
Impact of the COVID-19 Pandemic on Burnout in Primary Care Physicians in Catalonia

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Instrument
2.2. Analysis
3. Results
4. Discussion and Conclusions
- A new agreement for health among political forces in Catalonia and Spain;
- More economic resources: an estimated 5 billion euros of additional funding for health in Catalonia and of 25 billion in Spain;
- Better conditions and resources for health professionals, using 60% of the additional funding. Emphasis on increased salaries for junior staff and staff in training;
- Better facilities and infrastructure: 40% of additional funding to replace obsolete resources;
- Professionalism: the reform must be based on the values, knowledge, and experience of healthcare professionals;
- Health organisation: participative definition of healthcare goals and challenges of the Catalonia Health Plan. Results-based; autonomy in management; flexibility of working models;
- Coordination and patient-centered care across the various healthcare services;
- Greater social emphasis. Linking social and health services, with a new support model for the elderly;
- A solid public health service ready for the new challenges. Protection, prevention, participation. International coordination;
- The experience of COVID-19, an opportunity to learn from failures and to strenghthen assets. “Without health, there is no future”.
- -
- Establish a new social and political agreement to provide much needed additional resources;
- -
- Transform organizational models of primary care centres, making them more adaptable (improving leadership and decision-making) and improving their coordination with specialists and hospitals;
- -
- Empower primary care professionals with more self-management, training, and opportunities;
- -
- Reduce paperwork;
- -
- Promote and develop the values of primary healthcare [46].
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Freudenberger, H.J. Staff Burn-Out. J. Soc. Issues 1974, 30, 159–165. [Google Scholar] [CrossRef]
- Maslach, C.; Jackson, S.E. The Maslach Burnout Inventory. J. Occup. Behav. 1981, 2, 99–113. [Google Scholar] [CrossRef]
- Brigham, T.; Barden, C.; Dopp, A.L.; Hengerer, A.; Kaplan, J.; Malone, B.; Martin, C.; McHugh, M.; Nora, L.M. A Journey to Construct an All-Encompassing Conceptual Model of Factors Affecting Clinician Well-Being and Resilience. NAM Perspect. 2018, 8. Available online: https://nam.edu/journey-construct-encompassing-conceptual-model-factors-affecting-clinician-well-resilience/ (accessed on 2 March 2021). [CrossRef] [Green Version]
- Maslach, C.; Jackson, S.E. Maslach Burnout Inventory—ES Form. PsycTESTS. 1981. Available online: http://0-search-ebscohost-com.brum.beds.ac.uk/login.aspx?direct=true&db=pst&AN=9999-05190-000&site=ehost-live%5Cn (accessed on 2 March 2021).
- Rotenstein, L.S.; Torre, M.; Ramos, M.A.; Rosales, R.C.; Guille, C.; Sen, S.; Mata, D.A. Prevalence of burnout among physicians a systematic review. JAMA J. Am. Med. Assoc. 2018, 320, 1131–1150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manzano-García, G.; Ayala-Calvo, J.C. New perspectives: Towards an integration of the concept “burnout” and its explanatory models. An. Psicol. 2013, 29, 800–809. Available online: https://www.redalyc.org/articulo.oa?id=16728244019 (accessed on 28 July 2021).
- Soler, J.K.; Yaman, H.; Esteva, M.; Dobbs, F.; Asenova, R.S.; Katić, M.; Ožvačić, Z.; Desgranges, J.P.; Moreau, A.; Lionis, C.; et al. Burnout in European family doctors: The EGPRN study. Fam. Pract. 2008, 25, 245–265. [Google Scholar] [CrossRef]
- Blechter, B.; Jiang, N.; Cleland, C.; Berry, C.; Ogedegbe, O.; Shelley, D. Correlates of burnout in small independent primary care practices in an urban setting. J. Am. Board Fam. Med. 2018, 31, 529–536. Available online: http://www.jabfm.org (accessed on 2 March 2021). [CrossRef]
- Párraga Martínez, I.; González Hidalgo, E.; Méndez García, T.; Villarín Castro, A.; León Martín, A.A. Burnout y su relación con el estrés percibido y la satisfacción laboral en profesionales sanitarios de Atención Primaria de una Comunidad Autónoma. Rev. Clínica Med. Fam. 2018, 11, 51–60. Available online: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1699-695X2018000200051 (accessed on 2 March 2021).
- Zubatsky, M.; Pettinelli, D.; Salas, J.; Davis, D. Associations between integrated care practice and burnout factors of primary care physicians. Fam. Med. 2018, 50, 770–774. Available online: https://journals.stfm.org/familymedicine/2018/november-december/zubatsky-2018-0158/?fbclid=IwAR1idAUllu74spLTG5fIkfmlbstYMDEnewPMwbe62qDNmsRmyA03U63rZL0 (accessed on 2 March 2021). [CrossRef] [PubMed] [Green Version]
- Babbott, S.; Manwell, L.B.; Brown, R.; Montague, E.; Williams, E.; Schwartz, M.; Hess, E.; Linzer, M. Electronic medical records and physician stress in primary care: Results online the MEMO Study. J. Am. Med. Inform. Assoc. 2014, 21, e100–e106. [Google Scholar] [CrossRef] [Green Version]
- Linzer, M.; Manwell, L.B.; Williams, E.S.; Bobula, J.A.; Brown, R.L.; Varkey, A.B.; Man, B.; McMurray, J.E.; Maguire, A.; Horner-Ibler, B.; et al. Working conditions in primary care: Physician reactions and care quality. Ann. Intern. Med. 2009, 151, 28–36. [Google Scholar] [CrossRef]
- Rabatin, J.; Williams, E.; Baier Manwell, L.; Schwartz, M.D.; Brown, R.L.; Linzer, M. Predictors and Outcomes of Burnout in Primary Care Physicians. J. Prim. Care Community Health 2016, 7, 41–43. Available online: https://pubmed.ncbi.nlm.nih.gov/26416697/ (accessed on 26 February 2021). [CrossRef] [Green Version]
- Helfrich, C.D.; Dolan, E.D.; Simonetti, J.; Reid, R.J.; Joos, S.; Wakefield, B.J.; Schectman, G.; Stark, R.; Fihn, S.D.; Harvey, H.B.; et al. Elements of team-based care in a patient-centered medical home are associated with lower burnout among VA primary care employees. J. Gen. Intern. Med. 2014, 29, 659–666. [Google Scholar] [CrossRef]
- Barello, S.; Palamenghi, L.; Graffigna, G. Burnout and somatic symptoms among frontline healthcare professionals at the peak of the Italian COVID-19 pandemic. Psychiatry Res. 2020, 290, 113129. Available online: https://pmc/articles/PMC7255285/ (accessed on 28 July 2021). [CrossRef]
- Luceño-Moreno, L.; Talavera-Velasco, B.; García-Albuerne, Y.; Martín-García, J. Symptoms of posttraumatic stress, anxiety, depression, levels of resilience and burnout in spanish health personnel during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2020, 17, 5514. [Google Scholar] [CrossRef] [PubMed]
- Maslach, C.; Jackson, S.E.; Leiter, M. The Maslach Burnout Inventory Manual; The Scarecrow Press: Lanham, MD, USA, 1981; Available online: https://www.researchgate.net/publication/277816643 (accessed on 11 February 2021).
- Estudi Demogràfic dels Metges del COMB Importància dels Metges Estrangers; Col·legi de Metges de Barcelona: Barcelona, Spain, 2019.
- Atención Primaria 2025. Available online: https://www.cgcom.es/sites/default/files/atencion_primaria_2025/69/ (accessed on 28 July 2021).
- Brown, P.A.; Slater, M.; Lofters, A. Personality and burnout among primary care physicians: An international study. Psychol. Res. Behav. Manag. 2019, 12, 169–177. Available online: https://pmc/articles/PMC6430002/ (accessed on 2 March 2021). [CrossRef] [PubMed] [Green Version]
- Denning, M.; Goh, E.T.; Tan, B.; Kanneganti, A.; Almonte, M.; Scott, A.; Martin, G.; Clarke, J.; Sounderajah, V.; Markar, S.; et al. Determinants of burnout and other aspects of psychological well-being in healthcare workers during the Covid-19 pandemic: A multinational cross-sectional study. PLoS ONE 2021, 16, e0238666. [Google Scholar] [CrossRef]
- Khasne, R.W.; Dhakulkar, B.S.; Mahajan, H.C. Burnout among Healthcare Workers during COVID-19 Pandemic in India: Results of a Questionnaire-based Survey. Indian J. Crit. Care Med. 2020, 24, 664–671. Available online: https://pubmed.ncbi.nlm.nih.gov/33024372/ (accessed on 28 July 2021). [CrossRef]
- Baptista, S.; Teixeira, A.; Castro, L.; Cunha, M.; Serrão, C.; Rodrigues, A.; Duarte, I. Physician Burnout in Primary Care during the COVID-19 Pandemic: A Cross-Sectional Study in Portugal. J. Prim. Care Community Health 2021, 12. Available online: https://pmc/articles/PMC8044566/ (accessed on 28 July 2021). [CrossRef]
- Koh, D.; Meng, K.L.; Sin, E.C.; Soo, M.K.; Qian, F.; Ng, V.; Ban, H.T.; Kok, S.W.; Wuen, M.C.; Hui, K.T.; et al. Risk perception and impact of severe acute respiratory syndrome (SARS) on work and personal lives of healthcare workers in Singapore: What can we learn? Med. Care 2005, 43, 676–682. Available online: https://pubmed.ncbi.nlm.nih.gov/15970782/ (accessed on 28 July 2021). [CrossRef]
- Jalili, M.; Niroomand, M.; Hadavand, F.; Zeinali, K.; Fotouhi, A. Burnout among healthcare professionals during COVID-19 pandemic: A cross-sectional study. Int. Arch. Occup. Environ. Health 2021, 94, 1–8. Available online: https://pubmed.ncbi.nlm.nih.gov/33864490/ (accessed on 28 July 2021). [CrossRef]
- Gosseries, O.; Demertzi, A.; Ledoux, D.; Bruno, M.A.; Vanhaudenhuyse, A.; Thibaut, A.; Laureys, S.; Schnakers, C. Burnout in healthcare workers managing chronic patients with disorders of consciousness. Brain Inj. 2012, 26, 1493–1499. Available online: https://pubmed.ncbi.nlm.nih.gov/22725684/ (accessed on 28 July 2021). [CrossRef]
- Torrente, M.; Sousa, P.A.; Sánchez-Ramos, A.; Pimentao, J.; Royuela, A.; Franco, F.; Collazo-Lorduy, A.; Menasalvas, E.; Provencio, M. To burn-out or not to burn-out: A cross-sectional study in healthcare professionals in Spain during COVID-19 pandemic. BMJ Open 2021, 11, e044945. Available online: https://0-bmjopen-bmj-com.brum.beds.ac.uk/content/11/2/e044945 (accessed on 28 July 2021). [CrossRef]
- Brewer, E.W.; Shapard, L. Employee Burnout: A Meta-Analysis of the Relationship between Age or Years of Experience. Hum. Resour. Dev. Rev. 2004, 3, 102–123. [Google Scholar] [CrossRef]
- Vela-Bueno, A.; Moreno-Jiménez, B.; Rodríguez-Muñoz, A.; Olavarrieta-Bernardino, S.; Fernández-Mendoza, J.; De la Cruz-Troca, J.J.; Bixler, E.O.; Vgontzas, A.N. Insomnia and sleep quality among primary care physicians with low and high burnout levels. J. Psychosom. Res. 2008, 64, 435–442. Available online: https://pubmed.ncbi.nlm.nih.gov/18374744/ (accessed on 28 July 2021). [CrossRef] [PubMed]
- Stewart, N.H.; Arora, V.M. The Impact of Sleep and Circadian Disorders on Physician Burnout. Chest 2019, 156, 1022–1030. [Google Scholar] [CrossRef]
- Kim, L.Y.; Rose, D.E.; Soban, L.M.; Stockdale, S.E.; Meredith, L.S.; Edwards, S.T.; Helfrich, C.D.; Rubenstein, L.V. Primary Care Tasks Associated with Provider Burnout: Findings online a Veterans Health Administration Survey. J. Gen. Intern. Med. 2018, 33, 50–56. [Google Scholar] [CrossRef]
- Edwards, S.T.; Marino, M.; Balasubramanian, B.A.; Solberg, L.I.; Valenzuela, S.; Springer, R.; Stange, K.C.; Miller, W.L.; Kottke, T.E.; Perry, C.K. Burnout among Physicians, Advanced Practice Clinicians and Staff in Smaller Primary Care Practices. J. Gen. Intern. Med. 2018, 33, 2138–2146. Available online: https://pubmed.ncbi.nlm.nih.gov/30276654/ (accessed on 2 March 2021). [CrossRef] [Green Version]
- Knox, M.; Willard-Grace, R.; Huang, B.; Grumbach, K. Maslach Burnout Inventory and a Self-Defined, Single-Item Burnout Measure Produce Different Clinician and Staff Burnout Estimates. J. Gen. Intern. Med. 2018, 33, 1344–1351. [Google Scholar] [CrossRef] [Green Version]
- García-Sierra, R.; Fernández-Castro, J.; Martínez-Zaragoza, F. Relationship between job demand and burnout in nurses: Does it depend on work engagement? J. Nurs. Manag. 2016, 24, 780–788. Available online: https://pubmed.ncbi.nlm.nih.gov/27111251/ (accessed on 26 March 2021). [CrossRef]
- Ratanawongsa, N.; Roter, D.; Beach, M.C.; Laird, S.L.; Larson, S.M.; Carson, K.A.; Cooper, L.A. Physician burnout and patient-physician communication during primary care encounters. J. Gen. Intern. Med. 2008, 23, 1581–1588. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pmc/articles/PMC2533387/ (accessed on 26 February 2021). [CrossRef] [Green Version]
- Willard-Grace, R.; Knox, M.; Huang, B.; Hammer, H.; Kivlahan, C.; Grumbach, K. Burnout and health care workforce turnover. Ann. Fam. Med. 2019, 17, 36–41. Available online: https://www.annfammed.org/content/17/1/36 (accessed on 26 February 2021). [CrossRef] [PubMed] [Green Version]
- Iglesias, F.H.; Fontán, A.C.; Camacho, J.G.; Calderón, M.S.M.; Alvarez-Dardet, C. El futuro del Sistema Nacional de Salud y su piedra angular, la atención primaria. Informe SESPAS 2012. Gac. Sanit. 2012, 26, 3–5. [Google Scholar] [CrossRef] [PubMed]
- Abraham, C.M.; Zheng, K.; Poghosyan, L. Predictors and Outcomes of Burnout among Primary Care Providers in the United States: A Systematic Review. Med. Care Res. Rev. 2020, 77, 387–401. [Google Scholar] [CrossRef]
- Reeves, D.; Pye, S.; Ashcroft, D.M.; Clegg, A.; Kontopantelis, E.; Blakeman, T.; Van Marwijk, H. The challenge of ageing populations and patient frailty: Can primary care adapt? BMJ 2018, 362, k3349. Available online: http://0-www-bmj-com.brum.beds.ac.uk/ (accessed on 26 February 2021). [CrossRef] [PubMed]
- Yarnall, A.J.; Sayer, A.A.; Clegg, A.; Rockwood, K.; Parker, S.; Hindle, J.V. New horizons in multimorbidity in older adults. Age Ageing 2017, 46, 882–888. Available online: https://pubmed.ncbi.nlm.nih.gov/28985248/ (accessed on 26 February 2021). [CrossRef] [Green Version]
- Albrecht, S.; Breidahl, E.; Marty, A. Organizational resources, organizational engagement climate, and employee engagement. Career Dev. Int. 2018, 23, 67–85. [Google Scholar] [CrossRef]
- Aronsson, G.; Theorell, T.; Grape, T.; Hammarström, A.; Hogstedt, C.; Marteinsdottir, I.; Skoog, I.; Träskman-Bendz, L.; Hall, C.A. Systematic review including meta-analysis of work environment and burnout symptoms. BMC Public Health 2017, 17, 264. [Google Scholar] [CrossRef] [Green Version]
- García-Sierra, R.M.; Perich, E.B.; Dominguez, J.M.M.; Millan, N.M.; Cintas, V.S.; Romero Martínez, M.; Gabriel, E.M.; Pera, G.; Gombau, G.S.; Jordana, N.M.; et al. Estudio descriptivo de los trabajadores de servicios sanitarios de una dirección de atención primaria confinados por Covid-19 [Descriptive study of the health service workers of a Primary Care Department confined by Covid-19.]. Rev. Esp. Salud. Publica 2020, 94, e202009106. [Google Scholar]
- Fòrum Català d’Atenció Primària.FoCAP. Accions per Abordar el Malestar dels Professionals de l’Atenció Primària de Salut. Barcelona. 2019. Available online: https://focap.files.wordpress.com/2019/07/accions-per-abordar-el-malestar-professional.pdf (accessed on 17 August 2021).
- Decàleg per a la Reforma del Sistema de Salut de Catalunya. Deu Propostes de Canvi a Partir de les Lliçons Apreses Durant la Crisi Sanitària de la COVID-19. 2020. Available online: https://www.comb.cat/Upload/Documents/8/8/8873.PDF (accessed on 17 August 2021).
- Sánchez-Amat, M.; Bernáldez, J.P.; Moral, E.G. Qué es la Atención Primaria de Salud? AMF 2021, 17, 76–84. [Google Scholar]


{kind=link}
| Variable | Obs. | Mean (%) | Std. Dev. | Min | Max |
|---|---|---|---|---|---|
| Socio-demographic factors | |||||
| Age | 39 | 47.44 | 8.00 | 32 | 63 |
| Gender | |||||
| Female | 31 | 79.49 | |||
| Male | 8 | 20.51 | |||
| Graduation year | 39 | 1993 | 8.40 | 1977 | 2012 |
| Seniority | 38 | 12.42 | 7.04 | 1 | 29 |
| Have children | |||||
| No | 6 | 15 | |||
| Yes | 34 | 85 | |||
| Do you practice sport? | |||||
| No | 8 | 20 | |||
| Sometimes | 8 | 20 | |||
| Yes | 24 | 60 | |||
| Do you sleep well? | |||||
| No | 11 | 27.5 | |||
| Sometimes | 6 | 15 | |||
| Yes | 23 | 57.5 | |||
| Work-related factors | |||||
| Work location | |||||
| Urban | 18 | 47.37 | |||
| Semirural | 20 | 52.63 | |||
| Are they teaching? | |||||
| No | 35 | 89.74 | |||
| Yes | 4 | 10.26 | |||
| Being on duty | |||||
| No, almost never | 12 | 30 | |||
| Sometimes | 10 | 25 | |||
| Regularly | 18 | 45 | |||
| Relocation during pandemic | |||||
| No | 4 | 10 | |||
| Yes | 36 | 90 | |||
| How many doctors have taken leave of absence in your centre? | |||||
| 0 | 11 | 27.5 | |||
| 1 | 10 | 25 | |||
| 2 | 11 | 27.5 | |||
| 3 | 5 | 12.5 | |||
| 4 | 2 | 5 | |||
| 8 | 1 | 2.5 | |||
| Have you thought about changing your work place? | |||||
| No | 17 | 42.5 | |||
| Yes, in Spain | 20 | 50 | |||
| Yes, outside Spain | 3 | 7.5 | |||
| In the lasts months, have you thought about quitting the profession? | |||||
| No | 25 | 62.5 | |||
| Yes | 15 | 37.5 | |||
| MBI Scores | Mean ± SD * | % High Burnout | % with 3 Domains High | |
|---|---|---|---|---|
| Time 1 | Emotional Exhaustion | 227 ± 12.6 | 37.5% | 7.5% |
| Depersonalization | 7.9 ± 7.2 | 32.5% | ||
| Personal Accomplishment | 37.1 ± 7.2 | 27.5% | ||
| Time 2 | Emotional Exhaustion | 26.4 ± 122 | 55.0% | 10% |
| Depersonalization | 7.8 ± 5.1 | 30.0% | ||
| Personal Accomplishment | 36.8 ± 6.3 | 27.5% | ||
| Time 3 | Emotional Exhaustion | 35 ± 13.2 | 77.5% | 50% |
| Depersonalization | 13.2 ± 6.5 | 70.0% | ||
| Personal Accomplishment | 30.4 ± 7.3 | 67.5% |
| T1 | T2 | T3 | T2 vs. T3 | T1 vs. T2 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Median (IQR) | Median (IQR) | Median (IQR) | z Value | p Value | No. (%) | X2 | z Value | p Value | No. (%) | X2 | |
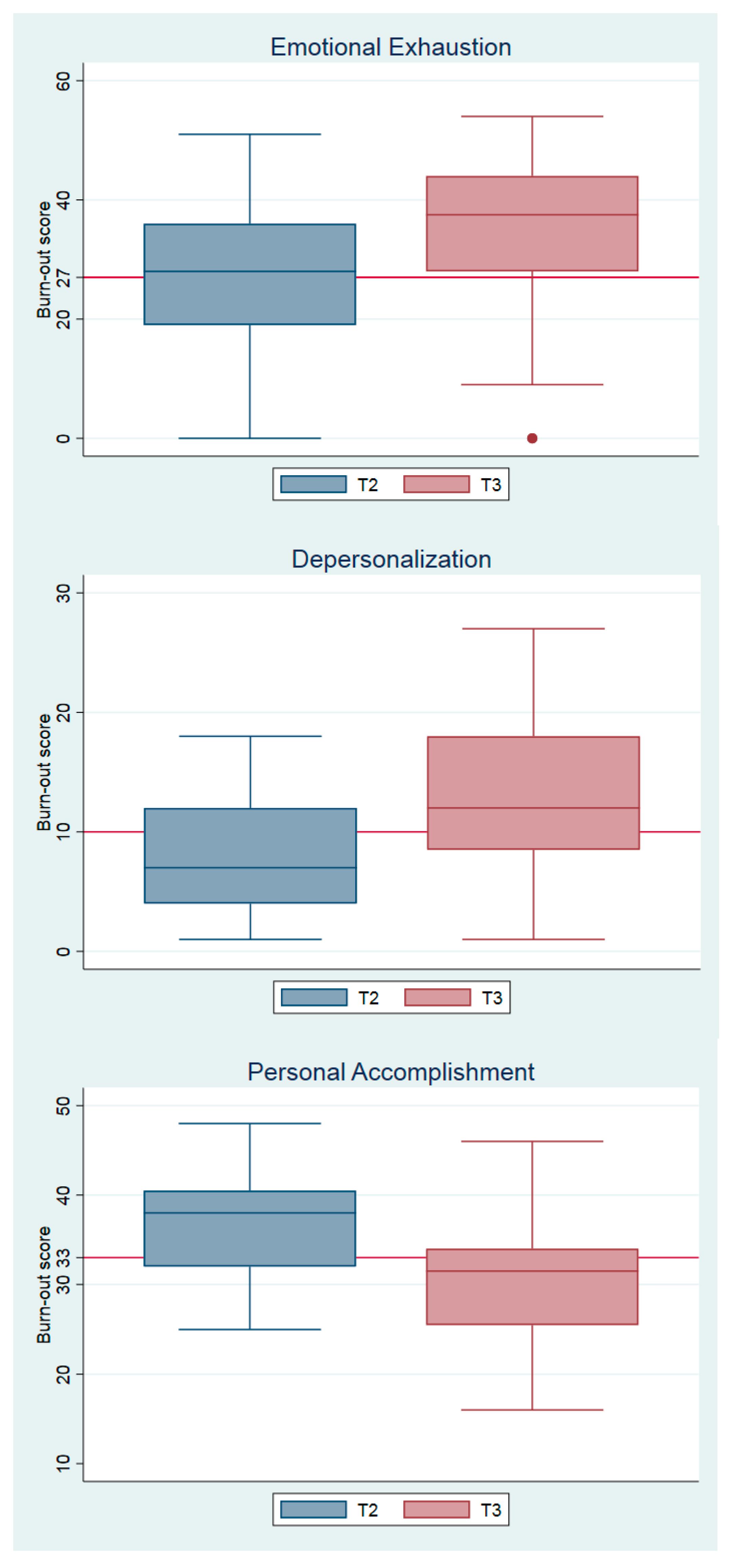
| Emotional Exhaustion | 23 (19) | 28 (17) | 37.5 (16) | 3.87 | 0.00 | 9 (40) | 0.00 | 1.81 | 0.06 | 7 (46) | 0.07 |
| Depersonalization | 5.5 (9) | 7 (8) | 38 (8.5) | 4.29 | 0.00 | 16 (133) | 0.00 | −0.26 | 0.79 | −1 (7) | 0.73 |
| Personal Accomplishment | 38 (9) | 38 (7.7) | 31.5 (8.5) | 4.40 | 0.00 | 16 (145) | 0.00 | 0.22 | 0.82 | 0 | 1.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seda-Gombau, G.; Montero-Alía, J.J.; Moreno-Gabriel, E.; Torán-Monserrat, P. Impact of the COVID-19 Pandemic on Burnout in Primary Care Physicians in Catalonia. Int. J. Environ. Res. Public Health 2021, 18, 9031. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179031
Seda-Gombau G, Montero-Alía JJ, Moreno-Gabriel E, Torán-Monserrat P. Impact of the COVID-19 Pandemic on Burnout in Primary Care Physicians in Catalonia. International Journal of Environmental Research and Public Health. 2021; 18(17):9031. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179031
Chicago/Turabian StyleSeda-Gombau, Gemma, Juan José Montero-Alía, Eduard Moreno-Gabriel, and Pere Torán-Monserrat. 2021. "Impact of the COVID-19 Pandemic on Burnout in Primary Care Physicians in Catalonia" International Journal of Environmental Research and Public Health 18, no. 17: 9031. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179031