
Implementation, Mechanisms and Context of the MAMAACT Intervention to Reduce Ethnic and Social Disparity in Stillbirth and Infant Health


 , , and
, , and
Abstract
:1. Introduction
Aims
- To analyze the implementation of the MAMAACT intervention in relation to which elements were implemented and how (dose, reach, and fidelity);
- To identify important mechanisms of impact by examining participants’ responses to and interactions with the intervention;
- To analyze how contextual factors enabled or hindered the implementation process and the intended mechanisms and outcomes of the intervention.
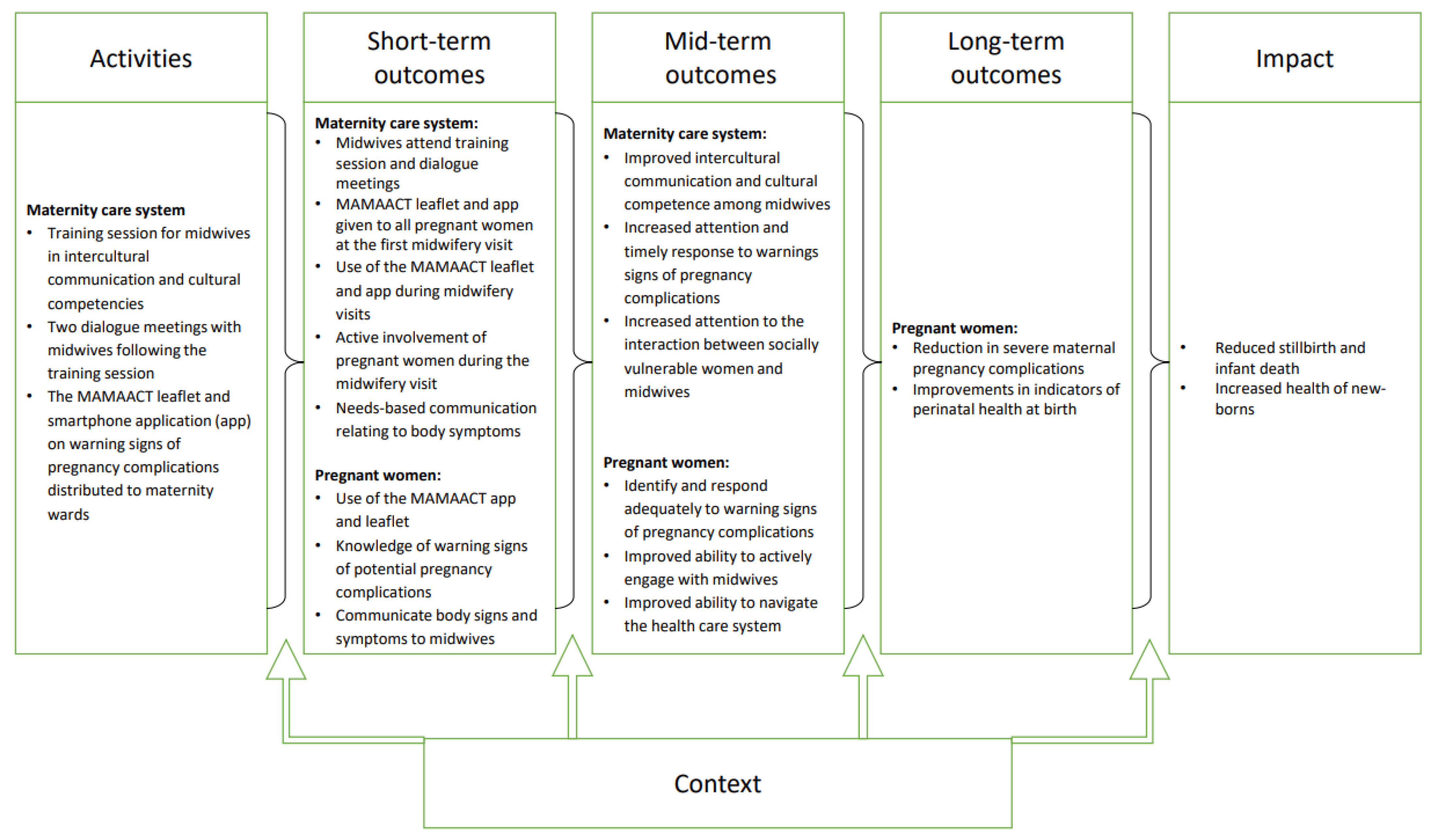
2. The Framework of the Intervention
2.1. Setting
2.2. The MAMAACT Intervention and the Intended Implementation
- A six-hour training session for all midwives working in ANC in intercultural communication and cultural competence;
- Two one-hour follow-up dialogue meetings with ANC midwives;
- Health education materials (leaflet and smartphone app) on warning signs of severe pregnancy complications and how to respond for pregnant women.
2.2.1. Training Session in Intercultural Communication and Competence
2.2.2. The Dialogue Meetings
2.2.3. The Leaflet and App
3. Materials and Methods
3.1. Implementation
3.1.1. Reach and Dose
3.1.2. Fidelity and Adaptations
3.2. Mechanisms of Impact
3.3. Context
4. Results
4.1. Implementation
4.1.1. Reach and Dose
4.1.2. Fidelity and Adaption
“… it is a great supplement to the most insecure women. For the more resourceful it seems too simple”(W1, meeting 1.3).
“They (the midwives) experience a lot of one-way communication”(W6, meeting 1.2).
“The midwives express more awareness about preconceptions and less stigmatization”(W4, meeting 1.1).
“The important things we would like to come around drown in those things we have to do KRAM (assessment of diet, smoking, alcohol and physical activity), urine tests, etc.”(W7, meeting 2.5).
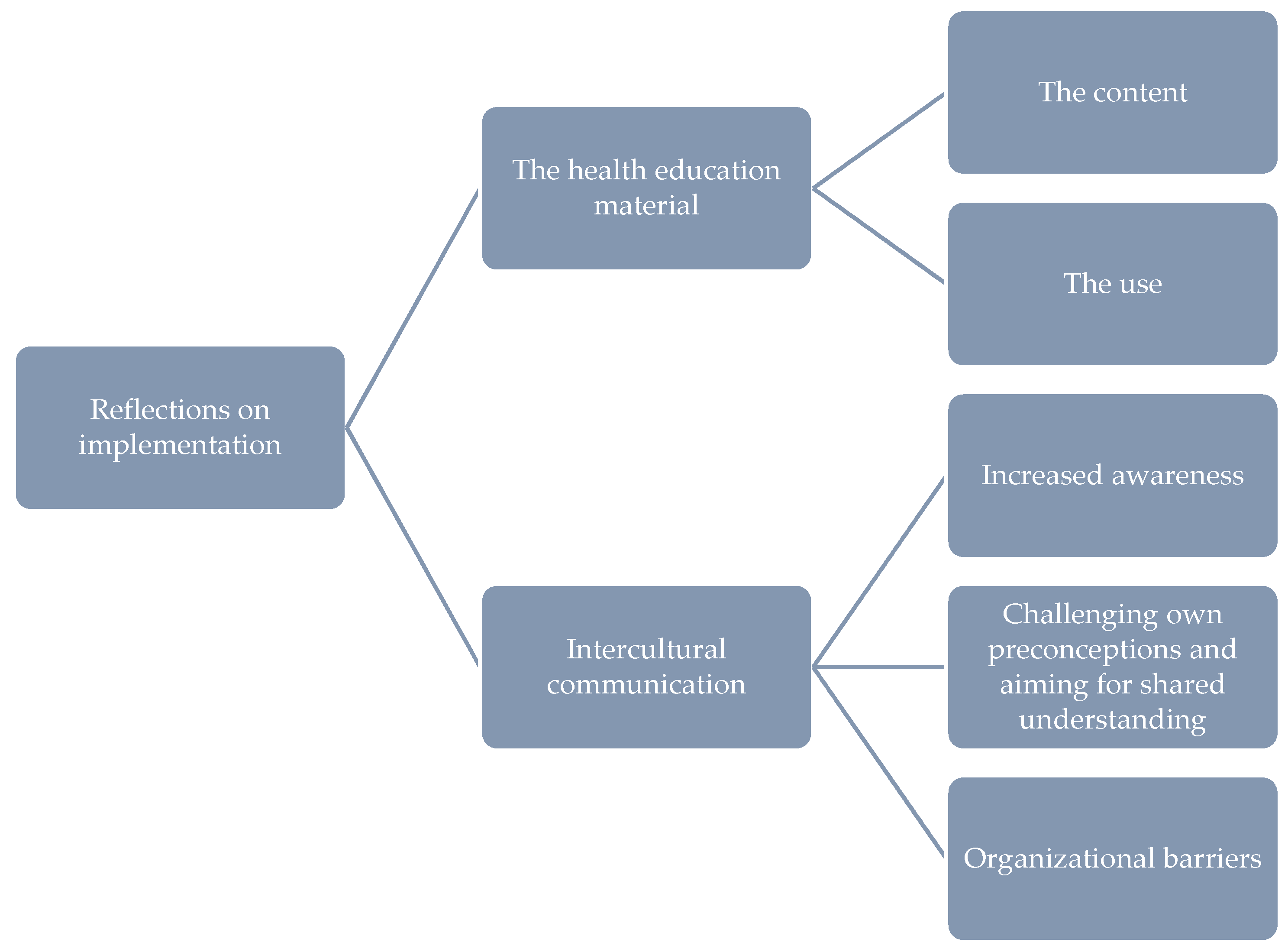
4.2. Mechanisms
4.3. Contextual Factors
5. Discussion
5.1. Main Findings and Interpretations
5.2. Strengths and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tweed, E.J.; Mackay, D.F.; Nelson, S.M.; Cooper, S.-A.; Pell, J.P. Five-minute Apgar score and educational outcomes: Retrospective cohort study of 751|369 children. Arch. Dis. Child. Fetal Neonatal Ed. 2016, 101, F121–F126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Small, R.; Gagnon, A.; Gissler, M.; Zeitlin, J.; Bennis, M.; Glazier, R.; Haelterman, E.; Martens, G.; McDermott, S.; Urquia, M.; et al. Somali women and their pregnancy outcomes postmigration: Data from six receiving countries. BJOG 2008, 115, 1630–1640. [Google Scholar] [CrossRef] [PubMed]
- Reeske, A.; Razum, O. Maternal and child health—From conception to first birthday. In Migration and Health in the European Union; Rechel, B., Mladovsky, P., Deville, W., Rijks, B., Petrova-Benedict, R., Mckee, M., Eds.; European Observatory on Health Systems and Policies Series; McGraw Hill/Open University Press: Maidenhead, UK, 2011; ISBN 9780335245673. [Google Scholar]
- World Health Organization. Improving the Health Care of Pregnant Refugee and Migrant Women and Newborn Children; Technical Guidance; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2018. [Google Scholar]
- Flenady, V.; Wojcieszek, A.M.; Middleton, P.; Ellwood, D.; Erwich, J.J.; Coory, M.; Khong, T.Y.; Silver, R.M.; Smith, G.C.S.; Boyle, F.M.; et al. Stillbirths: Recall to action in high-income countries. Lancet 2016, 387, 691–702. [Google Scholar] [CrossRef] [Green Version]
- Bilsteen, J.F.; Andresen, J.B.; Mortensen, L.H.; Hansen, A.V.; Andersen, A.M.N. Educational disparities in perinatal health in Denmark in the first decade of the 21st century: A register-based cohort study. BMJ Open 2018, 8, e023531. [Google Scholar] [CrossRef] [PubMed]
- Gissler, M.; Alexander, S.; Macfarlane, A.; Small, R.; Stray-Pedersen, B.; Zeitlin, J.; Zimbeck, M.; Gagnon, A. Stillbirths and infant deaths among migrants in industrialized countries. Acta Obstet. Gynecol. Scand. 2009, 88, 134–148. [Google Scholar] [CrossRef]
- Urquia, M.L.; Glazier, R.H.; Mortensen, L.; Nybo-Andersen, A.M.; Small, R.; Davey, M.A.; Rööst, M.; Essén, B. Severe maternal morbidity associated with maternal birthplace in three high-immigration settings. Eur. J. Public Health 2015, 25, 620–625. [Google Scholar] [CrossRef] [Green Version]
- Christensen, M.B.; Villadsen, S.F.; Weber, T.; Wilken-jensen, C.; Andersen, A.N. Higher rate of serious perinatal events in non-Western women in Denmark. Dan. Med. J. 2016, 63, A5197. [Google Scholar]
- Urquia, M.L.; Ying, I.; Glazier, R.H.; Berger, H.; De Souza, L.R.; Ray, J.G. Serious Preeclampsia Among Different Immigrant Groups. J. Obstet. Gynaecol. Can. 2012, 34, 348–352. [Google Scholar] [CrossRef]
- Essén, B.; Bödker, B.; Sjöberg, N.O.; Langhoff-Roos, J.; Greisen, G.; Gudmundsson, S.; Östergren, P.O. Are some perinatal deaths in immigrant groups linked to suboptimal perinatal care services? BJOG Int. J. Obstet. Gynaecol. 2002, 109, 677–682. [Google Scholar] [CrossRef] [Green Version]
- Jonkers, M.; Richters, A.; Zwart, J.; Öry, F.; van Roosmalen, J. Severe maternal morbidity among immigrant women in the Netherlands: Patients’ perspectives. Reprod. Health Matters 2011, 19, 144–153. [Google Scholar] [CrossRef] [Green Version]
- Dixon-Woods, M.; Cavers, D.; Agarwal, S.; Annandale, E.; Arthur, A.; Harvey, J.; Hsu, R.; Katbamna, S.; Olsen, R.; Smith, L.; et al. Conducting a critical interpretive synthesis of the literature on access to healthcare by vulnerable groups. BMC Med. Res. Methodol. 2006, 6, 35. [Google Scholar] [CrossRef]
- Dubbin, L.A.; Chang, J.S.; Shim, J.K. Cultural health capital and the interactional dynamics of patient-centered care. Soc. Sci. Med. 2013, 93, 113–120. [Google Scholar] [CrossRef] [Green Version]
- Kleinman, A.; Benson, P. Anthropology in the clinic: The problem of cultural competency and how to fix it. PLoS Med. 2006, 3, e294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seeleman, C.; Suurmond, J.; Stronks, K. Cultural competence: A conceptual framework for teaching and learning. Med. Educ. 2009, 43, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Brorsen, E.; Rasmussen, T.D.; Ekstrøm, C.T.; Osborne, R.H.; Villadsen, S.F. Health literacy responsiveness: A cross-sectional study among pregnant women in Denmark. Scand. J. Public Health 2021, 14034948211004320. [Google Scholar] [CrossRef]
- Brega, A.G.; Hamer, M.K.; Albright, K.; Brach, C.; Saliba, D.; Abbey, D.; Gritz, R.M. Organizational Health Literacy: Quality Improvement Measures with Expert Consensus. Health Lit. Res. Pract. 2019, 3, e127–e146. [Google Scholar] [CrossRef] [Green Version]
- Nawabi, F.; Krebs, F.; Vennedey, V.; Shukri, A.; Lorenz, L.; Stock, S. Health literacy in pregnant women: A systematic review. Int. J. Environ. Res. Public Health 2021, 18, 3847. [Google Scholar] [CrossRef]
- Rasmussen, T.D.; Villadsen, S.F.; Andersen, P.K.; Jervelund, S.S.; Andersen, A.-M.N. Social and ethnic disparities in stillbirth and infant death in Denmark, 2005–2006. Sci. Rep. 2021, 11, 8001. [Google Scholar] [CrossRef]
- Villadsen, S.F.; Mortensen, L.H.; Andersen, A.M.N. Care during pregnancy and childbirth for migrant women: How do we advance? Development of intervention studies—The case of the MAMAACT intervention in Denmark. Best Pract. Res. Clin. Obstet. Gynaecol. 2016, 32, 100–112. [Google Scholar] [CrossRef]
- Johnsen, H.; Ghavami Kivi, N.; Morrison, C.H.; Juhl, M.; Christensen, U.; Villadsen, S.F. Addressing ethnic disparity in antenatal care: A qualitative evaluation of midwives’ experiences with the MAMAACT intervention. BMC Pregnancy Childbirth 2020, 20, 118. [Google Scholar] [CrossRef]
- Statistics Denmark Immigrants in Denmark 2020 [Indvandrere i Danmark 2020]; Statistics Denmark: Copenhagen, Denmark, 2020.
- Osborne, R.H.; Batterham, R.W.; Elsworth, G.R.; Hawkins, M.; Buchbinder, R. The grounded psychometric development and initial validation of the Health Literacy Questionnaire (HLQ). BMC Public Health 2013, 13, 658. [Google Scholar] [CrossRef] [Green Version]
- Moore, G.F.; Audrey, S.; Barker, M.; Bond, L.; Bonell, C.; Hardeman, W.; Moore, L.; O’Cathain, A.; Tinati, T.; Wight, D.; et al. Process evaluation of complex interventions: Medical Research Council guidance. BMJ Br. Med. J. 2015, 350, h1258. [Google Scholar] [CrossRef] [Green Version]
- Moore, G.F.; Audrey, S.; Barker, M.; Bond, L.; Bonell, C.; Hardeman, W.; Moore, L.; O’Cathain, A.; Tinati, T.; Wight, D. Process Evaluation of Complex Interventions: UK Medical Research (MRC) Guidance. Available online: https://mrc.ukri.org/documents/pdf/mrc-phsrn-process-evaluation-guidance-final/ (accessed on 6 June 2021).
- Marmot, M. Social justice, epidemiology and health inequalities. Eur. J. Epidemiol. 2017, 32, 537–546. [Google Scholar] [CrossRef] [PubMed]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. BMJ 2008, 337, 29–983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Craig, P.; Di Ruggiero, E.; Frohlich, K.L.; Mykhalovskiy, E.; White, M.; Campbell, R.; Cummins, S.; Edwards, N.; Hunt, K.; Kee, F.; et al. Taking Account of Context in Population Health Intervention Research: Guidance for Producers, Users and Funders of Research; National Institute for Health Research University of Southampton: Southampton, UK, 2018. [Google Scholar]
- Johnsen, H.; Christensen, U.; Juhl, M.; Villadsen, S.F. Contextual factors influencing the MAMAACT intervention: A qualitative study of non-western immigrant women’s response to potential pregnancy complications in everyday life. Int. J. Environ. Res. Public Health 2020, 17, 1040. [Google Scholar] [CrossRef] [Green Version]
- Johnsen, H.; Christensen, U.; Juhl, M.; Villadsen, S.F. Implementing the MAMAACT intervention in Danish antenatal care: A qualitative study of non-Western immigrant women’s and midwives’ attitudes and experiences. Midwifery 2021, 95, 102935. [Google Scholar] [CrossRef]
- Johnsen, H.; Christensen, U.; Juhl, M.; Villadsen, S.F. Organisational barriers to implementing the MAMAACT intervention to improve maternity care for non-Western immigrant women: A qualitative evaluation. Int. J. Nurs. Stud. 2020, 111, 103742. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health The National Health Act. Available online: https://www.retsinformation.dk/eli/lta/2019/903 (accessed on 4 June 2021).
- Danish Health Authority. Anbefalinger for Svangreomsorgen [Recommendations for Antenatal Care]; Danish Health Authority: Copenhagen, Denmark, 2013; ISBN 9788776769062. [Google Scholar]
- Mothers, N. Introduction to Neighbourhood Mothers. Available online: https://bydelsmor.dk/english (accessed on 6 June 2021).
- Statistics Denmark. Immigrants in Denmark 2019 [Indvandrere i Danmark 2019]; Statistics Denmark: Copenhagen, Denmark, 2019. [Google Scholar]
- Malterud, K. Systematic text condensation: A strategy for qualitative analysis. Scand. J. Public Health 2012, 40, 795–805. [Google Scholar] [CrossRef]
- Riishede Christiansen, I. PRESIDE—First Trimester Screening for Preeclampsia. Available online: https://www.rigshospitalet.dk/afdelinger-og-klinikker/julianemarie/obstetrisk-afdeling/forskning/aktuelle-projekter/Sider/preside.aspx (accessed on 6 June 2021).
- Wiggins, M.; Sawtell, M.; Wiseman, O.; McCourt, C.; Eldridge, S.; Hunter, R.; Bordea, E.; Mustard, C.; Hanafiah, A.; Hatherall, B.; et al. Group antenatal care (Pregnancy Circles) for diverse and disadvantaged women: Study protocol for a randomised controlled trial with integral process and economic evaluations. BMC Health Serv. Res. 2020, 20, 919. [Google Scholar] [CrossRef]
- Byrskog, U.; Ahrne, M.; Small, R.; Andersson, E.; Essen, B.; Adan, A.; Ahmed, F.H.; Tesser, K.; Lidén, Y.; Israelsson, M.; et al. Rationale, development and feasibility of group antenatal care for immigrant women in Sweden: A study protocol for the Hooyo Project. BMJ Open 2019, 9, e030314. [Google Scholar] [CrossRef] [Green Version]
- Schytt, E.; Wahlberg, A.; Eltayb, A.; Small, R.; Tsekhmestruk, N.; Lindgren, H. Community-based doula support for migrant women during labour and birth: Study protocol for a randomised controlled trial in Stockholm, Sweden (NCT03461640). BMJ Open 2020, 10, e031290. [Google Scholar] [CrossRef]
- Fair, F.; Soltani, H.; Raben, L.; van Streun, Y.; Sioti, E.; Papadakaki, M.; Burke, C.; Watson, H.; Jokinen, M.; Shaw, E.; et al. Midwives’ experiences of cultural competency training and providing perinatal care for migrant women a mixed methods study: Operational Refugee and Migrant Maternal Approach (ORAMMA) project. BMC Pregnancy Childbirth 2021, 21, 340. [Google Scholar] [CrossRef]
- Jongen, C.; McCalman, J.; Bainbridge, R. Health workforce cultural competency interventions: A systematic scoping review. BMC Health Serv. Res. 2018, 18, 232. [Google Scholar] [CrossRef] [PubMed]
- Horvat, L.; Horey, D.; Romios, P.; Kis-Rigo, J.; Horvat, L. Cultural competence education for health professionals. Cochrane Database Syst Rev. 2014, 2014. [Google Scholar] [CrossRef] [PubMed]
- Seeleman, C.; Essink-Bot, M.L.; Stronks, K.; Ingleby, D. How should health service organizations respond to diversity? A content analysis of six approaches Health policy, reform, governance and law. BMC Health Serv. Res. 2015, 15, 510. [Google Scholar] [CrossRef] [Green Version]
- Handtke, O.; Schilgen, B.; Mösko, M. Culturally competent healthcare—A scoping review of strategies implemented in healthcare organizations and a model of culturally competent healthcare provision. PLoS ONE 2019, 14, e0219971. [Google Scholar] [CrossRef]
- Ogden, T.; Hagen, K.; Askeland, E.; Christensen, B. Implementing and Evaluating Evidence-Based Treatments of Conduct Problems in Children and Youth in Norway. Res. Soc. Work Pract. 2009, 19, 582–591. [Google Scholar] [CrossRef]
- Statistics Denmark Statistikbanken. Available online: https://www.statistikbanken.dk/statbank5a/default.asp?w=1920 (accessed on 6 June 2021).



{kind=link}
{kind=link}
| Women with Low-Level Education a N = 78 (100) | Non-Western Immigrant N = 217 (100) | Total N = 1304 (100) | |
|---|---|---|---|
| Did the midwife give you the leaflet “MAMAACT”? | |||
| Yes | 67 (85.9) | 174 (80.2) | 1051 (80.6) |
| No | 11 (14.1) | 38 (17.5) | 227 (17.4) |
| Unanswered | 0 (0.0) | 5 (2.3) | 26 (2.0) |
| Did the leaflet provide you with information about body signals that you have been able to use during your pregnancy? b | |||
| Yes | 35 (52.2) | 111 (62.0) | 522 (48.5) |
| No | 16 (23.9) | 31 (17.3) | 266 (24.7) |
| Have not read the leaflet | 14 (20.9) | 32 (17.9) | 264 (24.5) |
| Unanswered | 2 (3.0) | 5 (2.8) | 25 (2.3) |
| Did you download the app “MAMAACT”? b | |||
| Yes | 12 (17.9) | 40 (22.3) | 251 (23.3) |
| No | 55 (82.1) | 135 (75.4) | 811 (75.3) |
| Unanswered | 0 (0.0) | 4 (2.3) | 15 (1.4) |
| Why did you not download the app? You can choose between one of the following four options: c | |||
| TheMAMAACT leaflet was sufficient | 10 (18.2) | 34 (24.5) | 174 (21.1) |
| You did not have a smartphone to install it on | 1 (1.8) | 2 (1.4) | 12 (1.5) |
| It was difficult to find or install | 5 (9.1) | 12 (8.6) | 15 (1.8) |
| It was irrelevant; please elaborate | 35 (63.6) | 80 (57.6) | 595 (72.0) |
| Unanswered | 4 (7.3) | 11 (7.9) | 30 (3.6) |
| It was irrelevant; please elaborate d | |||
| Forgot to download the app | 8 (22.9) | 14 (17.5) | 102 (17.1) |
| Did not use the app due to technical problems | 0 (0.0) | 1 (1.3) | 10 (1.7) |
| Woman herself or partner works within healthcare | 0 (0.0) | 1 (1.2) | 12 (2.0) |
| Lost or did not read the leaflet | 5 (14.3) | 18 (22.5) | 145 (24.4) |
| Did not have time/surplus to get acquainted with the app | 0 (0.0) | 1 (1.2) | 12 (2.0) |
| Use other apps | 1 (2.8) | 6 (7.5) | 35 (5.9) |
| Felt no need for the app (partly due to knowledge from previous pregnancy) | 7 (20.0) | 14 (17.5) | 125 (21.0) |
| Did not know there was an app | 8 (22.9) | 19 (23.8) | 111 (18.7) |
| Other reasons | 6 (17.1) | 6 (7.5) | 43 (7.2) |
| Did the app provide you with information about body signals that you have been able to use during your pregnancy? e | |||
| Yes | 10 (83.3) | 32 (72.7) | 147 (55.3) |
| No | 1 (8.3) | 2 (4.6) | 56 (21.0) |
| Have not used the app | 1 (8.3) | 6 (13.6) | 47 (17.7) |
| Unanswered | 0 (0.0) | 4 (9.1) | 16 (6.0) |
| Number of Printed Leaflets | App Downloads (Woman) a | App Downloads (Partner) a | |
|---|---|---|---|
| Danish | 29,640 | 4184 (14.1) | 1145 (3.9) |
| English | 3350 | 527 (15.7) | 174 (5.2) |
| Arabic | 1570 | 130 (8.3) | 39 (2.5) |
| Turkish | 810 | 34 (4.2) | 9 (1.1) |
| Somali | 790 | 13 (1.6) | 3 (0.4) |
| Urdu | 790 | 26 (3.3) | 9 (1.1) |
| Total | 36,950 | 4914 (13.3) | 1379 (3.7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Damsted Rasmussen, T.; Johnsen, H.; Smith Jervelund, S.; Christensen, U.; Nybo Andersen, A.-M.; Villadsen, S.F. Implementation, Mechanisms and Context of the MAMAACT Intervention to Reduce Ethnic and Social Disparity in Stillbirth and Infant Health. Int. J. Environ. Res. Public Health 2021, 18, 8583. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168583
Damsted Rasmussen T, Johnsen H, Smith Jervelund S, Christensen U, Nybo Andersen A-M, Villadsen SF. Implementation, Mechanisms and Context of the MAMAACT Intervention to Reduce Ethnic and Social Disparity in Stillbirth and Infant Health. International Journal of Environmental Research and Public Health. 2021; 18(16):8583. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168583
Chicago/Turabian StyleDamsted Rasmussen, Trine, Helle Johnsen, Signe Smith Jervelund, Ulla Christensen, Anne-Marie Nybo Andersen, and Sarah Fredsted Villadsen. 2021. "Implementation, Mechanisms and Context of the MAMAACT Intervention to Reduce Ethnic and Social Disparity in Stillbirth and Infant Health" International Journal of Environmental Research and Public Health 18, no. 16: 8583. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168583