
A Cluster-Randomised Crossover Pilot Feasibility Study of a Multicomponent Intervention to Reduce Occupational Sedentary Behaviour in Professional Male Employees


Abstract
:1. Introduction
2. Materials and Methods
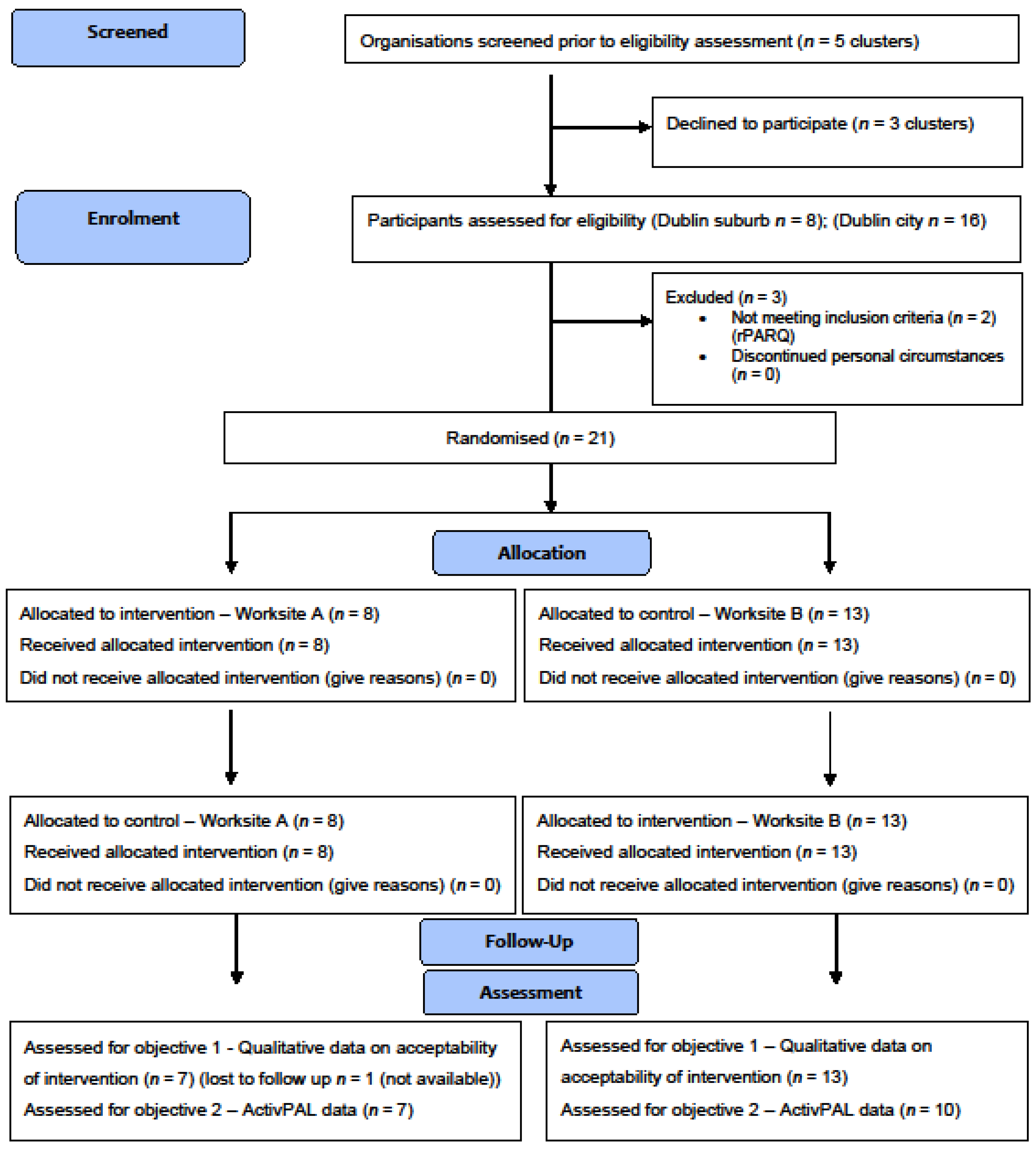
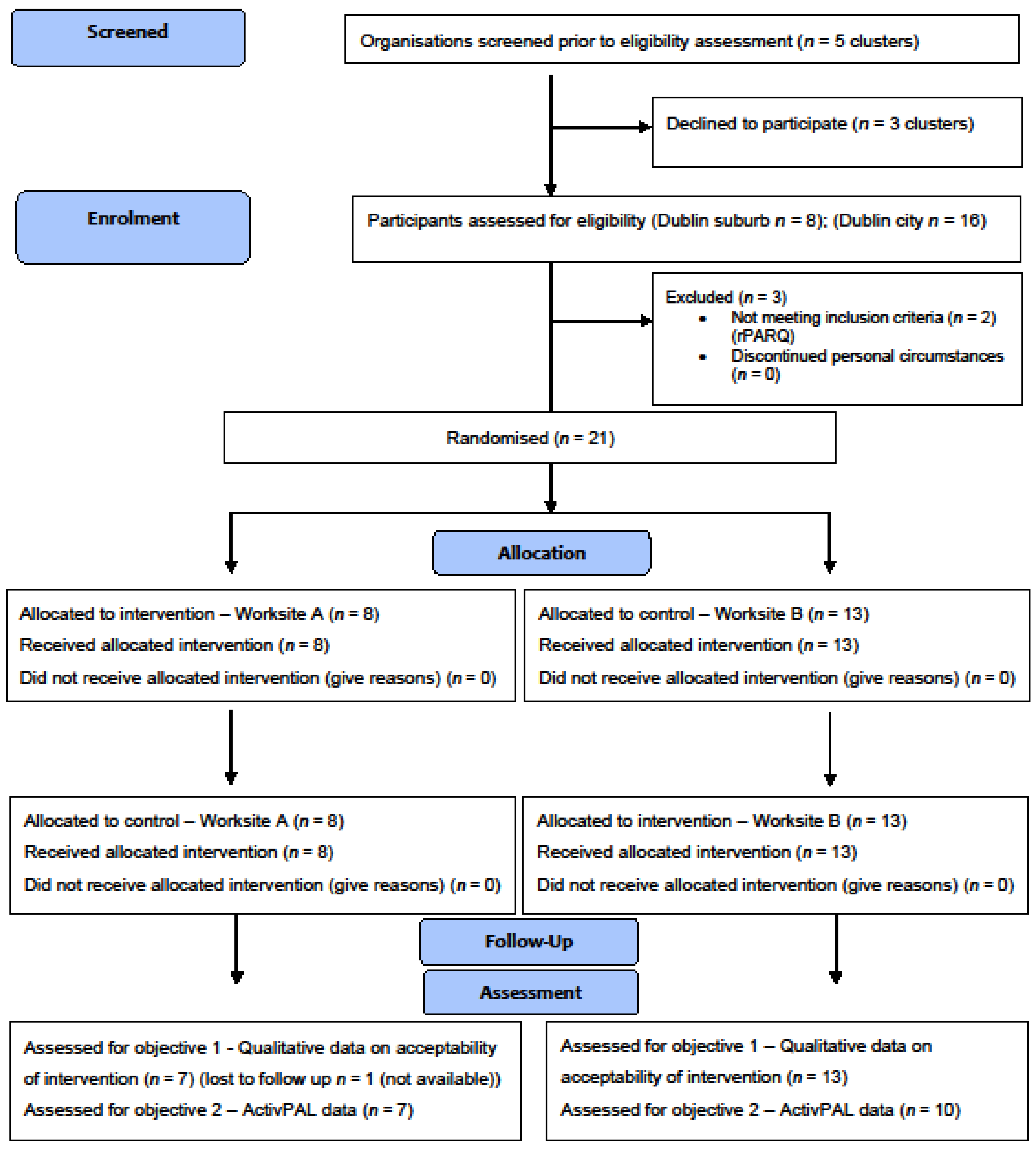
2.1. Participants
- Females
- Aged under 18 years
- Those with contraindications or limitations to physical activity as indicated by the Physical Activity Readiness Questionnaire [49]
- Those without a personal desk
- Those who planned to be absent from the workplace for more than two days in one week during the study period
- Those who were involved in another sedentary behaviour reduction programme or intervention.
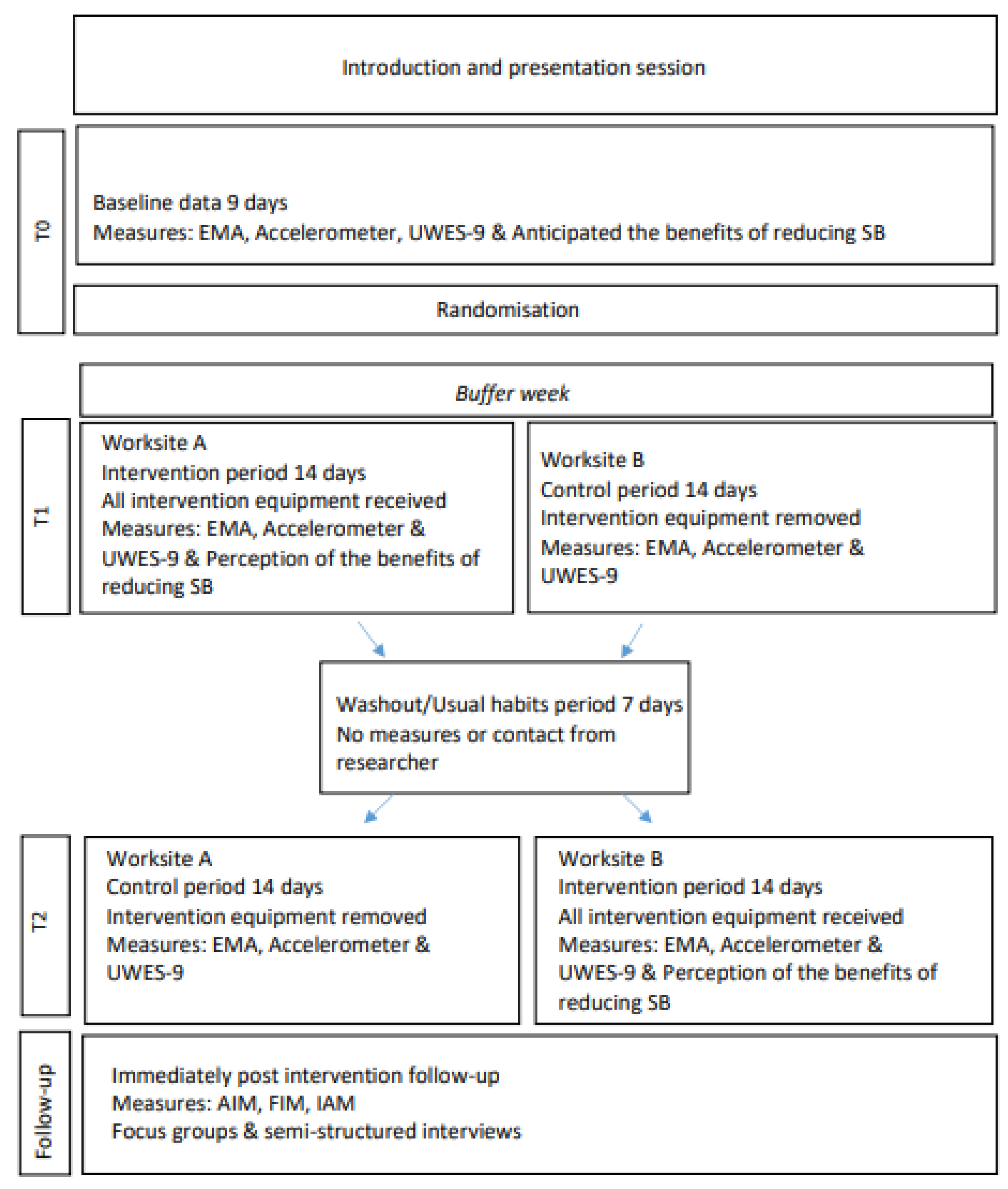
2.2. Study Design and Procedures
2.3. Intervention Description of ‘Cycle at Work’
2.4. Primary Outcomes—Acceptability and Feasibility
2.5. Secondary Outcomes
2.5.1. Sedentary Behaviour, Standing, Physical Activity
- Total sedentary behaviour: waking hours
- Total sedentary behaviour: work hours
- Total physical activity: waking hours
- Total physical activity: work hours
- Pedalling time: work hours
2.5.2. Work Engagement
2.5.3. Anticipated/Perceived Intervention Benefits
2.6. Qualitative Analyses
2.7. Quantitative Analyses
2.8. Progression Criteria to Full cRCT
- Green—≥80% of participants achieved >60% of their pedalling goal
- Amber—60–79% of participants achieved >60% of their pedalling goal
- Red—<60% of participants achieved >60% of their pedalling goal.
- Green—≥80% participants provided main trial-related outcomes (SB/PA) at T2
- Amber—60–79% of participants provided main trial-related outcomes at T2
- Red—<60% of participants provided main trial-related outcomes at T2.
3. Results
3.1. Feasibility
3.2. Acceptability
3.3. Acceptability of Measures—Ecological Momentary Assessment
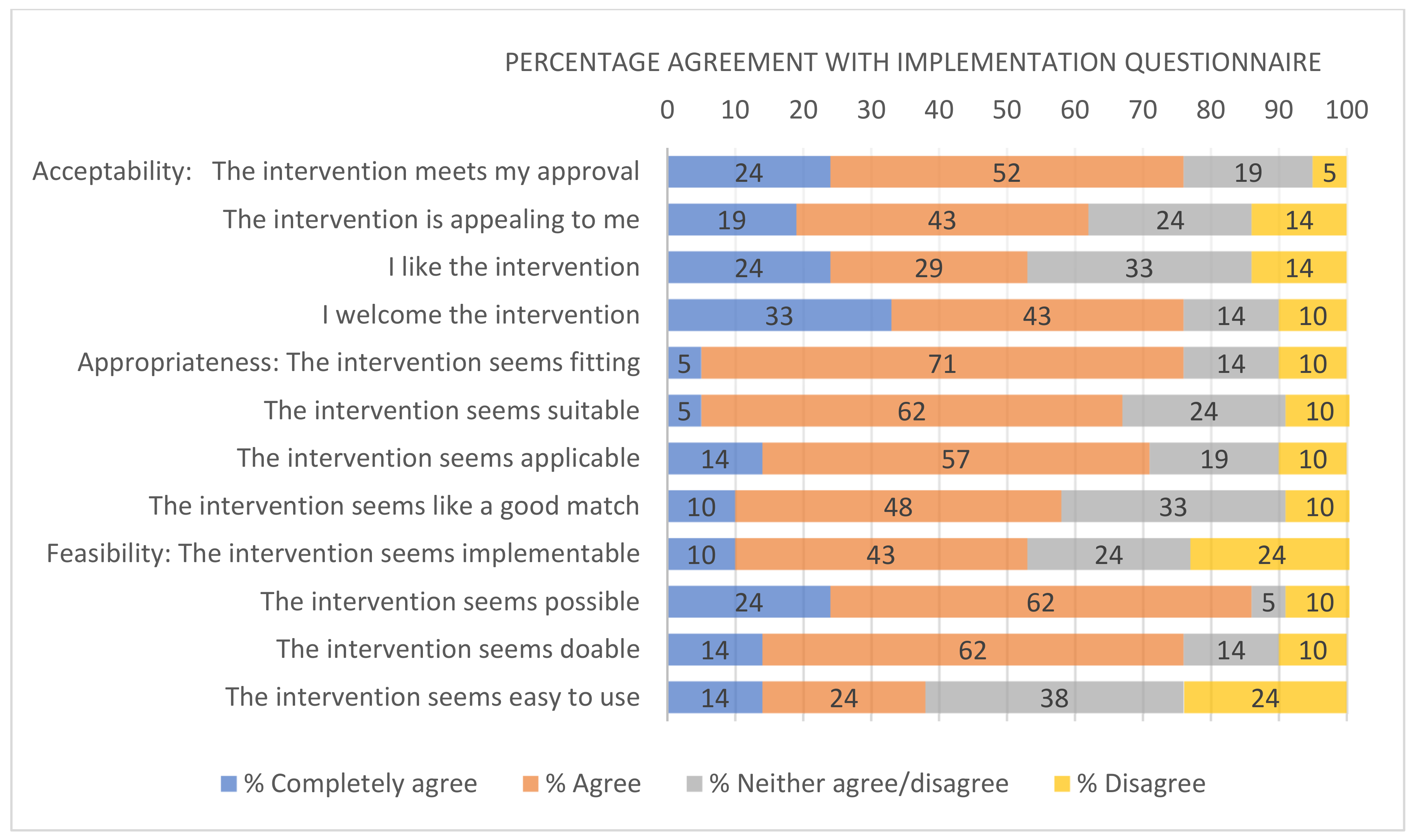
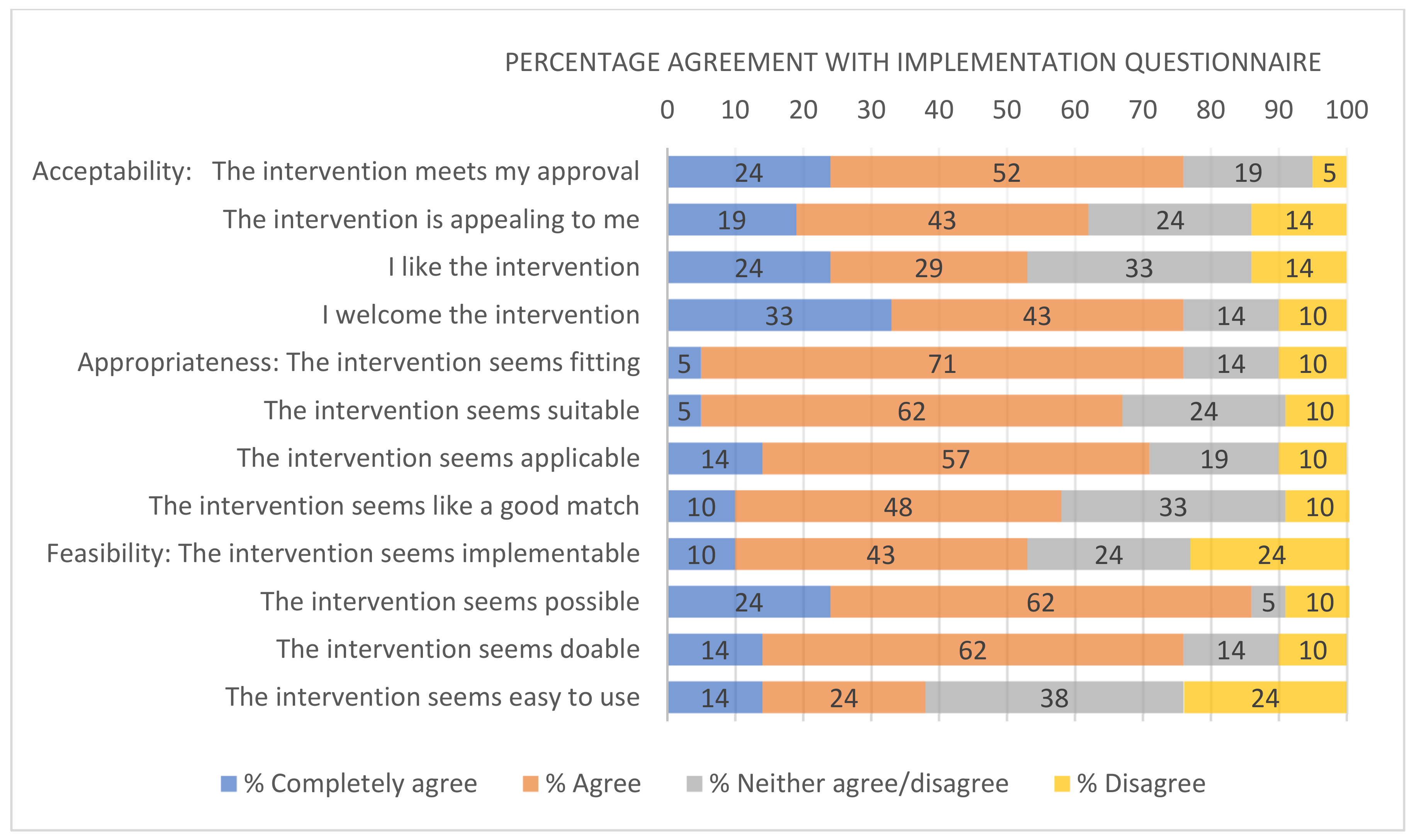
3.4. Acceptability, Appropriateness and Feasibility Questionnaire
3.5. Sedentary Behaviour, Standing and Physical Activity
3.6. Work Engagement
3.7. Anticipated and Perceived Intervention Benefits of the Intervention
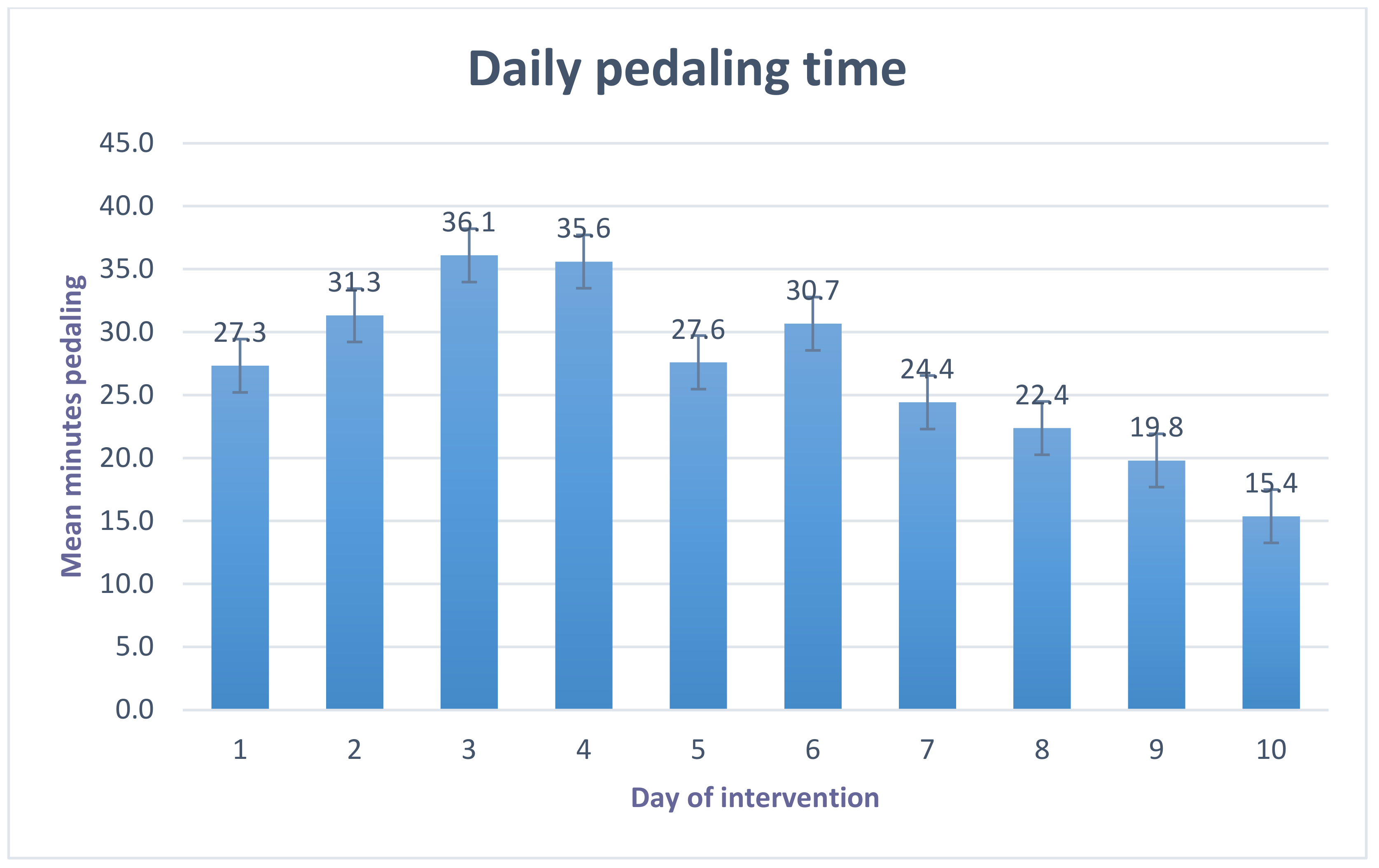
3.8. Pedaling Activity and Adherence to the Protocol
3.9. Progression Criteria
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chau, J.Y.; Grunseit, A.C.; Chey, T.; Stamatakis, E.; Brown, W.J.; Matthews, C.E.; Bauman, A.E.; Van Der Ploeg, H.P. Daily sitting time and all-cause mortality: A meta-analysis. PLoS ONE 2013, 8, e80000. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ihira, H.; Sawada, N.; Yamaji, T.; Goto, A.; Shimazu, T.; Kikuchi, H.; Inoue, S.; Inoue, M.; Iwasaki, M.; Tsugane, S.; et al. Occupational sitting time and subsequent risk of cancer: The Japan Public Health Center-based Prospective Study. Cancer Sci. 2020, 111, 974–984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnsson, A.; Broberg, P.; Johnsson, A.; Tornberg, Å.B.; Olsson, H. Occupational sedentariness and breast cancer risk. Acta Oncol. 2017, 56, 75–80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicolson, G.; Hayes, C.; Darker, C. Examining total and domain-specific sedentary behaviour using the socio-ecological model—A cross-sectional study of Irish adults. BMC Public Health 2019, 19, 1155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quintiliani, L.; Sattelmair, J.; Sorensen, G. The Workplace as a Setting for Interventions to Improve Diet and Promote Physical Activity; Background Paper Prepared for the WHO/WEF Joint Event on Preventing Noncommunicable Diseases in the Workplace, Dalian, China; WHO: Geneva, Switzerland, 2007. [Google Scholar]
- Owen, N.; Sugiyama, T.; Eakin, E.E.; Gardiner, P.A.; Tremblay, M.S.; Sallis, J.F. Adults’ sedentary behavior: Determinants and interventions. Am. J. Prev. Med. 2011, 41, 189–196. [Google Scholar] [CrossRef] [PubMed]
- Gardner, B.; Smith, L.; Lorencatto, F.; Hamer, M.; Biddle, S.J. How to reduce sitting time? A review of behaviour change strategies used in sedentary behaviour reduction interventions among adults. Health Psychol. Rev. 2015, 7199, 89–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tosi, H.L.; Locke, E.A.; Latham, G.P. A Theory of Goal Setting and Task Performance. Acad. Manag. Rev. 1991, 16, 480. [Google Scholar] [CrossRef]
- Gardner, B.; Rebar, A.L.; Gardner, B.; Rebar, A.L. Habit Formation and Behavior Change. Oxford Res. Encycl. Psychol. 2019. [Google Scholar] [CrossRef]
- Hermsen, S.; Frost, J.; Renes, R.J.; Kerkhof, P. Using feedback through digital technology to disrupt and change habitual behavior: A critical review of current literature. Comput. Human Behav. 2016, 57, 61–74. [Google Scholar] [CrossRef] [Green Version]
- Turner-McGrievy, G.M.; Beets, M.W.; Moore, J.B.; Kaczynski, A.T.; Barr-Anderson, D.J.; Tate, D.F. Comparison of traditional versus mobile app self-monitoring of physical activity and dietary intake among overweight adults participating in an mHealth weight loss program. J. Am. Med. Inform. Assoc. 2013, 20, 513–518. [Google Scholar] [CrossRef]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef]
- Van Dantzig, S.; Geleijnse, G.; Van Halteren, A.T. Toward a persuasive mobile application to reduce sedentary behavior. Pers. Ubiquitous Comput. 2013, 17, 1237–1246. [Google Scholar] [CrossRef]
- Bond, D.S.; Thomas, J.G.; Raynor, H.A.; Moon, J.; Sieling, J.; Trautvetter, J.; Leblond, T.; Wing, R.R. B-MOBILE—A smartphone-based intervention to reduce sedentary time in overweight/obese individuals: A within-subjects experimental trial. PLoS ONE 2014, 9, e100821. [Google Scholar] [CrossRef]
- Pedersen, S.J.; Cooley, P.D.; Mainsbridge, C. An e-health intervention designed to increase workday energy expenditure by reducing prolonged occupational sitting habits. Work 2014, 49, 289–295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swartz, A.M.; Rote, A.E.; Welch, W.A.; Maeda, H.; Hart, T.L.; Cho, Y.I.; Strath, S.J. Prompts to Disrupt Sitting Time and Increase Physical Activity at Work, 2011–2012. Prev. Chronic Dis. 2014, 11, 130318. [Google Scholar] [CrossRef] [Green Version]
- Evans, J.M.M.; Connelly, J.; Jepson, R.; Gray, C.; Shepherd, A.; Mackison, D. A physical activity intervention in a Bingo club: Significance of the setting. Health Educ. J. 2018, 77, 377–384. [Google Scholar] [CrossRef]
- Bergouignan, A.; Rudwill, F.; Simon, C.; Blanc, S. Physical inactivity as the culprit of metabolic inflexibility: Evidence from bed-rest studies. J. Appl. Physiol. 2011, 111, 1201–1210. [Google Scholar] [CrossRef] [PubMed]
- Healy, G.N.; Dunstan, D.W.; Salmon, J.; Cerin, E.; Shaw, J.; Zimmet, P.; Owen, N. Breaks in Sedentary Time: Beneficial associations with metabolic risk. Diabetes Care 2008, 31, 661–666. [Google Scholar] [CrossRef] [Green Version]
- Healy, G.N.; Matthews, C.E.; Dunstan, D.W.; Winkler, E.A.H.; Owen, N. Sedentary time and cardio-metabolic biomarkers in US adults: NHANES 200306. Eur. Heart J. 2011, 32, 590–597. [Google Scholar] [CrossRef]
- Rynders, C.A.; Blanc, S.; Dejong, N.; Bessesen, D.H.; Bergouignan, A. Sedentary behaviour is a key determinant of metabolic inflexibility. J. Physiol. 2018, 596, 1319–1330. [Google Scholar] [CrossRef] [PubMed]
- Peachey, M.M.; Richardson, J.; Tang, A.V.; Dal-Bello Haas, V.; Gravesande, J. Environmental, behavioural and multicomponent interventions to reduce adults’ sitting time: A systematic review and meta-analysis. Br. J. Sports Med. 2018, 54, 315–325. [Google Scholar] [CrossRef]
- Chu, A.H.Y.; Ng, S.H.X.; Tan, C.S.; Win, A.M.; Koh, D.; Müller-Riemenschneider, F.; Muller-Riemenschneider, F. A systematic review and meta-analysis of workplace intervention strategies to reduce sedentary time in white-collar workers. Obes. Rev. 2016, 17, 467–481. [Google Scholar] [CrossRef] [PubMed]
- Tremblay, M.S.; Aubert, S.; Barnes, J.D.; Saunders, T.J.; Carson, V.; Latimer-Cheung, A.E.; Chastin, S.F.M.; Altenburg, T.M.; Chinapaw, M.J.M.; Aminian, S.; et al. Sedentary Behavior Research Network (SBRN)—Terminology Consensus Project process and outcome. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 75. [Google Scholar] [CrossRef] [Green Version]
- Powell, C.; Browne, L.D.; Carson, B.P.; Dowd, K.P.; Perry, I.J.; Kearney, P.M.; Harrington, J.M.; Donnelly, A.E. Use of Compositional Data Analysis to Show Estimated Changes in Cardiometabolic Health by Reallocating Time to Light-Intensity Physical Activity in Older Adults. Sports Med. 2019, 50, 205–217. [Google Scholar] [CrossRef] [PubMed]
- Bailey, D.P.; Locke, C.D. Breaking up prolonged sitting with light-intensity walking improves postprandial glycemia, but breaking up sitting with standing does not. J. Sci. Med. Sport 2015, 18, 294–298. [Google Scholar] [CrossRef]
- Ojo, S.O.; Bailey, D.P.; Brierley, M.L.; Hewson, D.J.; Chater, A.M. Breaking barriers: Using the behavior change wheel to develop a tailored intervention to overcome workplace inhibitors to breaking up sitting time. BMC Public Health 2019, 19, 1126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waters, T.R.; Dick, R.B. Evidence of health risks associated with prolonged standing at work and intervention effectiveness. Rehabil. Nurs. 2015, 40, 148–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brand, F.N.; Dannenberg, A.L.; Abbott, R.D.; Kannel, W.B. The epidemiology of varicose veins: The Framingham Study. Am. J. Prev. Med. 1988, 4, 96–101. [Google Scholar] [CrossRef]
- Rempel, D.; Krause, N. Do Sit–Stand Workstations Improve Cardiovascular Health? J. Occup. Environ. Med. 2018, 60, 319–320. [Google Scholar]
- Mansoubi, M.; Pearson, N.; Clemes, S.A.; Biddle, S.J.H.; Bodicoat, D.H.; Tolfrey, K.; Edwardson, C.L.; Yates, T. Energy expenditure during common sitting and standing tasks: Examining the 1.5 MET definition of sedentary behaviour. BMC Public Health 2015, 15, 516. [Google Scholar] [CrossRef] [Green Version]
- Chaput, J.P.; Saunders, T.J.; Tremblay, M.S.; Katzmarzyk, P.T.; Tremblay, A.; Bouchard, C. Workplace standing time and the incidence of obesity and type 2 diabetes: A longitudinal study in adults. BMC Public Health 2015, 15, 111. [Google Scholar] [CrossRef] [Green Version]
- Carr, L.J.; Swift, M.; Ferrer, A.; Benzo, R. Cross-sectional Examination of Long-term Access to Sit-Stand Desks in a Professional Office Setting. Am. J. Prev. Med. 2016, 50, 96–100. [Google Scholar] [CrossRef]
- Carr, L.J.; Walaska, K.A.; Marcus, B.H. Feasibility of a portable pedal exercise machine for reducing sedentary time in the workplace. Br. J. Sports Med. 2012, 46, 430–435. [Google Scholar] [CrossRef] [PubMed]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. 2011 Compendium of Physical Activities: A Second Update of Codes and MET Values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef] [Green Version]
- Loh, R.; Stamatakis, E.; Folkerts, D.; Allgrove, J.E.; Moir, H.J. Effects of Interrupting Prolonged Sitting with Physical Activity Breaks on Blood Glucose, Insulin and Triacylglycerol Measures: A Systematic Review and Meta-analysis. Sports Med. 2020, 50, 295–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benatti, F.B.; Ried-Larsen, M. The Effects of Breaking up Prolonged Sitting Time: A Review of Experimental Studies. Med. Sci. Sports Exerc. 2015, 47, 2053–2061. [Google Scholar] [CrossRef] [Green Version]
- Keegan, R.; Middleton, G.; Henderson, H.; Girling, M. Auditing the socio-environmental determinants of motivation towards physical activity or sedentariness in work-aged adults: A qualitative study. BMC Public Health 2016, 16, 1–20. [Google Scholar] [CrossRef] [Green Version]
- Hadgraft, N.T.; Winkler, E.A.H.H.; Healy, G.N.; Lynch, B.M.; Neuhaus, M.; Eakin, E.G.; Dunstan, D.W.; Owen, N.; Fjeldsoe, B.S. Intervening to reduce workplace sitting: Mediating role of social-cognitive constructs during a cluster randomised controlled trial. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Such, E.; Mutrie, N. Using organisational cultural theory to understand workplace interventions to reduce sedentary time. Int. J. Health Promot. Educ. 2017, 55, 18–29. [Google Scholar] [CrossRef] [Green Version]
- Bottorff, J.L.; Seaton, C.L.; Johnson, S.T.; Caperchione, C.M.; Oliffe, J.L.; More, K.; Jaffer-Hirji, H.; Tillotson, S.M. An Updated Review of Interventions that Include Promotion of Physical Activity for Adult Men. Sport. Med. 2015, 45, 775–800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Regional Committee for Europe Strategy on the health and well-being of men in the WHO European Region (17–20 September 2018). 2018. Available online: http://www.euro.who.int/__data/assets/pdf_file/0003/378165/68wd12e_MensHealthStrategy_180480.pdf? (accessed on 1 February 2019).
- Johnson, S.T.; Stolp, S.; Seaton, C.; Sharp, P.; Caperchione, C.M.; Bottorff, J.L.; Oliffe, J.L.; Jones-Bricker, M.; Lamont, S.; Medhurst, K.; et al. A Men’s Workplace Health Intervention. J. Occup. Environ. Med. 2016, 58, 765–769. [Google Scholar] [CrossRef] [Green Version]
- Patzelt, C.; Heim, S.; Deitermann, B.; Theile, G.; Krauth, C.; Hummers-Pradier, E.; Walter, U. Reaching the Elderly: Understanding of health and preventive experiences for a tailored approach—Results of a qualitative study. BMC Geriatr. 2016, 16, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Michie, S.; Ashford, S.; Sniehotta, F.F.; Dombrowski, S.U.; Bishop, A.; French, D.P. A refined taxonomy of behaviour change techniques to help people change their physical activity and healthy eating behaviours: The CALO-RE taxonomy. Psychol. Health 2011, 26, 1479–1498. [Google Scholar] [CrossRef]
- The WHO Regional Office For Europe. The Health and Well-Being of Men in the WHO European Region: Better Health through a Gender Approach. 2018. Available online: https://apps.who.int/iris/handle/10665/329686 (accessed on 1 February 2019).
- Yardley, L.; Ainsworth, B.; Arden-Close, E.; Muller, I. The person-based approach to enhancing the acceptability and feasibility of interventions. Pilot Feasibility Stud. 2015, 1, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. Int. J. Nurs. Stud. 2013, 50, 587–592. [Google Scholar] [CrossRef] [Green Version]
- Cardinal, B.J.; Esters, J.; Cardinal, M.K. Evaluation of the revised physical activity readiness questionnaire in older adults. Med. Sci. Sports Exerc. 1996, 28, 468–472. [Google Scholar] [CrossRef]
- Nicolson, G.H.; Hayes, C.; Darker, C. A theory-based multicomponent intervention to reduce occupational sedentary behaviour in professional male workers: Protocol for a cluster randomised crossover pilot feasibility study. Pilot Feasibility Stud. 2020, 6, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Schaufeli, W.; Bakker, A. UWES: Utrecht Work Engagement Scale. 2004. Available online: https://0-journals-sagepub-com.brum.beds.ac.uk/doi/10.1177/0013164405282471 (accessed on 13 March 2019).
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348, 1687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eldridge, S.M.; Chan, C.L.; Campbell, M.J.; Bond, C.M.; Hopewell, S.; Thabane, L.; Lancaster, G.A.; O’Cathain, A.; Altman, D.; Bretz, F.; et al. CONSORT 2010 statement: Extension to randomised pilot and feasibility trials. Pilot Feasibility Stud. 2016, 2, i5239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiner, B.J.; Lewis, C.C.; Stanick, C.; Powell, B.J.; Dorsey, C.N.; Clary, A.S.; Boynton, M.H.; Halko, H. Psychometric assessment of three newly developed implementation outcome measures. Implement. Sci. 2017, 12, 1–12. [Google Scholar] [CrossRef]
- Edwardson, C.L.; Winkler, E.A.H.; Bodicoat, D.H.; Yates, T.; Davies, M.J.; Dunstan, D.W.; Healy, G.N. Considerations when using the activPAL monitor in field-based research with adult populations. J. Sport Health Sci. 2017, 6, 162–178. [Google Scholar] [CrossRef] [Green Version]
- Engelen, L.; Chau, J.Y.; Burks-Young, S.; Bauman, A. Application of ecological momentary assessment in workplace health evaluation. Health Promot. J. Aust. 2016, 27, 259–263. [Google Scholar] [CrossRef]
- Maher, J.P.; Rebar, A.L.; Dunton, G.F. Ecological momentary assessment is a feasible and valid methodological tool to measure older adults’ physical activity and sedentary behavior. Front. Psychol. 2018, 9, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Hallingberg, B.; Turley, R.; Segrott, J.; Wight, D.; Craig, P.; Moore, L.; Murphy, S.; Robling, M.; Simpson, S.A.; Moore, G. Exploratory studies to decide whether and how to proceed with full-scale evaluations of public health interventions: A systematic review of guidance. Pilot Feasibility Stud. 2018, 4, 104. [Google Scholar] [CrossRef] [PubMed]
- O’Dolan, C.; Grant, M.; Lawrence, M.; Dall, P. A randomised feasibility study to investigate the impact of education and the addition of prompts on the sedentary behaviour of office workers. Pilot Feasibility Stud. 2018, 4, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Kozey-Keadle, S.; Libertine, A.; Staudenmayer, J.; Freedson, P. The feasibility of reducing and measuring sedentary time among overweight, non-exercising office workers. J. Obes. 2012, 2012. [Google Scholar] [CrossRef] [Green Version]
- Leon, A.C.; Davis, L.L.; Kraemer, H.C. The Role and Interpretation of Pilot Studies in Clinical Research. J. Psychiatr. Res. 2012, 45, 626–629. [Google Scholar] [CrossRef] [Green Version]
- Trost, S.G.; Mciver, K.L.; Pate, R.R. Conducting accelerometer-based activity assessments in field-based research. Med. Sci. Sports Exerc. 2005, 37, 531–543. [Google Scholar] [CrossRef] [PubMed]
- Eldridge, S.; Chan, C.; Campbell, M.; Bond, C.; Hopewell, S.; Thabane, L.; Lancaster, G. CONSORT extension for Pilot and Feasibility Trials Checklist. BMJ 2016, 355, i5239. [Google Scholar]
- Eldridge, S.M.; Costelloe, C.E.; Kahan, B.C.; Lancaster, G.A.; Kerry, S.M. How big should the pilot study for my cluster randomised trial be? Stat. Methods Med. Res. 2015, 25, 1039–1056. [Google Scholar] [CrossRef]
- Avery, K.N.L.; Williamson, P.R.; Gamble, C.; Francischetto, E.O.C.; Metcalfe, C.; Davidson, P.; Williams, H.; Blazeby, J.M.; Blencowe, N.; Bugge, C.; et al. Informing efficient randomised controlled trials: Exploration of challenges in developing progression criteria for internal pilot studies. BMJ Open 2017, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goyder, E.; Hind, D.; Breckon, J.; Dimairo, M.; Minton, J.; Everson-Hock, E.; Read, S.; Copeland, R.; Crank, H.; Horspool, K.; et al. A randomised controlled trial and cost-effectiveness evaluation of “booster” interventions to sustain increases in physical activity in middle-aged adults in deprived urban neighbourhoods. Health Technol. Assess. 2014, 18, 1–209. [Google Scholar] [CrossRef]
- Peterman, J.E.; Morris, K.L.; Kram, R.; Byrnes, W.C. Cardiometabolic Effects of a Workplace Cycling Intervention. J. Phys. Act. Health 2019, 16, 547–555. [Google Scholar] [CrossRef]
- Duncan, M.J.; Gilson, N.; Vandelanotte, C. Which population groups are most unaware of CVD risks associated with sitting time? Prev. Med. 2014, 65, 103–108. [Google Scholar] [CrossRef]
- Brakenridge, C.L.; Fjeldsoe, B.S.; Young, D.C.; Winkler, E.A.H.; Dunstan, D.W.; Straker, L.M.; Healy, G.N. Evaluating the effectiveness of organisational-level strategies with or without an activity tracker to reduce office workers’ sitting time: A cluster-randomised trial. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 1–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richardson, N.; Carroll, P.; Harrison, M.; Donohoe, A.; Keohane, A.; Robertson, S.; Kelly, L. An investigation of a community based physical activity intervention for adult men, ‘Men on the Move’. Eur. J. Public Health 2017, 27, 2017. [Google Scholar] [CrossRef] [Green Version]
- Wyke, S.; Hunt, K.; Gray, C.M.; Fenwick, E.; Bunn, C.; Donnan, P.T.; Rauchhaus, P.; Mutrie, N.; Anderson, A.S.; Boyer, N.; et al. Football Fans in Training (FFIT): A randomised controlled trial of a gender-sensitised weight loss and healthy living programme for men—end of study report. Public Health Res. 2015, 3, 1–130. [Google Scholar] [CrossRef] [Green Version]
- Ojo, S.O.; Bailey, D.P.; Hewson, D.J.; Chater, A.M. Perceived Barriers and Facilitators to Breaking Up Sitting Time among Desk-Based Office Workers: A Qualitative Investigation Using the TDF and COM-B. Int. J. Environ. Res. Public Health 2019, 16, 2903. [Google Scholar] [CrossRef] [Green Version]
- Hadgraft, N.T.; Brakenridge, C.L.; LaMontagne, A.D.; Fjeldsoe, B.S.; Lynch, B.M.; Dunstan, D.W.; Owen, N.; Healy, G.N.; Lawler, S.P. Feasibility and acceptability of reducing workplace sitting time: A qualitative study with Australian office workers. BMC Public Health 2016, 16. [Google Scholar] [CrossRef] [Green Version]
- Mackenzie, K.; Such, E.; Norman, P.; Goyder, E. Sitting less at work: A qualitative study of barriers and enablers in organisations of different size and sector. BMC Public Health 2019, 19, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Bagozzi, R.P.; Lee, K.H. Multiple routes for social influence: The role of compliance, internalization, and social identity. Soc. Psychol. Q. 2002, 65, 226–247. [Google Scholar] [CrossRef]
- Bredahl, T.V.G.; Særvoll, C.A.; Kirkelund, L.; Sjøgaard, G.; Andersen, L.L. When Intervention Meets Organisation, a Qualitative Study of Motivation and Barriers to Physical Exercise at the Workplace. Sci. World J. 2015, 2015, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Dutta, N.; Walton, T.; Pereira, M.A. Experience of switching from a traditional sitting workstation to a sit-stand workstation in sedentary office workers. Work 2015, 52, 83–89. [Google Scholar] [CrossRef]
- Carey, R.N.; Johnston, M.; Bruin, M.D.; Kelly, M.P. Behavior Change Techniques and Their Mechanisms of Action: A Synthesis of Links Described in Published Intervention Literature. Ann. Behav. Med. 2018, 53, 693–707. [Google Scholar]
- Duncan, M.; Vandelanotte, C.; Kolt, G.S.; Rosenkranz, R.R.; Cristina, M.; Duncan, M. Effectiveness of a web-and mobile phone-based intervention to promote physical activity and healthy eating in middle-aged males: Randomized controlled trial of the ManUp study. J. Med. Internet Res. 2014, 16, e3107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buckingham, S.A.; Williams, A.J.; Morrissey, K.; Price, L.; Harrison, J. Mobile health interventions to promote physical activity and reduce sedentary behaviour in the workplace: A systematic review. Digit. Health 2019, 5, 205520761983988. [Google Scholar] [CrossRef] [Green Version]
- Hunter, J.R.; Gordon, B.A.; Bird, S.R.; Benson, A.C. Perceived barriers and facilitators to workplace exercise participation. Int. J. Workplace Health Manag. 2018, 11, 349–363. [Google Scholar] [CrossRef]
- Carr, L.J.; Karvinen, K.; Peavler, M.; Smith, R.; Cangelosi, K. Multicomponent intervention to reduce daily sedentary time: A randomised controlled trial. BMJ Open 2013, 3, e003261. [Google Scholar] [CrossRef] [Green Version]
- Anderson, A.; Thornton, O.; Coats, R.; Capozio, A.; Astill, S. The effect of using a cycling workstation on mouse dexterity. PLoS ONE 2019, 14, e0220896. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, R.; Coenen, P.; Howie, E.; Williamson, A.; Straker, L. The short term musculoskeletal and cognitive effects of prolonged sitting during office computer work. Int. J. Environ. Res. Public Health 2018, 15, 1678. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evans, R.E.; Fawole, H.O.; Sheriff, S.A.; Dall, P.M.; Grant, P.M.; Ryan, C.G. Point-of-choice prompts to reduce sitting time at work: A randomized trial. Am. J. Prev. Med. 2012, 43, 293–297. [Google Scholar] [CrossRef] [PubMed]
- Healy, G.N.; Eakin, E.G.; LaMontagne, A.D.; Owen, N.; Winkler, E.A.H.; Wiesner, G.; Gunning, L.; Neuhaus, M.; Lawler, S.; Fjeldsoe, B.S.; et al. Reducing sitting time in office workers: Short-term efficacy of a multicomponent intervention. Prev. Med. 2013, 57, 43–48. [Google Scholar] [CrossRef] [Green Version]
- Danquah, I.H.; Kloster, S.; Holtermann, A.; Aadahl, M.; Bauman, A.; Ersbøll, A.K.; Tolstrup, J.S.; Ersboll, A.K.; Tolstrup, J.S. Take a stand!—A multi-component intervention aimed at reducing sitting time among office workers-a cluster randomized trial. Int. J. Epidemiol. 2017, 46, 128–140. [Google Scholar] [CrossRef]
- Tronarp, R.; Nyberg, A.; Hedlund, M.; Häger, C.K.; McDonough, S.; Björklund, M. Office-Cycling: A Promising Way to Raise Pain Thresholds and Increase Metabolism with Minimal Compromising of Work Performance. Biomed Res. Int. 2018, 2018, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jans, M.P.; Proper, K.I.; Hildebrandt, V.H. Sedentary Behavior in Dutch Workers: Differences Between Occupations and Business Sectors. Am. J. Prev. Med. 2007, 33, 450–454. [Google Scholar] [CrossRef]
- Bennie, J.A.; Pedisic, Z.; Timperio, A.; Crawford, D.; Dunstan, D.; Bauman, A.; Van Uffelen, J.; Salmon, J. Total and domain-specific sitting time among employees in desk-based work settings in Australia. Aust. N. Z. J. Public Health 2015, 39, 237–242. [Google Scholar] [CrossRef] [Green Version]
- Miller, R.; Brown, W. Steps and sitting in a working population. Int. J. Behav. Med. 2004, 11, 219–224. [Google Scholar] [CrossRef]
- Abdin, S.; Welch, R.K.; Byron-Daniel, J.; Meyrick, J. The effectiveness of physical activity interventions in improving well-being across office-based workplace settings: A systematic review. Public Health 2018, 160, 70–76. [Google Scholar] [CrossRef]
- Howarth, A.; Quesada, J.; Silva, J.; Judycki, S.; Mills, P.R. The impact of digital health interventions on health-related outcomes in the workplace: A systematic review. Digit. Health 2018, 4, 205520761877086. [Google Scholar] [CrossRef] [Green Version]
- Hartvigsen, J.; Leboeuf-Yde, C.; Lings, S.; Corder, E.H. Review Article: Is sitting-while-at-work associated with low back pain? A systematic, critical literature review. Scand. J. Public Health 2000, 28, 230–239. [Google Scholar] [CrossRef] [PubMed]
- Søndergaard, K.H.E.; Olesen, C.G.; Søndergaard, E.K.; de Zee, M.; Madeleine, P. The variability and complexity of sitting postural control are associated with discomfort. J. Biomech. 2010, 43, 1997–2001. [Google Scholar] [CrossRef] [PubMed]
- Karakolis, T.; Callaghan, J.P. The impact of sit–stand office workstations on worker discomfort and productivity: A review. Appl. Ergon. 2014, 45, 799–806. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, N.; Kukkonen-Harjula, K.T.; Verbeek, J.H.; Ijaz, S.; Hermans, V.; Pedisic, Z. Workplace interventions for reducing sitting at work. Cochrane Database Syst. Rev. 2018. [Google Scholar] [CrossRef]
- Neuhaus, M.; Eakin, E.G.; Straker, L.; Owen, N.; Dunstan, D.W.; Reid, N.; Healy, G.N. Reducing occupational sedentary time: A systematic review and meta-analysis of evidence on activity-permissive workstations. Obes. Rev. 2014, 15, 822–838. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agarwal, S.; Steinmaus, C.; Harris-Adamson, C. Sit-stand workstations and impact on low back discomfort: A systematic review and meta-analysis. Ergonomics 2018, 61, 538–552. [Google Scholar] [CrossRef]
- Podrekar, N.; Kozinc, Ž.; Šarabon, N. Effects of cycle and treadmill desks on energy expenditure and cardiometabolic parameters in sedentary workers: Review and meta-analysis. Int. J. Occup. Saf. Ergon. 2019, 27, 728–736. [Google Scholar] [CrossRef] [Green Version]
- Van Dongen, J.M.; Proper, K.I.; van Wier, M.F.; van der Beek, A.J.; Bongers, P.M.; van Mechelen, W.; van Tulder, M.W. Systematic review on the financial return of worksite health promotion programmes aimed at improving nutrition and/or increasing physical activity. Obes. Rev. 2011, 12, 1031–1049. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Worksite A | Worksite B | Total |
|---|---|---|---|
| Type of company | Online training | Legal firm | |
| Location | Dublin suburb | Dublin city centre | |
| Total participants | 8 | 14 | 22 |
| Total no. managers | 1 | 7 | 8 |
| Total no. of employees | 7 | 7 | 14 |
| Mean age years (SD) | 44.4 (11.0) | 41.5 (11.0) | 42.9 (11.0) |
| Hours worked per week (SD) | 41.1 (4.1) | 44.0 (10.5) | 42.6 (7.3) |
| Workday sedentary behaviour min (n = 20) | 399.7 (36.8) | 406.7(141.1) | 403.6 (111.2) |
| Total weekday sedentary behaviour | 630.7 (82.4) | 611.3 (115.4) | 619.9 (105.5) |
| Total weekend sedentary behaviour | 560.3 (85.0) | 467.1 (81.7) | 508.6 (97.9) |
| Workday physical activity | 37.6 (7.8) | 50.1 (12.7) | 45.1 (12.9) |
| Total weekday physical activity | 79.9 (18.6) | 102.9 (21.3) | 93.7 (23.8) |
| Total weekend physical activity | 122.2 (64.7) | 136.0 (38.3) | 130.5 (52.3) |
| Workday standing | 73.4 (16.4) | 122.5 (89.7) | 102.9 (76.2) |
| Weekday total standing | 171.6 (31.0) | 225.9 (115.02) | 204.2 (97.5) |
| Weekend standing | 220.8 (64.7) | 241.8 (57.3) | 233.4 (62.8) |
| Intervention Facilitator Themes | Quotes |
|---|---|
| Individual | |
| (a) Knowledge, education, and awareness |
|
| (b) Sense of enjoyment |
|
| (c) Motivation to improve cardiovascular health |
|
| (d) Domino effect |
|
| Interpersonal | |
| (a) Sense of togetherness |
|
| (b) Observational learning |
|
| (c) Social comparison |
|
| (d) Opportunity for social interaction |
|
| Environmental | |
| (a) Privacy of under-desk pedalling |
|
| (b) Musculoskeletal improvement |
|
| (c) Use of pedal device as alternative |
|
| (d) Complementation of work tasks while pedalling |
|
| (e) Move bar prompted movement |
|
| Organisational | |
| No detrimental effect on productivity |
|
| Intervention barriers | |
| Individual | |
| Time priorities |
|
| Interpersonal | |
| Social judgement |
|
| Environmental | |
| (a) Ergonomic set-up |
|
| (b) Garmin watch manual- recording |
|
| Intervention (I) n = 17 | Control (C) n = 19 | Difference C-I | |
|---|---|---|---|
| Workday SB minutes (SD) | 358.9 (96.6) | 379.3 (79.0) | −20.4 |
| Total weekday SB | 588.8 (107.8) | 634.5 (102.5) | −45.7 |
| Weekend sedentary behaviour | 498.9 (108.4) | 507.7 (106.4) | −8.9 |
| Workday physical activity | 48.7 (13.8) | 48.5 (13.8) | 0.3 |
| Total weekday PA | 103.2 (29.2) | 93.4 (24.3) | 9.9 |
| Weekend physical activity | 124.0 (38.7) | 125.5 (36.1) | −1.5 |
| Workday standing | 110.1 (72.1) | 95.7 (36.2) | 14.4 |
| Total weekday standing | 219.7 (94.7) | 196.5 (52.0) | 23.2 |
| Weekend standing | 239.4 (62.5) | 229.3 (58.7) | 10.1 |
| Intervention | Control | |||
|---|---|---|---|---|
| n = 21 | Mean (SD) | n = 19 | Mean (SD) | |
| Work engagement (total) | 4.23 (0.8) | 4.33 (0.8) | ||
| Vigour | 3.94 (1.1) | 4.16 (0.9) | ||
| Dedication | 4.44 (0.8) | 4.49 (0.8) | ||
| Absorption | 4.32 (0.8) | 4.35 (0.9) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nicolson, G.H.; Hayes, C.B.; Darker, C.D. A Cluster-Randomised Crossover Pilot Feasibility Study of a Multicomponent Intervention to Reduce Occupational Sedentary Behaviour in Professional Male Employees. Int. J. Environ. Res. Public Health 2021, 18, 9292. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179292
Nicolson GH, Hayes CB, Darker CD. A Cluster-Randomised Crossover Pilot Feasibility Study of a Multicomponent Intervention to Reduce Occupational Sedentary Behaviour in Professional Male Employees. International Journal of Environmental Research and Public Health. 2021; 18(17):9292. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179292
Chicago/Turabian StyleNicolson, Gail Helena, Catherine B. Hayes, and Catherine D. Darker. 2021. "A Cluster-Randomised Crossover Pilot Feasibility Study of a Multicomponent Intervention to Reduce Occupational Sedentary Behaviour in Professional Male Employees" International Journal of Environmental Research and Public Health 18, no. 17: 9292. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179292