uganda. BMC Health Serv. Res. 2019, 19, 1–12. [Google Scholar] [CrossRef]
- Turinawe, E.B.; Rwemisisi, J.T.; Musinguzi, L.K.; De Groot, M.; Muhangi, D.; De Vries, D.H.; Mafigiri, D.K.; Pool, R. Selection and performance of village health teams (VHTs) in Uganda: Lessons from the natural helper model of health promotion. Hum. Resour. Health 2015, 13, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Brunie, A.; Mucheri, P.N.W.; Akol, A.; Chen, M.; Mercer, S.J.; Petruney, T. Integrating Family Planning and HIV Services at the Community Level: Formative Assessment with Village Health Teams in Uganda. Afr. J. Reprod. Health 2017, 21, 73–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ojo, T.T.; Hawley, N.L.; Desai, M.M.; Akiteng, A.R.; Guwatudde, D.; Schwartz, J.I. Exploring knowledge and attitudes toward non-communicable diseases among village health teams in Eastern Uganda: A cross-sectional study. BMC Public Health 2017, 17, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boyce, M.R.; Katz, R. Community Health Workers and Pandemic Preparedness: Current and Prospective Roles. Front. Public Health 2019, 7, 62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buregyeya, E.; Atusingwize, E.; Nsamba, P.; Musoke, D.; Naigaga, I.; Kabasa, J.D.; Amuguni, H.; Bazeyo, W. Operationalizing the One Health Approach in Uganda: Challenges and Opportunities. J. Epidemiol. Glob. Health 2020, 10, 250–257. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Village * | Konglel | Reberwo | Ngorna | Sundet | Kitawoi | Kapkwowet | Sukut | Senendet | Magunga | Moyok |
|---|---|---|---|---|---|---|---|---|---|---|
| Average herd size (number of cows) | 12 ± 3 | 14 ± 3 | 19 ± 2 | 22 ± 1 | 6 ± 4 | 12 ± 9 | 7 ± 2 | 12 ± 1 | 16 ± 3 | 13 ± 3 |
| Average herd size (number of sheep) | 1 ± 1 | 0 | 3 ± 5 | 5 ± 3 | 0 | 0 | 0 | 0 | 1 ± 1 | 2 ± 7 |
| Average herd size goats | 16 ± 7 | 13 ± 1 | 22 ± 2 | 26 ± 6 | 11 ± 3 | 5 ± 5 | 14 ± 2 | 13 ± 4 | 11 ± 2 | 12 ± 9 |
| Average farm size (ha) | 1 ± 2 | 1.2 ± 5 | 12 ± 1 | 25 ± 3 | 1 ± 3 | 1.3 ± 1 | 1.1 ± 2 | 1 ± 3 | 1.2 ± 2 | 1 ± 2 |
| Level of access to water source point | Medium | Yes | Low | Low | Medium | Medium | Medium | Medium | Low | Medium |
| Access to electricity | No | No | No | No | No | No | No | No | No | Yes |
| Number of nearby primary schools | 4 | 3 | 2 | 2 | 4 | 2 | 2 | 1 | 3 | 4 |
| Number of nearby secondary schools | 2 | 2 | 1 | 1 | 2 | 2 | 2 | 2 | 2 | 2 |
| Where do you access health services? Traditional healer or Western medicine? | Both | Both | Both | Both | Both | Both | Both | Both | Both | Both |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siya, A.; Mafigiri, R.; Migisha, R.; Kading, R.C. Uganda Mountain Community Health System—Perspectives and Capacities towards Emerging Infectious Disease Surveillance. Int. J. Environ. Res. Public Health 2021, 18, 8562. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168562
Siya A, Mafigiri R, Migisha R, Kading RC. Uganda Mountain Community Health System—Perspectives and Capacities towards Emerging Infectious Disease Surveillance. International Journal of Environmental Research and Public Health. 2021; 18(16):8562. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168562
Chicago/Turabian StyleSiya, Aggrey, Richardson Mafigiri, Richard Migisha, and Rebekah C. Kading. 2021. "Uganda Mountain Community Health System—Perspectives and Capacities towards Emerging Infectious Disease Surveillance" International Journal of Environmental Research and Public Health 18, no. 16: 8562. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168562