
The Mediated Role of Credibility on Information Sources and Patient Awareness toward Patient Rights



Abstract
:1. Introduction
2. Patient Rights
3. Channel Complementarity Theory and Health Information Seeking
4. Credibility of Health Information Sources
5. Age and Health Information Seeking
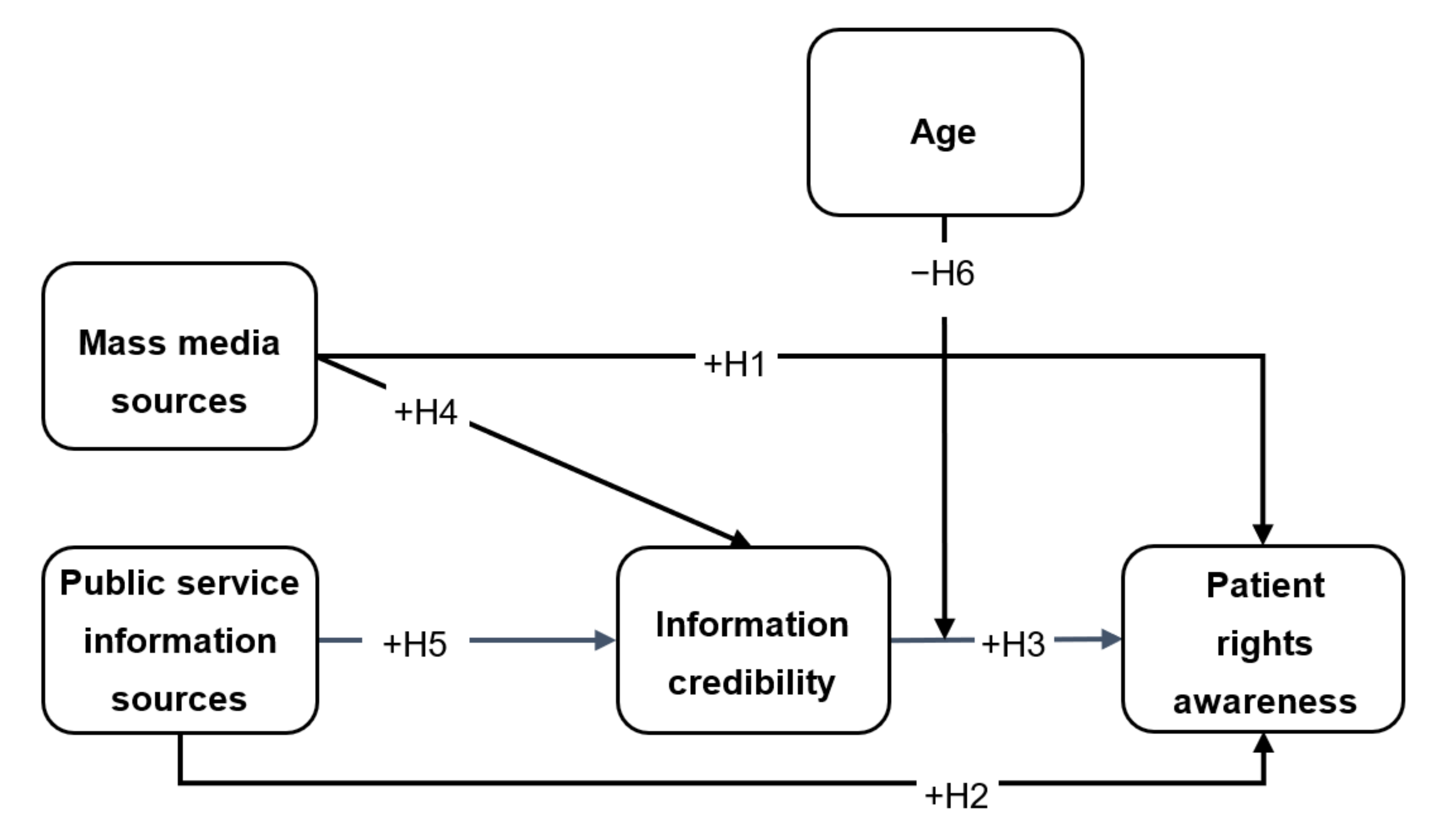
6. Study Framework and Hypotheses
7. Method
7.1. Study Design and Data Collection
7.2. Measures
8. Results
8.1. Validity and Reliability
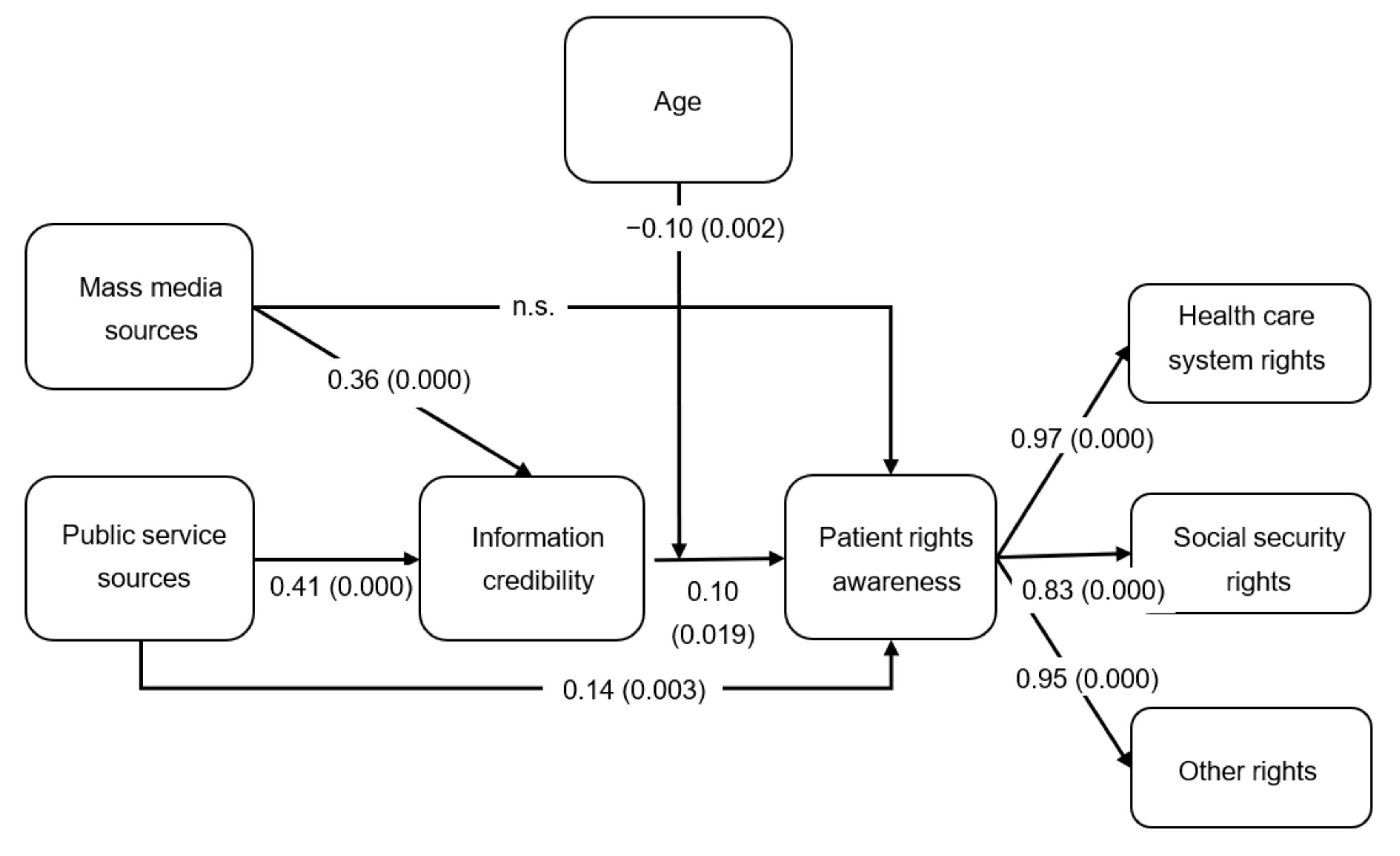
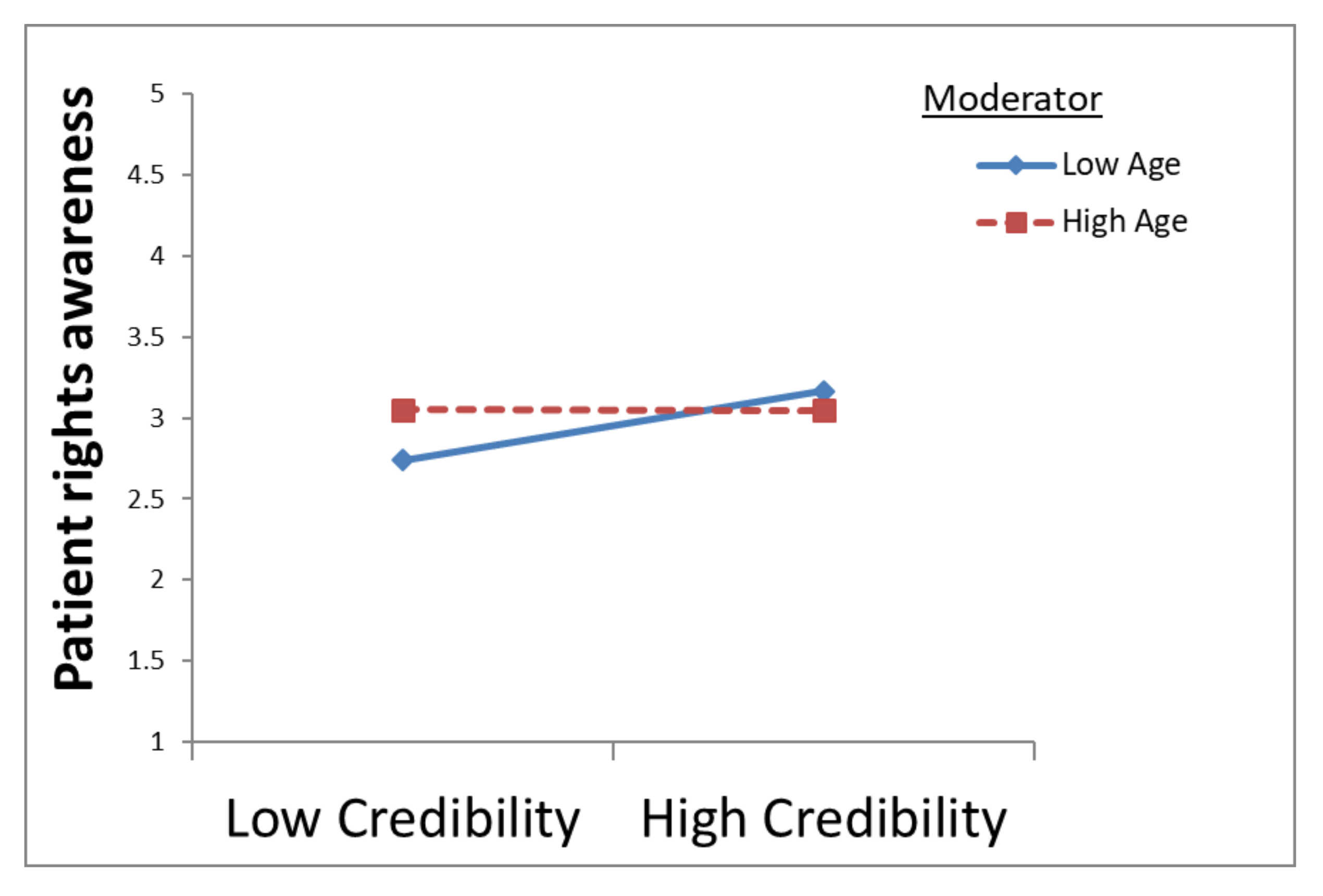
8.2. Model Testing
9. Discussion
10. Conclusions
Practice Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Eurofound. Access to Social Benefits: Reducing Non-Take-Up; Publications Office of the European Union: Luxembourg, 2015; Available online: www.eurofound.europa.eu/sites/default/files/ef_publication/field_ef_document/ef1536en.pdf (accessed on 3 June 2021).
- World Health Organization. Patient Safety and Rights. Developing Tools to Support Consumer Health Literacy. 2010. Available online: www.euro.who.int/__data/assets/pdf_file/0018/133128/e94739.pdf (accessed on 5 May 2021).
- Palm, W.; Townend, D.; Nys, H. Patients’ Rights in the European Union: From Recognition to Implementation. Eur. J. Public Health 2016, 26, ckw170-010. [Google Scholar] [CrossRef] [Green Version]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.T.; Lin, J. The Influence of Offline and Online Intrinsic Motivations on Online Health Information Seeking. Health Commun. 2020, 35, 1129–1136. [Google Scholar] [CrossRef]
- Zigdon, A.; Eckhaus, E.; Lerer, R.; Rosenfeld, M. Patients’ Perspectives on Services and Activities of Patient Organizations–Development of a Patient-Oriented Questionnaire. Chronic Illn. under review.
- Unnikrishnan, B.; Trivedi, D.; Kanchan, T.; Rekha, T.; Mithra, P.; Kumar, N.; Kulkarni, V.; Holla, R.; Talish, M. Patients’ Awareness about Their Rights: A Study from Coastal South India. Sci. Eng. Ethics 2017, 23, 203–214. [Google Scholar] [CrossRef] [PubMed]
- Getz, I.; Weissman, G. An Information Needs Profile of Israeli Older Adults, Regarding the Law and Services. J. Libr. Inf. Sci. 2010, 42, 136–146. [Google Scholar] [CrossRef]
- Zhang, Y. Beyond Quality and Accessibility: Source Selection in Consumer Health Information Searching: Beyond Quality and Accessibility: Source Selections in Consumer Health Information Searching. J. Assoc. Inf. Sci. Technol. 2014, 65, 911–927. [Google Scholar] [CrossRef] [Green Version]
- Eurobarometer. Special Eurobarometer 425: Patients’ Rights in Cross-Border Healthcare in the European Union 2015. 2015. Available online: https://data.europa.eu/data/datasets/s2034_82_2_425_eng?locale=en (accessed on 3 June 2021).
- Mishra, A.S.; Roy, S.; Bailey, A.A. Exploring Brand Personality-Celebrity Endorser Personality Congruence in Celebrity Endorsements in the Indian Context: Brand-Celebrity Personality. Psychol. Mark. 2015, 32, 1158–1174. [Google Scholar] [CrossRef]
- Biswas, D.; Biswas, A.; Das, N. The Differential Effects of Celebrity and Expert Endorsements on Consumer Risk Perceptions. The Role of Consumer Knowledge, Perceived Congruency, and Product Technology Orientation. J. Advert. 2006, 35, 17–31. [Google Scholar] [CrossRef]
- Choi, W. Older Adults’ Credibility Assessment of Online Health Information: An Exploratory Study Using an Extended Typology of Web Credibility. J. Assoc. Inf. Sci. Technol. 2020, 71, 1295–1307. [Google Scholar] [CrossRef]
- Sun, Y.; Zhang, Y.; Gwizdka, J.; Trace, C.B. Consumer Evaluation of the Quality of Online Health Information: Systematic Literature Review of Relevant Criteria and Indicators. J. Med. Internet Res. 2019, 21, e12522. [Google Scholar] [CrossRef]
- Putturaj, M.; Van Belle, S.; Criel, B.; Engel, N.; Krumeich, A.; Nagendrappa, B.P.; Prashanth, N.S. Towards a Multilevel Governance Framework on the Implementation of Patient Rights in Health Facilities: A Protocol for a Systematic Scoping Review. BMJ Open 2020, 10, e038927. [Google Scholar] [CrossRef] [PubMed]
- Abedi, G.; Shojaee, J.; Moosazadeh, M.; Rostami, F.; Nadi, A.; Abedini, E.; Palenik, C.J.; Askarian, M. Awareness and Observance of Patient Rights from the Perspective of Iranian Patients: A Systematic Review and Meta-Analysis. Iran. J. Med. Sci. 2017, 42, 227–234. [Google Scholar]
- Hobdell, M.H. Health as a Fundamental Human Right. Br. Dent. J. 1996, 180, 267–270. [Google Scholar] [CrossRef]
- Epstein-Lubow, G. Care Is A Basic Human Right: A Review of Arthur Kleinman’s ‘The Soul of Care’, a Compelling Depiction of Family Caregiving with Important Implications for People Living with Dementia and Everyone Who Supports Them. Health Aff. 2020, 39, 1094–1095. [Google Scholar] [CrossRef]
- State Comptroller. Annual Report (65C) and Accounts for the Fiscal Year 2013, Non-Take-up of Social Rights. 65C. 2015. Available online: www.mevaker.gov.il/he/Reports/Report_290/ReportFiles/fullreport_2.pdf (accessed on 11 November 2020).
- Janssens, J.; Van Mechelen, N. Who Is to Blame? An Overview of the Factors Contributing to the Non-Take-up of Social Rights; Herman Deleeck Centre for Social Policy, University of Antwerp: Antwerp, Belgium, 2017. [Google Scholar]
- Dutta-Bergman, M.J. Complementarity in Consumption of News Types across Traditional and New Media. J. Broadcast. Electron. Media 2004, 48, 41–60. [Google Scholar] [CrossRef]
- Dutta-Bergman, M.J. Interpersonal Communication after 9/11 via Telephone and Internet: A Theory of Channel Complementarity. New Media Soc. 2004, 6, 659–673. [Google Scholar] [CrossRef]
- Ruppel, E.K.; Rains, S.A. Information Sources and the Health Information-Seeking Process: An Application and Extension of Channel Complementarity Theory. Commun. Monogr. 2012, 79, 385–405. [Google Scholar] [CrossRef]
- Lai, C.-H. An Integrated Approach to Untangling Mediated Connectedness with Online and Mobile Media. Comput. Human Behav. 2014, 31, 20–26. [Google Scholar] [CrossRef]
- Ruppel, E.K.; Burke, T.J. Complementary Channel Use and the Role of Social Competence. J. Comput. Mediat. Commun. 2015, 20, 37–51. [Google Scholar] [CrossRef] [Green Version]
- Dimmick, J.; Chen, Y.; Li, Z. Competition between the Internet and Traditional News Media: The Gratification-Opportunities Niche Dimension. J. Media Econ. 2004, 17, 19–33. [Google Scholar] [CrossRef]
- Rains, S.A.; Ruppel, E.K. Channel Complementarity Theory and the Health Information-Seeking Process: Further Investigating the Implications of Source Characteristic Complementarity. Communic. Res. 2016, 43, 232–252. [Google Scholar] [CrossRef]
- Tian, Y.; Robinson, J.D. Media Complementarity and Health Information Seeking in Puerto Rico. J. Health Commun. 2014, 19, 710–720. [Google Scholar] [CrossRef]
- Lin, J.; Dutta, M.J. A Replication of Channel Complementarity Theory among Internet Users in India. Health Commun. 2017, 32, 483–492. [Google Scholar] [CrossRef] [PubMed]
- Neyazi, T.A.; Kumar, A.; Dutta, M.J. Channel Complementarity or Displacement? Theory and Evidence from a Non-Western Election Context. J. Broadcast. Electron. Media 2019, 63, 656–676. [Google Scholar] [CrossRef]
- Roth-Cohen, O.; Tamir, I. ‘The Winner Takes It All’: Values and Benefits of Israeli Sports Gambling Advertisements. Int. J. Hist. Sport 2017, 34, 639–655. [Google Scholar] [CrossRef]
- Gal, J.; Madhala, S. The Social Welfare System and the Coronavirus Crisis: An Overview. Available online: www.taubcenter.org.il/wp-content/uploads/2021/01/socialwelfareandthecoronaviruscrisisoverviewheb.pdf (accessed on 2 August 2021).
- Chang, Y.-S.; Zhang, Y.; Gwizdka, J. The Effects of Information Source and EHealth Literacy on Consumer Health Information Credibility Evaluation Behavior. Comput. Human. Behav. 2021, 115, 106629. [Google Scholar] [CrossRef]
- Mertens, F.; Távora, R.; Nakano, E.Y.; Castilhos, Z.C. Information Sources, Awareness and Preventive Health Behaviors in a Population at Risk of Arsenic Exposure: The Role of Gender and Social Networks. PLoS ONE 2017, 12, e0186130. [Google Scholar] [CrossRef] [Green Version]
- Fornell, C.; Larcker, D.F. Evaluating Structural Equation Models with Unobservable Variables and Measurement Error. J. Mark. Res. 1981, 18, 39. [Google Scholar] [CrossRef]
- MacLeod, S.; Musich, S.; Gulyas, S.; Cheng, Y.; Tkatch, R.; Cempellin, D.; Bhattarai, G.R.; Hawkins, K.; Yeh, C.S. The Impact of Inadequate Health Literacy on Patient Satisfaction, Healthcare Utilization, and Expenditures among Older Adults. Geriatr. Nurs. 2017, 38, 334–341. [Google Scholar] [CrossRef]
- Van Hoa, H.; Giang, H.T.; Vu, P.T.; Van Tuyen, D.; Khue, P.M. Factors Associated with Health Literacy among the Elderly People in Vietnam. Biomed Res. Int. 2020, 2020, 3490635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zigdon, A.; Zigdon, T.; Moran, D.S. Attitudes of Nurses towards Searching Online for Medical Information for Personal Health Needs: Cross-Sectional Questionnaire Study. J. Med. Internet Res. 2020, 22, e16133. [Google Scholar] [CrossRef]
- Kovner, C.T.; Mezey, M.; Harrington, C. Who Cares for Older Adults? Workforce Implications of an Aging Society. Health Aff. 2002, 21, 78–89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, X.; Hay, J.L.; Waters, E.A.; Kiviniemi, M.T.; Biddle, C.; Schofield, E.; Li, Y.; Kaphingst, K.; Orom, H. Health Literacy and Use and Trust in Health Information. J. Health Commun. 2018, 23, 724–734. [Google Scholar] [CrossRef] [PubMed]
- Song, X.; Song, S.; Chen, S.; Zhao, Y.; Zhu, Q. Factors Influencing Proxy Internet Health Information Seeking among the Elderly in Rural China: A Grounded Theory Study. In Human Aspects of IT for the Aged Population. Design for the Elderly and Technology Acceptance; Springer International Publishing: Cham, Switzerland, 2019; pp. 332–343. [Google Scholar]
- Atkinson, N.L.; Saperstein, S.L.; Pleis, J. Using the Internet for Health-Related Activities: Findings from a National Probability Sample. J. Med. Internet Res. 2009, 11, e4. [Google Scholar] [CrossRef]
- Gehrau, V.; Fujarski, S.; Lorenz, H.; Schieb, C.; Blöbaum, B. The Impact of Health Information Exposure and Source Credibility on COVID-19 Vaccination Intention in Germany. Int. J. Environ. Res. Public Health 2021, 18, 4678. [Google Scholar] [CrossRef]
- Robertson-Lang, L.; Major, S.; Hemming, H. An Exploration of Search Patterns and Credibility Issues among Older Adults Seeking Online Health Information. Can. J. Aging 2011, 30, 631–645. [Google Scholar] [CrossRef]
- Seo, H.; Blomberg, M.; Altschwager, D.; Vu, H.T. Vulnerable Populations and Misinformation: A Mixed-Methods Approach to Underserved Older Adults’ Online Information Assessment. New Media Soc. 2021, 23, 2012–2033. [Google Scholar] [CrossRef]
- Tentori, K.; Osherson, D.; Hasher, L.; May, C. Wisdom and Aging: Irrational Preferences in College Students but Not Older Adults. Cognition 2001, 81, B87–B96. [Google Scholar] [CrossRef]
- Kim, S.; Hasher, L. The Attraction Effect in Decision Making: Superior Performance by Older Adults. Q. J. Exp. Psychol. A 2005, 58, 120–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Central Bureau of Statistics (CBS). Population of Israel on the Eve of 2021. Available online: www.cbs.gov.il/en/mediarelease/Pages/2020/Population-of-Israel-on-the-Eve-of-2021.aspx (accessed on 2 August 2021).
- Slaughter, J.E.; Cable, D.M.; Turban, D.B. Changing Job Seekers’ Image Perceptions during Recruitment Visits: The Moderating Role of Belief Confidence. J. Appl. Psychol. 2014, 99, 1146–1158. [Google Scholar] [CrossRef] [Green Version]
- Remmerswaal, D.; Muris, P. Children’s Fear Reactions to the 2009 Swine Flu Pandemic: The Role of Threat Information as Provided by Parents. J. Anxiety Disord. 2011, 25, 444–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hair, J.F.; Anderson, R.E.; Babin, B.J.; Black, W.C. Multivariate Data Analysis: A Global Perspective, 7th ed.; Prentice Hall: Upper Saddle River, NJ, USA, 2009. [Google Scholar]
- Lam, L.W. Impact of Competitiveness on Salespeople’s Commitment and Performance. J. Bus. Res. 2012, 65, 1328–1334. [Google Scholar] [CrossRef]
- Cortina, J.M.; Chen, G.; Dunlap, W.P. Testing Interaction Effects in LISREL: Examination and Illustration of Available Procedures. Organ. Res. Methods 2001, 4, 324–360. [Google Scholar] [CrossRef] [Green Version]
- Bagozzi, R.P.; Edwards, J.R. A General Approach for Representing Constructs in Organizational Research. Organ. Res. Methods 1998, 1, 45–87. [Google Scholar] [CrossRef] [Green Version]
- Duff, B.R.-L.; Sar, S. Seeing the Big Picture: Multitasking and Perceptual Processing Influences on Ad Recognition. J. Advert. 2015, 44, 173–184. [Google Scholar] [CrossRef]
- Metzger, M.J.; Flanagin, A.J.; Medders, R.B. Social and Heuristic Approaches to Credibility Evaluation Online. J. Commun. 2010, 60, 413–439. [Google Scholar] [CrossRef] [Green Version]
- Wu, M.; Huang, Y.; Li, R.; Bortree, D.S.; Yang, F.; Xiao, A.; Wang, R. A Tale of Two Sources in Native Advertising: Examining the Effects of Source Credibility and Priming on Content, Organizations, and Media Evaluations. Am. Behav. Sci. 2016, 60, 1492–1509. [Google Scholar] [CrossRef]
- Choi, W.; Stvilia, B. Web Credibility Assessment: Conceptualization, Operationalization, Variability, and Models. J. Assoc. Inf. Sci. Technol. 2015, 66, 2399–2414. [Google Scholar] [CrossRef]
- Tseng, S.; Fogg, B.J. Credibility and Computing Technology. Commun. ACM 1999, 42, 39–44. [Google Scholar] [CrossRef]
- Shen, C.; Kasra, M.; Pan, W.; Bassett, G.A.; Malloch, Y.; O’Brien, J.F. Fake Images: The Effects of Source, Intermediary, and Digital Media Literacy on Contextual Assessment of Image Credibility Online. New Media Soc. 2019, 21, 438–463. [Google Scholar] [CrossRef]
- Toncar, M.; Reid, J.S.; Anderson, C.E. Effective Spokespersons in a Public Service Announcement: National Celebrities, Local Celebrities and Victims. J. Commun. Manag. 2007, 11, 258–275. [Google Scholar] [CrossRef]
- Peters, E.; Diefenbach, M.A.; Hess, T.M.; Västfjäll, D. Age Differences in Dual Information-Processing Modes: Implications for Cancer Decision Making: Implications for Cancer Decision Making. Cancer 2008, 113, 3556–3567. [Google Scholar] [CrossRef]
- Brasel, S.A.; Gips, J. Media Multitasking Behavior: Concurrent Television and Computer Usage. Cyberpsychol. Behav. Soc. Netw. 2011, 14, 527–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Respondent Characteristics | n (%) |
|---|---|
| Gender | |
| Female | 711 (71.5) |
| Male | 283 (28.5) |
| Age (years) | |
| 18–24 | 211 (21.2) |
| 25–34 | 190 (19.1) |
| 35–44 | 166 (16.7) |
| 45–54 | 210 (21.1) |
| 55–64 | 143 (14.4) |
| 65+ | 74 (7.5) |
| Marital Status | |
| Married/Partner | 596 (60.0) |
| Bachelor/Never Married | 275 (27.7) |
| Divorced | 89 (9.0) |
| Widowed | 28 (2.8) |
| Others | 6 (0.6) |
| Country of Birth | |
| Israel | 657 (66.1) |
| Other | 337 (33.9) |
| Education Background | |
| Primary education | 51 (5.1) |
| Secondary education | 292 (29.3) |
| Further education | 131 (13.2) |
| University degree and higher | 499 (50.2) |
| Other | 22 (2.2) |
| Income | |
| Considerably below average | 298 (30.0) |
| Slightly below average | 230 (23.1) |
| Average (10,000 Shekels) | 184 (18.5) |
| Slightly above average | 202 (20.3) |
| Considerably above average | 61 (6.2) |
| Would rather not say | 19 (1.9) |
| Reported Health Status | |
| Very good | 183 (18.4) |
| Good | 519 (52.2) |
| Not so good | 229 (23.0) |
| Not good | 48 (4.9) |
| Bad | 15 (1.5) |
| Std. Coef. | AVE | CR | |
|---|---|---|---|
| Patient rights awareness—general | 0.82 *–0.99 * | 0.86 | 0.95 |
| Social security rights | 0.72 *–0.82 * | 0.58 | 0.91 |
| Health care system rights | 0.60 *–0.75 * | 0.46 | 0.88 |
| Other rights | 0.67 *–0.75 * | 0.50 | 0.89 |
| Information credibility | 0.54 *–0.80 * | 0.50 | 0.74 |
| Mass media information sources | 0.56 *–0.84 * | 0.57 | 0.79 |
| Public service information sources | 0.60 *–0.73 * | 0.42 | 0.68 |
| 1 | 2 | 3 | 4 | ||
|---|---|---|---|---|---|
| 1 | Patient rights awareness | 0.86 | 0.126 ** | 0.084 ** | 0.129 ** |
| 2 | Information credibility | 0.016 | 0.50 | 0.357 ** | 0.276 ** |
| 3 | Mass media information sources | 0.001 | 0.127 | 0.57 | 0.181 ** |
| 4 | Public service information sources | 0.017 | 0.076 | 0.033 | 0.42 |
| Relationships | Standardized Effect (β) | Regression Weights (Direct) | ||||
|---|---|---|---|---|---|---|
| Total | Direct | Indirect | Estimate (B) | C.R. (t) | p | |
| Public service sources → Patient rights awareness | 0.183 | 0.142 | 0.041 * | 0.258 | 2.977 | 0.003 |
| Mass media sources → Patient rights awareness | 0.036 | 0.000 | 0.036 ** | |||
| Information credibility → Patient rights awareness | 0.100 | 0.100 | 0.000 | 0.105 | 2.336 | 0.019 |
| Mass media sources → Information credibility | 0.359 | 0.359 | 0.000 | 0.313 | 9.035 | 0.000 |
| Public service sources → Information credibility | 0.405 | 0.405 | 0.000 | 0.699 | 7.890 | 0.000 |
| Age × Information credibility → Patient rights awareness | −0.101 | −0.101 | 0.000 | −0.109 | −3.059 | 0.002 |
| Path | Std. Coef. (β) | S.E. | Bootstrap with 95% CI |
|---|---|---|---|
| A | |||
| Mass media information sources → Information credibility (a) | 0.359 | 0.043 | 0.292–0.428 ** |
| Information credibility → Patient rights awareness (b) | 0.100 | 0.044 | 0.034–0172 * |
| Total effect: Mass media information sources → Patient rights awareness (c) | 0.036 | 0.017 | 0.012–0.070 * |
| Direct effect: Mass media information sources → Patient rights awareness (c′) | 0.000 | 0.000 | -- |
| B | |||
| Public service information sources → Information credibility (a) | 0.405 | 0.037 | 0.348–0.474 ** |
| Information credibility → Patient rights awareness (b) | 0.100 | 0.044 | 0.034–0.172 * |
| Total effect: Public service information sources → Patient rights awareness (c) | 0.183 | 0.043 | 0.104–0.252 * |
| Direct effect: Public service information sources → Patient rights awareness (c′) | 0.142 | 0.050 | 0.061–0.227 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roth-Cohen, O.; Levy, S.; Zigdon, A. The Mediated Role of Credibility on Information Sources and Patient Awareness toward Patient Rights. Int. J. Environ. Res. Public Health 2021, 18, 8628. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168628
Roth-Cohen O, Levy S, Zigdon A. The Mediated Role of Credibility on Information Sources and Patient Awareness toward Patient Rights. International Journal of Environmental Research and Public Health. 2021; 18(16):8628. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168628
Chicago/Turabian StyleRoth-Cohen, Osnat, Shalom Levy, and Avi Zigdon. 2021. "The Mediated Role of Credibility on Information Sources and Patient Awareness toward Patient Rights" International Journal of Environmental Research and Public Health 18, no. 16: 8628. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168628