
Access to Water and Sanitation Infrastructures for Primary Schoolchildren in the South-Central Part of Côte d’Ivoire


 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
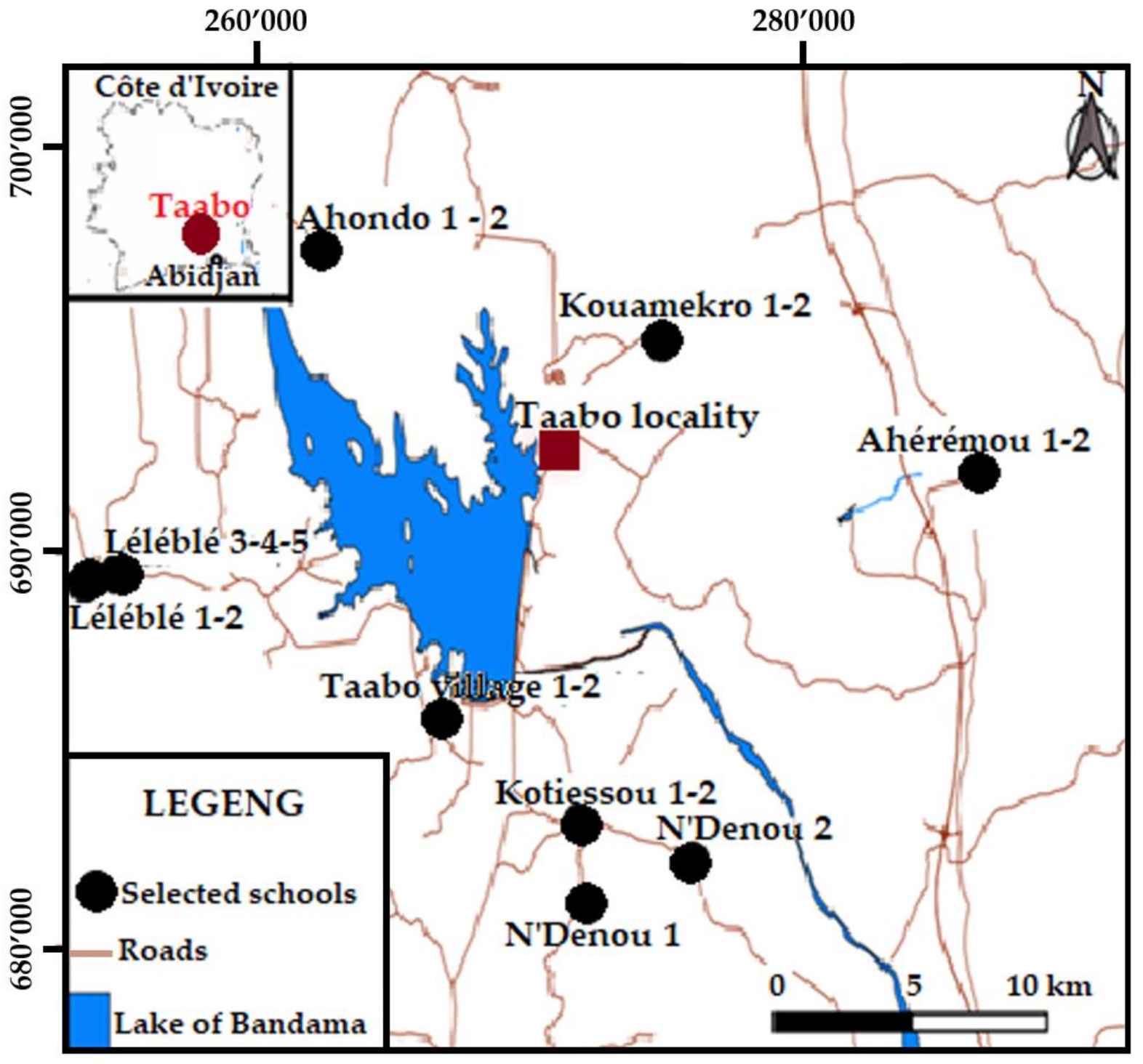
2.1. Study Area and Modules
2.2. Questionnaire Survey
2.3. WASH Facility Evaluation
2.4. Drinking Water Sampling and Quality Testing
2.5. Statistical Analysis
2.6. Ethical Considerations
3. Results
3.1. WASH-Related KAP in Schoolchildren
3.2. Availability and Quality of WASH Infrastructures
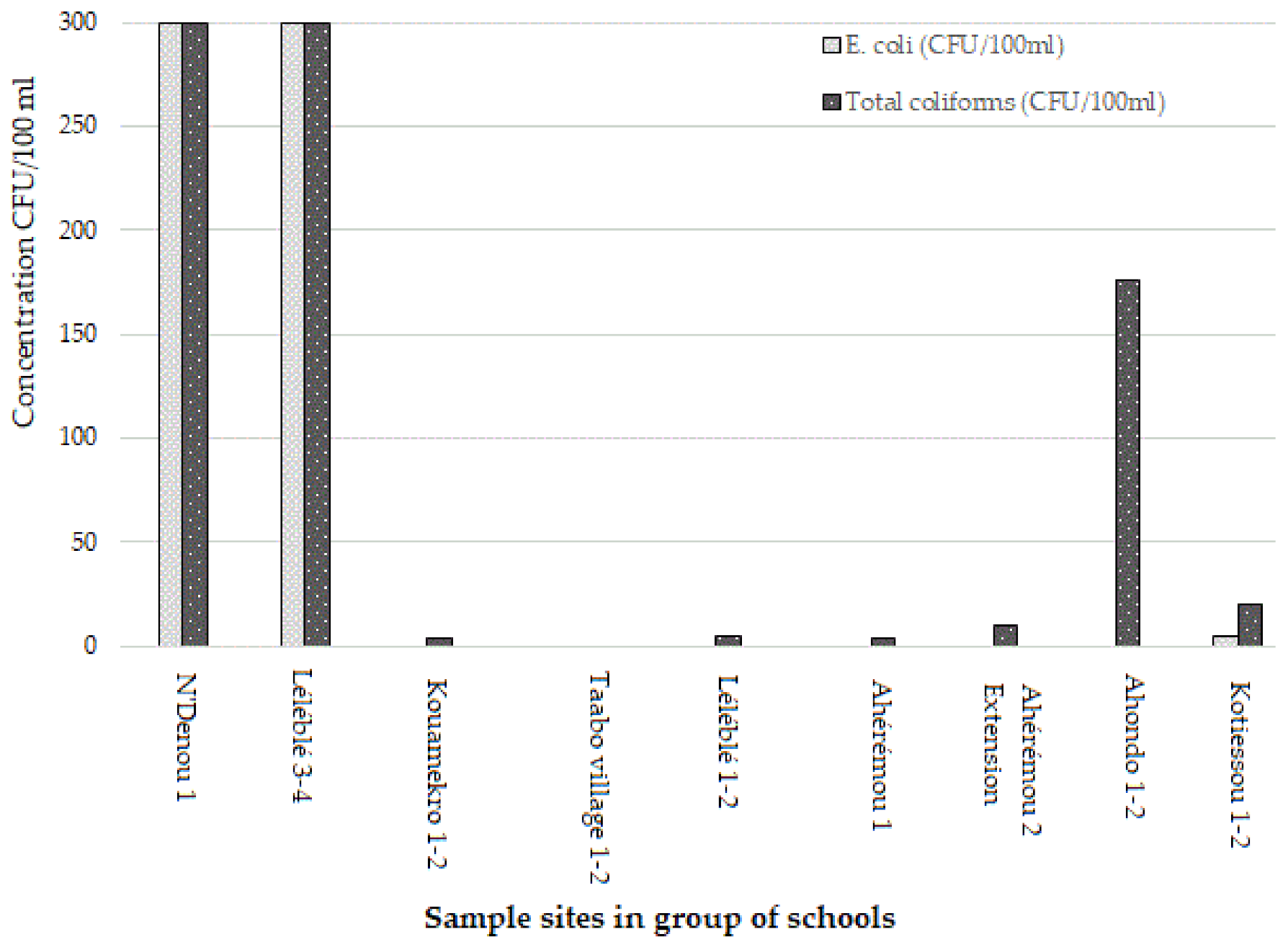
3.3. Drinking Water Quality
4. Discussion
4.1. WASH-Related Practices
4.2. Availability and Quality of WASH Infrastructure
4.3. Quality of Drinking Water
4.4. Strengths and Limitations
5. Conclusions
References
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| N° | Schools | Availability of Drinking Water | Observation and Comments |
|---|---|---|---|
| 1 | N’Denou 1 | No | Use of water from traditional wells No available latrine No handwashing facilities |
| 2 | Léléblé 3 and 4 | Yes | Foot water pump available Available latrine, not usable due to the lack of water No handwashing facilities Low flow of water, forage at 80 m |
| 3 | Kouamékro 1 and 2 | No | No water source for the school Water is provided from teacher’s homes from SODECI system No handwashing facilities |
| 4 | Taabo village 1 and 2 | Yes | Drinking water available from SODECI system No handwashing facilities Toilet available, but dirty |
| 5 | Léléblé 1 and 2 | Yes | Drinking water available Latrine available, not functioning No handwashing facilities |
| 6 | Aheremou 1 and 2 | Yes | Drinking water available No toilet or latrine available Handwashing available, not functioning |
| 7 | Aheremou 2 Extension | No | No water source for the school Water is provided from teacher’s home and stored in pots for school-children No toilet or latrine available |
| 8 | Ahondo 1 and 2 | No | No water source available Water is supplied from the village storage tanks Water is stored in pots No toilet or latrine available No handwashing facilities |
| 9 | Kotiessou 1 and 2 | Yes | Water source is available, not permanent No electricity available No handwashing facilities |
References
- Brain, R.; Johnston, R.; Slaymaker, T. Drinking water quality and the SDGs. NPJ Clean Water 2020, 3, 37. [Google Scholar] [CrossRef]
- Erridge, M. Human Right to Sanitation; Centre for Social Studies, University of Coimbra: Coimbra, Portugal, 2021; pp. 1–11. [Google Scholar]
- Prüss-Ustün, A.; Wolf, J.; Bartram, J.; Clasen, T.; Cumming, O.; Freeman, M.C.; Gordon, B.; Hunter, P.R.; Medlicott, K.; Johnston, R. Burden of disease from inadequate water, sanitation and hygiene for selected adverse health outcomes: An updated analysis with a focus on lowand middle-income countries. Int. J. Hyg. Environ. Health 2019, 2019, 765–777. [Google Scholar] [CrossRef]
- UN-SDGs. SDG 6 for Water, Sanitation and Well-Being. Available online: https://www.onedrop.org/en/news/clean-water-and-sanitation-facts-and-solutions/?gclid=EAIaIQobChMIrdK4pam_8gIVAlRgCh0i0wZzEAAYASAAEgLH8vD_BwE (accessed on 4 March 2021).
- Hürlimann, E.; Silué, K.D.; Zouzou, F.; Ouattara, M.; Schmidlin, T.; Yapi, R.B.; Houngbedji, C.A.; Dongo, K.; Kouadio, B.A.; Koné, S.; et al. Effect of an integrated intervention package of preventive chemotherapy, community-led total sanitation and health education on the prevalence of helminth and intestinal protozoa infections in Côte d’Ivoire. Parasites Vectors 2018, 11, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Wagner, J.T.; Samuelsson, I.P. WASH from the START: Water, sanitation and hygiene education in preschool. Int J. Early Child. 2019, 51, 5–21. [Google Scholar] [CrossRef]
- Strunz, E.C.; Addiss, D.G.; Stocks, M.E.; Ogden, S.; Utzinger, J.; Freeman, M.C. Water, sanitation, hygiene, and soil-transmitted helminth infection: A systematic review and meta-analysis. PLoS Med. 2014, 12, e1001620. [Google Scholar] [CrossRef] [Green Version]
- Dey, N.C.; Parvez, M.; Islam, M.R.; Mistry, S.K.; Levine, D.I. Effectiveness of a community-based water, sanitation, and hygiene (WASH) intervention in reduction of diarrhoea among under-five children: Evidence from a repeated cross-sectional study (2007–2015) in rural Bangladesh. Int. J. Hyg. Environ. Health 2019, 222, 1098–1108. [Google Scholar] [CrossRef] [PubMed]
- Freeman, M.C.; Ogden, S.; Jacobson, J.; Abbott, D.; Addiss, D.G.; Amnie, A.G.; Beckwith, C.; Cairncross, S.; Callejas, R.; Jr, J.M.C.; et al. Integration of water, sanitation, and hygiene for the prevention and control of neglected tropical diseases: A rationale for inter-sectoral collaboration. PLoS Negl. Trop. Dis. 2019, 7, e2439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melariri, P.; Steenkamp, L.; Williams, M.; Mtembu, C.; Ronaasen, J.; Truter, I. Water, sanitation and hygiene practices in early childhood development (ECD) centres in low socio-economic areas in Nelson Mandela Bay, South Africa. J. Water Sanit. Hyg. Dev. 2019, 9, 164–171. [Google Scholar] [CrossRef] [Green Version]
- Nery, S.V.; Pickering, A.J.; Abate, E.; Asmare, A.; Barrett, L.; Chung, J.B.; Bundy, D.A.P.; Thomas, C.; Clements, A.C.A.; Colford, J.M., Jr.; et al. The role of water, sanitation and hygiene interventions in reducing soil-transmitted helminths: Interpreting the evidence and identifying next steps. Parasites Vectors 2019, 12, 273. [Google Scholar] [CrossRef] [PubMed]
- Vilcins, D.; Sly, P.D.; Jagals, P. Environmental risk factors associated with child stunting: A systematic review of the literature. Ann. Glob. Health 2018, 84, 551–562. [Google Scholar] [CrossRef]
- Shao, T.; Zhao, J.; Hu, H.; Zhang, Q. Analysis of factors affecting students going to school toilets in a rural primary school in China. BMC Public Health 2021, 21, 32. [Google Scholar] [CrossRef] [PubMed]
- Aschale, A.; Adane, M.; Getachew, M.; Faris, K.; Gebretsadik, D.; Sisay, T.; Dewau, R.; Chanie, M.G.; Muche, A.; Zerga, A.A.; et al. Water, sanitation, and hygiene conditions and prevalence of intestinal parasitosis among primary school children in Dessie City, Ethiopia. PLoS ONE 2021, 16, e0245463. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Planning and Develoment Côte d’Ivoire. Rapport Volontaire D’examen National de Mise en Oeuvre des Objectifs du Developpement Durable (ODD); Côte d’Ivoire; 2019; pp. 1–153. Available online: https://sustainabledevelopment.un.org/content/documents/23390Burkina_Faso_VNR_FINAL.pdf/ (accessed on 22 April 2021).
- UNESCO Institute for Statistics. Leaving no One Behind: How far on the Way to Universal Primary and Secondary Education? UNESCO, 2016; pp. 1–16. Available online: https://en.unesco.org/gem-report/leaving-no-one-behind-how-far-way-universal-primary-and-secondary-education (accessed on 22 April 2021).
- UNICEF. Analyse de la Situation des Enfants en Côte D’ivoire; UNICEF: Côte d’Ivoire, 2019; p. 139. Available online: https://www.unicef.org/cotedivoire/rapports/analyse-de-la-situation-des-enfants-et-des-femmes-de-c%C3%B4te-divoire-2019 (accessed on 22 April 2021).
- Koné, S.; Baikoro, N.; N’Guessan, Y.; Jaeger, F.N.; Silué, K.D.; Fürst, T.; Hürlimann, E.; Ouattara, M.; Séka, M.-C.Y.; N’Guessan, N.A.; et al. Health & demographic surveillance system profile: The Taabo health and demographic surveillance system, Côte d’Ivoire. Int. J. Epidemiol 2015, 44, 87–97. [Google Scholar] [CrossRef] [Green Version]
- Schmidlin, T.; Hürlimann, E.; Silué, K.D.; Yapi, R.B.; Houngbedji, C.; Kouadio, B.A.; Acka-Douabé, C.A.; Dongo, K.; Ouattara, M.; Zouzou, F.; et al. Effects of hygiene and defecation behavior on helminths and intestinal protozoa infections in Taabo, Côte d’Ivoire. PLoS ONE 2013, 8, e65722. [Google Scholar] [CrossRef] [Green Version]
- Koné, S.; Fürst, T.; Jaeger, F.N.; Esso, E.L.J.C.; Baïkoro, N.; Kouadio, K.A.; Adiossan, L.G.; Zouzou, F.; Boti, L.I.; Tanner, M.; et al. Causes of death in the Taabo health and demographic surveillance system, Côte d’Ivoire, from 2009 to 2011. Glob. Health Action 2015, 8, 27271. [Google Scholar] [CrossRef]
- Baiden, F.; Hodgson, A.; Binka, F.N. Demographic Surveillance Sites and emerging CHALLENGES in International Health. Available online: https://www.who.int/bulletin/volumes/84/3/editorial20306html/en/ (accessed on 22 April 2021).
- WHO. Weekly bulletin on outbreaks and other emergencies. In WHO Report; 2018; pp. 1–25. Available online: https://www.afro.who.int/health-topics/disease-outbreaks/outbreaks-and-other-emergencies-updates (accessed on 22 April 2021).
- Nissui. Pharmaceutical—Compact Dry™. Available online: https://www.nissui-pharm.co.jp/english/ (accessed on 5 July 2021).
- Baker, J.M.; Trinies, V.; Bronzan, R.N.; Dorkenoo, A.M.; Garn, J.V.; Sognikin, S.; Freeman, M.C. The associations between water and sanitation and hookworm infection using cross-sectional data from Togo’s national deworming program. PLoS Negl. Trop. Dis. 2018, 12, e0006374. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenland, K.; Dixon, R.; Khan, S.A.; Gunawardena, K.; Kihara, J.H.; Smith, J.L.; Drake, L.; Makkar, P.; Raman, S.; Singh, S.; et al. The epidemiology of soil-transmitted helminths in Bihar state, India. PLoS Negl. Trop. Dis. 2015, 9, e0003790. [Google Scholar] [CrossRef] [Green Version]
- Grimes, J.E.T.; Croll, D.; Harrison, W.E.; Utzinger, J.; Freeman, M.C.; Templeton, M.R. The relationship between water, sanitation and schistosomiasis: A systematic review and meta-analysis. PLoS Negl. Trop. Dis. 2014, 8, e3296. [Google Scholar] [CrossRef] [PubMed]
- Speich, B.; Croll, D.; Fürst, T.; Utzinger, J.; Keiser, J. Effect of sanitation and water treatment on intestinal protozoa infection: A systematic review and meta-analysis. Lancet Infect. Dis. 2016, 16, 87–99. [Google Scholar] [CrossRef]
- Saleem, M.; Burdett, T.; Heaslip, V. Health and social impacts of open defecation on women: A systematic review. BMC Public Health 2019, 19, 158. [Google Scholar] [CrossRef] [Green Version]
- MacRae, E.R.; Clasen, T.; Dasmohapatra, M.; Caruso, B.A. ‘It’s like a burden on the head’: Redefining adequate menstrual hygiene management throughout women’s varied life stages in Odisha, India. PLoS ONE 2019, 14, e0220114. [Google Scholar] [CrossRef] [Green Version]
- Schmitt, M.L.; Wood, O.R.; Clatworthy, D.; Rashid, S.F.; Sommer, M. Innovative strategies for providing menstruation-supportive water, sanitation and hygiene (WASH) facilities: Learning from refugee camps in Cox’s bazar, Bangladesh. BMC Confl. Health 2021, 15, 10. [Google Scholar] [CrossRef]
- Beshearse, E.; Bruce, B.B.; Nane, G.F.; Cooke, R.M.; Aspinall, W.; Hald, T.; Crim, S.M.; Griffin, P.M.; Fullerton, K.E.; Collier, S.A.; et al. Attribution of illnesses transmitted by food and water to comprehensive transmission pathways using structured expert judgment, United States. Emerg. Infect. Dis. 2021, 27, 182–195. [Google Scholar] [CrossRef] [PubMed]
- Sibiya, J.E.; Jabulani, R.G. Knowledge, attitude and practices (KAP) survey on water, sanitation and hygiene in selected schools in Vhembe district, Limpopo, South Africa. Int. J. Environ. Res. Public Health 2013, 10, 2282–2295. [Google Scholar] [CrossRef]
- Sangalang, S.O.; Medina, S.A.J.; Ottong, Z.J.; Lemence, A.L.G.; Totanes, D.; Valencia, J.C.; Singson, P.A.A.; Olaguera, M.; Prado, N.O.; Ocaña, R.M.Z.; et al. Protocol for a trial assessing the impacts of school-based WASH interventions on children’s health literacy, handwashing, and nutrition status in low- and middle-income countries. Study protocol. Int. J. Environ. Res. Public Health 2021, 18, 226. [Google Scholar] [CrossRef] [PubMed]
- McMichael, C. Water, sanitation and hygiene (WASH) in schools in low-income countries: A review of evidence of impact. Int J. Environ. Res. Public Health 2019, 16, 359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Odonkor, S.T.; Ampofo, J.K. Escherichia coli as an indicator of bacteriological quality of water: An overview. Microbiol. Res. 2013, 4, 5–11. [Google Scholar] [CrossRef]
- Kubera, Ł. Spread patterns of antibiotic resistance in faecal indicator bacteria contaminating an urbanized section of the Brda River. Microb. Ecol. 2021, 81, 592–600. [Google Scholar] [CrossRef] [PubMed]
- Acheampong, P.; Akodwaa-Boadi, K.; Appiah-Effah, E.; Nyarko, K.B. WASH infrastructure and menstrual hygiene management in basic schools: A study in Kumasi, Ghana. In Proceedings of the 41st WEDC International Conference, Nakuru, Kenya, 9–13 July 2018. [Google Scholar]
- Guehi, E.Z.; Secredou, K.M. The experience of menstruation at school: A study with high school girls in the northern Côte D’Ivoire. Coll. Antropol. 2019, 43, 183–190. [Google Scholar]
- Cronk, R.; Guo, A.; Lisa, F.; Bartram, J. Factors associated with water quality, sanitation, and hygiene in rural schools in 14 low- and middle-income countries. Sci. Total Environ. 2021, 761, 144226. [Google Scholar] [CrossRef] [PubMed]
- Saric, J.; Blaettler, D.; Bonfoh, B.; Hostettler, S.; Jimenez, E.; Kiteme, B.; Koné, I.; Lys, J.-A.; Masanja, H.; Steinger, E.; et al. Leveraging research partnerships to achieve the 2030 Agenda: Experiences from North-South cooperation. GAIA 2019, 28, 143–150. [Google Scholar] [CrossRef]
- Fernandez, A.G.; Symonds, E.M.; Gallard-Gongora, J.F.; Mull, B.; Lukasik, J.O.; Rivera, N.P.; Aguilar, A.B.; Peraud, J.; Brown, M.L.; Alvarado, D.M.; et al. Relationships among microbial indicators of fecal pollution, microbial source tracking markers, and pathogens in Costa Rican coastal waters. Water Res. 2021, 188, 116507. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, D.C.; Graziele, I.; Marques, R.C.; Gonçalves, J. Investment in drinking water and sanitation infrastructure and its impact on waterborne diseases dissemination: The Brazilian case. Sci. Total Environ. 2021, 779, 146279. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.M.; Kunwar, S.B.; Bohara, A.K. The interconnection between water quality level and health status: An analysis of Escherichia coli contamination and drinking water from Nepal. Water Resour. Econ. 2021, 34, 100179. [Google Scholar] [CrossRef]
- Uprety, S.; Dangol, B.; Nakarmi, P.; Dhakal, I.; Sherchan, S.P.; Shisler, J.L.; Jutla, A.; Amarasiri, M.; Sano, D.; Nguyen, T.H. Assessment of microbial risks by characterization of Escherichia coli presence to analyze the public health risks from poor water quality in Nepal. Int. J. Hyg. Environ. Health 2020, 226, 113484. [Google Scholar] [CrossRef]
- Singh, A.K.; Bhardwaj, S.K.; Devi, S. Microbiological status of drinking water sources and its relationship with human health in Solan, India. Environ. Monit. Assess. 2021, 193, 32. [Google Scholar] [CrossRef]
- Zouandé, S.F. GOVERNANCE and Democratic Transition in Africa: Understanding “Ivoirité” and the Ethnicity Challenges to Citizenship and Nation-Building in Côte d’Ivoire. Master’s Thesis, Howard University, Washington, DC, USA, 2011. [Google Scholar]
- Mulopo, C.; Chimbari, M.J. Water, sanitation, and hygiene for schistosomiasis prevention: A qualitative analysis of experiences of stakeholders in rural KwaZulu-Natal. J. Water Sanit. Hyg. Dev. 2021, 11, 255–270. [Google Scholar] [CrossRef]



| Schools with Access to Drinking Water (95% CI) | Schools without Access to Drinking Water (95% CI) | p-Value for Difference | |
|---|---|---|---|
| Number of students Female (%) | 394 52.8 (47.7–57.9) | 377 55.7 (50.7–61.0) | 0.382 |
| Age (median in years) IQR | 11 2 | 11 2 | 0.847 |
| School level (%) Level 1 (CM1) Level 2 (CM2) NA | 47.2 (42.1–52.4) 50.8 (45.7–55.9) 2.0 (0.0–7.2) | 50.7 (45.6–56.1) 49.3 (44.3–54.7) | 0.157 |
| Schools with Access to Drinking Water | Schools without Access to Drinking Water | p-Value for Difference | |
|---|---|---|---|
| Toilet/latrine use at school (%) | 27.7 (23.4–32.2) | 22.0 (18.8–26.3) | 0.530 |
| Reasons for not using the toilet/latrine (%) Bad smell Dirty Not functioning Not enough toilets No privacy No water No soap Toilets are always open | 16.5 (11.9–21.6) 27.9 (22.8–33.3) 6.1 (2.0–10.6) 1.5 (0.0–5.8) 1.0 (0.0–5.2) 7.4 (3.0–11.8) 7.6 (3.3–12.1) 31.5 (26.4–36.9) | 12.7 (8.0–17.9) 15.4 (10.6–20.5) 3.7 (0.0–9.0) 1.1 (0.0–6.3) 0.3 (0.0–5.5) 8.5 (3.7–13.7) 7.9 (3.2–13.2) 39.0 (33.7–44.7) | 0.309 0.736 0.747 0.682 0.619 0.098 0.229 0.263 |
| Preferred place of defecation/urination while at school (%): Toilet/latrine In the bushes Behind the latrine At home | 4.1 (0.8–7.8) 56.9 (52.0–62.1) 3.0 (0.0–6.6) 15.7 (11.4–20.2) | 6.6 (2.4–11.2) 58.1 (53.1–63.3) 1.3 (0.0–5.5) 14.9 (15.4–25.0) | 0.384 0.355 0.212 0.916 |
| Schools with Access to Drinking Water | Schools without Access to Drinking Water | p-Value for Difference2 | |
|---|---|---|---|
| Handwashing with soap/detergent (practice) (%) Before eating After eating After defecation After playing | 70.3 (66.0–75.1) 58.1 (53.3–63.3) 60.2 (55.3–65.3) 38.6 (33.8–43.6) | 72.7 (68.4–77.4) 49.1 (44.0–54.5) 65.0 (60.2–70.0) 35.5 (30.8–40.7) | 0.668 0.224 0.421 0.540 |
| Handwashing with soap/detergent (knowledge) (%) Before eating After eating After defecation After playing | 78.9 (75.1–83.0) 69.8 (65.5–74.6) 73.1 (68.8–77.5) 62.9 (58.1–67.9) | 80.9 (77.2–84.9) 59.4 (54.4–64.6) 77.7 (73.7–82.0) 52.5 (47.5–57.9) | 0.705 0.145 0.475 0.100 |
| Handwashing score practice (comparison of means) | 2.27 | 2.22 | 0.794 |
| Handwashing score knowledge (comparison of means) | 2.85 | 2.71 | 0.479 |
| Water can cause diseases (%) | 68.0 (63.5–72.8) | 84.1 (80.6–87.6) | <0.001 *** |
| Fresh water exposure (%) Doing the laundry Playing Fishing Working | 55.8 (51.0–61.2) 32.0 (27.4–36.9) 20.1 (15.7–24.7) 19.8 (14.7–24.6) | 36.3 (31.3–41.6) 34.2 (29.4–39.3) 11.7 (7.4–16.0) 5.0 (0.3–10.3) | <0.001 *** 0.773 0.075 <0.001 *** |
| Disease | Number of Students | % |
|---|---|---|
| Stomach ache | 326 | 42.3 |
| Diarrhoea | 126 | 16.3 |
| Typhoid fever | 13 | 1.7 |
| Cholera | 14 | 1.8 |
| Vomiting | 9 | 1.2 |
| Schistosomiasis | 16 | 2.1 |
| Malaria | 127 | 16.5 |
| Headaches | 51 | 6.6 |
| Skin rashes | 26 | 3.4 |
| AIDS or HIV | 24 | 3.1 |
| Fever | 18 | 2.3 |
| Diabetes | 7 | 0.9 |
| Not applicable. or do not know | 277 | 35.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kouamé, P.K.; Galli, A.; Peter, M.; Loss, G.; Wassa, D.; Bonfoh, B.; Utzinger, J.; Winkler, M.S. Access to Water and Sanitation Infrastructures for Primary Schoolchildren in the South-Central Part of Côte d’Ivoire. Int. J. Environ. Res. Public Health 2021, 18, 8863. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168863
Kouamé PK, Galli A, Peter M, Loss G, Wassa D, Bonfoh B, Utzinger J, Winkler MS. Access to Water and Sanitation Infrastructures for Primary Schoolchildren in the South-Central Part of Côte d’Ivoire. International Journal of Environmental Research and Public Health. 2021; 18(16):8863. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168863
Chicago/Turabian StyleKouamé, Parfait K., Anaïs Galli, Maryna Peter, Georg Loss, Diarassouba Wassa, Bassirou Bonfoh, Jürg Utzinger, and Mirko S. Winkler. 2021. "Access to Water and Sanitation Infrastructures for Primary Schoolchildren in the South-Central Part of Côte d’Ivoire" International Journal of Environmental Research and Public Health 18, no. 16: 8863. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168863