
Absolute Reliability and Concurrent Validity of Hand-Held Dynamometry in Shoulder Rotator Strength Assessment: Systematic Review and Meta-Analysis

 and
and 
Abstract
:1. Introduction
2. Materials and Methods
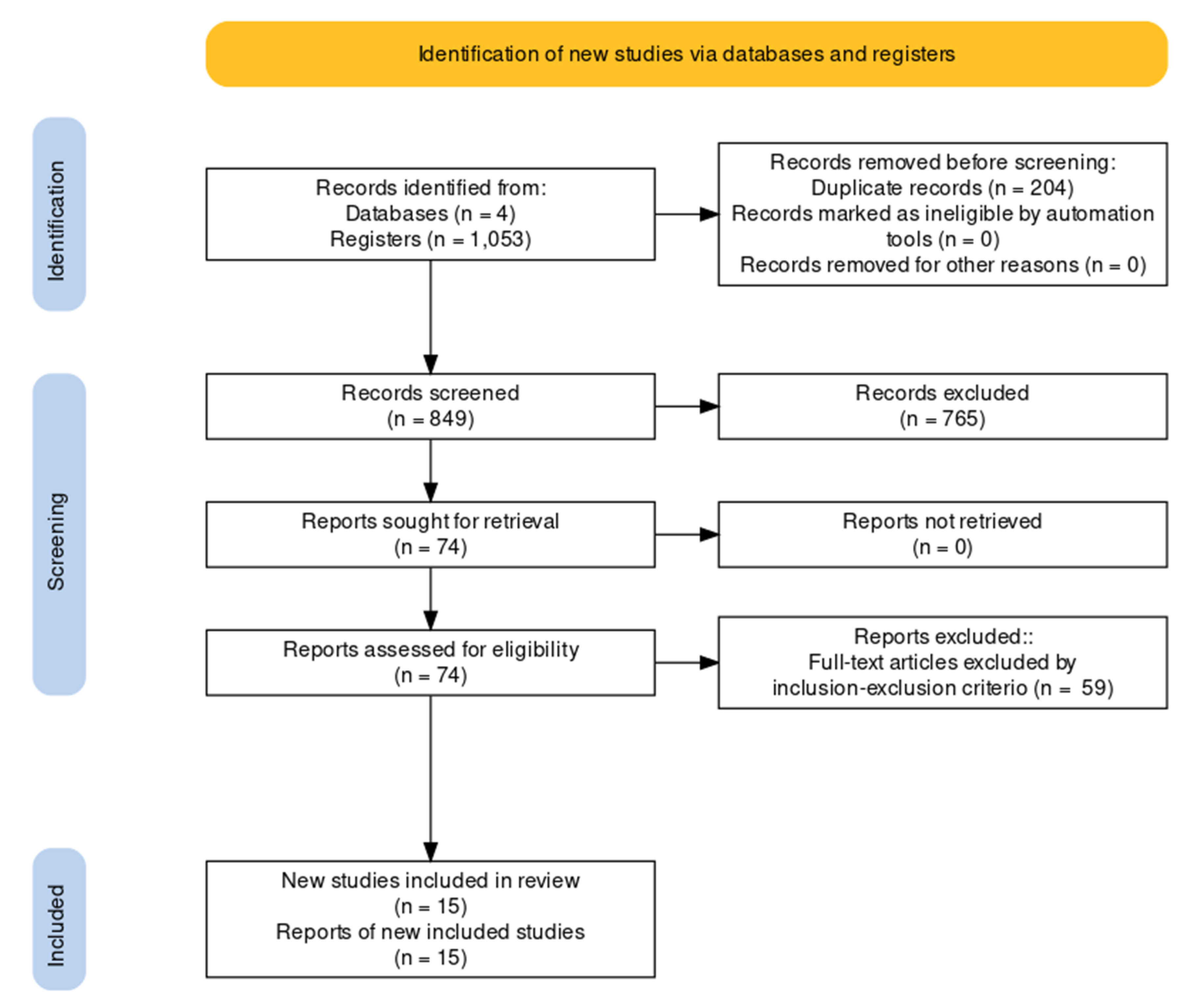
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction
2.4. Quality Assessment Methodology
2.5. Data Synthesis and Analysis
3. Results
3.1. Overall Results
3.2. Methodological Quality of Studies
3.2.1. Absolute Reliability
3.2.2. Concurrent Validity
3.2.3. Absolute Reliability of HHD and Concurrent Validity between HHDs and IDs Based on the Criteria for Good Measurement Properties
3.3. Meta-Analysis
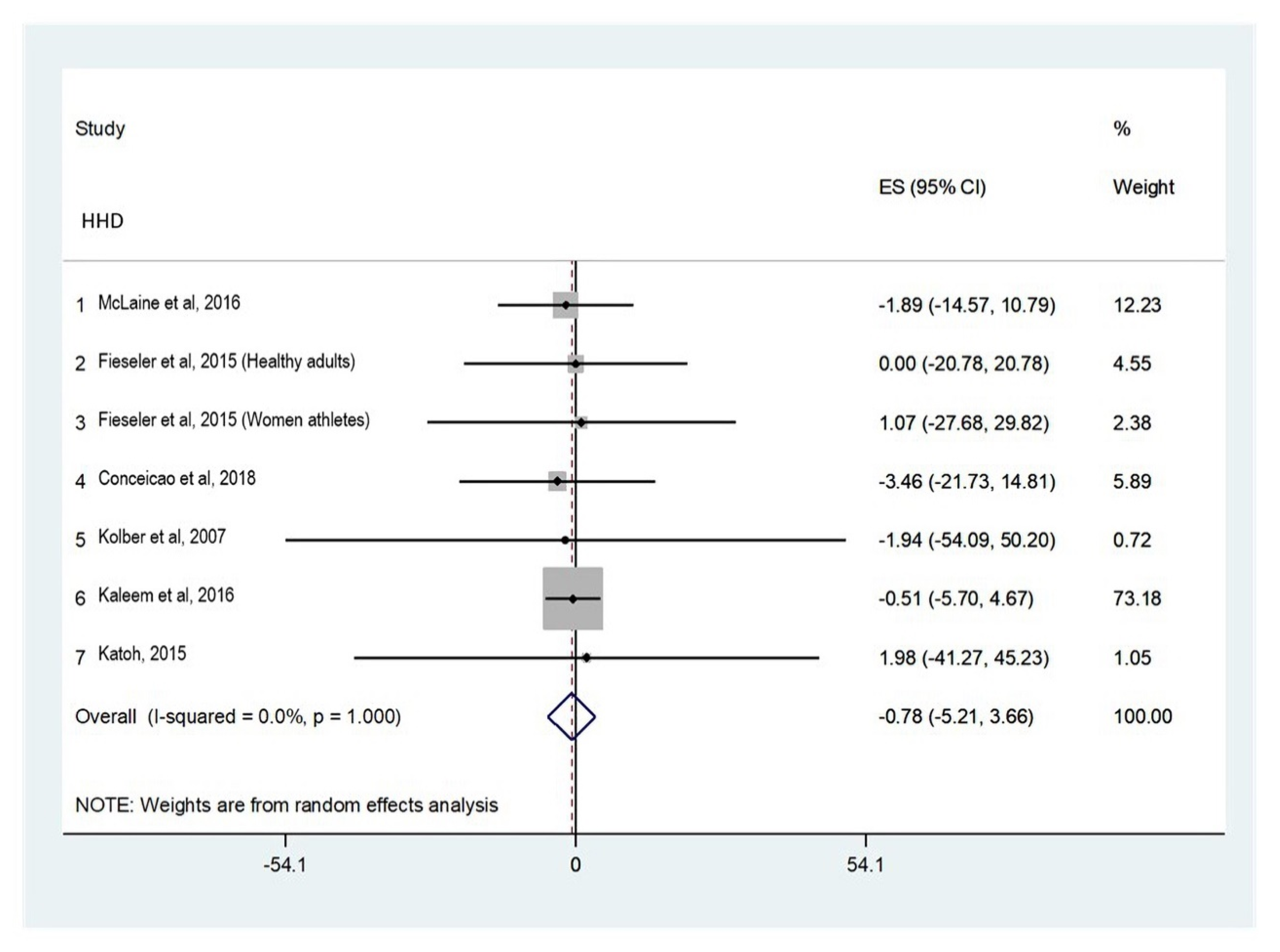
3.3.1. Hand-Held Dynamometry: Absolute Reliability
Shoulder Internal Rotators
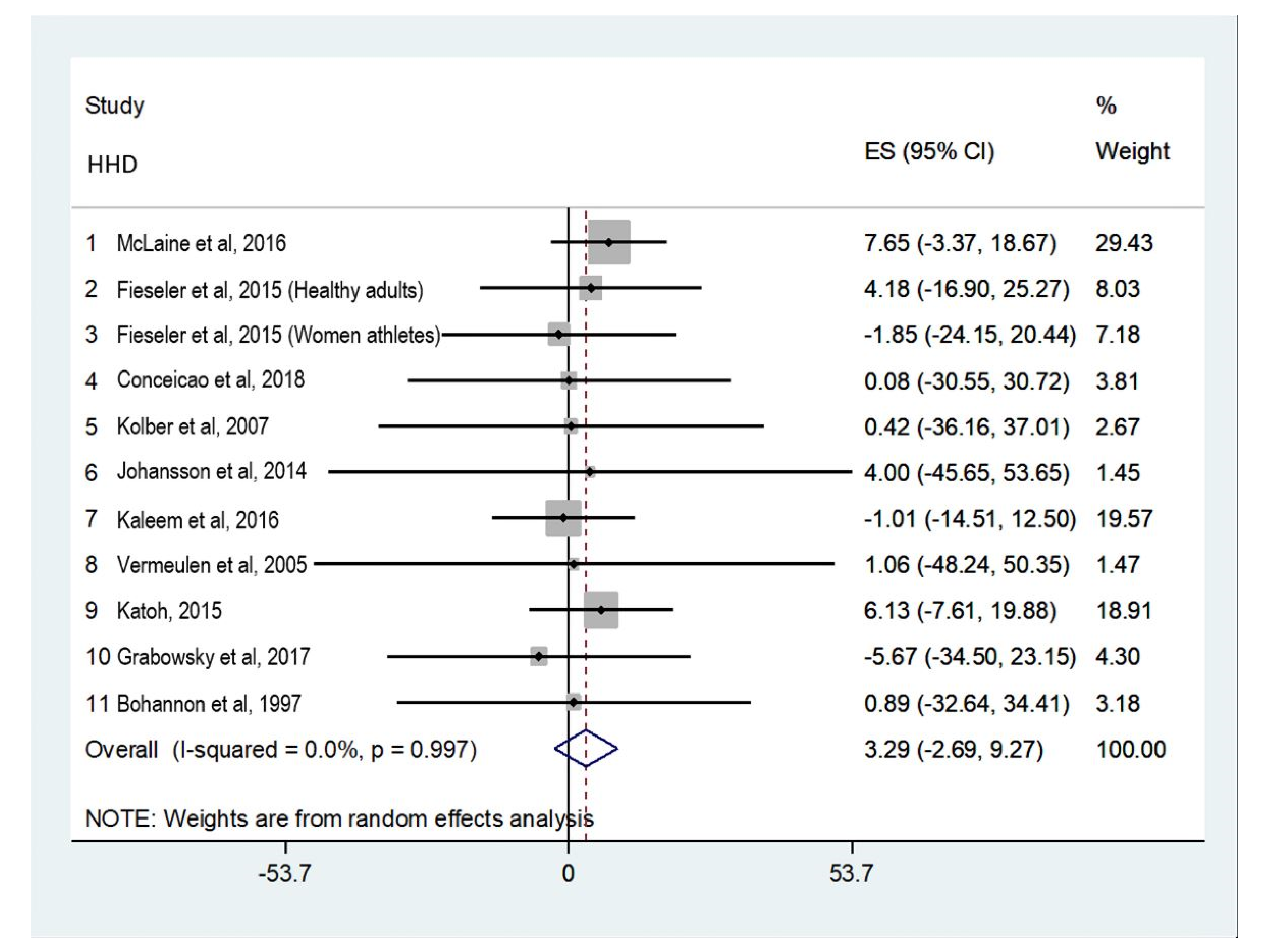
Shoulder External Rotators
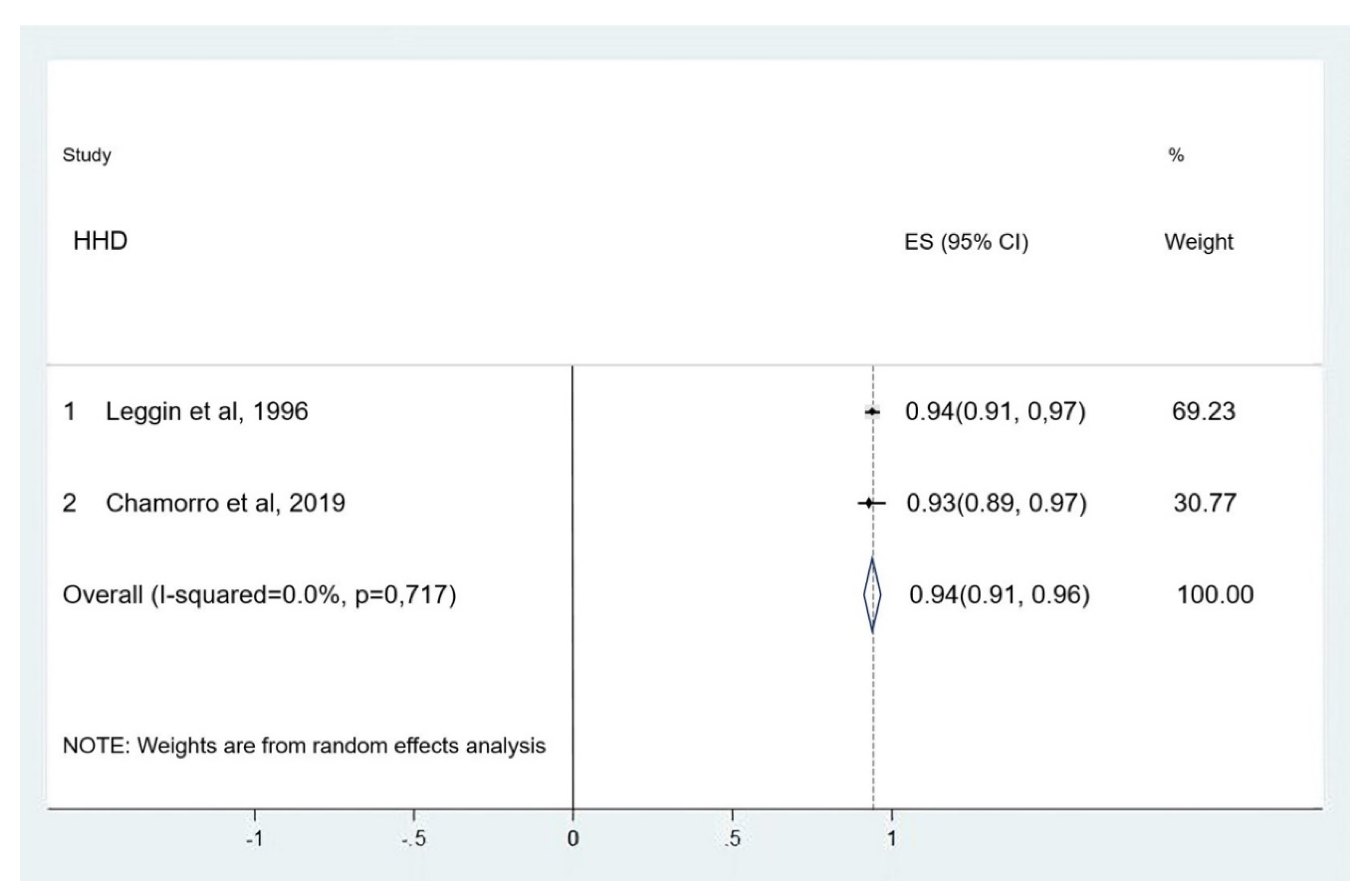
3.3.2. Concurrent Validity between Hand-Held Dynamometers and Isokinetic Dynamometers
Shoulder Internal Rotators
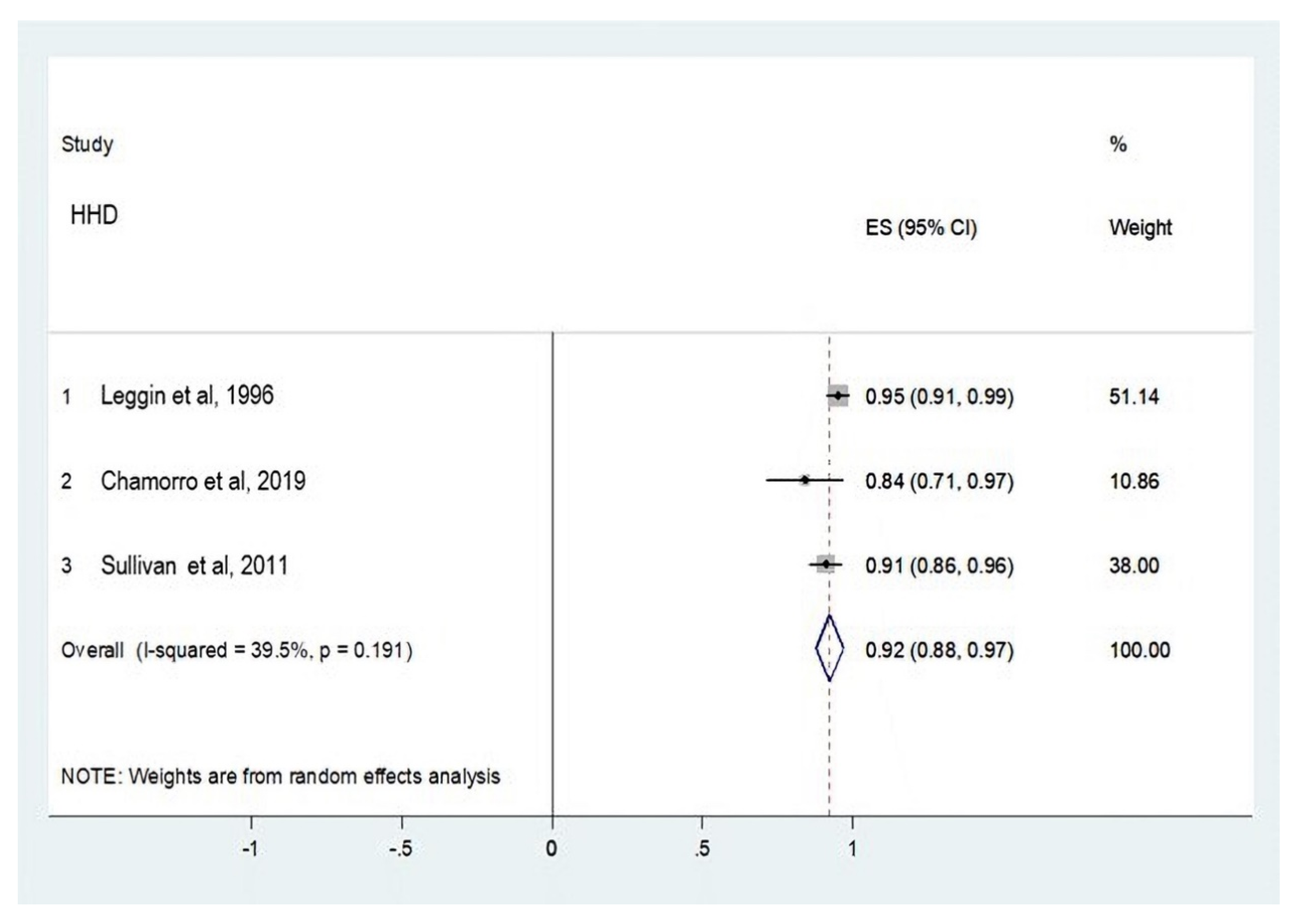
Shoulder External Rotators
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schrama, P.P.M.; Stenneberg, M.S.; Lucas, C.; Van Trijffel, E. Intraexaminer reliability of hand-held dynamometry in the upper extremity: A systematic review. Arch. Phys. Med. Rehabil. 2014, 95, 2444–2469. [Google Scholar] [CrossRef]
- Rabelo, M.; Nunes, G.S.; da Costa Amante, N.M.; de Noronha, M.; Fachin-Martins, E. Reliability 364 of muscle strength assessment in chronic post-stroke hemiparesis: A systematic review and meta-analysis. Top. Stroke Rehabil. 2016, 23, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Padulo, J.; Trajkovic, N.; Cular, D.; Grgantov, Z.; Madic, D.; Di Vico, R.; Traficante, A.; Alin, L.; Ardigo, L.P.; Russo, L. Validity and reliability of isometric-bench for knee isometric assessment. Int. J. Environ. Res. Public Health 2020, 17, 4326. [Google Scholar] [CrossRef]
- Dauty, M.; Delbrouck, C.; Huguet, D.; Rousseau, B.; Potiron-Josse, M.; Dubois, C. Reproducibility of concentric and eccentric isokinetic strength of the shoulder rotators in normal subjects 40 to 55 years old. Isokin. Exerc. Sci. 2003, 11, 95–100. [Google Scholar] [CrossRef]
- Martin, H.J.; Yule, V.; Syddall, H.E.; Dennison, E.M.; Cooper, C.; Aihie Sayer, A. Is hand-held dynamometry useful for the measurement of quadriceps strength in older people? A comparison with the gold standard Bodex dynamometry. Gerontology 2006, 52, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, G.; Nevill, A.M. Statistical methods for assessing measurement error (reliability) in variables relevant to sports medicine. Sports Med. 1998, 26, 217–238. [Google Scholar] [CrossRef]
- Hopkins, W.G. Measures of reliability in sports medicine and science. Sports Med. 2000, 30, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Drouin, J.M.; Valovich-mcLeod, T.C.; Shultz, S.J.; Gansneder, B.M.; Perrin, D.H. Reliability and validity of the Biodex system 3 pro isokinetic dynamometer velocity, torque and position measurements. Eur. J. Appl. Physiol. 2004, 91, 22–29. [Google Scholar] [PubMed]
- Stratford, P.W. Getting more from the literature: Estimating the standard error of measurement from reliability studies. Physiother. Can. 2004, 56, 27–30. [Google Scholar] [CrossRef]
- Edouard, P.; Samozino, P.; Julia, M.; Cervera, S.G.; Vanbiervliet, W.; Calmels, P.; Gremeaux, V. Reliability of Isokinetic Assessment of Shoulder-Rotator Strength: A Systematic Review of the Effect of Position. J. Sport Rehabil. 2011, 20, 367–383. [Google Scholar] [CrossRef] [Green Version]
- Sorensen, L.; Oestergaard, L.S.; van Tulder, M.; Petersen, A.K. Measurement properties of isokinetic dynamometry for assessment of shoulder muscle strength: A systematic review. Arch. Phys. Med. Rehabil. 2021, 102, 510–520. [Google Scholar] [CrossRef]
- Mokkink, L.B.; de Vet, H.C.W.; Prinsen, C.A.C. COSMIN Risk of Bias checklist for systematic reviews of Patient- Reported Outcome Measures. Qual. Life Res. 2018, 27, 1171–1179. [Google Scholar] [CrossRef] [Green Version]
- Mokkink, L.B.; De Vet, H.C.W.; Prinsen, C.A.C.; Patrick, D.L.; Alonso, J.; Bouter, L.; Terwee, C.B. COSMIN Risk of Bias checklist for systematic reviews of Patient-Reported Outcome Measures. Qual. Life Res. 2018, 27, 1171–1179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Terwee, C.B.; Bot, S.D.; de Boer, M.R.; van der Windt, D.A.; Knol, D.L.; Dekker, J.; Bouter, L.M.; de Vet, H.C. Quality criteria were proposed for measurement properties of health status questionnaires. J. Clin. Epidemiol. 2007, 60, 34–42. [Google Scholar] [CrossRef] [Green Version]
- Chamorro, C.; Armijo-Olivo, S.; De la Fuente, C.; Fuentes, J.; Chirosa, L.J. Absolute reliability and concurrent validity of hand held dynamometry and isokinetic dynamometry in the hip, knee and ankle joint: Systematic review and meta-analysis. Open Med. 2017, 12, 359–375. [Google Scholar] [CrossRef]
- Holt, K.L.; Raper, D.P.; Boettcher, C.E.; Waddington, G.S.; Drew, M.K. Hand-held dynamometry strength measures for internal and external rotation demonstrate superior reliability, lower minimal detectable change and higher correlation to isokinetic dynamometry than externally-fixed dynamometry of the shoulder. Phys. Ther. Sport Off. J. Assoc. Chart. Physiother. Sports Med. 2016, 21, 75–81. [Google Scholar] [CrossRef]
- Munro, B.H. Statistical Methods for Health Care Research; Lippincott Williams & Wilkins: Alphen aan den Rijn, The Netherlands, 2005. [Google Scholar]
- McLaine, S.J.; Ginn, K.A.; Kitic, C.M.; Fell, J.W.; Bird, M.-L. The Reliability of Strength Tests Performed In Elevated Shoulder Positions Using a Handheld Dynamometer. J. Sport Rehabil. 2016, 25. [Google Scholar] [CrossRef] [PubMed]
- Fieseler, G.; Molitor, T.; Irlenbusch, L.; Delank, K.-S.; Laudner, K.G.; Hermassi, S.; Schwesig, R. Intrarater reliability of goniometry and hand-held dynamometry for shoulder and elbow examinations in female team handball athletes and asymptomatic volunteers. Arch. Orthop. Trauma Surg. 2015, 135, 1719–1726. [Google Scholar] [CrossRef] [PubMed]
- Conceicao, A.; Parraca, J.; Marinho, D.; Costa, M.; Louro, H.; Silva, A.; Batalha, N. Assessment of isometric strength of the shoulder rotators in swimmers using a handheld dynamometer: A reliability study. Acta Bioeng. Biomech. 2018, 20, 114–119. [Google Scholar]
- Kolber, M.J.; Beekhuizen, K.; Cheng, M.S.S.; Fiebert, I.M. The reliability of hand-held dynamometry in measuring isometric strength of the shoulder internal and external rotator musculature using a stabilization device. Physio. Theory Pract. 2007, 23, 119–124. [Google Scholar] [CrossRef]
- Johansson, F.R.; Skillgate, E.; Lapauw, M.L.; Clijmans, D.; Deneulin, V.P.; Palmans, T.; Engineer, H.K.; Cools, A.M. Measuring Eccentric Strength of the Shoulder External Rotators Using a Handheld Dynamometer: Reliability and Validity. J. Athl. Train. 2014, 50, 719–725. [Google Scholar] [CrossRef]
- Raza, S. Reliability and Validity of EN-TreeM Dynamometer for Measurement of Shoulder Rotator Strength in Volleyball Players. J. Clin. Diagn. Res. 2016, 10, YC05–YC09. [Google Scholar] [CrossRef]
- Vermeulen, H.M.; de Bock, G.H.; van Houwelingen, H.C.; van der Meer, R.L.; Mol, M.C.; Plus, B.T.; Rozing, P.M.; Vlieland, T.V. A comparison of two portable dynamometers in the assessment of shoulder and elbow strength. Physiotherapy 2005, 91, 101–112. [Google Scholar] [CrossRef]
- Katoh, M. Test-retest reliability of isometric shoulder muscle strength measurement with a handheld dynamometer and belt. J. Phys. Ther. Sci. 2015, 27, 1719–1722. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grabowski, P.; Narveson, M.; Siegle, S. Reliability, responsiveness, and criterion validity of the Kiio sensor, a new tool for assessment of muscle function. Mil. Med. 2017, 182, 26–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bohannon, R.W. Reference values for extremity muscle strength obtained by hand-held dynamometry from adults aged 20 to 79 years. Arch. Phys. Med. Rehabil. 1997, 78, 26–32. [Google Scholar] [CrossRef]
- Leggin, B.G.; Neuman, R.M.; Iannotti, J.P.; Williams, G.R.; Thompson, E.C. Intrarater and interrater reliability of three isometric dynamometers in assessing shoulder strength. J. Shoulder Surg. 1996, 5, 18–24. [Google Scholar] [CrossRef]
- Chamorro, C.; de la Fuente, C.; Rubio, J.; Campos, C.; Chirosa, L.J. Absolute reliability and concurrent validity of a novel electromechanical pulley dynamometer for measuring shoulder rotation isometric strength in asymptomatic subjects. Study conducted at Pontificia Universidad Católica, Santiago, Chile. J. Pak. Med. Assoc. 2019, 69, 1000–1005. [Google Scholar]
- Hébert, L.J.; Maltais, D.B.; Lepage, C.; Saulnier, J.; Crête, M.; Perron, M. Isometric muscle strength in youth assessed by hand-held dynamometry: A feasibility, reliability, and validity study: A feasibility, reliability, and validity study. Pediatr. Phys. Ther. 2011, 23, 289–299. [Google Scholar] [CrossRef]
- Van Meeteren, J.; Roebroeck, M.E.; Stam, H.J. Test-retest reliability in isokinetic muscle strength measurements of the shoulder. J. Rehabil. Med. 2002, 34, 91–95. [Google Scholar] [CrossRef] [Green Version]
- Collado-Mateo, D.; Dominguez-Muñoz, F.J.; Batalha, N.; Parraça, J.; Tomas-Carus, P.; Adsuar, J.C. Test-retest reliability of isokinetic arm strength measurements in competitive swimmers. J. Hum. Kinet. 2018, 65, 5–11. [Google Scholar] [CrossRef] [Green Version]
- Wikholm, J.B.; Bohannon, R.W. Hand-held dynamometer measurements: Tester strength makes a difference. J. Orthop. Sports Phys. Ther. 1991, 13, 191–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bassett, R.W.; Browne, A.O.; Morrey, B.F.; An, K.N. Glenohumeral muscle force and moment mechanics in a position of shoulder instability. J. Biomech. 1990, 23, 405–415. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors | Participants | Age(SD) | Type of Dynamometer | Movement | Assessment Position | Shoulder Position | Type of Muscle Contraction | Test–Retest Interval |
|---|---|---|---|---|---|---|---|---|
| McLaine et al., 2016 | 15 healthy adults F:10 M:5 | 24 (8.2) | Jtech Powertrack Commander | IR/ER | Seated | ABD 90° | Isometric | 48 h |
| Fieseler et al., 2015 | 25 healthy adults F:13 M:12 | 21.9 (1.2) | IsoForce Control EVO2 | IR/ER | Supine | ABD 90° | Isometric | 7 days |
| 22 female athletes | 21 (3.8) | |||||||
| Conceicao et al., 2018 | 29 swimmers :21 M:8 | 16.2 (1.2) | Micro FET 2 | IR/ER | Prone | ABD 90° | Isometric | 7 days |
| Kolber et al., 2007 | 30 healthy adults F:15 M:15 | 35.6 (13.7) | Micro FET 2 | IR/ER | Seated | ABD scapular plane | Isometric | 10 min |
| Johansson et al., 2014 | 25 healthy adults:16 M:9 | 25.2 (10) | Compu FET | RE | Seated | ABD 90° | Excentric | 20 s |
| Kaleem et al., 2016 | 30 male volleyball players | 21 (1.8) | EN-TreeM | IR/ER | Seated | ABD scapular plane | Concentric | 48 h |
| Vermeulen et al., 2005 | 20 healthy adults F:8 M:16 | 25 (12) | Micro FET 2 | RE | Seated | ABD 90° | Isometric | 3 days |
| Katoh, 2015 | 40 healthy adults H:20 M:20 | 21(1) | μTas F-1 | IR/ER | Seated | ABD scapular plane | Isometric | 30 s |
| Grabowski et al., 2017 | 44 healthy adults H:24 M:20 | 21.2 (1.5) | Kiio Sensor | RE | Standing | 30° ABD scapular plane | Isometric | 7 days |
| Bohannon et al., 1997 | 231 healthy adults H:106 M:125 | 40 (20) | Accuforce II | RE | Supine | 45° ABD | Isometric | 1 min |
| Authors | Movement | Mean (%) | Difference Scores between Trials (%) | SEM (kg) (SEM%) | MDC Lower Limit (%) | MDC Upper Limit (%) |
|---|---|---|---|---|---|---|
| McLaine et al., 2016 | IR | 10.6 | −1.88 | 0.24 (2.26) | −4.45 | 8.22 |
| ER | 9.15 | 7.65 | 0.18 (1.96) | −13.15 | −2.14 | |
| Fieseler et al., 2015 | IR | 9.7 | 0 | 0.36 (3.71) | −10.39 | 10.39 |
| ER | 11.95 | 4.18 | 0.45 (3.76) | −14.72 | 6.35 | |
| IR | 9.35 | 1.06 | 0.48 (5.13) | −15.44 | 13.30 | |
| ER | 10.8 | −1.85 | 0.43 (3.98) | −9.29 | 13 | |
| Conceicao et al., 2018 | IR | 15.32 | −3.45 | 0.5 (3.26) | −5.67 | 12.59 |
| ER | 12.06 | 0.08 | 0.66 (5.47) | −15.39 | 15.23 | |
| Kolber et al., 2007 | IR | 12.35 | −1.94 | 1,15 (9,31) | −24.12 | 28.01 |
| ER | 9.49 | 0.42 | 0.62 (6.53) | −18.71 | 17.87 | |
| Johansson et al., 2014 | ER | 12.74 | 4 | 1.13 (8.86) | −28.82 | 20.82 |
| Kaleem et al., 2016 | IR | 19.45 | −0.51 | 0.18 (0.92) | −2.07 | 3.10 |
| ER | 9.95 | −1 | 0.24 (2.41) | −5.74 | 7.75 | |
| Vermeulen et al., 2005 | ER | 11.36 | 1.05 | 1.06 (9.33) | −27.18 | 25.07 |
| Katoh, 2015 | IR | 15.15 | 1.98 | 0.96 (6.33) | −19.72 | 15.76 |
| ER | 8.15 | 6.13 | 0.2 (2.45) | −13.00 | 0.73 | |
| Grabowski et al., 2017 | ER | 9.52 | −5.67 | 0.49 (5.14) | −8.73 | 20.08 |
| Bohannon et al., 1997 | ER | 13.53 | 0.88 | 0.81 (5.98) | −17.64 | 15.87 |
| Authors | Participants | Age (SD) | Movement | Assessment Position | Shoulder Position | Dinamometer | Comparison | Type of Muscular Contraction |
|---|---|---|---|---|---|---|---|---|
| Leggin et al., 1996 | 17 healthy adults F:10 M:7 | 30.5 (5.5) | IR/ER | Seated | Scapular plane | HHD Lafayette | ID BIODEX | Isometric |
| Chamorro et al., 2019 | 24 healthy adults F:19 M:5 | 23.1 (2.2) | IR/RE | Supine | ABD 90° | HHD FED | ID REV 7000 | Isometric |
| Hebert et al., 2011 | 74 healthy adults F:36 M:38 | 10.7 (3.9) | ER | Supine | ABD 0° | HHD Lafayette | ID CYBEX norm | Isometric |
| Authors | Participants | Movement (Strength Measurement Unit) | HHD (SD) | ID (SD) | Interdevice ICC (95% CI) |
|---|---|---|---|---|---|
| Leggin et al., 1996 | 17 healthy adults F:10 M:7 | IR (Nm) | NOT SHOWN | NOT SHOWN | 0.94 (0.91–0.97) |
| ER (Nm) | NOT SHOWN | NOT SHOWN | 0.95 (0.91–0.99) | ||
| Chamorro et al., 2019 | 24 healthy adults F:19 M:5 | IR (Nm) | 32.5 ± 11.1 | 30.9 ± 13.6 | 0.93 (0.89–0.97) |
| ER (Nm) | 23.9 ± 5.81 | 27.5 ± 12.0 | 0.84 (0.71–0.97) | ||
| Hebert et al., 2011 | 74 healthy adults | ER (Nm) | NOT SHOWN | NOT SHOWN | 0.91 (0.79–0.96) |
| Authors | Were Patients Stable in the Interim Period in the Construct to Be Measured? | Was the Time Interval Appropriate? | Were the Test Conditions Similar for the Measurements? | Was the Standard Error of Measurement (SEM), Minimum Detectable Change (MDC), or Limits of Agreement (LOA) Calculated? | Was the Standard Error of Measurement (SEM), Smallest Detectable Change (SDC), or Limits of Agreement (LoA) Calculated? | Were There Any Other Important Flaws in the Design or Statistical Methods of the Study? | Ranking |
|---|---|---|---|---|---|---|---|
| McLaine et al., 2016 | Very good | Inadequate | Very good | Very good | NA | Inadequate | Inadequate |
| Fieseler et al., 2015 | Very good | Very good | Very good | Very good | NA | Inadequate | Inadequate |
| Conceicao et al., 2018 | Very good | Very good | Very good | Very good | NA | Inadequate | Inadequate |
| Kolber et al., 2007 | Very good | Inadequate | Very good | Very good | NA | Adequate | Inadequate |
| Johansson et al., 2014 | Very good | Inadequate | Very good | Very good | NA | Inadequate | Inadequate |
| Kaleem et al., 2016 | Very good | Inadequate | Very good | Very good | NA | Adequate | Inadequate |
| Vermeulen et al., 2005 | Very good | Adequate | Very good | Very good | NA | Inadequate | Inadequate |
| Katoh, 2015 | Very good | Adequate | Very good | Very good | NA | Inadequate | Inadequate |
| Grabowski et al., 2017 | Very good | Adequate | Very good | Very good | NA | Adequate | Adequate |
| Bohannon et al., 1997 | Very good | Inadequate | Very good | Very good | NA | Very good | Inadequate |
| Authors | For Continuous Scores: Were Correlations or the Area under the Receiver Operating Curve Calculated? | For Dichotomous Scores: Were Sensitivity and Specificity Determined? | Were There Any Other Important Flaws in the Design or Statistical Methods of the Study? | Ranking |
|---|---|---|---|---|
| Leggin et al., 1996 | Very good | NA | Adequate | Adequate |
| Chamorro et al., 2019 | Very good | NA | Adequate | Inadequate |
| Hebert et al., 2011 | Very good | NA | Adequate | Inadequate |
| Authors | N | Rating MDC for Absolute Reliability HHDs | N | Rating ICC for Concurrent Validity HHD and ID |
|---|---|---|---|---|
| McLaine et al., 2016 | 15 | MDC IR:8.22 (+) ER:13.15 (+) | ||
| Fieseler et al., 2015 | 25 | MDC IRI:10.39 (+) ER:14.72(+) | ||
| 22 | MDC IR:15.44 (-) ER:13.00 (+) | |||
| Conceição et al., 2018 | 29 | MDC IR:12.59 (+) ER:15.39 (-) | ||
| Kolber et al., 2007 | 30 | MDC IR:28.01 (-) ER:18.71 (-) | ||
| Johansson et al., 2014 | 25 | MDC ER:28.82 (-) | ||
| Kaleem et al., 2016 | 30 | MDC IR:3.10 (+) ER:7.75 (+) | ||
| Vermeulen et al., 2005 | 20 | MDC ER:27.18 (-) | ||
| Katoh, 2015 | 40 | MDC IR:19.72 (-) ER:13.00 (+) | ||
| Grabowski et al., 2017 | 44 | MDC ER:20.08 (-) | ||
| Bohannon et al., 1997 | 231 | MDC ER:17.64 (-) | ||
| Leggin et al., 1996 | 17 | ICC IR:0.94 (+) ER:0.95 (+) | ||
| Chamorro et al., 2019 | 24 | ICC IR:0.93 (+) ER:0.84 (+) | ||
| Hebert et al., 2011 | 74 | ICC ER:0.91 (+) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chamorro, C.; Arancibia, M.; Trigo, B.; Arias-Poblete, L.; Jerez-Mayorga, D. Absolute Reliability and Concurrent Validity of Hand-Held Dynamometry in Shoulder Rotator Strength Assessment: Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 9293. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179293
Chamorro C, Arancibia M, Trigo B, Arias-Poblete L, Jerez-Mayorga D. Absolute Reliability and Concurrent Validity of Hand-Held Dynamometry in Shoulder Rotator Strength Assessment: Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(17):9293. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179293
Chicago/Turabian StyleChamorro, Claudio, Miguel Arancibia, Benjamín Trigo, Leónidas Arias-Poblete, and Daniel Jerez-Mayorga. 2021. "Absolute Reliability and Concurrent Validity of Hand-Held Dynamometry in Shoulder Rotator Strength Assessment: Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 17: 9293. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179293