
Heterogeneity of Modern Contraceptive Use among Urban Slum and Nonslum Women in Kinshasa, DR Congo: Cross-Sectional Analysis


Abstract
:1. Background
2. Methodology
2.1. Data
2.2. Variables
2.3. Exposures
2.3.1. Slum Household
2.3.2. Slum Neighborhood
2.4. Independent Variables
2.5. Statistical Analysis
2.6. Ethical Review
2.7. Patient and Public Involvement
3. Results
3.1. Respondent Characteristics
3.2. Bivariate Results
3.2.1. Prevalence of Modern Contraceptive Use
3.2.2. Contraceptive-Method Choice
3.3. Multivariable Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability
Conflicts of Interest
References
- UN-HABITAT. The Challenge of Slums: Global Report on Human Neighborhood 2003; London and Sterling; Earthscan Publications Ltd.: London, UK, 2003. [Google Scholar]
- WHO. The World Health Report 2002: Reducing Risks, Promoting Healthy Life; World Health Organization: Geneva, Switzerland, 2002.
- INS. Enquête par Grappes à Indicateurs Multiples, 2017–2018, Rapport de Résultats de L’enquête. Kinshasa, République Démocratique du Congo. 2019. Available online: https://mics-surveys-prod.s3.amazonaws.com/MICS6/West%20and%20Central%20Africa/Congo%2C%20Democratic%20Republic%20of%20the/2017-2018/Survey%20findings/Congo%2C%20Democratic%20Republic%20of%20the%2C%202017-18%20MICS%20SFR_French.pdf (accessed on 20 March 2020).
- Ministère du Plan and Macro International. Enquête Démographique et de Santé, République Démocratique du Congo 2007; Ministère du Plan and Macro International: Calverton, MD, USA, 2008. [Google Scholar]
- Ministère du Plan et Suivi de la Mise en Œuvre de la Révolution de la Modernité (MPSMRM); Ministère de la Santé Publique (MSP); ICF International. Enquête Démographique et de Santé en République Démocratique du Congo 2013–2014; MPSMRM, MSP, and ICF International: Rockville, MD, USA, 2014; Available online: https://dhsprogram.com/publications/publication-FR300-DHS-Final-Reports.cfm (accessed on 4 December 2018).
- Muanda, M.; Ndongo, P.G.; Taub, L.D.; Bertrand, J.T. Barriers to modern contraceptive use in Kinshasa, DRC. PLoS ONE 2016, 11, e0167560. [Google Scholar] [CrossRef] [Green Version]
- United Nations. World Population Prospects: The 2015 Revision, Volume II: Demographic Profiles (ST/ESA/SER.A/380); United Nations, Department of Economic and Social Affairs, Population Division: New York, NY, USA, 2015.
- World Bank. Revue de L’Urbanisation en République Démocratique du Congo: Des Villes Productives et Inclusives pour L’Émergence de la République Démocratique du Congo; Directions in Development—Environment and Sustainable Development; World Bank: Washington, DC, USA, 2018. Available online: https://openknowledge.worldbank.org/handle/10986/28931 (accessed on 20 March 2020).
- Piermay, J.-L. Kinshasa: A reprieved mega-city? In The Urban Challenge in Africa: Growth and Management of Its Largest Cities; Rakodi, C., Ed.; United Nations University Press: Tokyo, Japan, 1997. [Google Scholar]
- Matthews, Z.; Channon, A.; Neal, S.; Osrin, D.; Madise, N.; Stones, W. Examining the “urban advantage” in maternal health care in developing countries. PLoS Med. 2010, 7, e1000327. [Google Scholar] [CrossRef] [Green Version]
- White, M.J.; Lindstrom, D.P. Internal migration. In Handbook of Population; Springer: New York, NY, USA, 2005; pp. 311–346. [Google Scholar]
- Ochako, R.; Izugbara, C.; Okal, J.; Askew, I.; Temmerman, M. Contraceptive method choice among women in slum and non-slum communities in Nairobi, Kenya. BMC Womens Health 2016, 16, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fotso, J.C.; Izugbara, C.; Saliku, T.; Ochako, R. Unintended pregnancy and subsequent use of modern contraceptive among slum and non-slum women in Nairobi, Kenya. BMC Pregnancy Childbirth 2014, 14, 224. [Google Scholar] [CrossRef] [Green Version]
- Muhoza, D.N.; Ruhara, C.M. Closing the Poor-Rich Gap in Contraceptive Use in Rwanda: Understanding the Underlying Mechanisms. Int. Perspect. Sex Reprod. Health 2019, 45, 13–23. [Google Scholar] [CrossRef] [PubMed]
- White, M.J.; Muhidin, S.; Andrzejewski, C.; Tagoe, E.; Knight, R.; Reed, H. Urbanization and fertility: An event-history analysis of coastal Ghana. Demography 2008, 45, 803–816. [Google Scholar] [CrossRef] [PubMed]
- Cleland, J.; Wilson, C. Demand Theories of the Fertility Transition—An Iconoclastic View. Popul. Stud. 1987, 41, 5–30. [Google Scholar] [CrossRef]
- Cleland, J.; Bernstein, S.; Ezeh, A.; Faundes, A.; Glasier, A.; Innis, J. Family planning: The unfinished agenda. Lancet 2006, 368, 1810–1827. [Google Scholar] [CrossRef]
- UN-Habitat. The Challenge of Slums: Global Report on Human Settlements 2003. Chapter 1: Development Context and the Millennium Agenda. Revised and Updated Version. 2010. Available online: unhabitat.org (accessed on 23 June 2020).
- Festin, M.P.R.; Kiarie, J.; Solo, J.; Spieler, J.; Malarcher, S.; van Look, P.F.A.; Temmerman, M. Moving towards the goals of FP2020–classifying contraceptives. Contraception 2016, 94, 289–294. [Google Scholar] [CrossRef] [Green Version]
- Filmer, D.; Pritchett, L. Estimating wealth effects without expenditure data—Or tears: An application to educational enrollments in States of India. Demography 2001, 38, 115–132. [Google Scholar]
- Dehlendorf, C.; Rodriguez, M.I.; Levy, K.; Borrero, S.; Steinauer, J. Disparities in family planning. Am. J. Obstet. Gynecol. 2010, 202, 214–220. [Google Scholar] [CrossRef] [Green Version]
- Kaye, K.; Suellentrop, K.; Sloup, C. The Fog Zone: How Misperceptions, Magical Thinking, and Ambivalence Put Young Adults at Risk for Unplanned Pregnancy; The National Campaign to Prevent Teen and Unintended Pregnancy: Washington, DC, USA, 2009. [Google Scholar]
- Guendelman, S.; Denny, C.; Mauldon, J.; Chetkovich, C. Perceptions of hormonal contraceptive safety and side effects among low-income Latina and non-Latina women. Matern. Child Health J. 2000, 4, 233–239. [Google Scholar] [CrossRef]
- Sangi-Haghpeykar, H.; Ali, N.; Posner, S.; Poindexter, A.N. Disparities in contraceptive knowledge, attitude and use between Hispanic and non-Hispanic whites. Contraception 2006, 74, 125–132. [Google Scholar] [CrossRef]
- Todd, S.; Sommers, B. Overview of the Uninsured in the United States: A Summary of the 2012 Current Population Survey Report; Assistant Secretary for Planning and Evaluation: Washington, DC, USA, 2012.
- Speizer, I.S.; Nanda, P.; Achyut, P.; Pillai, G.; Guilkey, D.K. Family planning use among urban poor women from six cities of Uttar Pradesh, India. J. Urban Health 2012, 89, 639–658. [Google Scholar] [CrossRef] [Green Version]
- Tukue, D.; Gebremeskel, T.G.; Gebremariam, L.; Aregawi, B.; Hagos, M.G.; Gebremichael, T.; Tesfay, H.N.; Arefaine, Z.G. Prevalence and determinants of modern contraceptive utilization among women in the reproductive age group in Edaga-hamus Town, Eastern zone, Tigray region, Ethiopia, June 2017. PLoS ONE 2020, 15, e0227795. [Google Scholar] [CrossRef]
- Binanga, A.; Bertrand, J. Pilot Research as Advocacy: The Case of Sayana Press in Kinshasa, Democratic Republic of the Congo. Glob. Health Sci. Pract. 2016, 4, 542–551. [Google Scholar] [CrossRef] [Green Version]
- Hernandez, J.H.; Akilimali, P.; Glover, A.; Bertrand, J.T. Feasibility and acceptability of using medical and nursing students to provide Implanon NXT at the community level in Kinshasa, Democratic Republic of Congo. BMC Womens Health 2020, 24, 133. [Google Scholar] [CrossRef]
- Bertrand, J.T.; Bidashimwa, D.; Makani, P.B.; Hernandez, J.H.; Akilimali, P.; Binanga, A. An observational study to test the acceptability and feasibility of using medical and nursing students to instruct clients in DMPA-SC self-injection at the community level in Kinshasa. Contraception 2018, 98, 411–417. [Google Scholar] [CrossRef] [Green Version]
- Moses, O.; Mutisya, M.; Ngware, M.; Ezeh, A.C. Why are there proportionately more poor pupils enrolled in non-state schools in urban Kenya in spite of FPE policy? Int. J. Educ. Dev. 2010, 30, 23–32. [Google Scholar]
- Seth, A.; Tomar, S.; Singh, K.; Chandurkar, D.; Chakraverty, A.; Dey, A.; Das, A.K.; Hay, K.; Saggurti, N.; Boyce, S.; et al. Differential effects of community health worker visits across social and economic groups in Uttar Pradesh, India: A link between social inequities and health disparities. Int. J. Equity Health 2017, 16, 46. [Google Scholar] [CrossRef] [Green Version]
- Grant, M.; Wilford, A.; Haskins, L.; Phakathi, S.; Mntambo, N.; Horwood, C.M. Trust of community health workers influences the acceptance of community-based maternal and child health services. Afr. J. Prim. Health Care Fam. Med. 2017, 9, e1–e8. [Google Scholar] [CrossRef] [PubMed]
- Muhumuza, G.; Mutesi, C.; Mutamba, F.; Ampuriire, P.; Nangai, C. Acceptability and Utilization of Community Health Workers after the Adoption of the Integrated Community Case Management Policy in Kabarole District in Uganda. Health Syst. Policy Res. 2015, 2, 13. [Google Scholar]
- Nelago, I. Contraceptive Choice and Use of Methods among Young Women in Namibia; African Population Studies: Accra, Ghana, 2008; Volume 23. [Google Scholar]
- University of Kinshasa School of Public Health; The Bill & Melinda Gates Institute for Population and Reproductive Health at The Johns Hopkins Bloomberg School of Public Health. Performance Monitoring for Action (PMA) Survey Phase 1, DRC Kinshasa_Phase 1 Results Brief_English_Final. Available online: https://www.pmadata.org/sites/default/files/data_product_results/DRC%20Kinshasa_Phase%201%20Results%20Brief_English_Final.pdf (accessed on 25 July 2021).
- Wood, K.; Jewkes, R. Blood Blockages and Scolding Nurses: Barriers to Adolescent Contraceptive Use in South Africa. Reprod. Health Matters 2006, 14, 109–118. [Google Scholar] [CrossRef]
- Koster, A.; Kemp, J.; Offei, A. Utilisation of Reproductive Health Services by Adolescent Boys in the East- ern Region of Ghana. Afr. J. Reprod. Health 2001, 5, 40–49. [Google Scholar] [CrossRef] [Green Version]
- Langhaug, L.F.; Cowan, F.M.; Nyamurera, T.; Power, R. Improving Young Peolpe’s Access to Reproductive Health Care in Rural Zimbabwe. AIDS Care 2003, 15, 147–157. [Google Scholar] [CrossRef]
- World Bank. Democratic Republic of Congo Urbanization Review: Productive and Inclusive Cities for an Emerging Democratic Republic of Congo. Directions in Development; World Bank: Washington, DC, USA, 2008. [CrossRef]
- Kaplan, B.; Nahum, R.; Yairi, Y.; Hirsch, M.; Pardo, J.; Yogev, Y.; Orvieto, R. Use of various contraceptive methods and time of conception in a community-based population. Eur. J. Obstet. Gynecol. Reprod. Biol. 2005, 123, 72–76. [Google Scholar] [CrossRef]
- Kulier, R.; O’Brien, P.A.; Helmerhorst, F.M.; Usher-Patel, M.; D’Arcangues, C. Copper containing, framed intra-uterine devices for contraception. Cochrane Database Syst. Rev. 2007, 4, CD005347. [Google Scholar]
- Akilimali, P.; Anglewicz, P.; Engale, H.N.; Kurhenga, G.K.; Hernandez, J.; Kayembe, P.; Bertrand, J. Differences in family planning outcomes between military and general populations in Kinshasa, Democratic Republic of the Congo: A cross-sectional analysis. BMJ Open 2018, 8, e022295. [Google Scholar] [CrossRef] [Green Version]
- Akilimali, P.Z.; Nzuka, H.E.; La Nasa, K.H.; Wumba, A.M.; Kayembe, P.; Wisniewski, J.; Bertrand, J.T. The gap in contraceptive knowledge and use between the military and non-military populations of Kinshasa, DRC, 2016–2019. PLoS ONE 2021, 16, e0254915. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Background Characteristics | Type of Neighborhood | Overall | p Value | ||||
|---|---|---|---|---|---|---|---|
| Nonslum | Slum | ||||||
| n | % | n | % | n | % | ||
| Age | 0.256 | ||||||
| 15–19 | 176 | 20.6 | 392 | 23.0 | 569 | 22.2 | |
| 20–24 | 175 | 20.4 | 362 | 21.2 | 537 | 20.9 | |
| 25–49 | 506 | 59.0 | 953 | 55.8 | 1458 | 56.9 | |
| Education | <0.001 | ||||||
| None/primary | 45 | 5.3 | 154 | 9.0 | 199 | 7.8 | |
| Secondary | 587 | 68.5 | 1281 | 75.0 | 1867 | 72.8 | |
| Tertiary | 225 | 26.3 | 272 | 15.9 | 497 | 19.4 | |
| Marital status | <0.001 | ||||||
| Never married | 473 | 55.1 | 817 | 47.8 | 1289 | 50.3 | |
| Currently married | 321 | 37.4 | 774 | 45.4 | 1095 | 42.7 | |
| Divorced or widowed | 64 | 7.4 | 116 | 6.8 | 180 | 7.0 | |
| Religion | 0.202 | ||||||
| Catholic | 156 | 18.2 | 312 | 18.3 | 468 | 18.3 | |
| Protestant | 74 | 8.6 | 186 | 10.9 | 260 | 10.1 | |
| Evangelical church | 414 | 48.3 | 766 | 44.9 | 1179 | 46.0 | |
| Other | 213 | 24.9 | 443 | 26.0 | 656 | 25.6 | |
| Ethnic | <0.001 | ||||||
| Bakongo | 247 | 28.8 | 457 | 26.8 | 704 | 27.4 | |
| Bas-Kkasai | 213 | 24.8 | 693 | 40.6 | 905 | 35.3 | |
| Kasai | 200 | 23.3 | 262 | 15.4 | 462 | 18.0 | |
| Cuvette/Ubangi | 69 | 8.1 | 193 | 11.3 | 263 | 10.2 | |
| Other | 128 | 14.9 | 102 | 6.0 | 230 | 9.0 | |
| Household wealth | <0.001 | ||||||
| Low | 178 | 20.8 | 677 | 39.7 | 855 | 33.4 | |
| Medium | 269 | 31.4 | 584 | 34.2 | 853 | 33.3 | |
| High | 409 | 47.8 | 446 | 26.1 | 855 | 33.4 | |
| Mean of age at first sexual intercourse | 17.55 ± 3.01 | 17.17 ± 2.82 | 17.26 ± 2.87 | 0.004 | |||
| Age at first sexual intercourse (1) | 0.082 | ||||||
| ≤16 | 283 | 40.8 | 648 | 45.9 | 932 | 44.2 | |
| 17–18 | 216 | 31.1 | 399 | 28.3 | 615 | 29.2 | |
| 19+ | 195 | 28.1 | 364 | 25.8 | 559 | 26.5 | |
| Visited by CHW | <0.001 | ||||||
| No | 844 | 98.5 | 1615 | 94.6 | 2459 | 95.9 | |
| Yes | 13 | 1.5 | 92 | 5.4 | 105 | 4.1 | |
| Parity | 0.008 | ||||||
| None | 394 | 45.9 | 678 | 39.7 | 1072 | 41.8 | |
| 1–2 | 228 | 26.6 | 492 | 28.8 | 720 | 28.1 | |
| 3+ | 235 | 27.4 | 537 | 31.4 | 772 | 30.1 | |
| Fertility preference | <0.001 | ||||||
| Have another soon | 198 | 23.2 | 237 | 13.9 | 436 | 17.0 | |
| Have another, undecided when | 81 | 9.5 | 256 | 15.0 | 337 | 13.2 | |
| Undecided or do not know | 6 | 0.7 | 86 | 5.1 | 93 | 3.6 | |
| Have another later | 428 | 50.0 | 788 | 46.2 | 1216 | 47.4 | |
| No more/cannot become pregnant | 143 | 16.7 | 339 | 19.9 | 482 | 18.8 | |
| Nonslum | Slum | Total | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Background Characteristics | N | n | % | N | n | % | N | n | % | |
| Age | ||||||||||
| 15–19 | 130 | 14 | 10.8 | 444 | 53 | 11.9 | 569 | 66 | 11.6 | 0.731 |
| 20–24 | 129 | 23 | 17.9 | 410 | 139 | 33.9 | 537 | 154 | 28.7 | <0.001 |
| 25–49 | 373 | 87 | 23.3 | 1078 | 330 | 30.6 | 1458 | 409 | 28.1 | 0.004 |
| Education | ||||||||||
| None or primary | 33 | 3 | 9.8 | 175 | 65 | 37.5 | 199 | 62 | 31.2 | 0.001 |
| Secondary | 433 | 76 | 17.6 | 1449 | 358 | 24.7 | 1867 | 420 | 22.5 | 0.001 |
| Tertiary | 166 | 45 | 27.0 | 308 | 98 | 32.0 | 497 | 148 | 29.7 | 0.258 |
| Marital status | ||||||||||
| Never married | 349 | 66 | 19.1 | 924 | 202 | 21.9 | 1289 | 269 | 20.8 | 0.275 |
| Currently married | 236 | 50 | 21.0 | 876 | 292 | 33.3 | 1095 | 325 | 29.7 | <0.001 |
| Divorced or widowed | 47 | 8 | 17.2 | 131 | 28 | 21.5 | 180 | 36 | 20.0 | 0.530 |
| Religion | ||||||||||
| Catholic | 115 | 21 | 18.0 | 353 | 102 | 28.7 | 468 | 118 | 25.2 | 0.011 |
| Protestant | 55 | 17 | 30.7 | 210 | 65 | 30.8 | 260 | 80 | 30.8 | 0.988 |
| Evangelic church | 305 | 55 | 17.9 | 867 | 228 | 26.3 | 1179 | 275 | 23.4 | 0.002 |
| Other | 157 | 32 | 20.3 | 502 | 128 | 25.5 | 656 | 156 | 23.8 | 0.010 |
| Ethnic | ||||||||||
| Bakongo | 182 | 33 | 18.2 | 517 | 141 | 27.2 | 704 | 169 | 24.0 | 0.008 |
| Bas-Kasai | 157 | 28 | 17.8 | 784 | 214 | 27.2 | 905 | 227 | 25.0 | 0.007 |
| Kasai | 147 | 35 | 23.5 | 297 | 75 | 25.2 | 462 | 113 | 24.5 | 0.695 |
| Cuvette/Ubangi | 51 | 16 | 31.7 | 219 | 66 | 30.0 | 263 | 80 | 30.5 | 0.812 |
| Other | 94 | 12 | 13.0 | 115 | 27 | 23.6 | 230 | 41 | 17.7 | 0.026 |
| Household wealth | ||||||||||
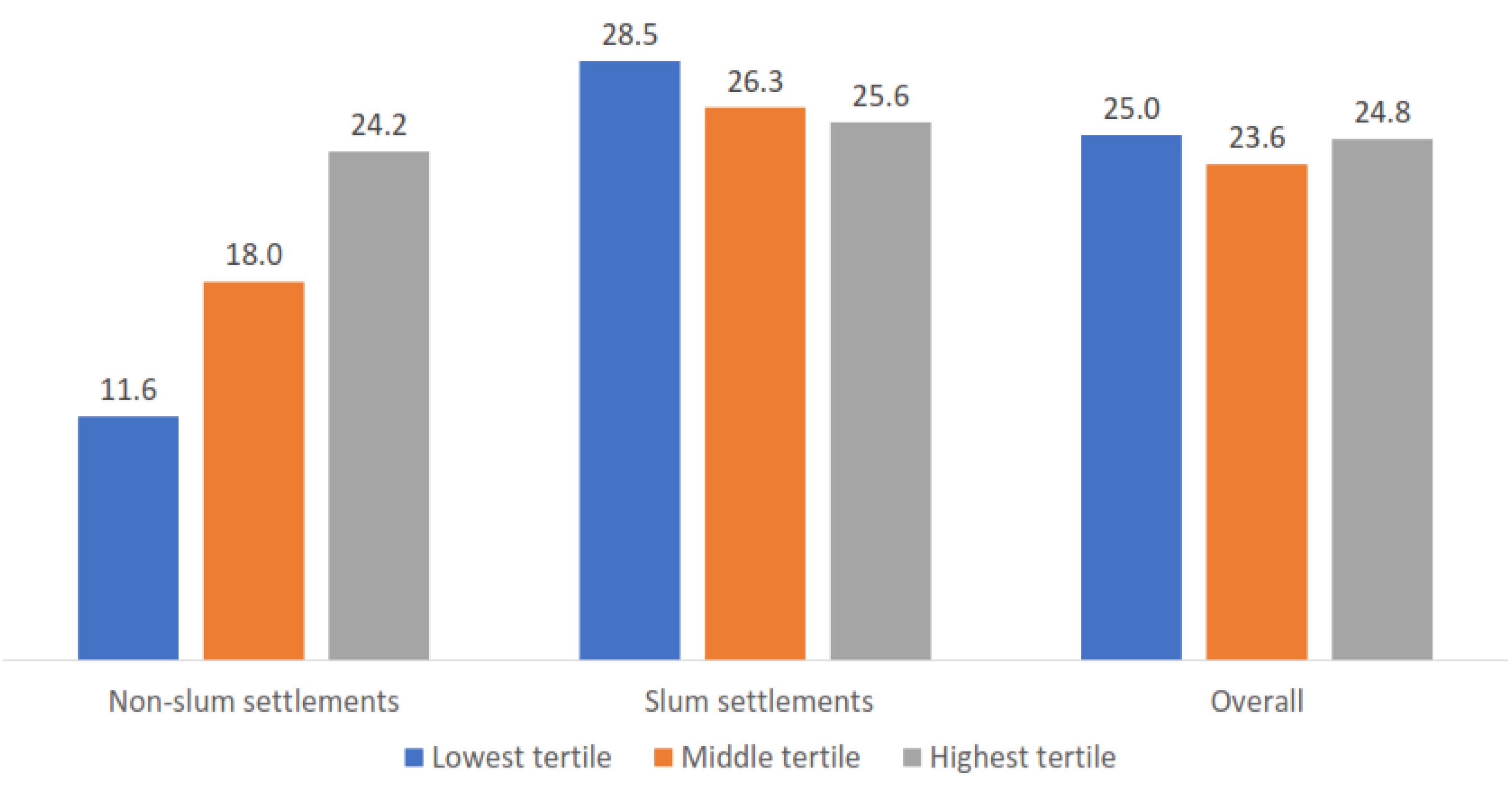
| Low | 131 | 15 | 11.6 | 767 | 219 | 28.5 | 855 | 214 | 25.0 | <0.001 |
| Medium | 199 | 36 | 18.0 | 661 | 174 | 26.3 | 853 | 202 | 23.7 | 0.008 |
| High | 302 | 73 | 24.2 | 504 | 129 | 25.6 | 855 | 213 | 24.9 | 0.657 |
| Age at first sexual intercourse (1) | ||||||||||
| ≤16 | 210 | 45 | 21.7 | 731 | 262 | 35.8 | 932 | 294 | 31.5 | 0.0001 |
| 17–18 | 160 | 43 | 27.0 | 450 | 143 | 31.7 | 615 | 185 | 30.0 | 0.267 |
| 19+ | 144 | 34 | 23.8 | 410 | 116 | 28.4 | 559 | 150 | 26.8 | 0.285 |
| Work | ||||||||||
| No | 309 | 53 | 17.1 | 994 | 244 | 24.6 | 1297 | 287 | 22.1 | 0.003 |
| Yes | 323 | 71 | 22.1 | 938 | 278 | 29.6 | 1267 | 342 | 27.0 | 0.005 |
| Parity | ||||||||||
| None | 290 | 43 | 14.9 | 768 | 131 | 17.1 | 1072 | 175 | 16.3 | 0.389 |
| 1–2 | 168 | 37 | 22.2 | 557 | 194 | 34.8 | 720 | 222 | 30.8 | 0.001 |
| 3+ | 173 | 44 | 25.2 | 607 | 197 | 32.4 | 772 | 233 | 30.2 | 0.035 |
| Fertility preference | ||||||||||
| Have another soon | 146 | 19 | 13.2 | 269 | 55 | 20.5 | 436 | 75 | 17.1 | 0.032 |
| Have another, undecided when | 60 | 5 | 9.1 | 290 | 62 | 21.3 | 337 | 62 | 18.4 | 0.014 |
| Undecided or do not know | 5 | 1 | 29.9 | 98 | 20 | 20.9 | 93 | 20 | 21.5 | 0.631 |
| Have another later | 316 | 70 | 22.3 | 892 | 267 | 30.0 | 1216 | 332 | 27.3 | 0.004 |
| No more or cannot become pregnant | 105 | 28 | 26.2 | 384 | 117 | 30.6 | 482 | 141 | 29.3 | 0.379 |
| Visited by CHW | ||||||||||
| No | 623 | 120 | 19.3 | 1828 | 476 | 26.0 | 2459 | 584 | 23.7 | <0.001 |
| Yes | 9 | 4 | 40.3 | 104 | 46 | 44.4 | 105 | 46 | 43.9 | 0.812 |
| Total | 632 | 124 | 19.6 | 1932 | 522 | 27.0 | 2564 | 630 | 24.6 | <0.001 |
| Non Slum (n = 341) % | Slums (n = 771) % | Overall (n = 1112) % | |
|---|---|---|---|
| Modern methods | |||
| Male condoms | 16.8 | 14.9 | 15.5 |
| Implants | 9.4 | 18.1 *** | 15.4 |
| Emergency contraception | 14.2 | 12.7 | 13.2 |
| Injectables, intramuscular | 2.8 | 5.4 * | 4.6 |
| Pills | 1.6 | 3.1 | 2.7 |
| Injectables, subcutaneous | 0.9 | 2.2 | 1.8 |
| Standard Days Method/CycleBeads | 1.9 | 1.5 | 1.6 |
| Female sterilization | 1.2 | 1.0 | 1.1 |
| Intrauterine device | 0.3 | 0.4 | 0.3 |
| Female condoms | 0.0 | 0.2 | 0.1 |
| Traditional methods | |||
| Rhythm methods | 36.6 ** | 27.9 | 30.6 |
| Withdrawal | 10.2 | 10.0 | 10.1 |
| Other traditional methods | 4.2 | 2.6 | 3.1 |
| Model 1 | Model 2 | |||
|---|---|---|---|---|
| Background Characteristics | aOR | 95% CI | aOR | 95% CI |
| Age | ||||
| 15–19 | 1 | 1 | ||
| 20–24 | 2.47 | 1.61–3.78 | 2.52 | 1.64–3.88 |
| 25–49 | 2.41 | 1.48–3.93 | 2.49 | 1.52–4.06 |
| Education | ||||
| None/primary education | 0.83 | 0.54–1.28 | 0.83 | 0.54–1.29 |
| Secondary | 0.58 | 0.42–0.79 | 0.57 | 0.42–0.78 |
| Tertiary | 1 | 1 | ||
| Marital status | ||||
| Never married | 1.35 | 0.94–1.93 | 1.40 | 0.97–2.00 |
| Currently married | 1 | 1 | ||
| Divorced or widowed | 0.63 | 0.40–0.99 | 0.64 | 0.40–1.01 |
| Ethnic | ||||
| Bakongo | 1 | 1 | ||
| Bas-kasai | 0.99 | 0.76–1.29 | 0.98 | 0.75–1.29 |
| Kasai | 1.13 | 0.79–1.60 | 1.10 | 0.78–1.56 |
| Cuvette/Ubangi | 1.31 | 0.91–1.89 | 1.28 | 0.88–1.87 |
| others | 0.73 | 0.44–1.21 | 0.73 | 0.44–1.22 |
| Parity | ||||
| None | 1 | 1 | ||
| 1–2 | 2.18 | 1.48–3.21 | 2.19 | 1.48–3.23 |
| 3+ | 2.26 | 1.39–3.65 | 2.28 | 1.41–3.69 |
| Fertility preference | ||||
| Have another soon | 1 | 1 | ||
| Have another, undecided when | 1.34 | 0.85–2.09 | 1.35 | 0.86–2.12 |
| Undecided or do not know | 1.41 | 0.77–2.57 | 1.42 | 0.78–2.59 |
| Have another later | 2.38 | 1.67–3.38 | 2.40 | 1.69–3.42 |
| No more or cannot become pregnant | 1.82 | 1.22–2.68 | 1.81 | 1.22–2.70 |
| Visited by CHWs | ||||
| No | 1 | 1 | ||
| Yes | 2.22 | 1.37–3.60 | 2.18 | 1.35–3.52 |
| Household wealth | ||||
| Low | 1 | 1 | ||
| Middle | 1.02 | 0.79–1.31 | 0.90 | 0.68–1.19 |
| High | 1.18 | 0.90–1.57 | 0.91 | 0.67–1.25 |
| Type of neighborhood | ||||
| Nonslum | 1 | 1 | ||
| Slum | 1.53 | 1.18–1.98 | 3.18 | 1.79–5.62 |
| Interaction terms (household wealth and neighborhood) | ||||
| Middle wealth and nonslum | 2.17 | 1.05–4.49 | ||
| High wealth and nonslum | 2.89 | 1.44–5.81 | ||
| Background Characteristics | Type of Neighborhood | |||||||
|---|---|---|---|---|---|---|---|---|
| Slum | Nonslum | |||||||
| OR | 95% CI | aOR | 95% CI | OR | 95% CI | aOR | 95% CI | |
| Age | ||||||||
| 15–19 | 1 | 1 | 1 | 1 | ||||
| 20–24 | 3.79 | 2.46–5.84 | 2.84 | 1.75–4.59 | 1.80 | 0.80–4.06 | 1.93 | 0.76–4.89 |
| 25–49 | 3.26 | 2.17–4.87 | 2.26 | 1.27–4.02 | 2.51 | 1.27–4.93 | 3.32 | 1.27–8.69 |
| Education | ||||||||
| None or primary | 1.27 | 0.81–1.99 | 1.04 | 0.64–1.71 | 0.29 | 0.09–0.86 | 0.28 | 0.09–0.85 |
| Secondary | 0.69 | 0.52–0.94 | 0.63 | 0.44–0.98 | 0.57 | 0.34–0.97 | 0.49 | 0.26–0.90 |
| Tertiary | 1 | 1 | 1 | 1 | ||||
| Marital status | ||||||||
| Never married | 0.56 | 0.44–0.72 | 1.12 | 0.74–1.70 | 0.88 | 0.53–1.48 | 2.39 | 1.12–5.10 |
| Currently married | 1 | 1 | 1 | 1 | ||||
| Divorced or widowed | 0.55 | 0.33–0.91 | 0.57 | 0.33–0.98 | 0.78 | 0.34–1.80 | .92 | 0.37–2.28 |
| Ethnic | ||||||||
| Bakongo | 1 | 1 | 1 | |||||
| Bas-Kasai | 1.00 | 0.75–1.34 | 0.96 | 0.72–1.29 | 0.98 | 0.52–1.85 | 1.01 | 0.52–1.95 |
| kasai | 0.90 | 0.61–1.33 | 0.95 | 0.64–1.41 | 1.39 | 0.71–2.70 | 1.52 | 0.76–3.08 |
| Cuvette or Ubangi | 1.15 | 0.77–1.71 | 1.09 | 0.72–1.67 | 2.10 | 0.99–4.42 | 1.91 | 0.87–4.20 |
| Other | 0.82 | 0.48–1.40 | 0.87 | 0.46–1.65 | 0.67 | 0.29–1.54 | 0.72 | 0.30–1.69 |
| Parity | ||||||||
| None | 1 | 1 | 1 | 1 | ||||
| 1–2 | 2.59 | 1.89–3.55 | 2.16 | 1.35–3.46 | 1.63 | 0.93–2.85 | 1.93 | 0.89–4.21 |
| 3+ | 2.32 | 1.70–3.15 | 2.20 | 1.23–3.95 | 1.92 | 1.12–3.30 | 2.32 | 0.94–5.73 |
| Fertility preference | ||||||||
| Have another soon | 1 | 1 | 1 | |||||
| Have another, undecided when | 1.05 | 0.66–1.69 | 1.44 | 0.86–2.39 | 0.66 | 0.26–1.68 | 0.77 | 0.29–2.08 |
| Undecided or do not know | 1.02 | 0.54–1.93 | 1.21 | 0.63–2.30 | 2.81 | 0.50–15.95 | 4.54 | 0.86–24.01 |
| Have another later | 1.66 | 1.15–2.41 | 2.11 | 1.42–3.16 | 1.89 | 1.01–3.54 | 3.11 | 1.58–6.11 |
| No more or cannot become pregnant | 1.72 | 1.15–2.57 | 1.50 | 0.95–2.36 | 2.34 | 1.12–4.87 | 2.99 | 1.35–6.62 |
| Visited by CHW | ||||||||
| No | 1 | 1 | 1 | 1 | ||||
| Yes | 2.27 | 1.40–3.67 | 2.14 | 1.29–3.53 | 2.81 | 0.59–13.44 | 2.21 | 0.47–10.43 |
| Household wealth | ||||||||
| Low | 1 | 1 | 1 | 1 | ||||
| Middle | 0.89 | 0.68–1.17 | 0.90 | 0.68–1.90 | 1.68 | 0.85–3.31 | 1.92 | 0.97–3.82 |
| High | 0.86 | 0.65–1.14 | 0.91 | 0.67–1.25 | 2.43 | 1.28–4.61 | 2.44 | 1.24–4.82 |
| N | 1886 | 635 | ||||||
| Variance inflation factor | 2.66 | 2.38 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akilimali, P.Z.; Tran, N.-T.; Gage, A.J. Heterogeneity of Modern Contraceptive Use among Urban Slum and Nonslum Women in Kinshasa, DR Congo: Cross-Sectional Analysis. Int. J. Environ. Res. Public Health 2021, 18, 9400. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179400
Akilimali PZ, Tran N-T, Gage AJ. Heterogeneity of Modern Contraceptive Use among Urban Slum and Nonslum Women in Kinshasa, DR Congo: Cross-Sectional Analysis. International Journal of Environmental Research and Public Health. 2021; 18(17):9400. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179400
Chicago/Turabian StyleAkilimali, Pierre Z., Nguyen-Toan Tran, and Anastasia J. Gage. 2021. "Heterogeneity of Modern Contraceptive Use among Urban Slum and Nonslum Women in Kinshasa, DR Congo: Cross-Sectional Analysis" International Journal of Environmental Research and Public Health 18, no. 17: 9400. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179400