
Current Issues within the Perinatal Mental Health Care System in Aichi Prefecture, Japan: A Cross-Sectional Questionnaire Survey

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
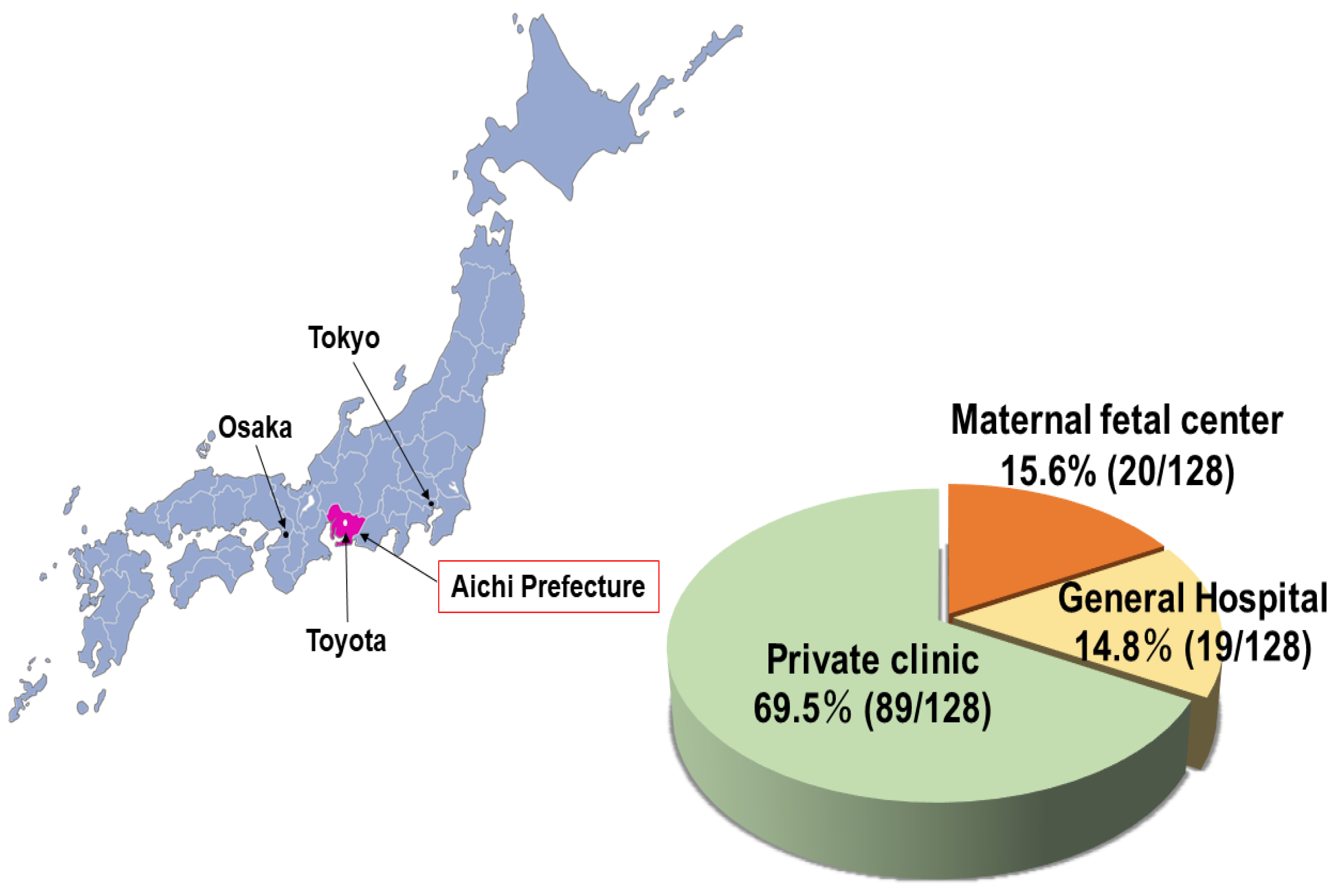
2.1. Setting
2.2. Design
2.3. Statistical Analysis
3. Results
3.1. Response Rates
3.2. Women with Worsening Mental Illness during the Perinatal Period
3.3. Multidisciplinary Perinatal Mental Health Care System
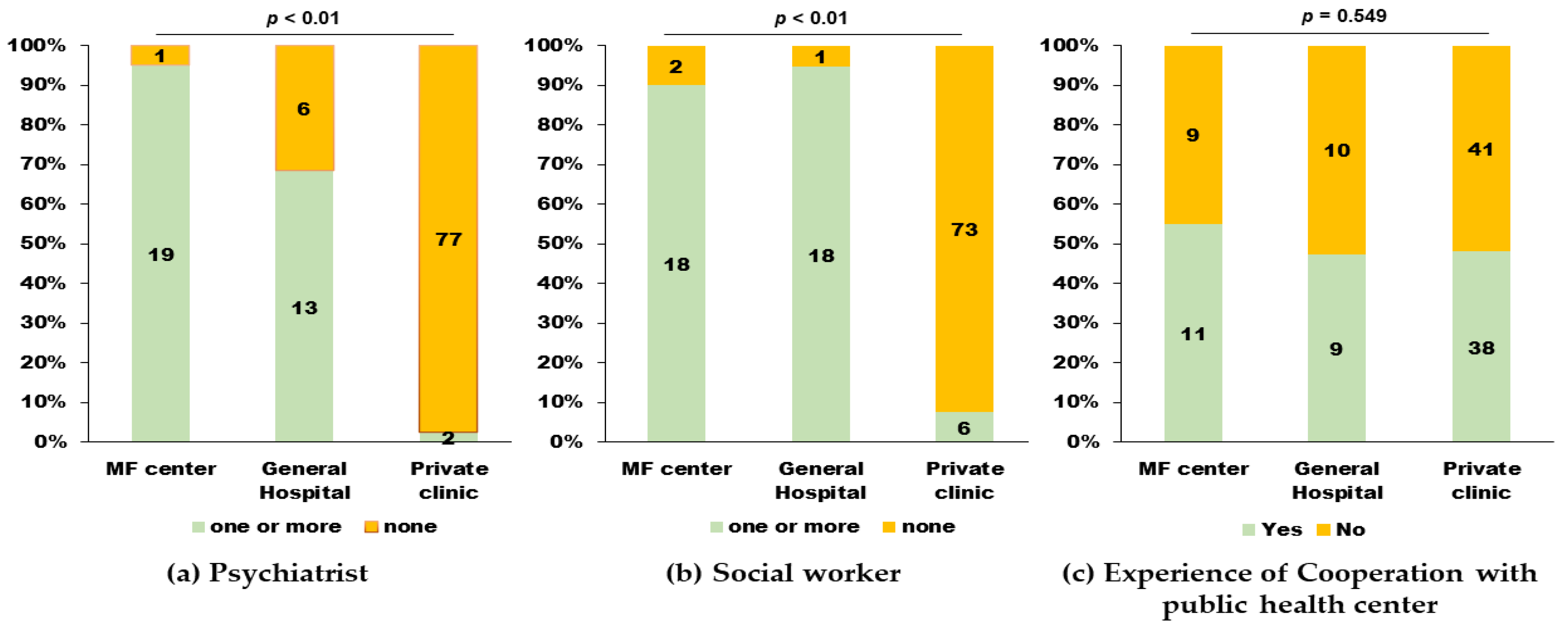
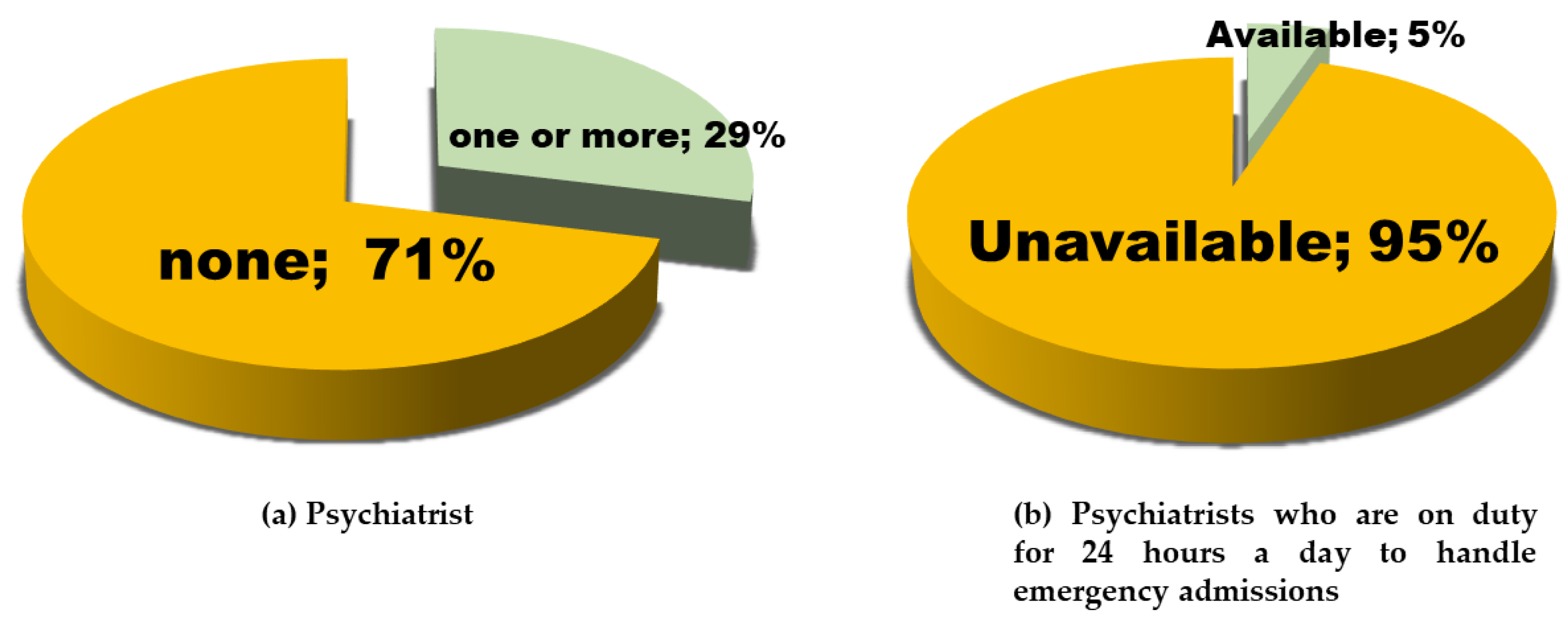
3.3.1. Psychiatrists
3.3.2. Social Workers
3.4. Problems within the Perinatal Mental Health Care System
3.5. Perspectives on Psychotropic Drug Use during Pregnancy among Obstetricians
3.6. NICU Admission of Infants Born to Mothers with Mental Illness
3.7. Preconception Counseling Provided by ART Units
4. Discussion
4.1. Main Findings
4.2. Interpretation of Main Findings
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Q1. About the medical care system | ||
| Q1-1 | Are there psychiatrists in your hospital? | |
| □ Yes →How many full-time psychiatrists are?  on holidays and nighttime; □available □not available →How many part-time psychiatrists are? How often in a week they work? in a week□ No →Do you manage the patients by contacting psychiatrists from other medical facilities? □ Yes □ No | ||
| Q1-2 | How do you manage pregnant or postpartum women with psychiatric complications or a history of psychiatric disorders? | |
| In principle, referral to □ Maternal-fetal center □ General hospital (other than the above) □ Manage on a case-by-case basis with protocols set at own facility → What do you consider to be the criteria when you judge that your facility can manage the patient? (Multiple answers are acceptable) □ Psychiatrist’s opinion □ Unnecessity of medication □ Stable symptoms □ Others □ Others. Please explain.  | ||
| Q1-3 | Are there medical social workers or mental health workers in your hospital? | |
| □ Yes → How many are there? □ No → Do you cooperate with social workers in the community? □ Yes □ No | ||
| Q1-4 | Did you collaborate with the public health center from 2016 to 2018? | |
| □ Yes → Did the collaboration was adopted seamlessly and without any problems? □ Yes □ No □ No | ||
| Q2. Clinical experience of pregnant or postpartum cases with mental illness | ||
| Q2-1 | Did you have any cases of psychiatric hospitalization during the perinatal period? | |
| □ Yes → Please tell us the number of cases. Please indicate the number of cases in which the patient was admitted to a single psychiatric facility in the parentheses. In 2016 → ( )casesIn 2017 → ( )casesIn 2018 → ( )cases□ No | ||
| Q2-2 | Only if you answered “Yes” in Q2-1. What types of psychiatric facilities were available? | |
| □ Your own facility □ Maternal transfer to other facilities → Please tell us about the type of facility. □ Psychiatric hospitals without maternity care units. □ General hospitals that had both maternity care units and mental care units. | ||
| Q2-3 | Despite a deterioration in their mental illness, did you have cases who emergently admitted to maternity care units because they could not be admitted to mental health care units from 2016 to 2018? | |
| □ Yes → Please tell us the number of cases. cases.□ No | ||
| Q2-4 | Were there any cases of legal abortion due to exacerbation of mental illness from 2016 to 2018? | |
| □ Yes →Please tell us the number of cases. cases.□ No | ||
| Q3. Do you think that psychotropic medications should be avoided as much as possible during pregnancy (except for contraindicated psychotropic drugs)? | ||
| □ Yes | □ No | |
| Q4. What problems exist within the present perinatal mental health care system in Aichi Prefecture? (free text) | ||
| Q1. How many beds does your unit have? | |
| beds | |
| Q2. Does your unit collect clinical data about maternal mental illness from the mothers to care for their neonates? | |
| □ Yes: 18 (95.0%) | □ No: 1 (0.5%) |
| Q3. Does your unit have a policy required to prepare for the resuscitation of neonates born to mothers with mental illness? | |
| □ Yes: 4 (21.1%) | □ No: 15 (78.9%) |
| Q4. Does your unit have a policy that required neonates born to mothers who have been prescribed psychotropic drugs to be admitted for toxicity evaluation? | |
| □ Yes: 0 (0.0%) →How long is the admission?  □ hours or □ days □ hours or □ days | □ No: 19 (100.0%) |
| Q5. Did your unit have any cases admitted to the NICU and born to mothers with complications or a history of mental illness? | |
| □ Yes In 2016 casesIn 2017 casesIn 2018 cases | □ No |
| Q1. Please describe the number of treatment cycles in your unit in 2017. | Total cycles (n = 28) |
| in vitro fertilization (IVF) | 3921 |
| intracytoplasmic sperm injection (ICSI) | 7624 |
| frozen embryo transfer (FET) | 13,192 |
| Q2. Have you collected any information on prior history of mental illness or associated complications from your patients through interviews (e.g., medical history)? | |
| number (%) | |
| □ Yes | 28 (100.0) |
| →How do you collect them? | |
| □ By proactively asking clients | 6 (21.4) |
| □ Only if clients voluntarily provide their information | 22 (78.6) |
| □ No | 0 (0.0) |
| Q3. Do you consult with psychiatrists before providing fertility treatment to clients who receive care in mental health hospitals or clinics? | |
| number (%) | |
| □ Yes | 28 (100.0) |
| →In what situation do you seek a consultation? (multiple options can be selected) | |
| □ Every case | 10 |
| □ Only cases with a prescription for mental illness | 6 |
| □ Only cases with unstable mental illness | 14 |
| □ Other | 3 |
| □ No | 0 (0.0) |
| Q4. Do you consult with psychiatrists before providing fertility treatment to clients with a history of mental illness but are not currently receiving psychiatric care? | |
| number (%) | |
| □ Yes | 22 (78.6) |
| →Which psychiatrist do you consult? (multiple options can be selected) | |
| □ A psychiatrist in a hospital that has maternal care and mental health care units | 5 |
| □ A psychiatrist who has previously provided care to my patients | 16 |
| □ Other | 7 |
| □ No | 6 (21.4) |
| Q5. To which obstetric facilities do you refer your clients with mental illnesses when they conceive? (multiple options can be selected) | |
| number | |
| □Undecided | 19 |
| □ A maternal-fetal center | 4 |
| □ A maternal care unit with one or more psychiatrists | 2 |
| □ A hospital with maternal care and mental health care unit | 4 |
| □ Unknown | 2 |
| Q6. Are you aware of any hospitals in Aichi that have both maternal care and mental health care units? | |
| number (%) | |
| □ Yes | 17 (60.7) |
| □ No | 11 (39.3) |
| Q7. Do you think that psychotropic medications should be avoided as much as possible during pregnancy (except for contraindicated psychotropic drugs)? | |
| number (%) | |
| □ Discontinue | 6 (21.4) |
| □ Continue | 18 (64.3) |
| □ Other | 4 (14.3) |
| Q8. What problems have you encountered until now when you are providing fertility treatment to women with a history of mental illness? (free text) | |
References
- Howard, L.M.; Khalifeh, H. Perinatal mental health: A review of progress and challenges. World Psychiatry 2020, 19, 313–327. [Google Scholar] [CrossRef] [PubMed]
- Aktar, E.; Qu, J.; Lawrence, P.J.; Tollenaar, M.S.; Elzinga, B.M.; Bögels, S.M. Fetal and Infant Outcomes in the Offspring of Parents with Perinatal Mental Disorders: Earliest Influences. Front. Psychiatry 2019, 10, 391. [Google Scholar] [CrossRef] [PubMed]
- Montagnoli, C.; Zanconato, G.; Cinelli, G.; Tozzi, A.E.; Bovo, C.; Bortolus, R.; Ruggeri, S. Maternal mental health and reproductive outcomes: A scoping review of the current literature. Arch. Gynecol Obs. 2020, 302, 801–819. [Google Scholar] [CrossRef]
- Tirumalaraju, V.; Suchting, R.; Evans, J.; Goetzl, L.; Refuerzo, J.; Neumann, A.; Anand, D.; Ravikumar, R.; Green, C.E.; Cowen, P.J.; et al. Risk of Depression in the Adolescent and Adult Offspring of Mothers With Perinatal Depression: A Systematic Review and Meta-analysis. JAMA Netw. Open 2020, 3, e208783. [Google Scholar] [CrossRef]
- Tachibana, Y.; Koizumi, N.; Akanuma, C.; Tarui, H.; Ishii, E.; Hoshina, T.; Suzuki, A.; Asano, A.; Sekino, S.; Ito, H. Integrated mental health care in a multidisciplinary maternal and child health service in the community: The findings from the Suzaka trial. BMC Pregnancy Childbirth 2019, 19, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khalifeh, H.; Hunt, I.M.; Appleby, L.; Howard, L.M. Suicide in perinatal and non-perinatal women in contact with psychiatric services: 15 year findings from a UK national inquiry. Lancet Psychiatry 2016, 3, 233–242. [Google Scholar] [CrossRef]
- Lancet, T. Perinatal mental health—Towards a robust system of care. Lancet 2015, 385, 1152. [Google Scholar] [CrossRef]
- Takeda, S.; Takeda, J.; Murakami, K.; Kubo, T.; Hamada, H.; Murakami, M.; Makino, S.; Itoh, H.; Ohba, T.; Naruse, K.; et al. Annual Report of the Perinatology Committee, Japan Society of Obstetrics and Gynecology, 2015: Proposal of urgent measures to reduce maternal deaths. J. Obs. Gynaecol Res. 2017, 43, 5–7. [Google Scholar] [CrossRef]
- Hanley, G.E.; Miller, T.; Mintzes, B. A Cohort Study of Psychotropic Prescription Drug Use in Pregnancy in British Columbia, Canada from 1997 to 2010. J. Womens Health 2020, 29, 1339–1349. [Google Scholar] [CrossRef]
- Cohen, L.S.; Altshuler, L.L.; Harlow, B.L.; Nonacs, R.; Newport, D.J.; Viguera, A.C.; Suri, R.; Burt, V.K.; Hendrick, V.; Reminick, A.M.; et al. Relapse of major depression during pregnancy in women who maintain or discontinue antidepressant treatment. JAMA 2006, 295, 499–507. [Google Scholar] [CrossRef] [Green Version]
- Raffi, E.R.; Nonacs, R.; Cohen, L.S. Safety of Psychotropic Medications During Pregnancy. Clin. Perinatol. 2019, 46, 215–234. [Google Scholar] [CrossRef] [PubMed]
- Betcher, H.K.; Wisner, K.L. Psychotropic Treatment During Pregnancy: Research Synthesis and Clinical Care Principles. J. Womens Health 2020, 29, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Creeley, C.E.; Denton, L.K. Use of Prescribed Psychotropics during Pregnancy: A Systematic Review of Pregnancy, Neonatal, and Childhood Outcomes. Brain Sci. 2019, 9, 235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chisolm, M.S.; Payne, J.L. Management of psychotropic drugs during pregnancy. BMJ 2016, 532, h5918. [Google Scholar] [CrossRef] [PubMed]
- Wilson, C.; Howard, L.M.; Reynolds, R.M.; Simonoff, E.; Ismail, K. Preconception health. Lancet 2018, 392, 2266–2267. [Google Scholar] [CrossRef] [Green Version]
- Catalao, R.; Mann, S.; Wilson, C.; Howard, L.M. Preconception care in mental health services: Planning for a better future. Br. J. Psychiatry 2020, 216, 180–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engelstad, H.J.; Roghair, R.D.; Calarge, C.A.; Colaizy, T.T.; Stuart, S.; Haskell, S.E. Perinatal outcomes of pregnancies complicated by maternal depression with or without selective serotonin reuptake inhibitor therapy. Neonatology 2014, 105, 149–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Latendresse, G.; Wong, B.; Dyer, J.; Wilson, B.; Baksh, L.; Hogue, C. Duration of Maternal Stress and Depression: Predictors of Newborn Admission to Neonatal Intensive Care Unit and Postpartum Depression. Nurs. Res. 2015, 64, 331–341. [Google Scholar] [CrossRef]
- Connellan, K.; Bartholomaeus, C.; Due, C.; Riggs, D.W. A systematic review of research on psychiatric mother-baby units. Arch. Womens Ment Health 2017, 20, 373–388. [Google Scholar] [CrossRef]
- Lever Taylor, B.; Mosse, L.; Stanley, N. Experiences of social work intervention among mothers with perinatal mental health needs. Health Soc. Care Community 2019, 27, 1586–1596. [Google Scholar] [CrossRef]
- Suzuki, S. Recent status of pregnant women with mental disorders at a Japanese perinatal center. J. Matern Fetal Neonatal Med. 2018, 31, 2131–2135. [Google Scholar] [CrossRef] [PubMed]
- Noonan, M.; Galvin, R.; Jomeen, J.; Doody, O. Public health nurses’ perinatal mental health training needs: A cross sectional survey. J. Adv. Nurs. 2019, 75, 2535–2547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berger, A.; Schenk, K.; Ging, A.; Walther, S.; Cignacco, E. Perinatal mental health care from the user and provider perspective: Protocol for a qualitative study in Switzerland. Reprod Health 2020, 17, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]




| Type of Maternity Care Units | Psychotropic Drug Use during Pregnancy | p-Value | ||
|---|---|---|---|---|
| Discontinue | Continue | Other | ||
| MF center (n = 20) | 1 (5.0) | 18 (90.0) | 1 (5.0) | 0.033 |
| General hospital (n = 19) | 6 (31.6) | 13 (68.4) | 0 (0.0) | |
| Private clinic (n = 79) | 28 (35.4) | 45 (57.0) | 6 (7.6) | |
| Total (n = 118) | 35 (29.7) | 76 (64.4) | 7 (5.9) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fujita, K.; Kotani, T.; Moriyama, Y.; Ushida, T.; Imai, K.; Kobayashi-Nakano, T.; Kato, N.; Kano, T.; Kikkawa, F.; Kajiyama, H. Current Issues within the Perinatal Mental Health Care System in Aichi Prefecture, Japan: A Cross-Sectional Questionnaire Survey. Int. J. Environ. Res. Public Health 2021, 18, 9122. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179122
Fujita K, Kotani T, Moriyama Y, Ushida T, Imai K, Kobayashi-Nakano T, Kato N, Kano T, Kikkawa F, Kajiyama H. Current Issues within the Perinatal Mental Health Care System in Aichi Prefecture, Japan: A Cross-Sectional Questionnaire Survey. International Journal of Environmental Research and Public Health. 2021; 18(17):9122. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179122
Chicago/Turabian StyleFujita, Kei, Tomomi Kotani, Yoshinori Moriyama, Takafumi Ushida, Kenji Imai, Tomoko Kobayashi-Nakano, Noriko Kato, Takeo Kano, Fumitaka Kikkawa, and Hiroaki Kajiyama. 2021. "Current Issues within the Perinatal Mental Health Care System in Aichi Prefecture, Japan: A Cross-Sectional Questionnaire Survey" International Journal of Environmental Research and Public Health 18, no. 17: 9122. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179122