
Advancing Our Understanding of Dental Care Pathways of Refugees and Asylum Seekers in Canada: A Qualitative Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants and Recruitment
2.2. Methods for Data Generation
2.3. Data Management and Analysis
2.4. Ethical Approval
3. Results
3.1. Participant Profile
3.2. Facilitators to Care
3.2.1. Importance of Oral Health
3.2.2. Changes in Oral Hygiene Practice
3.3. Barriers to Care
3.3.1. Financial Constraints
3.3.2. Waiting Time for Receipt of Dental Care
3.3.3. Language Barriers
“The first problem I had was with the receptionist because she said I needed a translator even though I told her I understood. Another woman helped me, she was kinder, filled out my forms and gave me an appointment.” (37-year-old Mexican man).
“The first thing I had to do is to fill out all the paperwork and I felt like it was overwhelming.” (41–year-old Venezuelan woman).
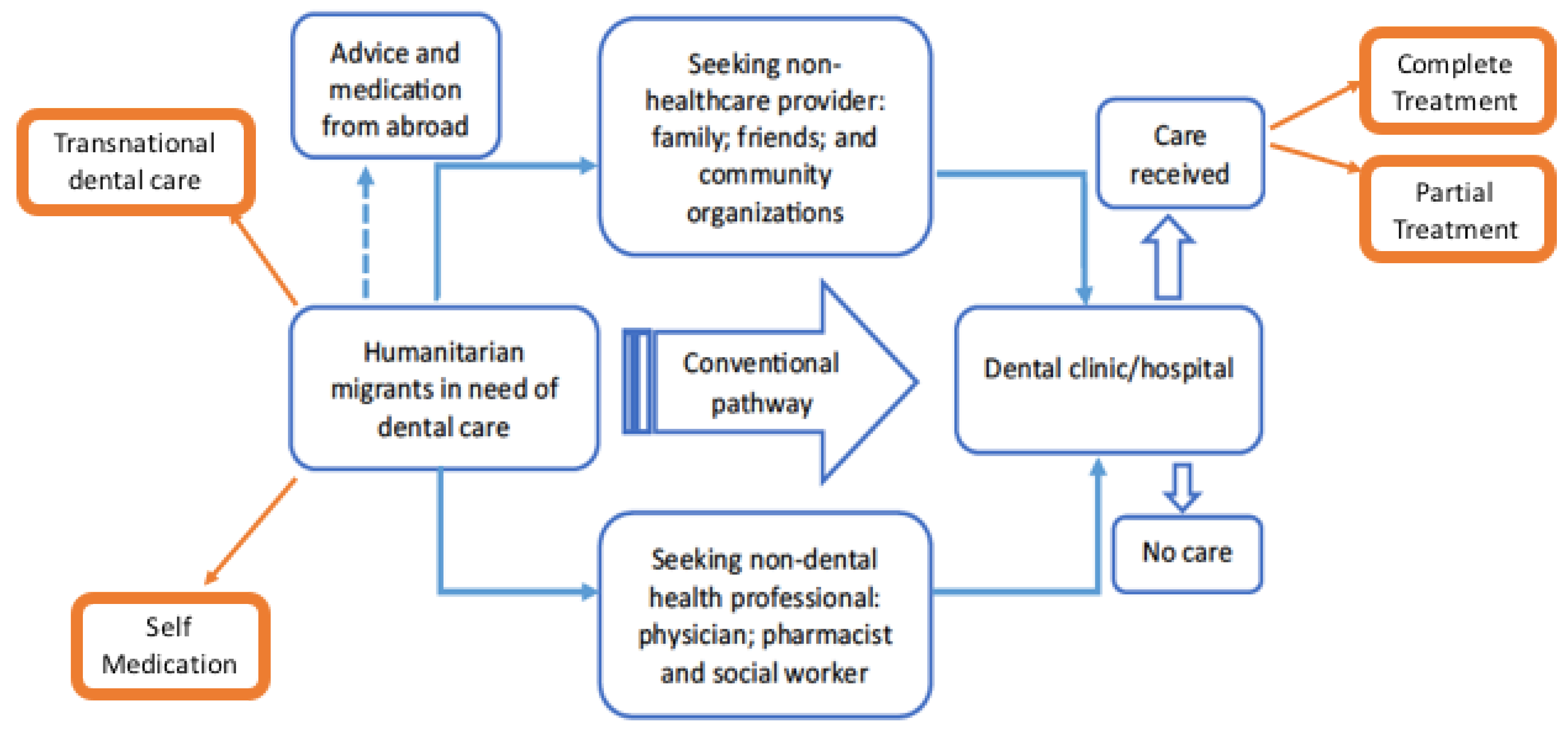
3.4. Two New Pathways
3.4.1. Transnational Dental Care
“In my country, we have better access and [treatment] is cheaper.” (56-year-old Venezuelan woman).
“In my country there isn’t much protocol; here you have to go through many steps.” (31-year-old Venezuelan man).
“In Egypt and Syria, dentists are very clever.... the filling does not come out.” (27-year-old Syrian woman).
“I had a crown done for me back home in Iraq before 2003. Until today, it is the same colour, the same colour as my teeth.” (47-year-old Iraqi woman).
3.4.2. Self-Medication
3.5. Outcomes of Care Received
“They did two fillings but one of then was very deep. When they did it, I think they touched the nerve… that in a week I couldn’t bear the pain. Three weeks passed, I went to see the dentist, he told me it was sensitivity and that I had to go somewhere else to get it fixed because he couldn’t. He gave me a card, so he referred me to another doctor where I had to pay. I had the pain for a month, I had to pay for a root canal treatment $1400 and I haven’t come back for the crown yet because it is another $900.”
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- UNHCR. Refugees at Glance. 2021. Available online: https://www.unhcr.org/figures-at-a-glance.html (accessed on 17 June 2021).
- UNHCR. Convention and Protocol Relating to the Status of Refugees. 1951. Available online: https://www.unhcr.org/3b66c2aa10.html (accessed on 17 June 2021).
- UNHCR. Refugees in Canada. 2021. Available online: https://www.unhcr.ca/in-canada/refugees-in-canada/ (accessed on 17 June 2021).
- Keboa, M.T.; Hiles, N.; Macdonald, M.E. The oral health of refugees and asylum seekers: A scoping review. Glob. Health 2016, 12, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghiabi, E.; Matthews, D.C.; Brillant, M.S. The Oral Health Status of Recent Immigrants and Refugees in Nova Scotia, Canada. J. Immigr. Minor. Health 2014, 16, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Kohlenberger, J.; Buber-Ennser, I.; Rengs, B.; Leitner, S.; Landesmann, M. Barriers to health care access and service utilization of refugees in Austria: Evidence from a cross-sectional survey. Health Policy 2019, 123, 833–839. [Google Scholar] [CrossRef] [PubMed]
- Dehmoobadsharifabadi, A.; Singhal, S.; Quiñonez, C. Investigating the “inverse care law” in dental care: A comparative analysis of Canadian jurisdictions. Can. J. Public Health 2017, 107, e538–e544. [Google Scholar] [CrossRef] [PubMed]
- Mathur, M.; Williams, D.; Reddy, K.S.; Watt, R. Universal Health Coverage: A Unique Policy Opportunity for Oral Health. J. Dent. Res. 2015, 94, 3S–5S. [Google Scholar] [CrossRef] [Green Version]
- Ramraj, C.; Weitzner, E.; Figueiredo, R.; Quiñonez, C. A macroeconomic review of dentistry in Canada in the 2000s. J. Can. Dent. Assoc. 2014, 80, e55–e61. [Google Scholar]
- Statistics Canada. Health Fact Sheets: Dental Care; Statistics Canada: Ottawa, ON, Canada, 2018.
- Quiñonez, C.; Grootendorst, P. Equity in dental care among Canadian households. Int. J. Equity Health 2011, 10, 14. [Google Scholar] [CrossRef] [Green Version]
- Keboa, M.T.; Hovey, R.; Nicolau, B.; Esfandiari, S.; Carnevale, F.; Macdonald, M.E. Oral healthcare experiences of humanitarian migrants in Montreal, Canada. Can. J. Public Health 2019, 110, 453–461. [Google Scholar] [CrossRef]
- Grembowski, D.; Andersen, R.M.; Chen, M.-S. A Public Health Model of the Dental Care Process. Med. Care Rev. 1989, 46, 439–496. [Google Scholar] [CrossRef]
- Antonipillai, V.; Baumann, A.; Hunter, A.; Wahoush, O.; O’Shea, T. Health Inequity and “Restoring Fairness” through the Canadian Refugee Health Policy Reforms: A Literature Review. J. Immigr. Minor. Health 2018, 20, 203–213. [Google Scholar] [CrossRef]
- Government of Canada. Interim Federal Health Program: What Is Covered. Available online: https://www.canada.ca/en/immigration-refugees-citizenship/services/refugees/help-within-canada/health-care/interim-federal-health-program/coverage-summary.html (accessed on 15 June 2021).
- Macdonald, M.E.; Keboa, M.T.; Nurelhuda, N.M.; Lawrence, H.P.; Carnevale, F.; McNally, M.; Singhal, S.; Ka, K.; Nicolau, B. The Oral Health of Refugees and Asylum Seekers in Canada: A Mixed Methods Study Protocol. Int. J. Environ. Res. Public Health 2019, 16, 542. [Google Scholar] [CrossRef] [Green Version]
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for reporting qualitative research: A synthesis of recommendations. Acad. Med. J. Assoc. Am. Med. Coll. 2014, 89, 1245–1251. [Google Scholar] [CrossRef]
- Reda, S.F.; Reda, S.M.; Thomson, W.M.; Schwendicke, F. Inequality in Utilization of Dental Services: A Systematic Review and Meta-analysis. Am. J. Public Health 2018, 108, e1–e7. [Google Scholar] [CrossRef]
- Allin, S.; Farmer, J.; Quiñonez, C.; Peckham, A.; Marchildon, G.; Panteli, D.; Henschke, C.; Fattore, G.; Lamloum, D.; Holden, A.C.; et al. Do health systems cover the mouth? Comparing dental care coverage for older adults in eight jurisdictions. Health Policy 2020, 124, 998–1007. [Google Scholar] [CrossRef] [PubMed]
- Zangiabadi, S.; Costanian, C.; Tamim, H. Dental care use in Ontario: The Canadian community health survey (CCHS). BMC Oral Health 2017, 17, 165. [Google Scholar] [CrossRef] [Green Version]
- Services Covered by Healthy Smiles Ontario. Available online: https://www.ontario.ca/page/services-covered-by-healthy-smiles-ontario (accessed on 16 June 2021).
- Kateeb, E.; Zaheer, K.; Fisher, J.; Ghani, A.A.E.; Williams, D.; Dartevelle, S. Promoting Oral Health for Refugees: An Advocacy Guide; FDI World Dental Federation: Geneva, Switzerland, 2020.
- Pottie, K.; Greenaway, C.; Feightner, J.; Welch, V.; Swinkels, H.; Rashid, M.; Narasiah, L.; Kirmayer, L.J.; Ueffing, E.; MacDonald, N.E.; et al. Evidence-based clinical guidelines for immigrants and refugees. Can. Med. Assoc. J. 2011, 183, E824–E925. [Google Scholar] [CrossRef] [Green Version]
- Calvasina, P.; Muntaner, C.; Quiñonez, C. Transnational dental care among Canadian immigrants. Community Dent. Oral Epidemiol. 2015, 43, 444–451. [Google Scholar] [CrossRef]
- Dong, M.; Levine, A.; Loignon, C.; Bedos, C. Chinese immigrants’ dental care pathways in Montreal, Canada. J. Can. Dent. Assoc. 2011, 77, b131. [Google Scholar]
- Adams, K.; Snyder, J.; Crooks, V. Narratives of a “Dental Oasis”: Examining Media Portrayals of Dental Tourism in the Border Town of Los Algodones, Mexico. J. Borderl. Stud. 2019, 34, 325–341. [Google Scholar] [CrossRef]
- Adams, K.; Snyder, J.; Crooks, V.A. The Perfect Storm: What’s Pushing Canadians Abroad for Dental Care? J. Can. Dent. Assoc. 2017, 83, h10. [Google Scholar] [PubMed]
- Hernandez-Juyol, M.; Job-Quesada, J.R. Dentistry and Self-Medication: A Current Challenge. Med. Oral 2002, 7, 344–347. [Google Scholar] [PubMed]
- Idowu, E.; Afolabi, A.; Fakuade, B.; Akintububo, O.; Ibiyemi, O. Self-Medication Profile of Dental Patients Attending a North Eastern Tertiary Hospital in Nigeria. Ann. Ib. Postgrad. Med. 2019, 17, 173–180. [Google Scholar]
- Jain, A.K.; Bhaskar, D.J.; Gupta, D.N.; Agali, C.; Yadav, P.; Khurana, R. Practice of Self-Medication for Dental Problems in Uttar Pradesh, India. Oral Health Prev. Dent. 2016, 14, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Agbor, A.M.; Azodo, C.C. Self medication for oral health problems in Cameroon. Int. Dent. J. 2011, 61, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Bennadi, D. Self-medication: A current challenge. J. Basic Clin. Pharm. 2013, 5, 19–23. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Middle East (Arabic) | Central and South America (Spanish) | South Asia (Dari) | Africa (English) | Total |
|---|---|---|---|---|---|
| Country of origin | Palestine, Syria, and Iraq. | Mexico, El Salvador, Honduras, and Venezuela. | Iran and Afghanistan. | Eritrea, Somalia, Nigeria, and the Democratic Republic of the Congo. | 13 |
| Number of participants | 7 | 9 | 4 | 7 | 27 |
| Age Range (years) | 28–62 | 31–56 | 29–51 | 21–49 | 28–62 |
| Gender | |||||
| Man | 1 | 5 | 1 | 2 | 9 |
| Woman | 6 | 4 | 3 | 5 | 18 |
| Completed Education | |||||
| Less than high school | 3 | 0 | 1 | 4 | 8 |
| High school and above | 4 | 9 | 3 | 3 | 19 |
| Immigration status upon arrival in Canada | |||||
| Refugee | 3 | 1 | 4 | 4 | 12 |
| Refugee Claimant (Asylum seeker) | 4 | 8 | 0 | 3 | 15 |
| Current immigration status | |||||
| Refugee | 6 | 1 | 4 | 6 | 17 |
| Refugee claimant (Asylum seeker) | 1 | 8 | 0 | 1 | 10 |
| Employment status | |||||
| Full or part time | 1 | 3 | 2 | 0 | 6 |
| Unemployed | 6 | 6 | 2 | 7 | 21 |
| Income | |||||
| ≤$20,000 | 6 | 6 | 2 | 7 | 21 |
| >$20,000 | 1 | 3 | 2 | 0 | 6 |
| Spent time in a refugee camp | |||||
| Yes | 3 | 2 | 0 | 0 | 5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nurelhuda, N.M.; Keboa, M.T.; Lawrence, H.P.; Nicolau, B.; Macdonald, M.E. Advancing Our Understanding of Dental Care Pathways of Refugees and Asylum Seekers in Canada: A Qualitative Study. Int. J. Environ. Res. Public Health 2021, 18, 8874. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168874
Nurelhuda NM, Keboa MT, Lawrence HP, Nicolau B, Macdonald ME. Advancing Our Understanding of Dental Care Pathways of Refugees and Asylum Seekers in Canada: A Qualitative Study. International Journal of Environmental Research and Public Health. 2021; 18(16):8874. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168874
Chicago/Turabian StyleNurelhuda, Nazik M., Mark T. Keboa, Herenia P. Lawrence, Belinda Nicolau, and Mary Ellen Macdonald. 2021. "Advancing Our Understanding of Dental Care Pathways of Refugees and Asylum Seekers in Canada: A Qualitative Study" International Journal of Environmental Research and Public Health 18, no. 16: 8874. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168874