
Minimal Clinically Important Difference and Patient Acceptable Symptom State for the Pittsburgh Sleep Quality Index in Patients Who Underwent Rotator Cuff Tear Repair

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Statistical Analysis
2.1.1. Calculation of MCID
2.1.2. Calculation of PASS
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Longo, U.G.; Candela, V.; De Salvatore, S.; Piergentili, I.; Panattoni, N.; Casciani, E.; Faldetta, A.; Marchetti, A.; De Marinis, M.G.; Denaro, V. Arthroscopic Rotator Cuff Repair Improves Sleep Disturbance and Quality of Life: A Prospective Study. Int. J. Environ. Res. Public Health 2021, 18, 3797. [Google Scholar] [CrossRef] [PubMed]
- Piper, C.C.; Hughes, A.J.; Ma, Y.; Wang, H.; Neviaser, A.S. Operative versus nonoperative treatment for the management of full-thickness rotator cuff tears: A systematic review and meta-analysis. J. Shoulder Elbow Surg. 2018, 27, 572–576. [Google Scholar] [CrossRef]
- Longo, U.G.; Berton, A.; Papapietro, N.; Maffulli, N.; Denaro, V. Epidemiology, genetics and biological factors of rotator cuff tears. Med. Sport Sci. 2012, 57, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Franceschi, F.; Longo, U.G.; Ruzzini, L.; Rizzello, G.; Maffulli, N.; Denaro, V. The Roman Bridge: A “double pulley-suture bridges” technique for rotator cuff repair. BMC Musculoskelet. Disord. 2007, 8, 123. [Google Scholar] [CrossRef] [Green Version]
- Franceschi, F.; Longo, U.G.; Ruzzini, L.; Rizzello, G.; Maffulli, N.; Denaro, V. Soft tissue tenodesis of the long head of the biceps tendon associated to the Roman Bridge repair. BMC Musculoskelet. Disord. 2008, 9, 78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kunze, K.N.; Movasagghi, K.; Rossi, D.M.; Polce, E.M.; Cohn, M.R.; Karhade, A.V.; Chahla, J. Systematic Review of Sleep Quality Before and After Arthroscopic Rotator Cuff Repair: Are Improvements Experienced and Maintained? Orthop. J. Sports Med. 2020, 8, 2325967120969224. [Google Scholar] [CrossRef]
- Franceschi, F.; Longo, U.G.; Ruzzini, L.; Rizzello, G.; Denaro, V. Arthroscopic management of calcific tendinitis of the subscapularis tendon. Knee Surg. Sports Traumatol. Arthrosc. 2007, 15, 1482–1485. [Google Scholar] [CrossRef]
- Longo, U.G.; Franceschi, F.; Ruzzini, L.; Rabitti, C.; Morini, S.; Maffulli, N.; Denaro, V. Histopathology of the supraspinatus tendon in rotator cuff tears. Am. J. Sports Med. 2008, 36, 533–538. [Google Scholar] [CrossRef]
- Khazzam, M.S.; Mulligan, E.P.; Brunette-Christiansen, M.; Shirley, Z. Sleep Quality in Patients with Rotator Cuff Disease. J. Am. Acad. Orthop. Surg. 2018, 26, 215–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maestroni, L.; Marelli, M.; Gritti, M.; Civera, F.; Rabey, M. Is rotator cuff related shoulder pain a multidimensional disorder? An exploratory study. Scand. J. Pain 2020, 20, 297–305. [Google Scholar] [CrossRef]
- Maffulli, N.; Longo, U.G.; Gougoulias, N.; Caine, D.; Denaro, V. Sport injuries: A review of outcomes. Br. Med. Bull. 2011, 97, 47–80. [Google Scholar] [CrossRef] [Green Version]
- Longo, U.G.; De Salvatore, S.; Piergentili, I.; Indiveri, A.; Di Naro, C.; Santamaria, G.; Marchetti, A.; Marinis, M.G.; Denaro, V. Total Hip Arthroplasty: Minimal Clinically Important Difference and Patient Acceptable Symptom State for the Forgotten Joint Score 12. Int. J. Environ. Res. Public Health 2021, 18, 2267. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Su, F.; Allahabadi, S.; Bongbong, D.N.; Feeley, B.T.; Lansdown, D.A. Minimal Clinically Important Difference, Substantial Clinical Benefit, and Patient Acceptable Symptom State of Outcome Measures Relating to Shoulder Pathology and Surgery: A Systematic Review. Curr. Rev. Musculoskelet. Med. 2021, 14, 27–46. [Google Scholar] [CrossRef] [PubMed]
- Malavolta, E.; Yamamoto, G.; Bussius, G.; Assunção, J.; Andrade-Silva, F.; Gracitelli, M.; Neto, A.F. Establishing minimal clinically important difference for the UCLA and ASES scores after rotator cuff repair. Orthop. Traumatol. Surg. Res. 2021, 102894. [Google Scholar] [CrossRef] [PubMed]
- Myles, P.S.; Myles, D.B.; Galagher, W.; Boyd, D.; Chew, C.; MacDonald, N.; Dennis, A. Measuring acute postoperative pain using the visual analog scale: The minimal clinically important difference and patient acceptable symptom state. Br. J. Anaesth. 2017, 118, 424–429. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Somerson, J.S.; Hsu, J.E.; Gorbaty, J.D.; Gee, A.O. Classifications in Brief: Goutallier Classification of Fatty Infiltration of the Rotator Cuff Musculature. Clin. Orthop. Relat. Res. 2016, 474, 1328–1332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Longo, U.G.; King, J.B.; Denaro, V.; Maffulli, N. Double-bundle arthroscopic reconstruction of the anterior cruciate ligament: Does the evidence add up? J. Bone Jt. Surg. Br. 2008, 90, 995–999. [Google Scholar] [CrossRef]
- Longo, U.G.; Buchmann, S.; Franceschetti, E.; Maffulli, N.; Denaro, V. A systematic review of single-bundle versus double-bundle anterior cruciate ligament reconstruction. Br. Med. Bull. 2012, 103, 147–168. [Google Scholar] [CrossRef]
- Alessandra, B. Delayed Rehabilitation Protocol after Rotator Cuff Repair. Osteology 2021, 1, 3. [Google Scholar] [CrossRef]
- Curcio, G.; Tempesta, D.; Scarlata, S.; Marzano, C.; Moroni, F.; Rossini, P.M.; Ferrara, M.; De Gennaro, L. Validity of the Italian version of the Pittsburgh Sleep Quality Index (PSQI). Neurol. Sci. 2013, 34, 511–519. [Google Scholar] [CrossRef]
- Glogovac, G.; Schumaier, A.P.; Kennedy, M.E.; Schramm, V.T.; Wells, J.; Hasselfeld, K.A.; Grawe, B.M. Narcotic Use and Resiliency Scores Do Not Predict Changes in Sleep Quality 6 Months After Arthroscopic Rotator Cuff Repair. Orthop. J. Sports Med. 2019, 7, 2325967119856282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Revicki, D.; Hays, R.D.; Cella, D.; Sloan, J. Recommended methods for determining responsiveness and minimally important differences for patient-reported outcomes. J. Clin. Epidemiol. 2008, 61, 102–109. [Google Scholar] [CrossRef]
- Mouelhi, Y.; Jouve, E.; Castelli, C.; Gentile, S. How is the minimal clinically important difference established in health-related quality of life instruments? Review of anchors and methods. Health Qual. Life Outcomes 2020, 18, 136. [Google Scholar] [CrossRef] [PubMed]
- Pickard, A.S.; Neary, M.P.; Cella, D. Estimation of minimally important differences in EQ-5D utility and VAS scores in cancer. Health Qual. Life Outcomes 2007, 5, 70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terwee, C.B.; Bot, S.D.; de Boer, M.R.; van der Windt, D.A.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C. Quality criteria were proposed for measurement properties of health status questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef] [Green Version]
- Kvien, T.K.; Heiberg, T.; Hagen, K.B. Minimal clinically important improvement/difference (MCII/MCID) and patient acceptable symptom state (PASS): What do these concepts mean? Ann. Rheum. Dis. 2007, 66 (Suppl. S3), iii40–iii41. [Google Scholar] [CrossRef]
- Galea, V.P.; Ingelsrud, L.H.; Florissi, I.; Shin, D.; Bragdon, C.R.; Malchau, H.; Gromov, K.; Troelsen, A. Patient-acceptable symptom state for the Oxford Hip Score and Forgotten Joint Score at 3 months, 1 year, and 2 years following total hip arthroplasty: A registry-based study of 597 cases. Acta Orthop. 2020, 91, 372–377. [Google Scholar] [CrossRef] [Green Version]
- Katz, P.; Kannowski, C.L.; Sun, L.; Michaud, K. Estimation of Minimally Important Differences and Patient Acceptable Symptom State Scores for the Patient-Reported Outcomes Measurement Information System Pain Interference Short Form in Rheumatoid Arthritis. ACR Open Rheumatol. 2020, 2, 320–329. [Google Scholar] [CrossRef]
- Weinberg, M.; Mollon, B.; Kaplan, D.; Zuckerman, J.; Strauss, E. Improvement in sleep quality after total shoulder arthroplasty. Phys. Sportsmed. 2020, 48, 194–198. [Google Scholar] [CrossRef]
- McDonnell, L.M.; Hogg, L.; McDonnell, L.; White, P. Pulmonary rehabilitation and sleep quality: A before and after controlled study of patients with chronic obstructive pulmonary disease. NPJ Prim. Care Respir. Med. 2014, 24, 14028. [Google Scholar] [CrossRef] [Green Version]
- Hughes, C.M.; McCullough, C.A.; Bradbury, I.; Boyde, C.; Hume, D.; Yuan, J.; Quinn, F.; McDonough, S.M. Acupuncture and reflexology for insomnia: A feasibility study. Acupunct. Med. 2009, 27, 163–168. [Google Scholar] [CrossRef]
- Eadie, J.; van de Water, A.T.; Lonsdale, C.; Tully, M.A.; van Mechelen, W.; Boreham, C.A.; Daly, L.; McDonough, S.M.; Hurley, D.A. Physiotherapy for sleep disturbance in people with chronic low back pain: Results of a feasibility randomized controlled trial. Arch. Phys. Med. Rehabil. 2013, 94, 2083–2092. [Google Scholar] [CrossRef]
- Shergis, J.L.; Ni, X.; Jackson, M.L.; Zhang, A.L.; Guo, X.; Li, Y.; Lu, C.; Xue, C.C. A systematic review of acupuncture for sleep quality in people with insomnia. Complement. Ther. Med. 2016, 26, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Jeong, J.H.; Lim, J.H.; Kim, B.K. Acupuncture using pattern-identification for the treatment of insomnia disorder: A systematic review and meta-analysis of randomized controlled trials. Integr. Med. Res. 2019, 8, 216–226. [Google Scholar] [CrossRef]
- Jaeschke, R.; Singer, J.; Guyatt, G.H. Measurement of health status. Ascertaining the minimal clinically important difference. Control. Clin. Trials 1989, 10, 407–415. [Google Scholar] [CrossRef]
- Longo, U.G.; De Salvatore, S.; Candela, V.; Berton, A.; Casciaro, C.; Sciotti, G.; Cirimele, G.; Marchetti, A.; Piergentili, I.; De Marinis, M.G.; et al. Unicompartmental Knee Arthroplasty: Minimal Important Difference and Patient Acceptable Symptom State for the Forgotten Joint Score. Medicina 2021, 57, 324. [Google Scholar] [CrossRef] [PubMed]
- Sloan, J.A.; Cella, D.; Hays, R.D. Clinical significance of patient-reported questionnaire data: Another step toward consensus. J. Clin. Epidemiol. 2005, 58, 1217–1219. [Google Scholar] [CrossRef] [PubMed]
- Norman, G.R.; Sloan, J.A.; Wyrwich, K.W. Interpretation of changes in health-related quality of life: The remarkable universality of half a standard deviation. Med. Care 2003, 41, 582–592. [Google Scholar] [CrossRef] [PubMed]
- Wyrwich, K.W.; Nienaber, N.A.; Tierney, W.M.; Wolinsky, F.D. Linking clinical relevance and statistical significance in evaluating intra-individual changes in health-related quality of life. Med. Care 1999, 37, 469–478. [Google Scholar] [CrossRef] [PubMed]
- Copay, A.G.; Glassman, S.D.; Subach, B.R.; Berven, S.; Schuler, T.C.; Carreon, L.Y. Minimum clinically important difference in lumbar spine surgery patients: A choice of methods using the Oswestry Disability Index, Medical Outcomes Study questionnaire Short Form 36, and pain scales. Spine J. 2008, 8, 968–974. [Google Scholar] [CrossRef] [PubMed]
- Stipancic, K.L.; Yunusova, Y.; Berry, J.D.; Green, J.R. Minimally Detectable Change and Minimal Clinically Important Difference of a Decline in Sentence Intelligibility and Speaking Rate for Individuals with Amyotrophic Lateral Sclerosis. J. Speech Lang. Hear. Res. 2018, 61, 2757–2771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Çelik, D.; Çoban, Ö.; Kılıçoğlu, Ö. Minimal clinically important difference of commonly used hip-, knee-, foot-, and ankle-specific questionnaires: A systematic review. J. Clin. Epidemiol. 2019, 113, 44–57. [Google Scholar] [CrossRef] [PubMed]
- MacKay, C.; Clements, N.; Wong, R.; Davis, A.M. A systematic review of estimates of the minimal clinically important difference and patient acceptable symptom state of the Western Ontario and McMaster Universities Osteoarthritis Index in patients who underwent total hip and total knee replacement. Osteoarthr. Cartil. 2019, 27, 1408–1419. [Google Scholar] [CrossRef]
- Maredupaka, S.; Meshram, P.; Chatte, M.; Kim, W.H.; Kim, T.K. Minimal clinically important difference of commonly used patient-reported outcome measures in total knee arthroplasty: Review of terminologies, methods and proposed values. Knee Surg. Relat. Res. 2020, 32, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishida, M.; Kuroiwa, Y.; Yoshida, E.; Sato, M.; Krupa, D.; Henry, N.; Ikeda, K.; Kaneko, Y. Residual symptoms and disease burden among patients with rheumatoid arthritis in remission or low disease activity: A systematic literature review. Mod. Rheumatol. 2018, 28, 789–799. [Google Scholar] [CrossRef] [Green Version]
- Innes, K.E.; Selfe, T.K.; Kandati, S.; Wen, S.; Huysmans, Z. Effects of Mantra Meditation versus Music Listening on Knee Pain, Function, and Related Outcomes in Older Adults with Knee Osteoarthritis: An Exploratory Randomized Clinical Trial (RCT). Evid. Based Complement. Altern. Med. 2018, 2018, 7683897. [Google Scholar] [CrossRef] [Green Version]
- Backhaus, J.; Junghanns, K.; Broocks, A.; Riemann, D.; Hohagen, F. Test-retest reliability and validity of the Pittsburgh Sleep Quality Index in primary insomnia. J. Psychosom. Res. 2002, 53, 737–740. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
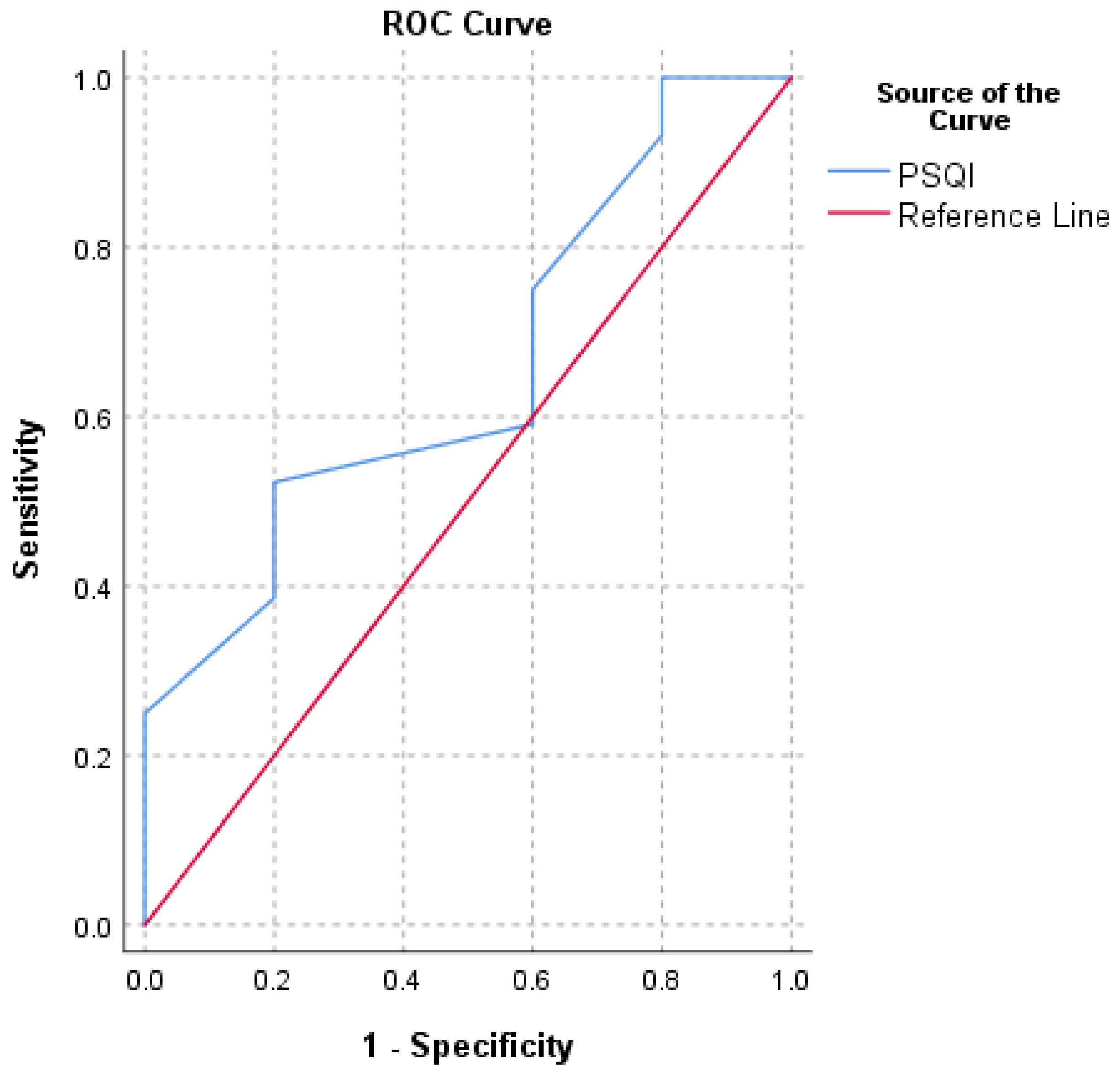
| Score | 0.5 SD | SEM | MDC | ROC (AUC) | MC |
|---|---|---|---|---|---|
| PSQI | 1.4 | 1.3 | 3.5 | 1.5 (0.8) | 4.4 |
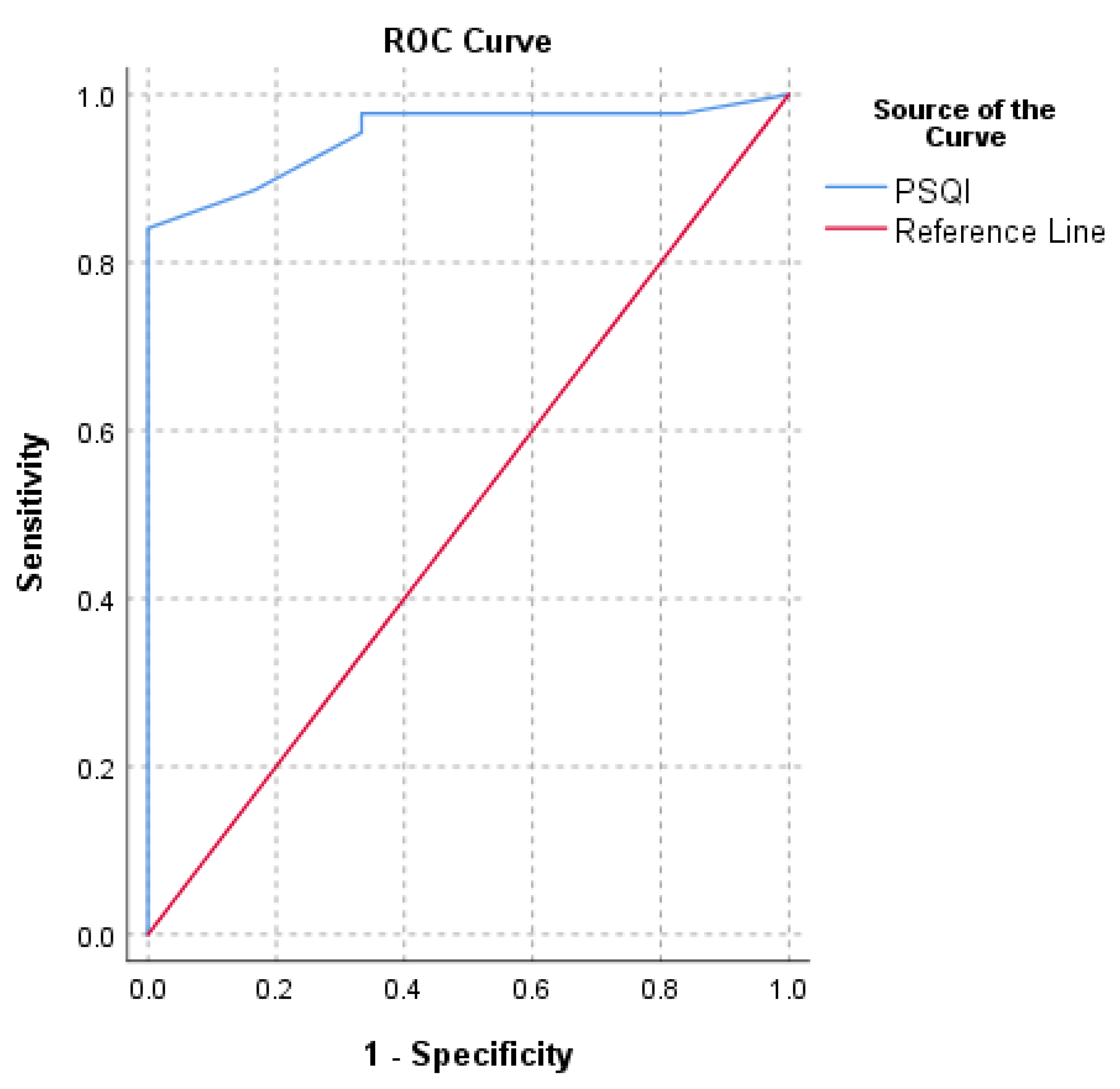
| Score | ROC (AUC) | 75th Percentile |
|---|---|---|
| PSQI | 5.5 (0.9) | 4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Longo, U.G.; Berton, A.; De Salvatore, S.; Piergentili, I.; Casciani, E.; Faldetta, A.; De Marinis, M.G.; Denaro, V. Minimal Clinically Important Difference and Patient Acceptable Symptom State for the Pittsburgh Sleep Quality Index in Patients Who Underwent Rotator Cuff Tear Repair. Int. J. Environ. Res. Public Health 2021, 18, 8666. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168666
Longo UG, Berton A, De Salvatore S, Piergentili I, Casciani E, Faldetta A, De Marinis MG, Denaro V. Minimal Clinically Important Difference and Patient Acceptable Symptom State for the Pittsburgh Sleep Quality Index in Patients Who Underwent Rotator Cuff Tear Repair. International Journal of Environmental Research and Public Health. 2021; 18(16):8666. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168666
Chicago/Turabian StyleLongo, Umile Giuseppe, Alessandra Berton, Sergio De Salvatore, Ilaria Piergentili, Erica Casciani, Aurora Faldetta, Maria Grazia De Marinis, and Vincenzo Denaro. 2021. "Minimal Clinically Important Difference and Patient Acceptable Symptom State for the Pittsburgh Sleep Quality Index in Patients Who Underwent Rotator Cuff Tear Repair" International Journal of Environmental Research and Public Health 18, no. 16: 8666. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168666