
A Study on Physical Exercise and General Mobility in People with Cerebral Palsy: Health through Costless Routines

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Study 1: Global Perspective of the Population
- Deficiencies in body structures and functions—this is the point which is assessed more methodologically;
- Activities performed by the person and their limitations—this aspect is less technical and based on observation;
- Interaction with the environment—this refers to the supporting context needed for their interaction: caregivers, technical aids, etc.
2.1. Participants
2.2. Methods
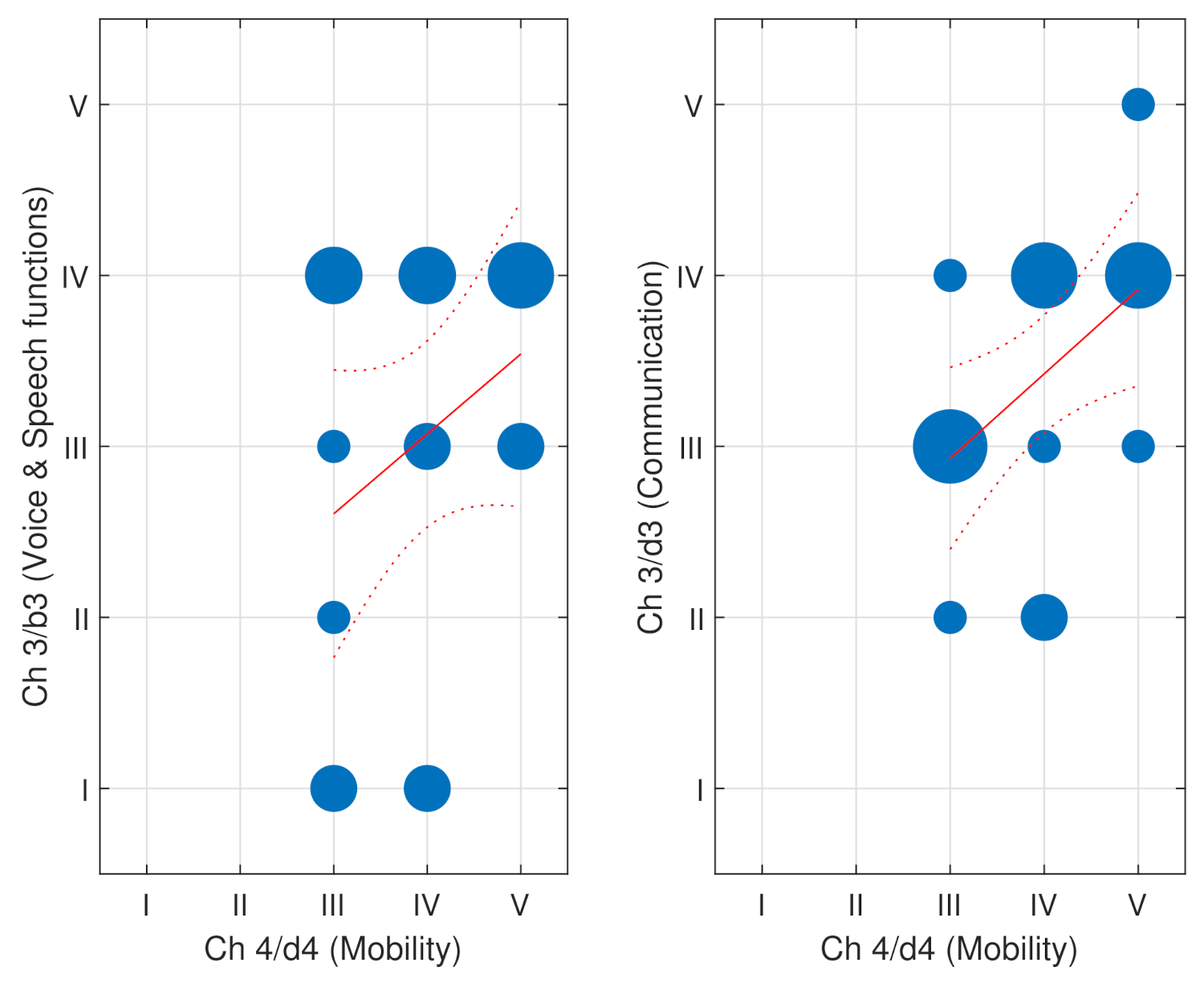
2.2.1. Instruments and Variables: The ICF Scale at ASPACE
- Functioning and disability
- (a)
- Body functions and structures
- (b)
- Activities and participation
- Contextual factors
- (a)
- Environmental factors
- (b)
- Personal factors
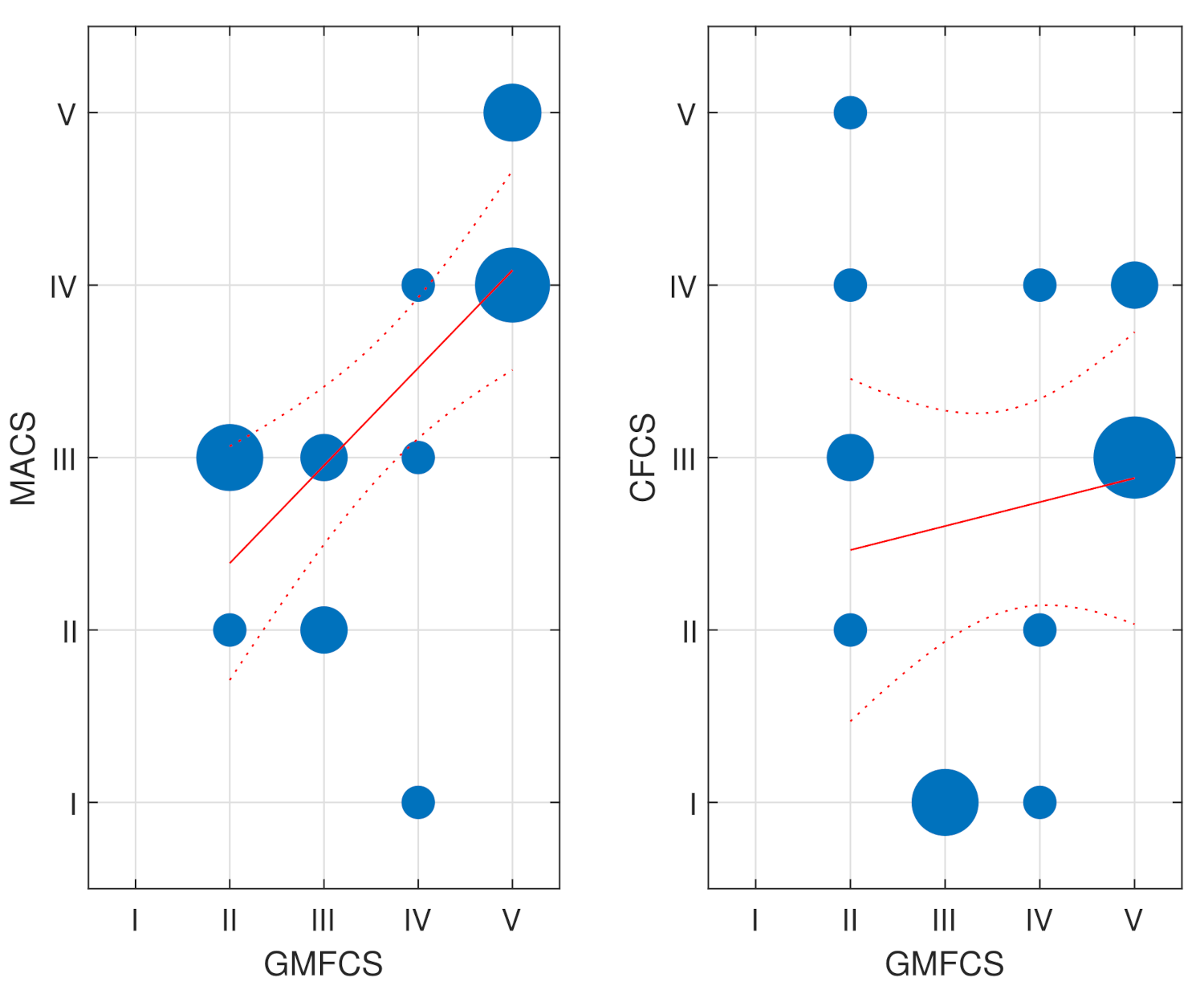
2.2.2. Instruments and Variables: GMFCS, MACS and CFCS Scales at CEEEMS
- Level I
- Ability to ambulate;
- Level II
- Independently ambulates with limitations;
- Level III
- Ambulates with walking aids;
- Level IV
- Independently mobile with powered mobility;
- Level V
- Dependent on AT for all mobility.
- Level I
- Handles objects easily and successfully;
- Level II
- Handles most items. Slight reduction in achievement quality and/or speed;
- Level III
- Handles objects with difficulty and needs help;
- Level IV
- Manipulates a limited selection of objects in adapted situations;
- Level V
- Does not manipulate objects. Limited ability to perform simple actions.
- Level I
- Efficient sender and receiver with known and unknown interlocutors;
- Level II
- Efficient sender and/or receiver, but with a slower pace with known and/or unknown interlocutors;
- Level III
- Efficient sender and efficient receiver with known interlocutors;
- Level IV
- Inconsistent sender and/or receiver with known interlocutors;
- Level V
- Sender and receiver rarely effective even with known interlocutors.
2.2.3. Homogenization of Scales
2.2.4. Data Analysis
2.3. Results
2.4. Discussion
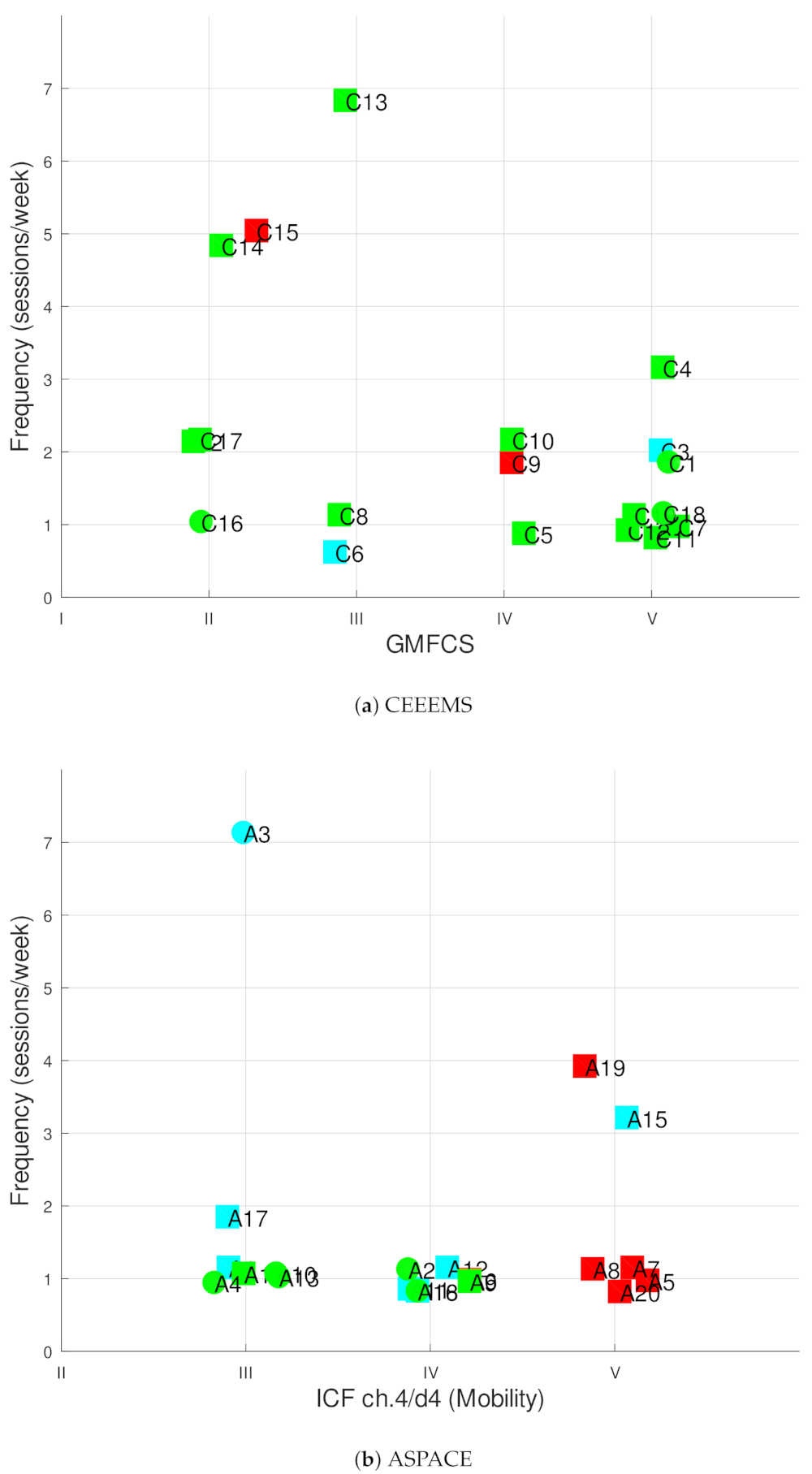
3. Study 2: Regular Physical Activity in People with CP
- Frequency refers to the number of sessions per week. The ACSM recommendation includes at least three to five sessions to increase or maintain cardiorespiratory fitness with a recovery between sessions of 24–36 h. Some studies demonstrated that training was still effective although the frequency did not meet the minimal recommendations [35,36,37];
- Intensity is related to effort and is often indicated relative to maximal heart rate, heart rate reserve (HRR), the difference between a person’s measured or predicted maximum heart rate and resting heart rate and/or peak oxygen consumption. Although the intensity may vary from the beginning of the training, in general, all studies were aligned with the recommendation of more than 60% of maximum heart rate or more than 40% of the HRR;
- Time refers to the duration of the training session, which may be at least 20 min for aerobic workout and for a minimum of 8 or 16 consecutive weeks, depending on frequency;
- Types of activities are diverse and suited to people’s conditions (sports, running, muscle strengthening, etc.), and they must fulfill the therapist’s recommendations.
3.1. Participants
3.2. Methods
Data Analysis
3.3. Results
3.4. Conclusions
4. Study 3: Review of Physical Activities
4.1. Methods
4.2. Results
4.2.1. Recommended Exercises and Equipment
4.2.2. Equipment for Monitoring Physical Activity
4.3. Discussion of Low-Cost Solutions
5. Global Discussion
Study Limitations
6. Conclusions and Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- WHO. A Guide for Population-Based Approaches to Increasing Levels of Physical Activity: Implementation of the WHO Global Strategy on Diet, Physical Activity and Health; World Health Organization: Geneva, Switzerland, 2007; pp. 1–20. [Google Scholar]
- WHO. Global Priority Research Agenda for Improving Access to High-Quality Affordable Assistive Technology; World Health Organization: Geneva, Switzerland, 2017; pp. 1–24. [Google Scholar]
- Scholtes, V.A.; Becher, J.G.; Comuth, A.; Dekkers, H.; van Dijk, L.; Dallmeijer, A.J. Effectiveness of functional progressive resistance exercise strength training on muscle strength and mobility in children with cerebral palsy: A randomized controlled trial. Dev. Med. Child Neurol. 2010, 52, e107–e113. [Google Scholar] [CrossRef]
- Engsberg, J.R.; Ross, S.A.; Collins, D.R. Increasing ankle strength to improve gait and function in children with cerebral palsy: A pilot study. Pediatr. Phys. Ther. 2006, 18, 266–275. [Google Scholar] [CrossRef]
- Stubbs, P.W.; Diong, J. The effect of strengthening interventions on strength and physical performance in people with cerebral palsy (PEDro synthesis). Br. J. Sport. Med. 2016, 50, 189–190. [Google Scholar] [CrossRef] [PubMed]
- Hanna, S.E.; Rosenbaum, P.L.; Bartlett, D.J.; Palisano, R.J.; Walter, S.D.; Avery, L.; Russell, D.J. Stability and decline in gross motor function among children and youth with cerebral palsy aged 2 to 21 years. Dev. Med. Child Neurol. 2009, 51, 295–302. [Google Scholar] [CrossRef]
- Palisano, R.; Rosenbaum, P.; Walter, S.; Russell, D.; Wood, E.; Galuppi, B. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev. Med. Child Neurol. 1997, 39, 214–223. [Google Scholar] [CrossRef] [PubMed]
- Pavone, P.; Gulizia, C.; Le Pira, A.; Greco, F.; Parisi, P.; Di Cara, G.; Falsaperla, R.; Lubrano, R.; Minardi, C.; Spalice, A.; et al. Cerebral palsy and epilepsy in children: Clinical perspectives on a common comorbidity. Children 2021, 8, 16. [Google Scholar] [CrossRef]
- Peterson, M.D.; Ryan, J.M.; Hurvitz, E.A.; Mahmoudi, E. Chronic conditions in adults with cerebral palsy. JAMA 2015, 314, 2303–2305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strauss, D.; Cable, W.; Shavelle, R. Causes of excess mortality in cerebral palsy. Dev. Med. Child Neurol. 1999, 41, 580–585. [Google Scholar] [CrossRef] [PubMed]
- Kim, M. Cerebral palsy update—Focusing on the treatments and interventions. Hanyang Med. Rev. 2016, 36, 59–64. [Google Scholar] [CrossRef] [Green Version]
- Verschuren, O.; Peterson, M.D.; Balemans, A.C.; Hurvitz, E.A. Exercise and physical activity recommendations for people with cerebral palsy. Dev. Med. Child Neurol. 2016, 58, 798–808. [Google Scholar] [CrossRef]
- Spanish-Labour-&-Social-Economy-Ministry. Dependence rating: Criteria and techniques of assessment and classification. Depend. White Pap. 2005, 9, 553–632. [Google Scholar]
- Romeo, S.; Gala, B.; Gómez, E. Uso de escalas de valoración en el proyecto de ley de promoción de la autonomía personal y de atención a las personas dependientes. Index Enferm. 2006, 15, 56–61. [Google Scholar]
- Bartlett, J.E.; Kotrlik, J.W.; Higgins, C.C. Organizational Research: Determining Appropriate Sample Size in Survey Research. Inf. Technol. Learn. Perform. J. 2001, 19, 43–50. [Google Scholar]
- WHO. International Classification of Functioning, Disability and Health: ICF; World Health Organization: Geneva, Switzerland, 2001; pp. 1–315. [Google Scholar]
- Jeevanantham, D.; Dyszuk, E.; Bartlett, D. The Manual Ability Classification System. Pediatr. Phys. Ther. 2015, 27, 236–241. [Google Scholar] [CrossRef]
- Hidecker, M.J.C.; Paneth, N.; Rosenbaum, P.L.; Kent, R.D.; Lillie, J.; Eulenberg, J.B.; Chester, K.; Johnson, B.; Michalsen, L.; Evatt, M.; et al. Developing and validating the Communication Function Classification System for individuals with cerebral palsy. Dev. Med. Child Neurol. 2011, 53, 704–710. [Google Scholar] [CrossRef] [PubMed]
- Westbom, L.; Hagglund, G.; Nordmark, E. Cerebral palsy in a total population of 4–11 year olds in southern Sweden. Prevalence and distribution according to different CP classification systems. BMC Pediatr. 2007, 7, 41. [Google Scholar] [CrossRef] [Green Version]
- Reid, S.M.; Carlin, J.B.; Reddihough, D.S. Using the Gross Motor Function Classification System to describe patterns of motor severity in cerebral palsy. Dev. Med. Child Neurol. 2011, 53, 1007–1012. [Google Scholar] [CrossRef] [PubMed]
- Bugler, K.E.; Gaston, M.S.; Robb, J.E. Distribution and motor ability of children with cerebral palsy in Scotland: A registry analysis. Scott. Med. J. 2019, 64, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Caspersen, C.J.; Powell, K.E.; Christenson, G.M. Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Rep. 1985, 100, 126–131. [Google Scholar]
- Clutterbuck, G.; Auld, M.; Johnston, L. Active exercise interventions improve gross motor function of ambulant/semi-ambulant children with cerebral palsy: A systematic review. Disabil. Rehabil. 2019, 41, 1131–1151. [Google Scholar] [CrossRef]
- Ryan, J.M.; Cassidy, E.E.; Noorduyn, S.G.; O’Connell, N.E. Exercise interventions for cerebral palsy. Cochrane Database Syst. Rev. 2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samsir, M.S.; Zakaria, R.; Razak, S.A.; Ismail, M.S.; Rahim, M.Z.A.; Lin, C.S.; Osman, N.M.F.N.; Asri, M.A.; Mohd, N.H.; Ahmad, A.H. Six months guided exercise therapy improves motor abilities and white matter connectivity in children with cerebral palsy. Malays. J. Med. Sci. 2020, 27, 90–100. [Google Scholar] [CrossRef]
- Bar-Haim, S.; Aviram, R.; Rabani, A.S.; Amro, A.; Nammourah, I.; Al-Jarrah, M.; Raanan, Y.; Loeppky, J.A.; Harries, N. Effects of exercise interventions on habitual physical activity and sedentary behavior in adolescents with cerebral palsy. Pediatr. Exerc. Sci. 2019, 31, 416–424. [Google Scholar] [CrossRef] [PubMed]
- Fujimoto, J.; Umemoto, Y.; Koike, Y.; Isida, K.; Sakamoto, K.; Tajima, F. Immediate effects of short period lower limb ergometer exercise in adolescent and young adult patients with cerebral palsy and spastic diplegia. J. Phys. Ther. Sci. 2021, 33, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Liang, X.; Tan, Z.; Yun, G.; Cao, J.; Wang, J.; Liu, Q.; Chen, T. Effectiveness of exercise interventions for children with cerebral palsy: A systematic review and meta-analysis of randomized controlled trials. J. Rehabil. Med. 2020, 53, 1–10. [Google Scholar] [CrossRef]
- Chen, Y.; Fanchiang, H.; Howard, A. Effectiveness of virtual reality in children with cerebral palsy: A systematic review and meta-analysis of randomized controlled trials. Phys. Ther. 2017, 98, 63–77. [Google Scholar] [CrossRef]
- Adar, S.; Dündar, Ü.; Demirdal, Ü.S.; Ulaşlı, A.M.; Toktaş, H.; Solak, Ö. The effect of aquatic exercise on spasticity, quality of life, and motor function in cerebral palsy. Turk. J. Phys. Med. Rehabil. 2017, 63, 239–248. [Google Scholar] [CrossRef]
- Reddy, S.; Balaji, G.K. Dynamic surface exercise training in improving trunk control and gross motor functions among children with quadriplegic cerebral palsy: A single center, randomized controlled trial. J. Pediatr. Neurosci. 2020, 15, 214–219. [Google Scholar] [PubMed]
- Carlon, S.L.; Taylor, N.F.; Dodd, K.J.; Shields, N. Differences in habitual physical activity levels of young people with cerebral palsy and their typically developing peers: A systematic review. Disabil. Rehabil. 2013, 35, 647–655. [Google Scholar] [CrossRef]
- Satonaka, A.; Suzuki, N. Aerobic fitness and lifestyle with non-exercise physical activity in adults with cerebral palsy. J. Phys. Fit. Sport. Med. 2018, 7, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sport. Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef]
- Saris, W. Physical training of school children with spastic cerebral palsy: Effects on daily activity. Int. J. Rehabil. Res. 1998, 21, 179–194. [Google Scholar]
- Verschuren, O.; Ketelaar, M.; Gorter, J.W.; Helders, P.J.; Uiterwaal, C.S.; Takken, T. Exercise training program in children and adolescents with cerebral palsy: A randomized controlled trial. Arch. Pediatr. Adolesc. Med. 2007, 161, 1075–1081. [Google Scholar] [CrossRef] [PubMed]
- Slaman, J.; Roebroeck, M.; van der Slot, W.; Twisk, J.; Wensink, A.; Stam, H.; van den Berg-Emons, R.; move Research Group, L. Can a lifestyle intervention improve physical fitness in adolescents and young adults with spastic cerebral palsy? A randomized controlled trial. Arch. Phys. Med. Rehabil. 2014, 95, 1646–1655. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.J. Effects of group exercise program on the health condition and quality of life in adults with cerebral palsy. J. Int. Acad. Phys. Ther. Res. 2018, 9, 1549–1557. [Google Scholar] [CrossRef]
- Gannotti, M.E.; Liquori, B.M.; Thorpe, D.E.; Fuchs, R.K. Designing exercise to improve bone health among individuals with cerebral palsy. Pediatr. Phys. Ther. 2021, 33, 50–56. [Google Scholar] [CrossRef]
- Kim, B.J.; Kim, S.M.; Kwon, H.Y. The effect of group exercise program on the self-efficacy and activities of daily living in adults with cerebral palsy. J. Phys. Ther. Sci. 2017, 29, 2184–2189. [Google Scholar] [CrossRef] [Green Version]
- Qi, Y.C.; Niu, X.L.; Gao, Y.R.; Wang, H.b.; Hu, M.; Dong, L.P.; Li, Y.Z. Therapeutic effect evaluation of neuromuscular electrical stimulation with or without strengthening exercise on spastic cerebral palsy. Clin. Pediatr. 2018, 57, 580–583. [Google Scholar] [CrossRef]
- Armstrong, E.L.; Boyd, R.N.; Kentish, M.J.; Carty, C.P.; Horan, S.A. Effects of a training programme of functional electrical stimulation (FES) powered cycling, recreational cycling and goal-directed exercise training on children with cerebral palsy: A randomised controlled trial protocol. Br. Med. J. Open 2019, 9, e024881. [Google Scholar] [CrossRef] [PubMed]
- Ahmadizadeh, Z.; Amozade Khalili, M.; Simin Ghalam, M.; Mokhlesin, M. Effect of whole body vibration with stretching exercise on active and passive range of motion in lower extremities in children with cerebral palsy: A randomized clinical trial. Iran. J. Pediatr. 2019, 29, e84436. [Google Scholar] [CrossRef] [Green Version]
- Peters, M.; Godfrey, C.; Mcinerney, P.; Soares, C.; Khalil, H.; Parker, D. Methodology for JBI Scoping Reviews. Joanna Briggs Inst. Rev. Man. 2015, 1, 3–24. [Google Scholar]
- Lawrence, H.; Hills, S.; Kline, N.; Weems, K.; Doty, A. Effectiveness of exercise on functional mobility in adults with cerebral palsy: A systematic review. Physiother. Can. 2016, 68, 398–407. [Google Scholar] [CrossRef] [Green Version]
- Leineweber, M.J.; Wyss, D.; Dufour, S.K.; Gane, C.; Zabjek, K.; Bouyer, L.J.; Maltais, D.B.; Voisin, J.I.; Andrysek, J. The effects of acute intense physical exercise on postural stability in children with cerebral palsy. Adapt. Phys. Act. Q. 2016, 33, 271–282. [Google Scholar] [CrossRef] [PubMed]
- Joung, H.J.; Park, J.; Ahn, J.; Park, M.S.; Lee, Y. Effects of creative dance-based exercise on gait performance in adolescents with cerebral palsy. J. Exerc. Rehabil. 2020, 16, 332–343. [Google Scholar] [CrossRef]
- Peungsuwan, P.; Parasin, P.; Siritaratiwat, W.; Prasertnu, J.; Yamauchi, J. Effects of combined exercise training on functional performance in children with cerebral palsy: A randomized-controlled study. Pediatr. Phys. Ther. 2017, 29, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Mullerpatan, R.; Thanawala, M.; Agarwal, B.; Ganesan, S. Development of the deep squat milestone in typically developing children. Crit. Rev. Phys. Rehabil. Med. 2019, 31, 63–73. [Google Scholar] [CrossRef]
- Claridge, E.A.; Van Den Berg-Emons, R.J.; Horemans, H.L.; Van Der Slot, W.M.; Van Der Stam, N.; Tang, A.; Timmons, B.W.; Gorter, J.W.; Bussmann, J.B. Detection of body postures and movements in ambulatory adults with cerebral palsy: A novel and valid measure of physical behaviour. J. Neuroeng. Rehabil. 2019, 16, 125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bahrami, F.; Noorizadeh Dehkordi, S.; Dadgoo, M. The efficacy of treadmill training on walking and quality of life of adults with spastic cerebral palsy: A randomized controlled trial. Iran. J. Child Neurol. 2019, 13, 121–133. [Google Scholar] [PubMed]
- Shemy, S.A.E. Trunk endurance and gait changes after core stability training in children with hemiplegic cerebral palsy: A randomized controlled trial. J. Back Musculoskelet. Rehabil. 2018, 31, 1159–1167. [Google Scholar] [CrossRef]
- Liaqat, S.; Butt, M.S.; Javaid, H.M. Effects of universal exercise unit therapy on sitting balance in children with spastic and athetoid cerebral palsy: A quasi-experimental study. Khyber Med. Univ. J. 2016, 8, 177–180. [Google Scholar]
- Afzal, F. Strength training by using universal exercise unit to improve the motor functions in cerebral palsy. Rawal Med. J. 2018, 43, 120–123. [Google Scholar]
- Ryan, J.M.; Theis, N.; Kilbride, C.; Baltzopoulos, V.; Waugh, C.; Shortland, A.; Lavelle, G.; Noorkoiv, M.; Levin, W.; Korff, T. Strength training for adolescents with cerebral palsy (STAR): Study protocol of a randomised controlled trial to determine the feasibility, acceptability and efficacy of resistance training for adolescents with cerebral palsy. Br. Med. J. Open 2016, 6, e012839. [Google Scholar] [CrossRef] [Green Version]
- Shin, S.O.; Kim, N.S. Upper extremity resistance exercise with elastic bands for respiratory function in children with cerebral palsy. J. Phys. Ther. Sci. 2017, 29, 2077–2080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lauruschkus, K.; Hallström, I.; Westbom, L.; Tornberg, Å.; Nordmark, E. Participation in physical activities for children with cerebral palsy: Feasibility and effectiveness of physical activity on prescription. Arch. Physiother. 2017, 7, 13. [Google Scholar] [CrossRef] [Green Version]
- Akinola, B.I.; Gbiri, C.A.; Odebiyi, D.O. Effect of a 10-week aquatic exercise training program on gross motor function in children with spastic cerebral palsy. Glob. Pediatr. Health 2019, 6. [Google Scholar] [CrossRef] [PubMed]
- Novak, I.; Morgan, C.; Fahey, M.; Finch-Edmondson, M.; Galea, C.; Hines, A.; Langdon, K.; Namara, M.M.; Paton, M.C.; Popat, H.; et al. State of the evidence traffic lights 2019: Systematic review of interventions for preventing and treating children with cerebral palsy. Curr. Neurol. Neurosci. Rep. 2020, 20, 3. [Google Scholar] [CrossRef] [Green Version]
- Cabrera, R.; Molina, A.; Gómez, I.; García-Heras, J. Kinect as an access device for people with cerebral palsy: A preliminary study. Int. J. Hum. Comput. Stud. 2017, 108, 62–69. [Google Scholar] [CrossRef]
- Camara Machado, F.R.; Antunes, P.P.; Souza, J.D.M.; Dos Santos, A.C.; Levandowski, D.C.; De Oliveira, A.A. Motor improvement using motion sensing game devices for cerebral palsy rehabilitation. J. Mot. Behav. 2017, 49, 273–280. [Google Scholar] [CrossRef]
- Sevick, M.; Eklund, E.; Mensch, A.; Foreman, M.; Standeven, J.; Engsberg, J. Using free internet videogames in upper extremity motor training for children with cerebral palsy. Behav. Sci. 2016, 6, 10. [Google Scholar] [CrossRef]
- Bonnechère, B.; Omelina, L.; Kostkova, K.; Van Sint Jan, S.; Jansen, B. The end of active video games and the consequences for rehabilitation. Physiother. Res. Int. 2018, 23, e1752. [Google Scholar] [CrossRef]
- Kassee, C.; Hunt, C.; Holmes, M.W.; Lloyd, M. Home-based Nintendo Wii training to improve upper-limb function in children ages 7 to 12 with spastic hemiplegic cerebral palsy. J. Pediatr. Rehabil. Med. 2017, 10, 145–154. [Google Scholar] [CrossRef]
- Gatica-Rojas, V.; Cartes-Velásquez, R.; Méndez-Rebolledo, G.; Olave-Godoy, F.; Villalobos-Rebolledo, D. Change in functional balance after an exercise program with Nintendo Wii in latino patients with cerebral palsy: A case series. J. Phys. Ther. Sci. 2016, 28, 2414–2417. [Google Scholar] [CrossRef] [Green Version]
- Cooper, T.; Williams, J.M. Does an exercise programme integrating the Nintendo Wii-Fit Balance Board improve balance in ambulatory children with cerebral palsy? Phys. Ther. Rev. 2017, 22, 229–237. [Google Scholar] [CrossRef]
- Ren, Z.; Wu, J. The effect of virtual reality games on the gross motor skills of children with cerebral palsy: A meta-analysis of randomized controlled trials. Int. J. Environ. Res. Public Health 2019, 16, 3883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Warnier, N.; Lambregts, S.; Port, I.V.D. Effect of virtual reality therapy on balance and walking in children with cerebral palsy: A systematic review. Dev. Neurorehabilit. 2020, 23, 502–518. [Google Scholar] [CrossRef]
- Ahmadi, M.N.; O’neil, M.E.; Baque, E.; Boyd, R.N.; Trost, S.G. Machine learning to quantify physical activity in children with cerebral palsy: Comparison of group, group-personalized, and fully-personalized activity classification models. Sensors 2020, 20, 3976. [Google Scholar] [CrossRef]
- Elmacı, D.T.; Cevizci, S. Dog-assisted therapies and activities in rehabilitation of children with cerebral palsy and physical and mental disabilities. Int. J. Environ. Res. Public Health 2015, 12, 5046–5060. [Google Scholar] [CrossRef]
- Mutoh, T.; Mutoh, T.; Takada, M.; Doumura, M.; Ihara, M.; Taki, Y.; Tsubone, H.; Ihara, M. Application of a tri-axial accelerometry-based portable motion recorder for the quantitative assessment of hippotherapy in children and adolescents with cerebral palsy. J. Phys. Ther. Sci. 2016, 28, 2970–2974. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sahebalzamani, M.; Rezaei, O.; Moghadam, L.F. Animal-assisted therapy on happiness and life quality of chronic psychiatric patients living in psychiatric residential care homes: A randomized controlled study. BMC Psychiatry 2020, 20, 575. [Google Scholar] [CrossRef]
- Bjornson, K.F.; Moreau, N.; Bodkin, A.W. Short-burst interval treadmill training walking capacity and performance in cerebral palsy: A pilot study. Dev. Neurorehabil. 2019, 22, 126–133. [Google Scholar] [CrossRef] [PubMed]
- Bjornson, K.; Fiss, A.; Avery, L.; Wentz, E.; Kerfeld, C.; Cicirello, N.; Hanna, S.E. Longitudinal trajectories of physical activity and walking performance by gross motor function classification system level for children with cerebral palsy. Disabil. Rehabil. 2020, 42, 1705–1713. [Google Scholar] [CrossRef]
- Benner, J.L.; McPhee, P.G.; Gorter, J.W.; Hurvitz, E.A.; Peterson, M.D.; Obeid, J.; Wright, M.; Balemans, A.C.; Verschuren, O.; van den Berg-Emons, R.H.; et al. Focus on risk factors for cardiometabolic disease in cerebral palsy: Toward a core set of outcome measurement instruments. Arch. Phys. Med. Rehabil. 2019, 100, 2389–2398. [Google Scholar] [CrossRef]
- Williams, S.A.; McFadden, L.M.; Blackmore, A.M.; Davey, P.; Gibson, N. Do adolescents with cerebral palsy meet recommendations for healthy weight and physical activity behaviours? Disabil. Rehabil. 2020, 42, 1227–1232. [Google Scholar] [CrossRef] [PubMed]
- Gerber, C.N.; Carcreff, L.; Paraschiv-Ionescu, A.; Armand, S.; Newman, C.J. Multidimensional measures of physical activity and their association with gross motor capacity in children and adolescents with cerebral palsy. Sensors 2020, 20, 5861. [Google Scholar] [CrossRef] [PubMed]
- Xing, R.; Huang, W.Y.; Sit, C.H. Validity of accelerometry for predicting physical activity and sedentary time in ambulatory children and young adults with cerebral palsy. J. Exerc. Sci. Fit. 2021, 19, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Goodlich, B.I.; Armstrong, E.L.; Horan, S.A.; Baque, E.; Carty, C.P.; Ahmadi, M.N.; Trost, S.G. Machine learning to quantify habitual physical activity in children with cerebral palsy. Dev. Med. Child Neurol. 2020, 62, 1054–1060. [Google Scholar] [CrossRef]
- Pingel, J.; Andersen, I.T.; Broholm, R.; Harder, A.; Bartels, E.M.; Bülow, J.; Harrison, A. An acoustic myography functional assessment of cerebral palsy subjects compared to healthy controls during physical exercise. J. Muscle Res. Cell Motil. 2019, 40, 53–58. [Google Scholar] [CrossRef]
- González, L.; Argüelles, J.; González, V.; Winge, K.; Iscar, M.; Olmedillas, H.; Blanco, M.; Valenzuela, P.L.; Lucia, A.; Federolf, P.A.; et al. Slackline training in children with spastic cerebral palsy: A randomized clinical trial. Int. J. Environ. Res. Public Health 2020, 17, 8649. [Google Scholar] [CrossRef]
- Michelsen, J.S.; Lund, M.C.; Alkjær, T.; Finni, T.; Nielsen, J.B.; Lorentzen, J. Wearable electromyography recordings during daily life activities in children with cerebral palsy. Dev. Med. Child Neurol. 2020, 62, 714–722. [Google Scholar] [CrossRef]
- Landis, C.; O’Neil, M.E.; Finnegan, A.; Shewokis, P.A. Calculating heart rate variability from ECG data from youth with cerebral palsy during active video game sessions. J. Vis. Exp. 2019, 148, e59230. [Google Scholar] [CrossRef] [Green Version]
- Ryan, J.; Theis, N.; Koufaki, P.; Phillips, S.; Anokye, N.; Andreopoulou, G.; Kennedy, F.; Jagadamma, K.C.; VanSchie, P.; Dines, H.; et al. Effect of RaceRunning on cardiometabolic disease risk factors and functional mobility in young people with moderate-to-severe cerebral palsy: Protocol for a feasibility study. Br. Med. J. Open 2020, 10, e036469. [Google Scholar]
- Malu, M.; Chundury, P.; Findlater, L. Exploring accessible smartwatch interactions for people with upper body motor impairments. Conf. Hum. Factors Comput. Syst. 2018, 38. [Google Scholar] [CrossRef]
- Díaz, S.; Stephenson, J.B.; Labrador, M.A. Use of wearable sensor technology in gait, balance, and range of motion analysis. Appl. Sci. 2020, 10, 234. [Google Scholar] [CrossRef] [Green Version]
- Cao, Z.; Hidalgo, G.; Simon, T.; Wei, S.E.; Sheikh, Y. Openpose: Realtime multi-person 2D pose estimation using part affinity fields. IEEE Trans. Pattern Anal. Mach. Intell. 2021, 43, 172–186. [Google Scholar] [CrossRef] [Green Version]
- Castro-Garcia, J.A.; Molina-Cantero, A.J.; Merino-Monge, M.; Gomez-Gonzalez, I.M. An open-source hardware acquisition platform for physiological measurements. IEEE Sens. J. 2019, 19, 11526–11534. [Google Scholar] [CrossRef]
- Kwon, K.B.; Choi, Y.; Sung, K.H.; Chung, C.Y.; Lee, K.M.; Kwon, S.S.; Cho, G.H.; Park, M.S. Correlation between accelerometer and questionnaire-based assessment of physical activity in patients with cerebral palsy. Clin. Orthop. Surg. 2020, 12, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Claridge, E.A.; Mcphee, P.G.; Timmons, B.W.; KA, M.G.; Macdonald, M.J.; Gorter, J.W. Quantification of physical activity and sedentary time in adults with cerebral palsy. Med. Sci. Sport. Exerc. 2015, 47, 1719–1726. [Google Scholar] [CrossRef] [PubMed]
- Nooijen, C.F.; Slaman, J.; Stam, H.J.; Roebroeck, M.E.; Van Den Berg-Emons, R.J. Inactive and sedentary lifestyles amongst ambulatory adolescents and young adults with cerebral palsy. J. Neuroeng. Rehabil. 2014, 11, 49. [Google Scholar] [CrossRef] [Green Version]
- Katzmarzyk, P.T.; Church, T.S.; Craig, C.L.; Bouchard, C. Sitting time and mortality from all causes, cardiovascular disease, and cancer. Med. Sci. Sport. Exerc. 2009, 41, 998–1005. [Google Scholar] [CrossRef]
- Healy, G.N.; Dunstan, D.W.; Salmon, J.; Cerin, E.; Shaw, J.E.; Zimmet, P.Z.; Owen, N. Breaks in sedentary time: Beneficial associations with metabolic risk. Diabetes Care 2008, 31, 661–666. [Google Scholar] [CrossRef] [Green Version]
- Peddie, M.C.; Bone, J.L.; Rehrer, N.J.; Skeaff, C.M.; Gray, A.R.; Perry, T.L. Breaking prolonged sitting reduces postprandial glycemia in healthy, normal-weight adults: A randomized crossover trial. Am. J. Clin. Nutr. 2013, 98, 358–366. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katzmarzyk, P.T. Physical activity, sedentary behavior, and health: Paradigm paralysis or paradigm shift? Diabetes 2010, 59, 2717–2725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsu, C.W.; Kang, Y.N.; Tseng, S.H. Effects of therapeutic exercise intensity on cerebral palsy outcomes: A systematic review with meta-regression of randomized clinical trials. Front. Neurol. 2019, 10, 657. [Google Scholar] [CrossRef]
- Cleary, S.L.; Taylor, N.F.; Dodd, K.J.; Shields, N. An aerobic exercise program for young people with cerebral palsy in specialist schools: A phase I randomized controlled trial. Dev. Neurorehabilit. 2017, 20, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Parent, A.; Raison, M.; Pouliot-Laforte, A.; Marois, P.; Maltais, D.B.; Ballaz, L. Impact of a short walking exercise on gait kinematics in children with cerebral palsy who walk in a crouch gait. Clin. Biomech. 2016, 34, 18–21. [Google Scholar] [CrossRef] [PubMed]
- Chappell, A.; Gibson, N.; Williams, G.; Allison, G.T.; Morris, S. Propulsion strategy in running in children and adolescents with cerebral palsy. Gait Posture 2019, 70, 305–310. [Google Scholar] [CrossRef]
- Noorkoiv, M.; Lavelle, G.; Theis, N.; Korff, T.; Kilbride, C.; Baltzopoulos, V.; Shortland, A.; Levin, W.; Ryan, J.M. Predictors of walking efficiency in children with cerebral palsy: Lower-body joint angles, moments, and power. Phys. Ther. 2019, 99, 711–720. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cleary, S.L.; Taylor, N.F.; Dodd, K.J.; Shields, N. A qualitative evaluation of an aerobic exercise program for young people with cerebral palsy in specialist schools. Dev. Neurorehabilit. 2017, 20, 339–346. [Google Scholar] [CrossRef]
- Tahayneh, M.; Humayra, S.; Fall, A.A.; Rosland, H.; Amro, A.; Mohammed, A.; Mohamed, A.L. Factors affecting mother’s adherence towards cerebral palsy home exercise program among children at Hebron and Bethlehem, Palestine. Int. J. Pharm. Res. 2020, 12, 1019–1024. [Google Scholar]
- Fauzi, A.A.; Khayat, M.M.; Sabirin, S.; Haron, N.; Mohamed, M.N.A.; Davis, G.M. Structured home-based exercise program for improving walking ability in ambulant children with cerebral palsy. J. Pediatr. Rehabil. Med. 2019, 12, 161–169. [Google Scholar] [CrossRef] [Green Version]
- Fauzi, A.A.; Khayat, M.M.; Haron, N.; Mahmud, S.; Sabirin, S. Structured home-based exercise program to improve ADL and participation among children with cerebral palsy. Ann. Phys. Rehabil. Med. 2018, 61, e319–e320. [Google Scholar] [CrossRef]
- Johnson, R.W.; Williams, S.A.; Gucciardi, D.F.; Bear, N.; Gibson, N. Can an online exercise prescription tool improve adherence to home exercise programmes in children with cerebral palsy and other neurodevelopmental disabilities? A randomised controlled trial. Br. Med. J. Open 2020, 10, e040108. [Google Scholar]
- Kim, S.H.; Shin, H.J.; Hahm, S.C.; Park, S.W.; Cho, H.Y.; Lee, M.G. The effect of a program combining resistance exercise and group exercise on balance, grip strength, and quality of life of children with cerebral palsy. J. Korean Soc. Phys. Med. 2020, 15, 75–85. [Google Scholar] [CrossRef]
- Ghadiri, F.; Sajjadi, H.R.; Bahmani, M.; Bahram, A. Effect of group resistance exercise with exciting music on spasticity, muscle strength and walking for children with cerebral palsy. Iran. J. Pediatr. Nurs. 2019, 6, 15–22. [Google Scholar]
- de Hollander, E.L.; Proper, K.I. Physical activity levels of adults with various physical disabilities. Prev. Med. Rep. 2018, 10, 370–376. [Google Scholar] [CrossRef] [PubMed]
- Komatireddy, R.; Chokshi, A.; Basnett, J.; Casale, M.; Goble, D.; Shubert, T. Quality and quantity of rehabilitation exercises delivered by a 3-D motion controlled camera: A pilot study. Int. J. Phys. Med. Rehabil. 2014, 2, 214. [Google Scholar] [CrossRef]
- Fasola, J.; Matarić, M.J. Socially assistive robot exercise coach: Motivating older adults to engage in physical exercise. Exp. Robot. 2013, 13, 463–479. [Google Scholar]
- Jafari, N.; Adams, K.; Tavakoli, M.; Wiebe, S.; Janz, H. Usability testing of a developed assistive robotic system with virtual assistance for individuals with cerebral palsy: A case study. Disabil. Rehabil. Assist. Technol. 2018, 13, 517–522. [Google Scholar] [CrossRef]
- Bainbridge, W.A.; Hart, J.W.; Kim, E.S.; Scassellati, B. The benefits of interactions with physically present robots over video-displayed agents. Int. J. Soc. Robot. 2011, 3, 41–52. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Body Functions | ||
|---|---|---|
| ID | Name | Definition |
| Ch 3/b3 | Voice and speech functions | Functions of producing sounds and speech. |
| Ch 7/b7 | Neuromusculoskeletal and movement-related functions | Functions of movement and mobility, including functions of joints, bones, reflexes and muscles. |
| Activities and participation | ||
| ID | Name | Definition |
| Ch 3/d3 | Communication | General and specific features of communicating by language, signs and symbols, including receiving and producing messages, carrying on conversations, and using communication devices and techniques. |
| Ch 4/d4 | Mobility | Moving by changing body position or location or by transferring from one place to another, by carrying, moving or manipulating objects, by walking, running or climbing, and by using various forms of transportation. |
| Subject | Gender | Age | CFCS | MACS | GMFCS |
|---|---|---|---|---|---|
| C01 | F | 18 | III | IV | V |
| C02 | M | 6 | III | III | II |
| C03 | M | 15 | III | IV | V |
| C04 | M | 8 | III | IV | V |
| C05 | M | 18 | I | I | IV |
| C06 | F | 18 | I | II | III |
| C07 | F | 19 | III | V | V |
| C08 | F | 19 | I | III | III |
| C09 | M | 18 | II | III | IV |
| C10 | M | 12 | IV | IV | IV |
| C11 | M | 14 | III | V | V |
| C12 | M | 17 | IV | IV | V |
| C13 | F | 18 | I | II | III |
| C14 | F | 19 | II | II | II |
| C15 | F | 19 | III | III | II |
| C16 | M | 10 | IV | III | II |
| C17 | M | 20 | V | III | II |
| C18 | F | 18 | IV | V | V |
| C19 | F | 21 | III | IV | V |
| C20 | M | 14 | I | III | III |
| ICF | ||||||
|---|---|---|---|---|---|---|
| MAC and GMFCS | CFCS | |||||
| Subject | Gender | Age | Ch. 7/b7 (Neuromusculoskeletal and Movement-Related Functions) | Ch. 4/d4 (Mobitliy) | Ch. 3/b3 (Voice and Speech Functions) | Ch. 3/d3 (Communication) |
| A01 | F | 51 | III | III | IV | III |
| A02 | F | 27 | IV | IV | IV | IV |
| A03 | M | 32 | IV | III | II | III |
| A04 | F | 36 | IV | III | I | II |
| A05 | F | 33 | IV | V | IV | IV |
| A06 | M | 50 | V | IV | III | IV |
| A07 | M | 58 | IV | V | III | III |
| A08 | M | 24 | V | V | IV | IV |
| A09 | F | 49 | IV | IV | I | II |
| A10 | M | 35 | III | III | IV | III |
| A11 | F | 35 | IV | IV | III | III |
| A12 | M | 42 | IV | IV | I | II |
| A13 | M | 46 | III | III | III | III |
| A14 | M | 43 | IV | III | IV | IV |
| A15 | F | 51 | IV | V | IV | V |
| A16 | F | 28 | IV | IV | IV | IV |
| A17 | F | 26 | IV | III | I | III |
| A18 | F | 33 | IV | IV | IV | IV |
| A19 | M | 26 | V | V | IV | IV |
| A20 | F | 35 | IV | V | III | IV |
| ID | Question |
|---|---|
| 1 | Sex. |
| 2 | Age. |
| 3 | Family environment. |
| 4 | Do you do physical activity? (Yes/No). If so, please continue with the survey, otherwise, you have just finished. |
| 5 | Indicate how often do you workout (number of days and sessions a week). |
| 6 | How long does the session usually take? (min) |
| 7 | Select its intensity (Light, Moderate, Vigorous). |
| 8 | Where do you usually do exercise? (At home, at a specific center, outdoors, others) |
| 9 | What is the purpose of your physical activity? (Rehabilitation, personal choice, both) |
| 10 | Score your motivation to do physical activity. (I do not like it at all, I do not like it, Neutral, I like it, I like it very much) |
| 11 | Do you use any kind of supporting device or gadget to do the activity? If so, please describe it. |
| 12 | Do you use any kind of software to do exercise? If so, please describe it. |
| 13 | Please give any further information you consider relevant for this survey. |
| Gender | ||||
|---|---|---|---|---|
| Sample | Male | Female | ||
| Survey Questions | Possible Answers | N | N | N |
| Never | 2 | 2 | 0 | |
| Once per week | 24 | 11 | 13 | |
| Frequency of PA | Twice per week | 7 | 4 | 3 |
| (5) | Three times per week | 2 | 1 | 1 |
| More than three times per week | 5 | 2 | 3 | |
| Intensity | Light | 22 | 10 | 12 |
| (7) | Moderate | 16 | 8 | 8 |
| Type of activity | Rehabilitation | 29 | 15 | 14 |
| (9) | RHB and personal choice | 9 | 3 | 6 |
| I like it very much | 4 | 2 | 2 | |
| I like it | 19 | 10 | 9 | |
| Motivation | Neutral | 9 | 4 | 5 |
| (10) | I do not like | 5 | 3 | 2 |
| I do not like at all | 3 | 1 | 2 | |
| Level | Activities | ||||
|---|---|---|---|---|---|
| I | Crawling, running, shuttle-run game, dancing, martial arts, skating, playing table tennis. | ||||
| II | Football, videogames (Nintendo’s Wii controller and Wii-Fit Balance Board). | ||||
| III | Sit-to-stand, step up-down, squatting, walking (free, gait, elliptical, treadmill), elastic bands for training upper limbs, swimming, playing videogames (Microsoft Kinect). | ||||
| IV | Strengthening of knee extensor, hip flexor, and ankle dorsiflexors, physio-ball exercises, universal exercise unit, feet ergometer, cycling using adapted bikes, wheelchair hockey, gymnastics, animal therapy. | ||||
| V | Virtual-reality games. | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Molina-Cantero, A.J.; Merino-Monge, M.; Castro-García, J.A.; Pousada-García, T.; Valenzuela-Muñoz, D.; Gutiérrez-Párraga, J.; López-Álvarez, S.; Gómez-González, I.M. A Study on Physical Exercise and General Mobility in People with Cerebral Palsy: Health through Costless Routines. Int. J. Environ. Res. Public Health 2021, 18, 9179. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179179
Molina-Cantero AJ, Merino-Monge M, Castro-García JA, Pousada-García T, Valenzuela-Muñoz D, Gutiérrez-Párraga J, López-Álvarez S, Gómez-González IM. A Study on Physical Exercise and General Mobility in People with Cerebral Palsy: Health through Costless Routines. International Journal of Environmental Research and Public Health. 2021; 18(17):9179. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179179
Chicago/Turabian StyleMolina-Cantero, Alberto J., Manuel Merino-Monge, Juan A. Castro-García, Thais Pousada-García, David Valenzuela-Muñoz, Juan Gutiérrez-Párraga, Setefilla López-Álvarez, and Isabel M. Gómez-González. 2021. "A Study on Physical Exercise and General Mobility in People with Cerebral Palsy: Health through Costless Routines" International Journal of Environmental Research and Public Health 18, no. 17: 9179. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179179