
Psychometric Properties of the 34-Item Short-Form Supportive Care Need Survey (SCNS-SF34) Scale in the Malaysian Cancer Healthcare Context

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sampling and Data Collection Procedure
2.2. Ethical Consideration
2.3. Instrumentation
2.4. Data Analysis Procedure
3. Results
3.1. Participants’ Characteristics
3.2. Reliability
3.3. Factor Analysis
3.3.1. Exploratory Factor Analysis
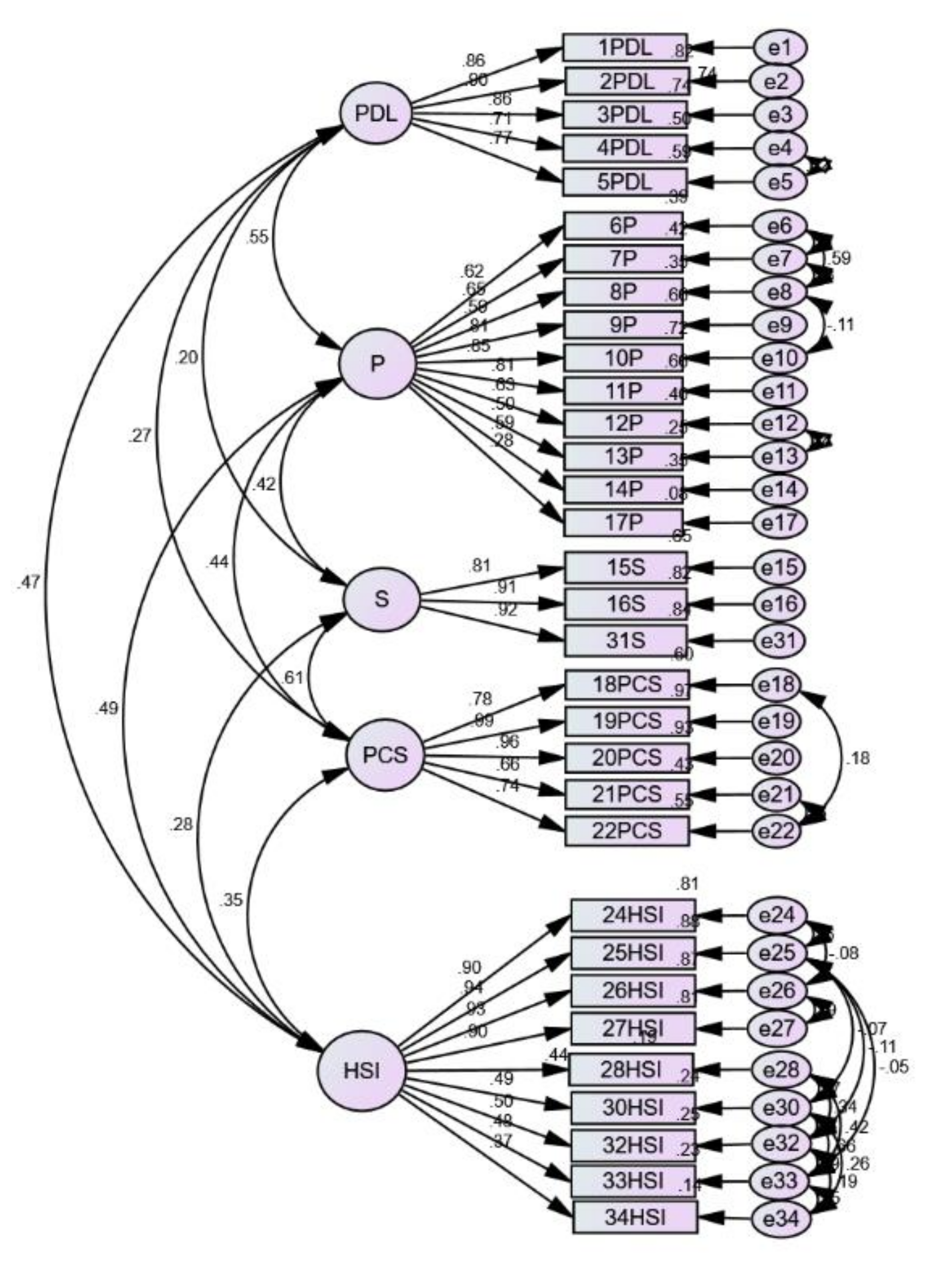
3.3.2. Confirmatory Factor Analysis
3.4. Discriminant Validity
4. Discussion
5. Conclusions and Future Recommendation
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Epplein, M.; Zheng, Y.; Zheng, W.; Chen, Z.; Gu, K.; Penson, D.; Lu, W.; Shu, X.-O. Quality of life after breast cancer diagnosis and survival. J. Clin. Oncol. 2011, 29, 406–412. [Google Scholar] [CrossRef] [Green Version]
- Uchida, M.; Akechi, T.; Okuyama, T.; Sagawa, R.; Nakaguchi, T.; Endo, C.; Yamashita, H.; Toyama, T.; Furukawa, T.A. Patients’ supportive care needs and psychological distress in advanced breast cancer patients in Japan. Jpn. J. Clin. Oncol. 2011, 41, 530–536. [Google Scholar] [CrossRef] [Green Version]
- Park, B.W.; Hwang, S.Y. Unmet needs of breast cancer patients relative to survival duration. Yonsei Med. J. 2012, 53, 118–125. [Google Scholar] [CrossRef] [Green Version]
- Bonevski, B.; Sanson-Fisher, R.; Girgis, A.; Burton, L.; Cook, P.; Boyes, A.; the Supportive Care Review Group. Evaluation of an instrument to assess the needs of patients with cancer. Cancer 2000, 88, 217–225. [Google Scholar] [PubMed]
- Macleduff, P.; Boyes, A.; Zucca, A.; Girgis, A. Supportive Care Needs Survey: A Guide to Administration, Scoring and Analysis; Centre for Health Research & Psycho-Oncology: Newcastle, UK, 2004. [Google Scholar]
- Boyes, A.; Girgis, A.; Lecathelinais, C. Brief assessment of adult cancer patients’ perceived needs: Development and validation of the 34-item supportive care needs survey (SCNS-SF34). J. Eval. Clin. Pract. 2009, 15, 602–606. [Google Scholar] [CrossRef] [PubMed]
- Au, A.; Lam, W.W.T.; Kwong, A.; Suen, D.; Tsang, J.; Yeo, W.; Suen, J.; Ho, W.M.; Yau, T.K.; Soong, I.; et al. Validation of the Chinese version of the Short-form Supportive Care Needs Survey Questionnaire (SCNS-SF34-C). Psychooncology 2011, 20, 1292–1300. [Google Scholar] [CrossRef]
- Li, W.W.Y.; Lam, W.W.T.; Shun, S.C.; Lai, Y.H.; Law, W.L.; Poon, J.; Fielding, R. Psychometric Assessment of the Chinese Version of the Supportive Care Needs Survey Short-Form (SCNS-SF34-C) among Hong Kong and Taiwanese Chinese Colorectal Cancer Patients. PLoS ONE 2013, 8, e75755. [Google Scholar] [CrossRef] [Green Version]
- Choi, E.P.H.; Liao, Q.; Soong, I.; Chan, K.K.L.; Lee, C.C.Y.; Ng, A.; Sze, W.K.; Tsang, J.W.H.; Lee, V.H.F.; Lam, W.W.T. Measurement invariance across gender and age groups, validity and reliability of the Chinese version of the short-form supportive care needs survey questionnaire (SCNS-SF34). Health Qual. Life Outcomes 2020, 18, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.Y.; Park, B.W. The perceived care needs of breast cancer patients in Korea. Yonsei Med. J. 2006, 47, 524–533. [Google Scholar] [CrossRef] [Green Version]
- Okuyama, T.; Akechi, T.; Yamashita, H.; Toyama, T.; Endo, C.; Sagawa, R.; Uchida, M.; Furukawa, T.A. Reliability and validity of the Japanese version of the Short-form Supportive Care Needs Survey Questionnaire (SCNS-SF34-J). Psychooncology 2009, 18, 1003–1010. [Google Scholar] [CrossRef] [PubMed]
- Brédart, A.; Kop, J.L.; Griesser, A.C.; Zaman, K.; Panes-Ruedin, B.; Jeanneret, W.; Delaloye, J.-F.; Zimmers, S.; Jacob, A.; Berthet, V.; et al. Validation of the 34-item Supportive Care Needs Survey and 8-item Breast module French versions (SCNS-SF34-Fr and SCNS-BR8-Fr) in breast cancer patients. Eur. J. Cancer Care 2012, 21, 450–459. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, C.; Koch, U.; Mehnert, A. Psychometric properties of the German version of the Short-Form Supportive Care Needs Survey Questionnaire (SCNS-SF34-G). Support. Care Cancer 2012, 20, 2415–2424. [Google Scholar] [CrossRef] [PubMed]
- Doubova, S.V.; Aguirre-Hernandez, R.; Gutiérrez-de la Barrera, M.; Infante-Castañeda, C.; Pérez-Cuevas, R. Supportive care needs of Mexican adult cancer patients: Validation of the Mexican version of the Short-Form Supportive Care Needs Questionnaire (SCNS-SFM). Support. Care Cancer 2015, 23, 2711–2719. [Google Scholar] [CrossRef]
- Ozbayir, T.; Geckil, O.S.; Aslan, A. An Adaptation of the Short-Form Supportive Care Needs Survey Questionnaire (SCNS-SF 34) into Turkish. Eur. J. Breast Health 2017, 13, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Edib, Z.; Kumarasamy, V.; Abdullah, N.B.; Rizal, A.M.; Al-Dubai, S.A.R. Most prevalent unmet supportive care needs and quality of life of breast cancer patients in a tertiary hospital in Malaysia. Health Qual. Life Outcomes 2016, 14, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Fong, E.J.; Cheah, W.L. Unmet Supportive Care Needs among Breast Cancer Survivors of Community-Based Support Group in Kuching, Sarawak. Int. J. Breast Cancer 2016, 2016, 7297813. [Google Scholar] [CrossRef] [Green Version]
- Karthikeyan, G.; Manoor, U.; Supe, S.S. Translation and validation of the questionnaire on current status of physiotherapy practice in the cancer rehabilitation. J. Cancer Res. Ther. 2015, 11, 29–36. [Google Scholar] [CrossRef]
- Memon, M.A.; Ting, H.; Ramayah, T.; Chuah, F.; Cheah, J.-H. A Review of the Methodological Misconceptions and Guidelines Related To the Application of Structural Equation Modeling: A Malaysian Scenario. J. Appl. Struct. Equ. Model. 2017, 1, i–xiii. [Google Scholar] [CrossRef]
- Anderson, J.C.; Gerbing, D.W. Predicting the Performance of Measures in a Confirmatory Factor Analysis with a Pretest Assessment of Their Substantive Validities. J. Appl. Psychol. 1991, 76, 732–740. [Google Scholar] [CrossRef]
- Goetz, C.; Coste, J.; Lemetayer, F.; Rat, A.C.; Montel, S.; Recchia, S.; Debouverie, M.; Pouchot, J.; Spitz, E.; Guillemin, F. Item reduction based on rigorous methodological guidelines is necessary to maintain validity when shortening composite measurement scales. J. Clin. Epidemiol. 2013, 66, 710–718. [Google Scholar] [CrossRef] [PubMed]
- Heene, M.; Bollmann, S.; Bühner, M. Much ado about nothing, or much to do about something?Effects of scale shortening on criterion validity and mean differences. J. Individ. Differ. 2014, 35, 245–249. [Google Scholar] [CrossRef]
- Zun, A.B.; Ibrahim, M.I.; Mokhtar, A.M.; Halim, A.S.; Wan Mansor, W.N.A. Translation, cross-cultural adaptation, and validation of the hospital consumer assessment of healthcare providers and systems (HCAHPS) into the Malay language. Int. J. Environ. Res. Public Health 2019, 16, 2054. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dedic, A. Mesurement in Business Research: A paradigm for developing better measures of marketing constructs. Course Mes. Bus. Res. 2012, 19. Available online: http://0-www-jstor-org.brum.beds.ac.uk/stable/3150876?origin=crossref (accessed on 26 May 2021).
- Schreiber, J.B.; Stage, F.K.; King, J.; Nora, A.; Barlow, E.A. Reporting structural equation modeling and confirmatory factor analysis results: A review. J. Educ. Res. 2006, 99, 323–338. [Google Scholar] [CrossRef]
- Kurian, A.W.; Bondarenko, I.; Jagsi, R.; Friese, C.R.; McLeod, M.C.; Hawley, S.T.; Hamilton, A.S.; Ward, K.C.; Hofer, T.P.; Katz, S.J. Recent Trends in Chemotherapy Use and Oncologists’ Treatment Recommendations for Early-Stage Breast Cancer. J. Natl. Cancer Inst. 2018, 110, 493–500. [Google Scholar] [CrossRef] [Green Version]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Floyd, F.J.; Widaman, K.F. Factor Analysis in the Development and Refinement of Clinical Assessment Instruments. Psychol. Assess. 1995, 7, 286–299. [Google Scholar] [CrossRef]
- Yusoff, M.S.B.; Rahim, A.F.A.; Pa, M.N.M.; Mey, S.C.; Ja’Afar, R.; Esa, A.R. The validity and reliability of USM emotional quotient inventory (USMEQ-i): Its use to measure emotional quotient (EQ) of future medical students. Int. Med. J. 2011, 18, 293–299. [Google Scholar]
- Rahlin, N.A.; Awang, Z.; Abdul Rahim, M.Z.; Bahkia, A.S. The impact of employee safety climate on safety behavior in small & medium enterprises: An empirical study. Humanit. Soc Sci Rev. 2020, 8, 163–177. [Google Scholar]
- Zainuddin, A. Overview of Structural Equation Modeling (SEM). In A Handbook on SEM; University Technology MARA Press: Kelantan, Malaysia, 2012; pp. 1–17. [Google Scholar]
- Hair, J.; Black, W.; Babin, B.; Anderson, R. Multivariate Data Analysis: A Global Perspective. In Multivariate Data Analysis: A Global Perspective, 7th ed.; Pearson: London, UK, 2010; Volume 7. [Google Scholar]
- Ab Hamid, M.R.; Sami, W.; Mohmad Sidek, M.H. Discriminant Validity Assessment: Use of Fornell & Larcker criterion versus HTMT Criterion. J. Phys. Conf. Ser. 2017, 890, 012163. [Google Scholar]
- So, W.K.W.; Chow, K.M.; Chan, H.Y.L.; Choi, K.C.; Wan, R.W.M.; Mak, S.S.S.; Chair, S.Y.; Chan, C.W. Quality of life and most prevalent unmet needs of Chinese breast cancer survivors at one year after cancer treatment. Eur. J. Oncol. Nurs. 2014, 18, 323–328. [Google Scholar] [CrossRef] [PubMed]
- Matheson, G.J. We need to talk about reliability: Making better use of test-retest studies for study design and interpretation. PeerJ 2019, 7, e6918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fiszer, C.; Dolbeault, S.; Sultan, S.; Brédart, A. Prevalence, intensity, and predictors of the supportive care needs of women diagnosed with breast cancer: A systematic review. Psychooncology 2014, 23, 361–374. [Google Scholar] [CrossRef] [PubMed]
- Sanson-Fisher, R.; Girgis, A.; Boyes, A.; Bonevski, B.; Burton, L.; Cook, P.; Supportive Care Review Group. The unmet supportive care needs of patients with cancer. Cancer 2000, 88, 226–237. [Google Scholar] [PubMed] [Green Version]
- Davis, M.C.; Matthews, K.A.; Twamley, E.W. Is life more difficult on mars or venus?A meta-analytic review of sex differences in major and minor life events. Ann. Behav. Med. 1999, 21, 83–97. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Patients’ Characteristics | n (%) |
|---|---|
| Gender | |
| Male | 17 (9.9) |
| Female | 154 (90.1) |
| Age (mean ± SD) | 52.21 ± 9.05 |
| Max (years) | 76 |
| Min (years) | 27 |
| Diagnosis * | |
| Breast cancer | 127 (74.3) |
| Colorectal cancer | 6 (3.5) |
| Cervical cancer | 3 (1.8) |
| Lung cancer | 2 (1.2) |
| Nasopharyngeal cancer | 2 (1.2) |
| Lymphoma cancer | 1 (0.6) |
| Oral cancer | 1 (0.6) |
| Skin cancer | 1 (0.6) |
| Synovial sarcoma | 1 (0.6) |
| Throat cancer | 1 (0.6) |
| Treatment received | |
| Chemotherapy | 51 (29.8) |
| Radiotherapy | 49 (28.7) |
| Surgery | 50 (29.2) |
| Hormone | 2 (1.2) |
| Factor and Item Number | Mean ± Standard Deviation | Floor Score (%) | Ceiling Score (%) | Factor Loadings | Cronbach Alpha | Eigenvalues | Total Variance Explained (%) |
|---|---|---|---|---|---|---|---|
| Physical and daily living needs (PDL) | 1.99 (0.98) | 44.0% | 4.3% | ||||
| Item 1 | 1.94 | 0.801 | 0.918 | 35.698 | 34.864 | ||
| Item 2 | 2.05 | 0.838 | |||||
| Item 3 | 1.71 | 0.831 | |||||
| Item 4 | 2.11 | 0.820 | |||||
| Item 5 | 2.16 | 0.831 | |||||
| Psychological needs (P) | 1.92 (0.54) | 30.6% | 0.7% | ||||
| Item 6 | 1.64 | 0.628 | 0.883 | 12.449 | 11.669 | ||
| Item 7 | 1.45 | 0.649 | |||||
| Item 8 | 1.74 | 0.640 | |||||
| Item 9 | 2.20 | 0.686 | |||||
| Item 10 | 2.01 | 0.729 | |||||
| Item 11 | 2.09 | 0.704 | |||||
| Item 12 | 2.11 | 0.627 | |||||
| Item 13 | 2.24 | 0.574 | |||||
| Item 14 | 1.89 | 0.662 | |||||
| Item 17 | 1.80 | 0.334 | |||||
| Sexuality needs (S) | 1.90 (0.80) | 38.8% | 0.6% | ||||
| Item 15 | 1.96 | 0.578 | 0.901 | 7.981 | 7.240 | ||
| Item 16 | 1.74 | 0.527 | |||||
| Item 31 | 1.99 | 0.623 | |||||
| Patient care and support needs (PCS) | 2.16 (0.90) | 29.8% | 1.8% | ||||
| Item 18 | 1.84 | 0.744 | 0.929 | 6.168 | 5.287 | ||
| Item 19 | 2.18 | 0.806 | |||||
| Item 20 | 2.22 | 0.824 | |||||
| Item 21 | 2.12 | 0.778 | |||||
| Item 22 | 2.46 | 0.844 | |||||
| Health system and information needs (HSI) | 2.73 (0.88) | 15.2% | 10.4% | ||||
| Item 23 | 2.81 | 0.459 | 0.918 | 4.823 | 4.048 | ||
| Item 24 | 2.42 | 0.812 | |||||
| Item 25 | 2.44 | 0.834 | |||||
| Item 26 | 2.57 | 0.796 | |||||
| Item 27 | 2.49 | 0.805 | |||||
| Item 28 | 3.18 | 0.755 | |||||
| Item 29 | 3.23 | 0.800 | |||||
| Item 30 | 2.92 | 0.803 | |||||
| Item 32 | 2.58 | 0.598 | |||||
| Item 33 | 3.15 | 0.725 | |||||
| Item 34 | 2.25 | 0.520 |
| Domain | PDL | P | S | PCS | HSI |
|---|---|---|---|---|---|
| PDL | |||||
| P | 0.506 ** | ||||
| S | 0.200 ** | 0.392 ** | |||
| PCS | 0.282 ** | 0.416 ** | 0.552 ** | ||
| HSI | 0.387 ** | 0.454 ** | 0.455 ** | 0.569 ** |
| Domain | Mean (SD) | p-Value * | |
|---|---|---|---|
| Male | Female | ||
| Physical and daily living needs (PDL) | 2.48 (0.98) | 1.94 (0.97) | 0.029 ** |
| Psychological needs (P) | 2.01 (0.59) | 1.91 (0.53) | 0.443 |
| Sexuality needs (S) | 1.65 (0.58) | 1.93 (0.82) | 0.172 |
| Patient care and support needs (PCS) | 1.99 (0.81) | 2.18 (0.91) | 0.400 |
| Health system and information needs (HSI) | 2.33 (0.60) | 2.78 (0.90) | 0.010 ** |
| Domain | Mean (SD) | p-Value * | ||
|---|---|---|---|---|
| <40 Years | 40–49 Years | ≥50 Years | ||
| Physical and daily living needs (PDL) | 2.11 (1.03) | 1.87 (0.87) | 2.10 (1.02) | 0.491 |
| Psychological needs (P) | 1.89 (0.30) | 2.01 (0.63) | 1.88 (0.56) | 0.552 |
| Sexuality needs (S) | 2.52 (0.90) | 2.40 (0.69) | 1.94 (0.71) | 0.004 ** |
| Patient care and support needs (PCS) | 2.86 (0.76) | 2.40 (0.95) | 2.23 (0.92) | 0.206 |
| Health system and information needs (HSI) | 3.05 (0.71) | 3.06 (0.96) | 2.98 (0.86) | 0.899 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Azman, N.; Thien, L.M.; Abdullah, M.F.I.L.; Mohd Shariff, N. Psychometric Properties of the 34-Item Short-Form Supportive Care Need Survey (SCNS-SF34) Scale in the Malaysian Cancer Healthcare Context. Int. J. Environ. Res. Public Health 2021, 18, 9403. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179403
Azman N, Thien LM, Abdullah MFIL, Mohd Shariff N. Psychometric Properties of the 34-Item Short-Form Supportive Care Need Survey (SCNS-SF34) Scale in the Malaysian Cancer Healthcare Context. International Journal of Environmental Research and Public Health. 2021; 18(17):9403. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179403
Chicago/Turabian StyleAzman, Nizuwan, Lei Mee Thien, Mohammad Farris Iman Leong Abdullah, and Noorsuzana Mohd Shariff. 2021. "Psychometric Properties of the 34-Item Short-Form Supportive Care Need Survey (SCNS-SF34) Scale in the Malaysian Cancer Healthcare Context" International Journal of Environmental Research and Public Health 18, no. 17: 9403. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18179403