
A Longitudinal Assessment of Risk Factors and Chronic Diseases among Immigrant and Non-Immigrant Adults in Australia




Abstract
:1. Introduction
2. Methods
2.1. Setting and Recruitment
2.2. Measures
2.2.1. Sociodemographic Measures
2.2.2. Chronic Diseases
2.2.3. Risk Factors
2.2.4. Ethnicity
2.3. Data Analysis
3. Results
3.1. Participant Sociodemographic Characteristics
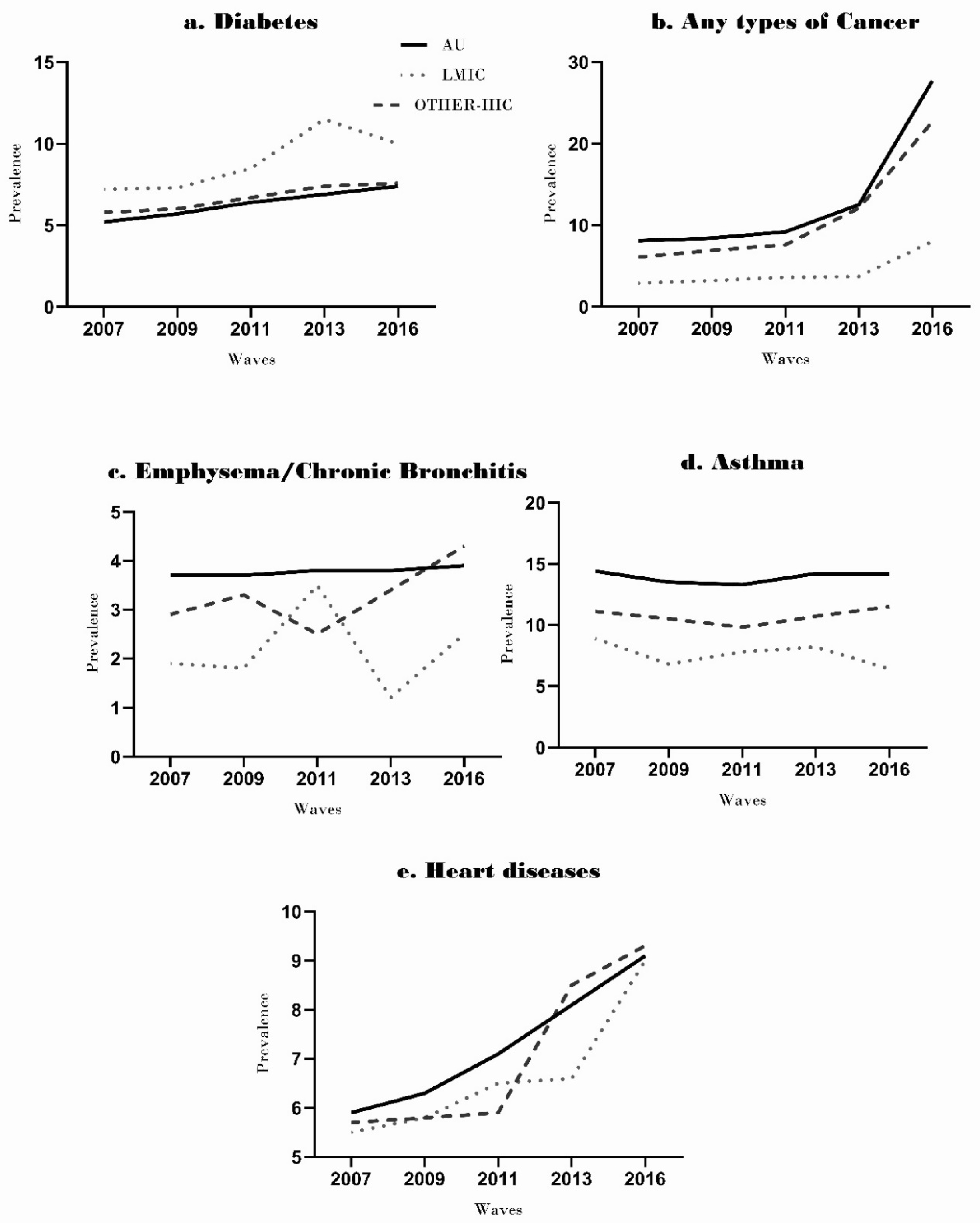
3.1.1. Chronic Diseases
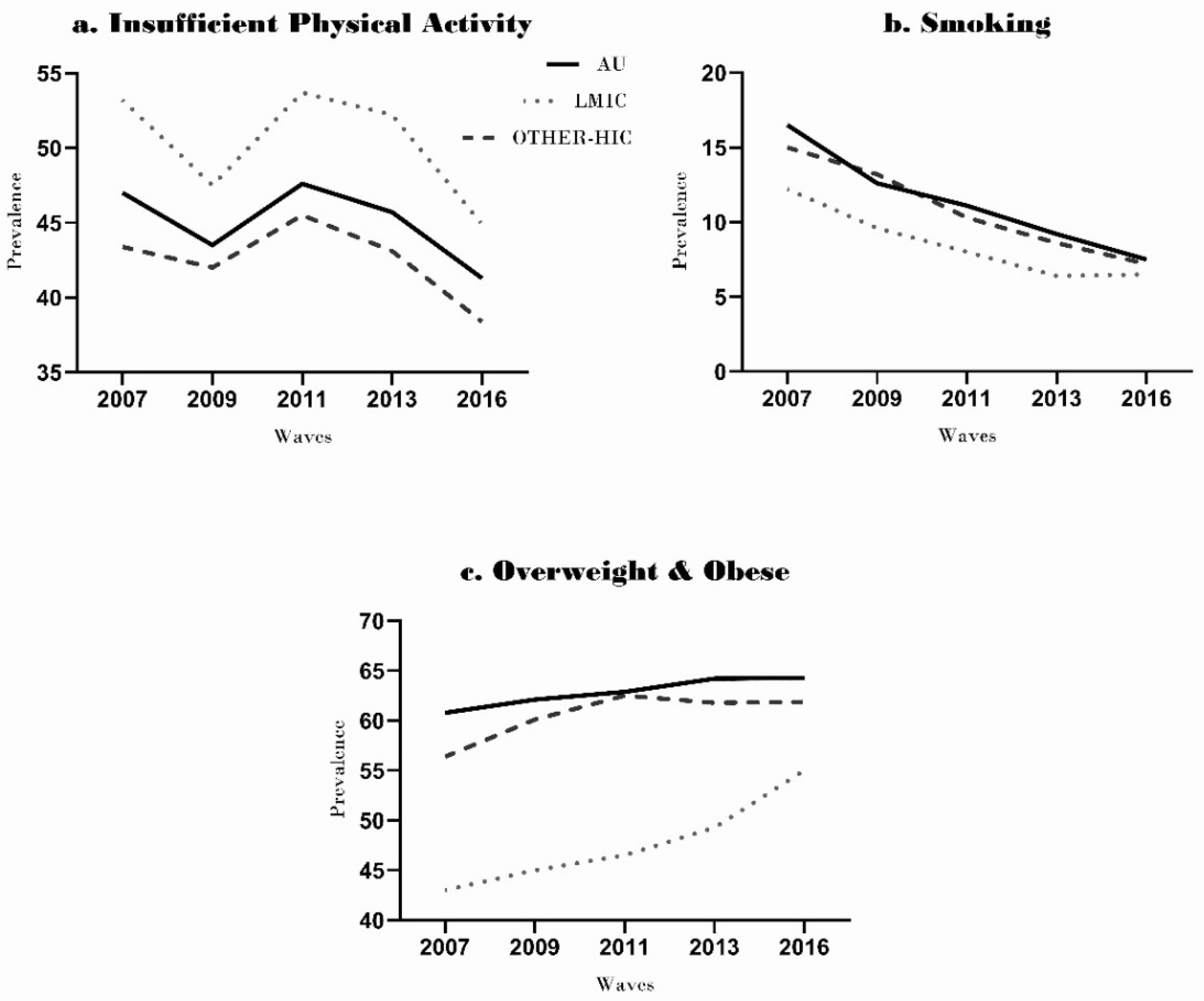
3.1.2. Risk Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Harris, R.E. Epidemiology of Chronic Disease: Global Perspectives; Jones & Bartlett Learning: Burlington, MA, USA, 2013. [Google Scholar]
- WHO. Preventing CHRONIC DISEASES A Vital Investment. 2019. Available online: https://www.who.int/chp/chronic_disease_report/contents/part2.pdf (accessed on 12 June 2021).
- Alwan, A. Global Status Report on Noncommunicable Diseases 2010; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Krueger, H.; Turner, D.; Krueger, J.; Ready, A.E. The economic benefits of risk factor reduction in Canada: Tobacco smoking, excess weight and physical inactivity. Can. J. Public Health 2014, 105, e69–e78. [Google Scholar] [CrossRef] [PubMed]
- WHO. Noncommunicable Diseases Country Profiles 2018; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- AIWH. Australia’s Health. 2018. Available online: https://www.aihw.gov.au/reports/australias-health/australias-health-2018/contents/table-of-contents (accessed on 12 June 2021).
- AIHW. Australia’s Health. 2020. Available online: https://www.aihw.gov.au/reports-data/australias-health (accessed on 12 June 2021).
- Crosland, P.; Ananthapavan, J.; Davison, J.; Lambert, M.; Carter, R. The health burden of preventable disease in Australia: A systematic review. Aust. N. Z. J. Public Health 2019, 43, 163–170. [Google Scholar] [CrossRef]
- ABS. Migration, Australia. 2017–2018. Statistics on Australia’s International Migration, Internal Migration (Interstate and Intrastate), and the Population by Country of Birth. Available online: http://www.abs.gov.au/ausstats/[email protected]/Latestproducts/3412.0Main%20Features22017-18?opendocument&tabname=Summary&prodno=3412.0&issue=2017-18&num=&view= (accessed on 12 June 2021).
- Jatrana, S.; Richardson, K.; Pasupuleti, S.S.R. Investigating the Dynamics of Migration and Health in Australia: A Longitudinal Study. Eur. J. Popul. 2018, 34, 519–565. [Google Scholar] [CrossRef] [PubMed]
- Sarich, P.E.A.; Ding, D.; Sitas, F.; Weber, M.F. Co-occurrence of chronic disease lifestyle risk factors in middle-aged and older immigrants: A cross-sectional analysis of 264,102 Australians. Prev. Med. 2015, 81, 209–215. [Google Scholar] [CrossRef]
- Gallegos, D.; Do, H.; To, Q.G.; Vo, B.; Goris, J.; Alraman, H. Differences in cardiometabolic risk markers among ethnic groups in Queensland, Australia. Health Soc. Care Community 2019, 27, e449–e458. [Google Scholar] [CrossRef]
- Bandyopadhyay, M.; Small, R.; Davey, M.A.; Oats, J.J.; Forster, D.A.; Aylward, A. Lived experience of gestational diabetes mellitus among immigrant South Asian women in Australia. Aust. N. Z. J. Obstet. Gynaecol. 2011, 51, 360–364. [Google Scholar] [CrossRef]
- Hodge, A.M.; English, D.R.; O’Dea, K.; Giles, G.G. Increased diabetes incidence in Greek and Italian migrants to Australia: How much can be explained by known risk factors? Diabetes Care 2004, 27, 2330–2334. [Google Scholar] [CrossRef] [Green Version]
- Burton, N.W.; Haynes, M.; Wilson, L.-A.M.; Giles-Corti, B.; Oldenburg, B.F.; Brown, W.J.; Giskes, K.M.; Turrell, G. HABITAT: A longitudinal multilevel study of physical activity change in mid-aged adults. BMC Public Health 2009, 9, 76. [Google Scholar] [CrossRef] [Green Version]
- ABS. Greater Brisbane. Available online: http://www.censusdata.abs.gov.au/census_services/getproduct/census/2016/quickstat/3GBRI?opendocument (accessed on 12 June 2021).
- Curtis, R.G.; Olds, T.; Plotnikoff, R.; Vandelanotte, C.; Edney, S.; Ryan, J.; Maher, C. Validity and bias on the online active Australia survey: Activity level and participant factors associated with self-report bias. BMC Med. Res. Methodol. 2020, 20, 6. [Google Scholar] [CrossRef]
- Nelson, E.M.; Rejeski, J.W.; Blair, N.S.; Duncan, W.P.; Judge, O.J.; King, C.A.; Macera, A.C.; Castaneda-Sceppa, A.C. Physical Activity and Public Health in Older Adults: Recommendation from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sports Exerc. 2007, 39, 1435–1445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WBG. Country Indebtendness Histroy. Available online: http://siteresources.worldbank.org/DATASTATISTICS/Resources/OGHIST.xls (accessed on 12 June 2021).
- Hirakata Vânia, N.B.A. Alternatives for logistic regression in cross-sectional studies: An empirical comparison of models that directly estimate the prevalence ratio. BMC Med. Res. Methodol. 2003, 3, 21. [Google Scholar]
- Pasupuleti, S.S.R.; Jatrana, S.; Richardson, K. Effect of nativity and duration of residence on chronic health conditions among Asian immigrants in Australia: A longitudinal investigation. J. Biosoc. Sci. 2016, 48, 322–341. [Google Scholar] [CrossRef]
- Anikeeva, O.; Bi, P.; Hiller, J.E.; Ryan, P.; Roder, D.; Han, G.S. The health status of migrants in Australia: A review. Asia Pac. J. Public Health 2010, 22, 159–193. [Google Scholar] [CrossRef]
- Magliano, D.J.; Barr, E.L.; Zimmet, P.Z.; Cameron, A.; Dunstan, D.; Colagiuri, S.; Jolley, D.; Owen, N.; Phillips, P.; Tapp, R.; et al. Glucose Indices, Health Behaviors, and Incidence of Diabetes in Australia: The Australian Diabetes, Obesity and Lifestyle Study. Diabetes Care 2008, 31, 267–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anikeeva, O.; Bi, P.; Hiller, J.E.; Ryan, P.; Roder, D.; Han, G.S. Trends in cancermortality rates among migrants in Australia: 1981–2007. Cancer Epidemiol. 2011, 36, e74–e82. [Google Scholar] [CrossRef]
- Kennedy, S.; McDonald, J.; Biddle, N. The Healthy Immigrant Effect and Immigrant Selection: Evidence from Four Countries; IDEAS Working Paper Series from RePEc 2006; SEDAP: Hamilton, ON, Canada, 2006. [Google Scholar]
- Renzaho, A.M.N. Globalisation, Migration and Health; Imperial College Press: London, UK, 2016; pp. 363–389. [Google Scholar]
- Singh Australian Health Inequalities: Birthplace. Available online: https://www.aihw.gov.au/reports/social-determinants/australian-health-inequalities-birthplace/contents/table-of-contents (accessed on 12 June 2021).
- Taylor, R.; Chey, T.; Bauman, A.; Webster, I. Socio-economic, migrant and geographic differentials in coronary heart disease occurrence in New South Wales. Aust. N. Z. J. Public Health 1999, 23, 20–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, A.W.; Grande, E.D.; Fateh-Moghadam, P.; Montgomerie, A.; Battisti, L.; Barrie, H.; Kourbelis, C.; Campostrini, S. Comparison of Health and Risk Factors of Older, Working-age Australians, Italians and Italian-born Migrants to Australia, with Data from an Italian (PASSI), and an Australian (SAMSS) Risk Factor Surveillance System. J. Immigr. Minor. Health 2018, 20, 1190–1196. [Google Scholar] [CrossRef] [Green Version]
- Sanou, D.; O’Reilly, E.; Ngnie-Teta, I.; Batal, M.; Mondain, N.; Andrew, C.; Newbold, B.K.; Bourgeault, I. Acculturation and Nutritional Health of Immigrants in Canada: A Scoping Review. J. Immigr. Minor. Health 2014, 16, 24–34. [Google Scholar] [CrossRef] [Green Version]
- Patel, M.; Boutin-Foster, C.; Phillips, E. Understanding of cardiovascular disease risk factors among Bangladeshi immigrants in New York City. Ethn. Health 2019, 24, 432–442. [Google Scholar] [CrossRef]
- Lassetter, J.H.; Callister, L.C. The Impact of Migration on the Health of Voluntary Migrants in Western Societies: A Review of the Literature. J. Transcult. Nurs. 2009, 20, 93–104. [Google Scholar] [CrossRef] [PubMed]
- Evenson, K.R.; Sarmiento, O.L.; Ayala, G.X. Acculturation and physical activity among North Carolina Latina immigrants. Soc. Sci. Med. 2004, 59, 2509–2522. [Google Scholar] [CrossRef]
- Mahmood, B.; Bhatti, J.A.; Leon, A.; Gotay, C. Leisure Time Physical Activity Levels in Immigrants by Ethnicity and Time Since Immigration to Canada: Findings from the 2011–2012 Canadian Community Health Survey. J. Immigr. Minor. Health 2019, 21, 801–810. [Google Scholar] [CrossRef]
- Gartner, C.E.; Barendregt, J.J.; Hall, W.D. Predicting the future prevalence of cigarette smoking in Australia: How low can we go and by when? Tob. Control 2009, 18, 183–189. [Google Scholar] [CrossRef]
- Owen, A.J.; Maulida, S.B.; Zomer, E.; Liew, D. Productivity burden of smoking in Australia: A life table modelling study. Tob. Control 2019, 28, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Joshi, S.; Jatrana, S.; Paradies, Y. Tobacco smoking between immigrants and non-immigrants in Australia: A longitudinal investigation of the effect of nativity, duration of residence and age at arrival. Health Promot. J. Aust. 2018, 29, 282–292. [Google Scholar] [CrossRef]
- Alidu, L.; Grunfeld, E. A systematic review of acculturation, obesity and health behaviours among migrants to high-income countries. Psychol. Health 2018, 33, 724–745. [Google Scholar] [CrossRef] [PubMed]
- Hauck, K.; Hollingsworth, B.; Morgan, L. BMI differences in 1st and 2nd generation immigrants of Asian and European origin to Australia. Health Place 2011, 17, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Burgard, S.A.; Chen, P.V. Challenges of health measurement in studies of health disparities. Soc. Sci. Med. 2014, 106, 143–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Characteristics | n | % |
|---|---|---|
| Sex | ||
| Male | 4942 | 45.0 |
| Female | 6093 | 55.0 |
| Age (years) | ||
| 42–44 | 2530 | 23.0 |
| 45–49 | 2382 | 21.0 |
| 50–54 | 2312 | 21.0 |
| 55–59 | 2080 | 19.0 |
| 60–65 | 1731 | 16.0 |
| Country of birth * | ||
| Australia | 8245 | 75.0 |
| High-income countries (HIC) | 1704 | 16.0 |
| Low–middle-income countries (LMIC) | 1011 | 9.0 |
| Employment status | ||
| Full-time work | 5846 | 53.0 |
| Part-time work | 1771 | 16.0 |
| Home duties | 683 | 6.0 |
| Unemployed | 160 | 1.0 |
| Other | 51 | 0.4 |
| Highest educational qualification | ||
| School only (up to 12 years) | 4311 | 39.0 |
| Certificate/diploma | 3220 | 29.0 |
| University degree | 3457 | 32.0 |
| Gross annual household income (AUD) | ||
| $0–41599 | 2232 | 24.0 |
| $41,600–72,799 | 2438 | 26.0 |
| $72,800–129,000 | 2845 | 30.0 |
| $130,000+ | 1889 | 20.0 |
| General health status | ||
| Excellent | 1117 | 10.0 |
| Very good | 3670 | 34.0 |
| Good | 4194 | 38.0 |
| Fair | 1575 | 15.0 |
| Poor | 375 | 3.0 |
| Body mass index (BMI) | ||
| Healthy weight (<25) | 4369 | 41.5 |
| Overweight (25–<30) | 3900 | 37.1 |
| Obese (≥30) | 2248 | 21.4 |
| Country of Birth | Prevalence Ratio (PRs) | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Chronic Diseases | |||
| Diabetes | |||
| Australian-born participants | 1.00 # | ||
| High-income countries | 1.00 | 0.99–1.01 | 0.59 |
| Low–middle-income countries | 1.02 | 1.01–1.03 | <0.00 |
| COPD: Emphysema/chronic bronchitis | |||
| Australian-born | 1.00 # | ||
| High-income countries | 0.99 | 0.98–1.00 | 0.07 |
| Low–middle-income countries | 0.98 | 0.97–0.99 | <0.00 |
| COPD: Asthma | |||
| Australian-born participants | 1.00 # | ||
| High-income countries | 0.98 | 0.96–0.99 | <0.00 |
| Low–middle-income countries | 0.95 | 0.94–0.95 | <0.00 |
| Heart diseases | |||
| Australian-born participants | 1.00 # | ||
| High-income countries | 0.99 | 0.98–1.01 | 0.22 |
| Low–middle-income countries | 0.99 | 0.98–1.01 | 0.28 |
| Cancer | |||
| Australian-born participants | 1.00 # | ||
| High-income countries | 0.98 | 0.96–0.99 | <0.00 |
| Low–middle-income countries | 0.93 | 0.92–0.95 | <0.00 |
| Risk Behaviors | |||
| Cigarette Smoking | |||
| Australian-born participants | 1.00 # | ||
| High-income countries | 0.99 | 0.87–1.12 | 0.86 |
| Low–middle-income countries | 0.75 | 0.63–0.91 | <0.00 |
| Insufficient Physical Activity | |||
| Australian-born participants | 1.00 # | ||
| High-income countries | 0.96 | 0.91–0.99 | 0.04 |
| Low–middle-income countries | 1.12 | 1.06–1.18 | <0.00 |
| Overweight and Obese | |||
| Australian-born participants | 1.00 # | ||
| High-income countries | 0.93 | 0.90–0.97 | <0.00 |
| Low–middle-income countries | 0.77 | 0.72–0.82 | <0.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nisar, M.; Kolbe-Alexander, T.L.; Burton, N.W.; Khan, A. A Longitudinal Assessment of Risk Factors and Chronic Diseases among Immigrant and Non-Immigrant Adults in Australia. Int. J. Environ. Res. Public Health 2021, 18, 8621. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168621
Nisar M, Kolbe-Alexander TL, Burton NW, Khan A. A Longitudinal Assessment of Risk Factors and Chronic Diseases among Immigrant and Non-Immigrant Adults in Australia. International Journal of Environmental Research and Public Health. 2021; 18(16):8621. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168621
Chicago/Turabian StyleNisar, Mehwish, Tracy L. Kolbe-Alexander, Nicola W. Burton, and Asaduzzaman Khan. 2021. "A Longitudinal Assessment of Risk Factors and Chronic Diseases among Immigrant and Non-Immigrant Adults in Australia" International Journal of Environmental Research and Public Health 18, no. 16: 8621. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168621