
Using Realist Evaluation to Understand Process Outcomes in a COVID-19-Impacted Yoga Intervention Trial: A Worked Example


Abstract
:1. Introduction
1.1. Realist Evaluation

| Term | Description |
|---|---|
| Intervention activities | Intervention activities offer resources (services, ideas, information, opportunities, constraints) with intended usages, but the manner in which people respond to these resources varies, depending on context. Thus an intervention itself does not work; rather, the recipients make it work depending on how they perceive and act in response to the resources it provides [29]. |
| Context | Context is conceptualised as any condition that existed prior to the intervention [30]. This includes aspects of the local or wider environment (physical, economic, cultural) but also any relevant characteristics and circumstances of the people taking part in the intervention. Realists assume that interventions take place within complex, open social systems [6]. |
| Mechanism | Program mechanisms are intangible forces usually comprising changes in participants’ cognitive or affective reasoning (conscious or unconscious), attitudes and choice-making or in their capacities (e.g. new skills, ideas, information, perspectives, or sources of support) [31]. Mechanisms are causal tendencies which are activated by intervention strategies, provided contextual factors are conducive [6]. |
| Outcomes | Realist evaluation investigates how intervention activities produce outcomes [6]: intended and unintended. In a process evaluation, the focus is on process outcomes: proximal impacts which influence intervention outcomes. Desired process outcomes are those considered to be prerequisites for a successful intervention [32]. |
| CMO and ICMO configurations | Realist evaluation links the elements described above in Context-Mechanism-Outcome configurations so that the causal connections between them are evident. Some program evaluators add intervention activities to this causal chain, resulting in Intervention activities-Context-Mechanisms-Outcome configurations (ICMOs) [8,33,34]. |
1.2. The Intervention: Successful AGEing (SAGE) Yoga Trial
2. Materials and Methods
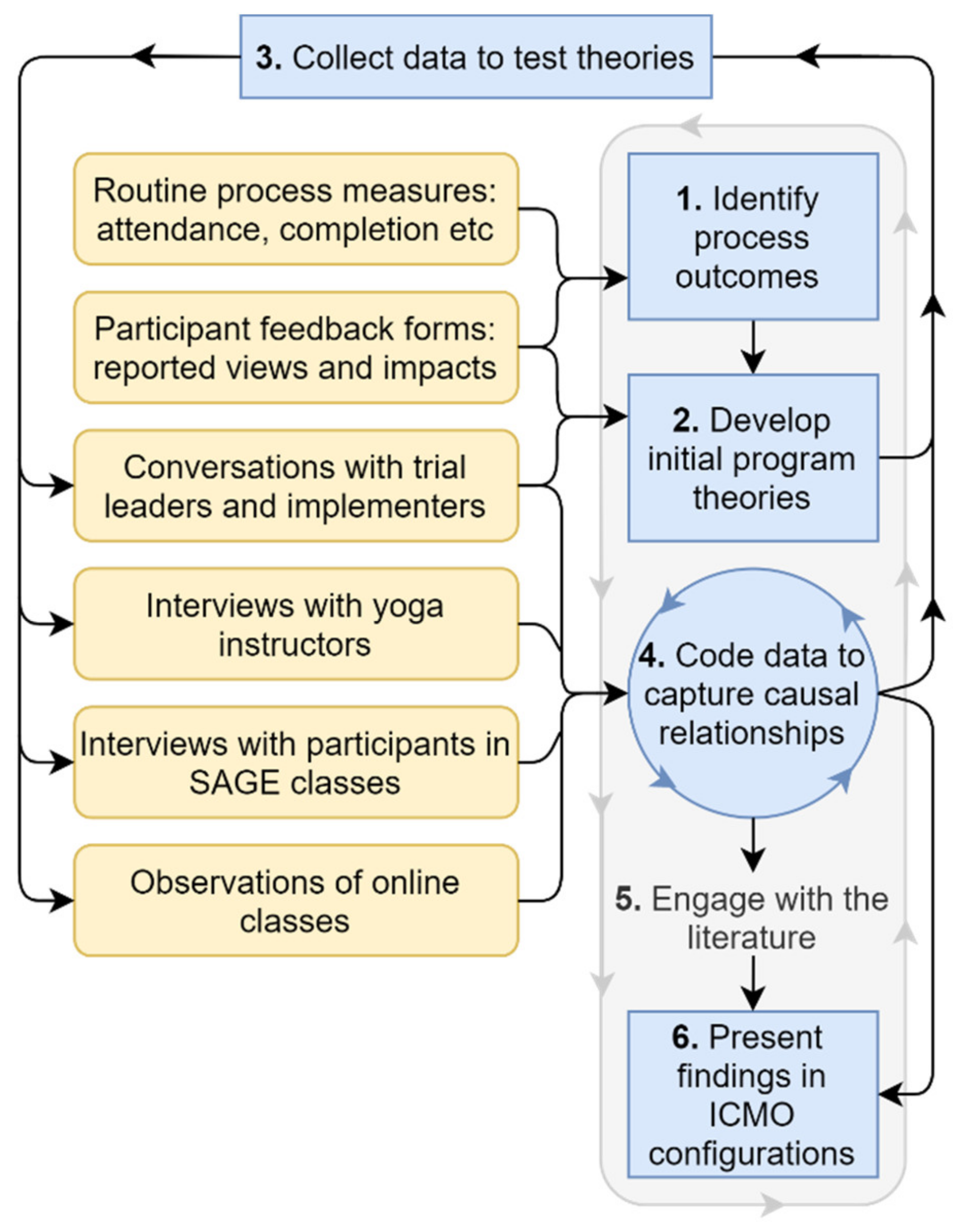
2.1. Study Design
- Identify outcomes of interest
- Develop initial program theories
- Collect data to test these theories
- Code data to capture causal relationships
- Engage with the literature
- Present findings in ICMO configurations
2.1.1. Task 1. Identify Outcomes of Interest
- Engagement with yoga program: attendance (including across transition to online classes), expressed commitment, motivation, and enjoyment.
- Self-reported health impacts: self-reported improved balance, flexibility, strength, mobility, stress reduction, sleep quality, sense of wellbeing, sense of achievement.
- Intention to continue yoga (or balance and strength-based physical activity).
2.1.2. Task 2. Develop Initial Program Theories
- Discussion with the SAGE trial leaders and implementers about the underlying causal hypotheses that had informed the intervention design. These hypotheses derived from their research and professional expertise in the field of fall prevention, physical activity, and behaviour change, but had also evolved in response to information generated by the unfolding trial, including formal, and informal participant feedback and discussions with the yoga instructors.
- The literature on falls and older people’s engagement in yoga and yoga-based exercise, and physical activity more broadly. This provided ideas about possible program theories including likely mechanisms.
2.1.3. Task 3. Collect Data to Test These Theories
Recruitment
Data Collection
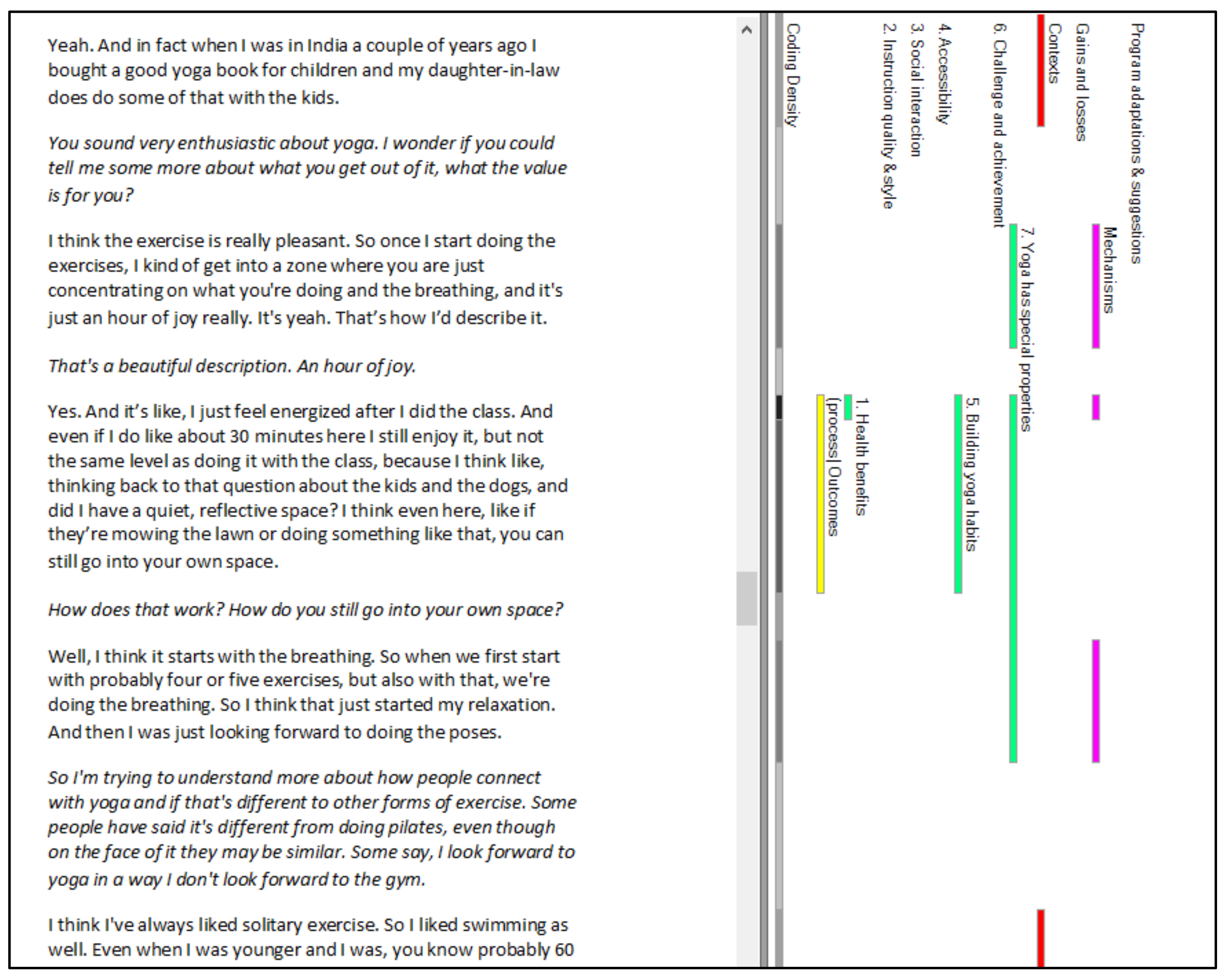
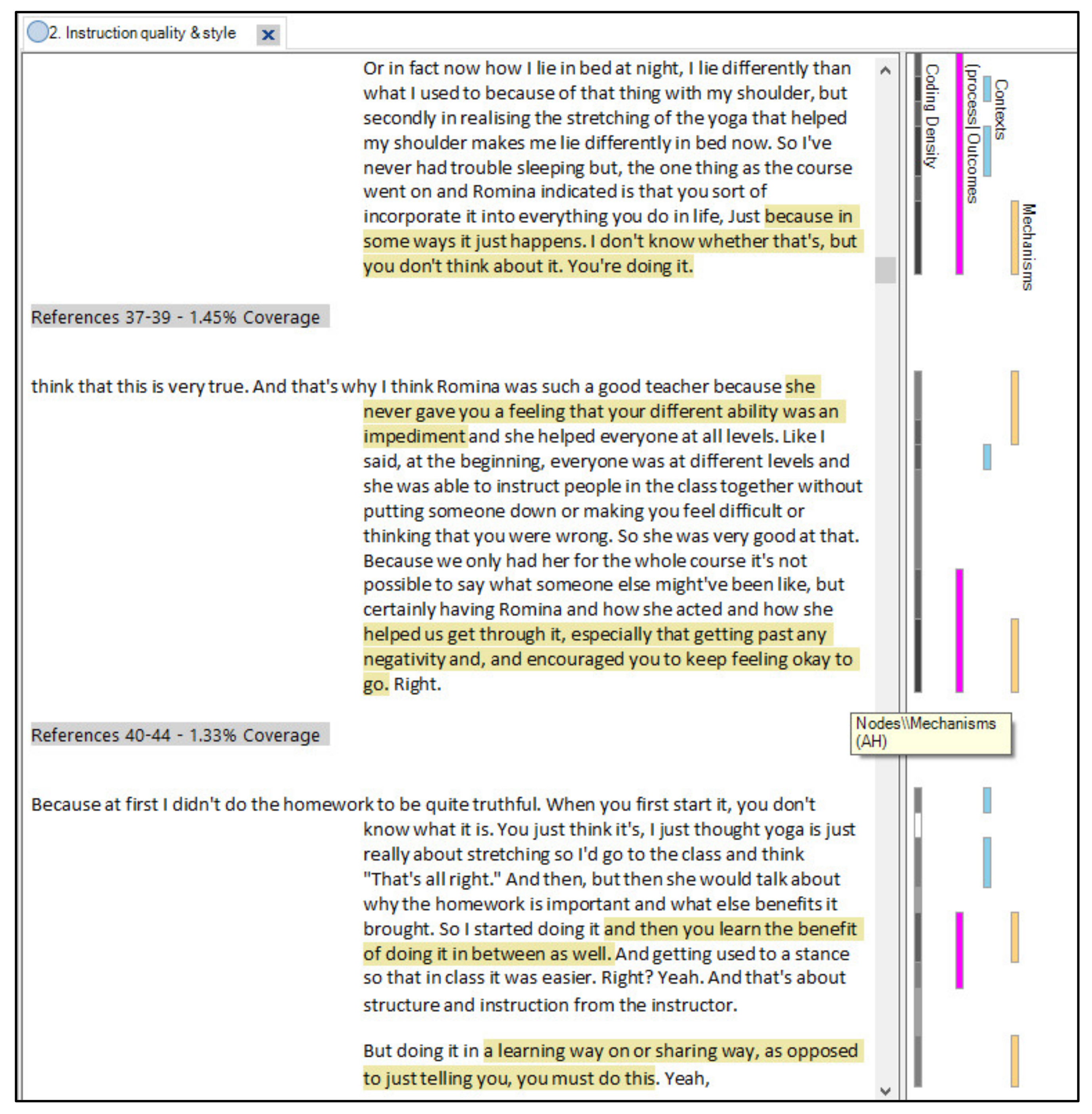
2.1.4. Task 4. Code Data to Capture Causal Relationships
“any description of perceptions, beliefs, ‘logic in use’, emotional responses to situations, or understanding of a role that is relevant to the intervention may provide a clue”([8] p. 156).
2.1.5. Task 5. Engage with the Literature
2.1.6. Task 6. Present Findings in ICMO Configurations
“…at a middle level of abstraction: specific enough to clearly explain the phenomenon, and general enough to apply across cases of the same type”([86] p. 3).
2.2. Research Rigour
2.3. Ethical Approvals and Consent
3. Results
4. Discussion
4.1. Coding That Captures Relationships between Different Elements of the Program Theory
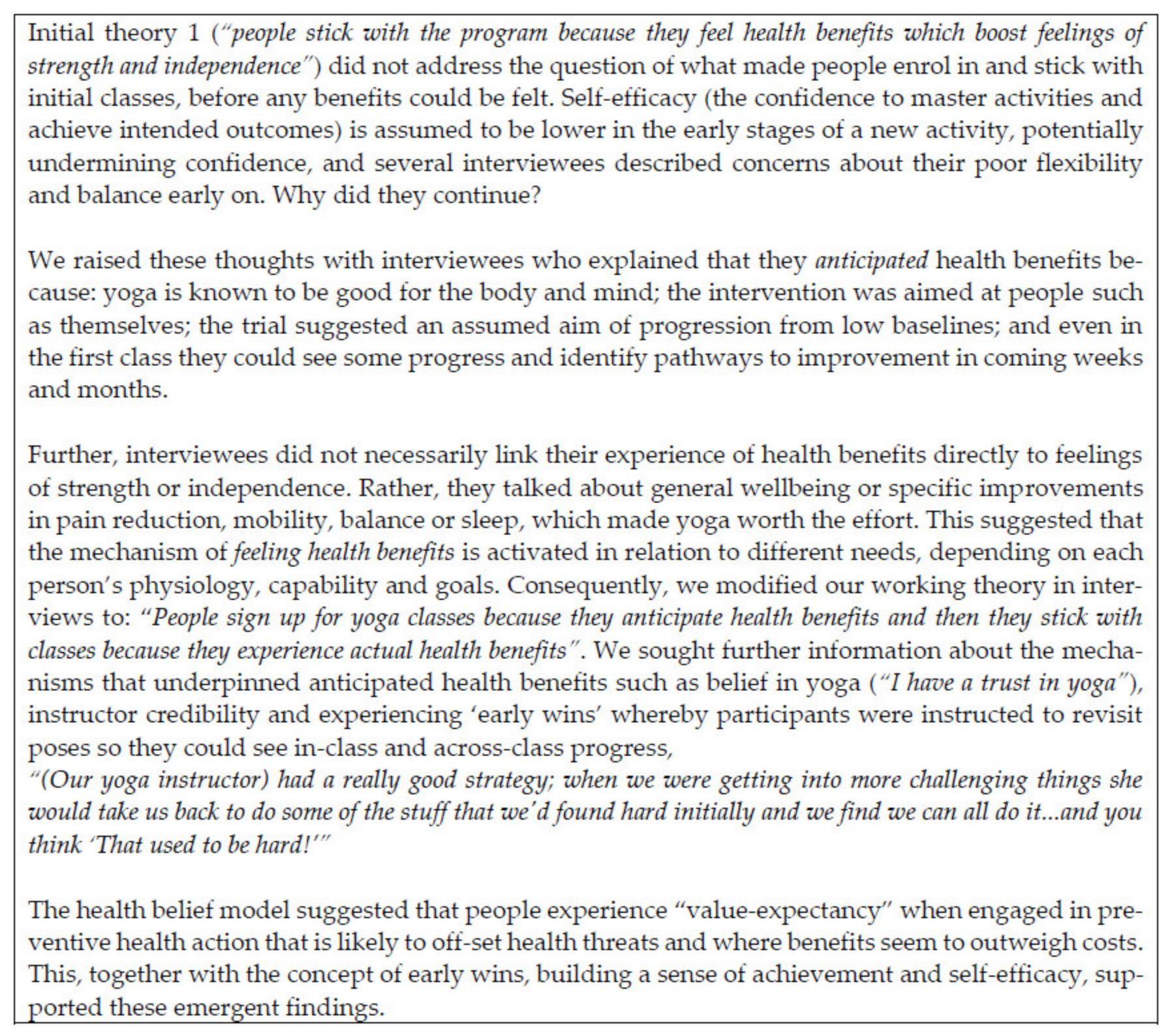
4.2. Integrating Theory into the Ongoing Analysis
“involves constant shuttling between theory and empirical data, using both inductive and deductive reasoning”([88] p. 374).
4.3. Identifying Clear Process Outcomes
“this is consistent with realist philosophy in which the same thing can be context, mechanism or outcome depending on the particular analysis being undertaken”([91] p. 378).
4.4. Presenting Findings Accessibly
“the end result will be partial knowledge about partial improvements we can make in the delivery and targeting of social interventions – quite an achievement”([5] p. 112).
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fletcher, A.; Jamal, F.; Moore, G.; Evans, R.E.; Murphy, S.; Bonell, C. Realist complex intervention science: Applying realist principles across all phases of the Medical Research Council framework for developing and evaluating complex interventions. Evaluation 2016, 22, 286–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, G.; Westhorp, G.; Manzano, A.; Greenhalgh, J.; Jagosh, J.; Greenhalgh, T. RAMESES II reporting standards for realist evaluations. BMC Med. 2016, 14, 1–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nurjono, M.; Shrestha, P.; Lee, A.; Lim, X.Y.; Shiraz, F.; Tan, S.; Wong, S.H.; Foo, K.M.; Wee, T.; Toh, S.-A.; et al. Realist evaluation of a complex integrated care programme: Protocol for a mixed methods study. BMJ Open 2018, 8, e017111. [Google Scholar] [CrossRef] [Green Version]
- Punton, M.; Isabel, V.; Leavy, J.; Michaelis, C.; Boydell, E. Reality Bites: Making Realist Evaluation Useful in the Real World (CDI Practice Paper); Centre for Development Impact: Ringmer, UK, 2020. [Google Scholar]
- Pawson, R. The Science of Evaluation: A Realist Manifesto; Sage: Los Angeles, CA, USA, 2013. [Google Scholar]
- Pawson, R.; Tilley, N. Realist Evaluation; Community Matters: Mount Torrens, South Australia, Australia, 2004. [Google Scholar]
- Westhorp, G. Realist Impact Evaluation: An Introduction; Overseas Development Institute: London, UK, 2014; pp. 1–12. [Google Scholar]
- Westhorp, G. Development of Realist Evaluation Models and Methods for Use in Small-Scale Community Based Settings. Ph.D. Thesis, Nottingham Trent University, Nottingham, UK, 2008. [Google Scholar]
- Bygstad, B.; Munkvold, B.E.; Volkoff, O. Identifying Generative Mechanisms through Affordances: A Framework for Critical Realist Data Analysis. J. Inform. Technol. 2016, 31, 83–96. [Google Scholar] [CrossRef]
- Davidoff, F.; Dixon-Woods, M.; Leviton, L.; Michie, S. Demystifying theory and its use in improvement. BMJ Qual. Saf. 2015, 24, 228–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, G.F.; Audrey, S.; Barker, M.; Bond, L.; Bonell, C.; Hardeman, W.; Moore, L.; O’Cathain, A.; Tinati, T.; Wight, D.; et al. Process evaluation of complex interventions: Medical Research Council guidance. BMJ 2015. [Google Scholar] [CrossRef] [Green Version]
- Henry, G.T. Realist Evaluation. In Encyclopedia of Evaluation; Mathison, S., Ed.; SAGE: Thousand Oaks, CA, USA, 2005; pp. 360–362. [Google Scholar]
- Westhorp, G.; Prins, E.; Kusters, C.; Hultink, M.; Guijt, I.; Brouwers, J. Realist Evaluation: An overview. In Report from an Expert Seminar with Dr Gill Westhorp; Wageningen University Research Centre for Development Innovation in Collaboration with Learning by Design and Context, International Cooperation: Wageningen, The Netherlands, 2011. [Google Scholar]
- O’Cathain, A.; Nicholl, J.; Murphy, E. Structural issues affecting mixed methods studies in health research: A qualitative study. BMC Med. Res. Methodol. 2009, 9, 82. [Google Scholar] [CrossRef] [Green Version]
- Richards, D.A.; Bazeley, P.; Borglin, G.; Craig, P.; Emsley, R.; Frost, J.; Hill, J.; Horwood, J.; Hutchings, H.A.; Jinks, C.; et al. Integrating quantitative and qualitative data and findings when undertaking randomised controlled trials. BMJ Open 2019, 9, e032081. [Google Scholar] [CrossRef] [Green Version]
- Drabble, S.J.; O’Cathain, A.; Thomas, K.J.; Rudolph, A.; Hewison, J. Describing qualitative research undertaken with randomised controlled trials in grant proposals: A documentary analysis. BMC Med. Res. Methodol. 2014, 14, 24. [Google Scholar] [CrossRef] [Green Version]
- O’Cathain, A.; Goode, J.; Drabble, S.J.; Thomas, K.J.; Rudolph, A.; Hewison, J. Getting added value from using qualitative research with randomized controlled trials: A qualitative interview study. Trials 2014, 15, 215. [Google Scholar] [CrossRef] [Green Version]
- Wells, M.; Williams, B.; Treweek, S.; Coyle, J.; Taylor, J. Intervention description is not enough: Evidence from an in-depth multiple case study on the untold role and impact of context in randomised controlled trials of seven complex interventions. Trials 2012, 13, 95–111. [Google Scholar] [CrossRef] [Green Version]
- RAMESES Projects. The RAMESES Projects UK: National Institute of Health Research, UK. Available online: https://www.ramesesproject.org/ (accessed on 4 May 2021).
- Manzano, A. The craft of interviewing in realist evaluation. Evaluation 2016, 22, 342–360. [Google Scholar] [CrossRef] [Green Version]
- RAMESES II Project. Quality Standards for Realist Evaluation. For Evaluators and Peer-Reviewers. 2017. Available online: https://www.ramesesproject.org/media/RE_Quality_Standards_for_evaluators_and_peer_reviewers.pdf (accessed on 19 December 2020).
- Maxwell, J.; Chmiel, M. Notes towards a theory of qualitative data analysis. In The SAGE Handbook of Qualitative Data Analysis; SAGE Publications: London, UK, 2014; pp. 21–34. [Google Scholar]
- Maxwell, J.A. A Realist Approach for Qualitative Research; Sage: Thousand Oaks, CA, USA, 2012. [Google Scholar]
- Wynn, J.D.; Williams, C.K. Principles for conducting critical realist case study research in information systems. MIS Q. 2012, 36, 787–810. [Google Scholar] [CrossRef] [Green Version]
- Sobh, R.; Perry, C. Research design and data analysis in realism research. Eur. J. Mark. 2006, 40, 1194–1209. [Google Scholar] [CrossRef]
- Gilmore, B.; McAuliffe, E.; Power, J.; Vallières, F. Data analysis and synthesis within a realist evaluation: Toward more transparent methodological approaches. Int. J. Qual. Method. 2019, 18. [Google Scholar] [CrossRef] [Green Version]
- Bergeron, D.A.; Gaboury, I. Challenges related to the analytical process in realist evaluation and latest developments on the use of NVivo from a realist perspective. Int. J. Soc. Res. Methodol. 2020, 23, 355–365. [Google Scholar] [CrossRef]
- Dalkin, S.; Forster, N.; Hodgson, P.; Lhussier, M.; Carr, S.M. Using computer assisted qualitative data analysis software (CAQDAS.; NVivo) to assist in the complex process of realist theory generation, refinement and testing. Int. J. Soc. Res. Methodol. 2020, 24, 123–134. [Google Scholar] [CrossRef]
- Coorey, G.; Peiris, D.; Neubeck, L.; Redfern, J. A realist evaluation approach to explaining the role of context in the impact of a complex eHealth intervention for improving prevention of cardiovascular disease. BMC Health Serv. Res. 2020, 20, 764. [Google Scholar] [CrossRef] [PubMed]
- Jackson, S.F.; Kolla, G. A New Realistic Evaluation Analysis Method: Linked Coding of Context, Mechanism, and Outcome Relationships. Am. J. Eval. 2012, 33, 339–349. [Google Scholar] [CrossRef]
- Shaw, J.; Gray, C.S.; Baker, G.R.; Denis, J.-L.; Breton, M.; Gutberg, J.; Embuldeniya, G.; Carswell, P.; Dunham, A.; McKillop, A.; et al. Mechanisms, contexts and points of contention: Operationalizing realist-informed research for complex health interventions. BMC Med. Res. Methodol. 2018, 18, 178. [Google Scholar] [CrossRef] [Green Version]
- Haynes, A.; Brennan, S.; Redman, S.; Williamson, A.; Makkar, S.R.; Gallego, G.; Butow, P. Policymakers’ experience of a capacity-building intervention designed to increase their use of research: A realist process evaluation. Health Res. Policy Syst. 2017, 15, 99. [Google Scholar] [CrossRef]
- Punton, M.; Vogel, I.; Lloyd, R. Reflections from a Realist Evaluation in Progress: Scaling Ladders and Stitching Theory; Institute of Development Studies: Brighton, UK, 2016. [Google Scholar]
- De Weger, E.; Van Vooren, N.J.E.; Wong, G.; Dalkin, S.; Marchal, B.; Drewes, H.W.; Baan, C.A. What’s in a Realist Configuration? Deciding Which Causal Configurations to Use, How, and Why. Int. J. Qual. Methods 2020, 19. [Google Scholar] [CrossRef]
- Oakley, A.; Strange, V.; Bonell, C.; Allen, E.; Stephenson, J.; Team, R.S. Process evaluation in randomised controlled trials of complex interventions. BMJ 2006, 332, 413–416. [Google Scholar] [CrossRef] [Green Version]
- Gardner, B.; Rebar, A.L. Habit Formation and Behavior Change. In Oxford Research Encyclopedia of Psychology; Oxford University Press: Oxford, UK, 2019. [Google Scholar]
- Kaushal, N.; Rhodes, R.E.; Spence, J.C.; Meldrum, J.T. Increasing Physical Activity Through Principles of Habit Formation in New Gym Members: A Randomized Controlled Trial. Ann. Behav. Med. 2017, 51, 578–586. [Google Scholar] [CrossRef] [PubMed]
- Cornish, K.; Fox, G.; Fyfe, T.; Koopmans, E.; Pousette, A.; Pelletier, C.A. Understanding physical literacy in the context of health: A rapid scoping review. BMC Public Health 2020, 20, 1569. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Sum, K.-W.R.; Yang, Y.-J.; Chun-Yiu Yeung, N. Measurements of Older Adults’ Physical Competence under the Concept of Physical Literacy: A Scoping Review. Int. J. Environ. Res. Public Health 2020, 17, 6570. [Google Scholar] [CrossRef]
- Keegan, R.; Barnett, L.; Dudley, D. Physical Literacy: Informing a Definition and Standard for Australia; Australian Sports Commission: Canberra, Australia, 2017.
- Ryan, R.; Deci, E. Self-Determination Theory: Basic Psychological Needs in Motivation, Development, and Wellness; Guilford Publishing: New York, NY, USA, 2017. [Google Scholar]
- Bonura, K.B.; Tenenbaum, G. Effects of Yoga on Psychological Health in Older Adults. J. Phys. Act. Health 2014, 11, 1334. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.K.; Newstead, A.H.; Ferrer, R.L. The effects of yoga on physical functioning and health related quality of life in older adults: A systematic review and meta-analysis. J. Altern. Complement. Med. 2012, 18, 902–917. [Google Scholar] [CrossRef]
- Franco, M.R.; Tong, A.; Howard, K.; Sherrington, C.; Ferreira, P.H.; Pinto, R.Z.; Ferreira, M.L. Older people’s perspectives on participation in physical activity: A systematic review and thematic synthesis of qualitative literature. Br. J. Sports Med. 2015, 49, 1268–1276. [Google Scholar] [CrossRef] [PubMed]
- Moore, A.J.; Holden, M.A.; Foster, N.E.; Jinks, C. Therapeutic alliance facilitates adherence to physiotherapy-led exercise and physical activity for older adults with knee pain: A longitudinal qualitative study. J. Physiother. 2020, 66, 45–53. [Google Scholar] [CrossRef]
- McKay, H.; Naylor, P.-J.; Lau, E.; Gray, S.M.; Wolfenden, L.; Milat, A.; Bauman, A.; Race, D.; Nettlefold, L.; Sims-Gould, J. Implementation and scale-up of physical activity and behavioural nutrition interventions: An evaluation roadmap. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stathi, A.; McKenna, J.; Fox, K.R. Processes Associated with Participation and Adherence to a 12-month Exercise Programme for Adults Aged 70 and older. J. Health Psychol. 2010, 15, 838–847. [Google Scholar] [CrossRef] [PubMed]
- Sherrington, C.; Lord, S.R.; Finch, C.F. Physical activity interventions to prevent falls among older people: Update of the evidence. J. Sci. Med. Sport 2004, 7 (Suppl. 1), 43–51. [Google Scholar] [CrossRef]
- Perracini, M.R.; Franco, M.R.C.; Ricci, N.A.; Blake, C. Physical activity in older people-case studies of how to make change happen. Best Pract. Res. Clin. Rheumatol. 2017, 31, 260–274. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fisher, K.L.; Reeder, B.A.; Harrison, E.L.; Bruner, B.G.; Ashworth, N.L.; Pahwa, P.; Sari, N.; Sheppard, M.S.; Shields, C.A.; Chad, K.E. Comparing Class-Based and Home-Based Exercise for Older Adults with Chronic Health Conditions: 12-Month Follow-Up of a Randomized Clinical Trial. J. Aging Phys. Act. 2018, 26, 471–485. [Google Scholar] [CrossRef] [PubMed]
- Graupensperger, S.; Gottschall, J.S.; Benson, A.J.; Eys, M.; Hastings, B.; Evans, M.B. Perceptions of groupness during fitness classes positively predict recalled perceptions of exertion, enjoyment, and affective valence: An intensive longitudinal investigation. Sport Exerc. Perform. Psychol. 2019, 8, 290–304. [Google Scholar] [CrossRef]
- Stathi, A.; Fox, K.R.; McKenna, J. Physical activity and dimensions of subjective well-being in older adults. J. Aging Phys. Act. 2002, 10, 76–92. [Google Scholar] [CrossRef]
- Deci, E.; Ryan, R. Self-determination theory. In Handbook of Theories of Social Psychology; Van Lange, P., Krugkanski, A., Higgens, T., Eds.; SAGE: London, UK, 2012; pp. 416–437. [Google Scholar]
- Rice, E.L.; Adair, K.C.; Tepper, S.J.; Fredrickson, B.L. Perceived social integration predicts future physical activity through positive affect and spontaneous thoughts. Emotion 2020, 20, 1074–1083. [Google Scholar] [CrossRef] [PubMed]
- Anokye, N.K.; Pokhrel, S.; Fox-Rushby, J. Economic analysis of participation in physical activity in England: Implications for health policy. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 117. [Google Scholar] [CrossRef] [Green Version]
- Boulton, E.R.; Horne, M.; Todd, C. Multiple influences on participating in physical activity in older age: Developing a social ecological approach. Health Expect. 2017, 21, 239–248. [Google Scholar] [CrossRef] [Green Version]
- Iizuka, T.; Shigeoka, H. Is Zero a Special Price? Evidence from Child Healthcare; Simon Fraser University, Department of Economics: Burnaby, BC, Canada, 2020. [Google Scholar]
- Brennan, K.; Tello, D. Do People Value What They Receive for Free? Alliance Magazine [Internet]. 2010, Volume 15. Available online: https://www.alliancemagazine.org/opinion/do-people-value-what-they-receive-for-free (accessed on 28 June 2021).
- Hawe, P. Lessons from Complex Interventions to Improve Health. Annu. Rev. Public Health 2015, 36, 307–323. [Google Scholar] [CrossRef] [Green Version]
- Mukumbang, F.C.; Marchal, B.; Van Belle, S.; Van Wyk, B. Using the realist interview approach to maintain theoretical awareness in realist studies. Qual. Res. 2019, 20, 485–515. [Google Scholar] [CrossRef] [Green Version]
- Dalkin, S.M.; Greenhalgh, J.; Jones, D.; Cunningham, B.; Lhussier, M. What’s in a mechanism? Development of a key concept in realist evaluation. Implement. Sci. 2015, 10, 49. [Google Scholar] [CrossRef] [Green Version]
- Miles, M.B.; Huberman, A.M. Qualitative Data Analysis: An Expanded Sourcebook; Sage: London, UK, 1994. [Google Scholar]
- Gale, N.K.; Heath, G.; Cameron, E.; Rashid, S.; Redwood, S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med. Res. Methodol. 2013, 13, 117. [Google Scholar] [CrossRef] [Green Version]
- Cheyne, H.; Abhyankar, P.; McCourt, C. Empowering change: Realist evaluation of a Scottish Government programme to support normal birth. Midwifery 2013, 29, 1110–1121. [Google Scholar] [CrossRef]
- Byng, R.; Norman, I.; Redfern, S. Using Realistic Evaluation to Evaluate a Practice-level Intervention to Improve Primary Healthcare for Patients with Long-term Mental Illness. Evaluation 2005, 11, 69–93. [Google Scholar] [CrossRef]
- Willis, C.E.; Reid, S.; Elliott, C.; Rosenberg, M.; Nyquist, A.; Jahnsen, R.; Girdler, S. A realist evaluation of a physical activity participation intervention for children and youth with disabilities: What works, for whom, in what circumstances, and how? BMC Pediatr. 2018, 18, 113. [Google Scholar] [CrossRef] [PubMed]
- Williams, L.; Rycroft-Malone, J.; Burton, C.R. Implementing best practice in infection prevention and control. A realist evaluation of the role of intermediaries. Int. J. Nurs. Stud. 2016, 60, 156–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feather, J.L. Developing programme theories as part of a realist evaluation of a healthcare quality improvement programme. Int. J. Care Coord. 2018, 21, 68–72. [Google Scholar] [CrossRef]
- Salter, K.L.; Kothari, A. Using realist evaluation to open the black box of knowledge translation: A state-of-the-art review. Implement. Sci. 2014, 9, 115. [Google Scholar] [CrossRef] [Green Version]
- Ntoumanis, N.; Thøgersen-Ntoumani, C.; Quested, E.; Chatzisarantis, N. Theoretical approaches to physical activity promo-tion. In Oxford Research Encyclopedia of Psychology; Braddick, O., Ed.; Oxford University Press: Oxford, UK, 2018. [Google Scholar]
- Abraham, C.; Sheeran, P. The health belief model. In Cambridge Handbook of Psychology, Health and Medicine, 2nd ed.; Ayers, S., Baum, A., McManus, C., Newman, S., Wallston, K., Weinman, J., West, R., Eds.; Cambridge University Press: Cambridge, UK, 2007; pp. 97–102. [Google Scholar]
- Rosenstock, I.M.; Strecher, V.J.; Becker, M.H. Social Learning Theory and the Health Belief Model. Health Educ. Q. 1988, 15, 175–183. [Google Scholar] [CrossRef]
- Williams, S.L.; French, D. What are the most effective intervention techniques for changing physical activity self-efficacy and physical activity behavior—And are they the same? Health Educ. Res. 2011, 26, 308–322. [Google Scholar] [CrossRef]
- Macdonald, M.; Pauly, B.; Wong, G.; Schick-Makaroff, K.; Van Roode, T.; Strosher, H.W.; Kothari, A.; Valaitis, R.; Manson, H.; O’Briain, W.; et al. Supporting successful implementation of public health interventions: Protocol for a realist synthesis. Syst. Rev. 2016, 5, 54. [Google Scholar] [CrossRef] [Green Version]
- Shankardass, K.; Renahy, E.; Muntaner, C.; O’Campo, P. Strengthening the implementation of Health in All Policies: A methodology for realist explanatory case studies. Health Policy Plan. 2014, 30, 462–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lemire, S.T.; Nielsen, S.B.; Dybdal, L. Making contribution analysis work: A practical framework for handling influencing factors and alternative explanations. Evaluation 2012, 18, 294–309. [Google Scholar] [CrossRef]
- Cox, A.E.; Tylka, T.L. A conceptual model describing mechanisms for how yoga practice may support positive embodiment. Eat. Disord. 2020, 28, 376–399. [Google Scholar] [CrossRef] [PubMed]
- Mahlo, L.; Tiggemann, M. Yoga and positive body image: A test of the Embodiment Model. Body Image 2016, 18, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Piran, N.; Neumark-Sztainer, D. Yoga and the experience of embodiment: A discussion of possible links. Eat. Disord. 2020, 28, 330–348. [Google Scholar] [CrossRef]
- Zoogman, S.; Goldberg, S.B.; Vousoura, E.; Diamond, M.C.; Miller, L. Effect of yoga-based interventions for anxiety symptoms: A meta-analysis of randomized controlled trials. Spiritual. Clin. Pract. 2019, 6, 256–278. [Google Scholar] [CrossRef]
- Gaiswinkler, L.; Unterrainer, H. The relationship between yoga involvement, mindfulness and psychological well-being. Complement. Ther. Med. 2016, 26, 123–127. [Google Scholar] [CrossRef]
- Smith, J.A.M.A.; Greer, T.P.; Sheets, T.P.; Watson, S.P. Is There More to Yoga Than Exercise? Altern. Ther. Health Med. 2011, 17, 22–29. [Google Scholar]
- Park, C.L.; Riley, K.E.; Bedesin, E.; Stewart, V.M. Why practice yoga? Practitioners’ motivations for adopting and maintaining yoga practice. J. Health Psychol. 2014, 21, 887–896. [Google Scholar] [CrossRef]
- Wheeler, M.S.; Arnkoff, D.B.; Glass, C.R. The Neuroscience of Mindfulness: How Mindfulness Alters the Brain and Facilitates Emotion Regulation. Mindfulness 2017, 8, 1471–1487. [Google Scholar] [CrossRef]
- Tang, Y.-Y.; Hölzel, B.K.; Posner, M.I. The neuroscience of mindfulness meditation. Nat. Rev. Neurosci. 2015, 16, 213–225. [Google Scholar] [CrossRef]
- RAMESES II Project. “Theory” in Realist Evaluation. 2017. Available online: https://www.ramesesproject.org/media/RAMESES_II_Theory_in_realist_evaluation.pdf (accessed on 20 December 2020).
- Ronkainen, N.J.; Wiltshire, G. Rethinking validity in qualitative sport and exercise psychology research: A realist perspective. Int. J. Sport Exerc. Psychol. 2019, 19, 13–28. [Google Scholar] [CrossRef]
- Astbury, B.; Leeuw, F.L. Unpacking Black Boxes: Mechanisms and Theory Building in Evaluation. Am. J. Eval. 2010, 31, 363–381. [Google Scholar] [CrossRef]
- Astbury, B. Some reflections on Pawson’s Science of Evaluation: A Realist Manifesto. Evaluation 2013, 19, 383–401. [Google Scholar] [CrossRef]
- Lemire, S.; Kwako, A.; Nielsen, S.B.; Christie, C.A.; Donaldson, S.I.; Leeuw, F.L. What Is This Thing Called a Mechanism? Findings From a Review of Realist Evaluations. In Causal Mechanisms in Program Evaluation New Directions for Evaluation; Schmitt, J., Ed.; Wiley: Hoboken, NJ, USA, 2020; pp. 73–86. [Google Scholar]
- Westhorp, G. Developing complexity-consistent theory in a realist investigation. Evaluation 2013, 19, 364–382. [Google Scholar] [CrossRef]
- Spiby, H.; Green, J.M.; Darwin, Z.; Willmot, H.; Knox, D.; McLeish, J.; Smith, M. Multisite implementation of trained volunteer doula support for disadvantaged childbearing women: A mixed-methods evaluation. Health Serv. Deliv. Res. 2015, 3, 1–332. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}

| Initial Program Theory | Supporting Theories from the Literature | |
|---|---|---|
| 1. | People stick with the program because they feel health benefits (e.g., improved balance and mobility) which boost feelings of strength and independence | PA generates feelings of physical and psychological wellness [41], and yoga does this particularly effectively, including for older people [42,43] |
| 2. | The perceived quality of yoga instructors is important for making people feel safe and confident. This includes instructors who understand the needs of older people | The quality of instructors affects older people’s feelings of safety and confidence in PA [44]. The concept of therapeutic alliance is key to understanding instructor/participant relationship quality [45] |
| 3. | Tailoring of the classes is crucial. People must feel they can participate according to their abilities and health needs | Tailoring of PA programs is a key motivator in adherence [46,47]. Fall prevention interventions should be tailored for targeted recipients to maximise safety and effects [48] |
| 4. | Social connections are an incentive and may add to the enjoyment of classes | Many empirical studies [47,49,50,51,52] and theories back this concept including self-determination theory [53] and the upward spiral theory of lifestyle change [54] |
| 5. | Free classes are an incentive to give yoga a go and stick with it long-term | Subsidised costs increase participation in PA [55,56]. The ‘zero price effect’ [57] increases the perceptions of value |
| Key Questions Re Validity Criteria | Tasks for Establishing Validity | Methods Used in This Study |
|---|---|---|
| How empirically adequate is the research account? | Establish descriptive validity | Transcription correction Timely note-taking re-emergent theories Multiple researchers engaged in coding and reviewing accuracy of findings against the data |
| Guard against data collection limitations | Purposive sampling for maximum coverage Multiple methods triangulation Evolving interview questions taking account of new theories and concepts | |
| How ontologically plausible is the research account? | Engage with theoretical explanations of the empirical evidence | Development of tentative initial theories Theory-checking with interviewees Continuous exploration of relevant existing theories in the literature |
| Take account of context and complexity | In-depth exploration of context from multiple perspectives: diverse participants and intervention deliverers Particular attention to COVID-19 impacts | |
| Engage with competing alternative explanations of the evidence | Critical reflexivity Workshops with “critical friends” Inviting alternative theories from interviewees Multi-researcher coding Searching for alternative theories | |
| How much practical utility does the research account have? | Findings are used to suggest practical real-world actions | Practical responses to the findings will be addressed in the main evaluation paper |
| Those practical actions are likely to have a meaningful impact | The theoretical and empirical basis of the trial (which draws on demonstrably successful intervention strategies) plus self-reported benefits from participation and the scalability of the intervention indicate likely impact |
| Program Theories | Intervention Activities What Did We Do? | Context Who Did It Work for? | Mechanisms How Did It Work? | Outcomes With What Process Effects? |
|---|---|---|---|---|
| It is worth the effort | Program of Iyengar yoga-based exercise with progressively challenging poses designed to prevent falls in older people |
|
|
|
| Impelling instruction | Experienced instructors deliver the program, individualising it for participants’ different capabilities | |||
| Other people help | Group classes with a maximum of 18 people WhatsApp forum for each group when classes moved online |
|
| |
| Putting yoga within reach | Free classes in local yoga studios... ... then online via Zoom with tech support from the SAGE team |
|
| |
| Building yoga habits | Twice-weekly classes over 12 months with:
|
|
| |
| Yoga has special properties | The SAGE program utilises core Iyengar yoga practices |
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haynes, A.; Gilchrist, H.; Oliveira, J.S.; Tiedemann, A. Using Realist Evaluation to Understand Process Outcomes in a COVID-19-Impacted Yoga Intervention Trial: A Worked Example. Int. J. Environ. Res. Public Health 2021, 18, 9065. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179065
Haynes A, Gilchrist H, Oliveira JS, Tiedemann A. Using Realist Evaluation to Understand Process Outcomes in a COVID-19-Impacted Yoga Intervention Trial: A Worked Example. International Journal of Environmental Research and Public Health. 2021; 18(17):9065. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179065
Chicago/Turabian StyleHaynes, Abby, Heidi Gilchrist, Juliana S. Oliveira, and Anne Tiedemann. 2021. "Using Realist Evaluation to Understand Process Outcomes in a COVID-19-Impacted Yoga Intervention Trial: A Worked Example" International Journal of Environmental Research and Public Health 18, no. 17: 9065. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179065