1. Introduction
The increasing prevalence of cardiovascular (CV) risk factors which include Metabolic Syndrome (MetS) represents a public health issue of growing concern [
1]. MetS is defined by a clustering of CV risk factors which include central obesity, dyslipidaemia, elevated blood glucose and elevated blood pressure [
2]. Individuals with MetS were twice as likely to develop CV events, namely, heart attack and stroke [
3]. The prevalence of MetS globally has reached epidemic proportion [
4]. In Malaysia, 43.4% of Malaysian adults have MetS [
5]. The Chronic Care Model (CCM) is a guide to transform the management of chronic conditions including MetS to improve outcomes in primary care [
6]. It is a conceptual model for restructuring the healthcare system to ensure productive interactions between an informed, activated patient and a proactive, prepared practice team [
7]. The CCM focuses on optimizing 6 interrelated key elements which include healthcare organization, delivery system design, patient self-management support, clinical information system, decision support and use of community resources [
8].
Self-management support has been recognized as one of the most important components of the CCM [
9]. Evidence has shown that self-management support by healthcare professionals and utilization of self-management tools were effective in improving knowledge, motivation, self-management behaviours and health outcomes in patients with MetS [
10,
11,
12,
13,
14]. In Malaysia, a self-management support tool named the EMPOWER-PAR Global CV Risks Self-Management Booklet
© was developed in the EMPOWER-PAR study [
15,
16]. This booklet has recently been revised to become the EMPOWER-SUSTAIN Global CV Risks Self-Management Booklet
©. It is given to patients so that they can be empowered to actively participate in the management of their own health. Therefore, it is important to assess the usability of this self-management booklet among the target population to ensure its usefulness.
Usability is defined as “the extent to which a product can be used by a specific user for a specific goal in a specific context or environment, and provides a satisfying experience” [
17]. Two types of study that can be used to assess usability are qualitative or quantitative studies. One of the quantitative methods to assess usability is by using a questionnaire. The System Usability Scale (SUS) is one of the most widely used questionnaires to assess the usability of mobile apps [
18]. It consists of 10 items which can be answered on a five-point Likert scale ranging from “strongly disagree” to “strongly agree”. SUS has been translated into various languages, i.e., Indonesian, Spanish, French, Dutch, Portuguese, Slovenian, Persian, German, and more recently into the Malay language, which is called the “
Skala Kebolehgunaan Aplikasi Mudah Alih” (SKAMA) (
Appendix A) [
19]. However, to the best of our knowledge, there is no available questionnaire that assesses the usability of a self-management booklet. Thus, the first objective of this study was to adapt SKAMA into the EMPOWER-SUSTAIN Usability Questionnaire (E-SUQ) to assess usability of the EMPOWER-SUSTAIN Global CV Risks Self-Management Booklet
© exploring the extent to which this book can be used by patients with MetS in primary care and their personal experience. The second objective was to validate the questionnaire among patients with MetS in primary care.
2. Materials and Methods
2.1. Study Design and Population
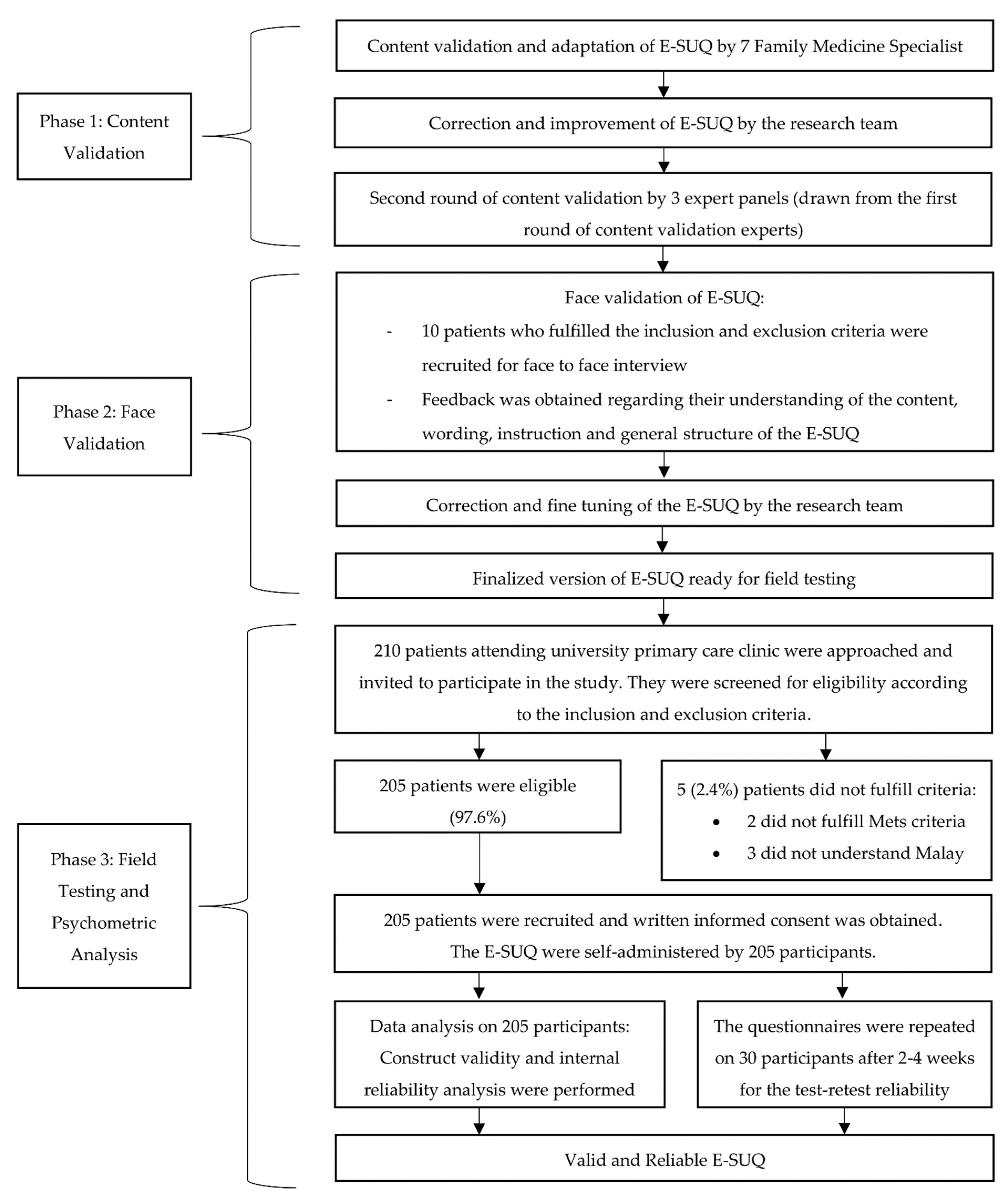
This was a cross-sectional validation study that was conducted in three phases. The first phase consisted of adaptation and content validation of the E-SUQ. This was followed by face validation in the second phase, and field testing and psychometric evaluation of the questionnaire in the final phase. The study population included patients with MetS attending a university primary care clinic in Selangor, Malaysia. It was conducted based on the Consensus-based Standards for the selection of health Measurement Instruments (COSMIN) guideline and principles of good practice for validation of a questionnaire [
20,
21]. The conduct of the study is shown in the flowchart presented in
Figure 1.
The inclusion criteria were as follows: (a) aged 18–80 years old; (b) attended the university primary care clinic for at least one year; (c) given the EMPOWER-SUSTAIN Global CV Risks Self-Management Booklet
© for ≥6 months; (d) had blood investigations (Fasting Plasma Glucose (FPG), Fasting Serum Lipid (FSL) and HbA1c) done in the last one year; (e) fulfilled at least 3 out of 5 diagnostic criteria for MetS based on the 2008 Joint Interim Statement definition [
2] (i.e., waist circumference South Asian cut points: male ≥ 90 cm, female ≥ 80 cm; systolic blood pressure (BP) ≥ 130 and/or diastolic BP ≥ 85 mmHg or on treatment for hypertension (HTN); FPG ≥ 5.6 mmol/L or on treatment for elevated glucose; triglycerides (TG) ≥ 1.7 mmol/L or on treatment for dyslipidaemia; high-density lipoprotein-cholesterol (HDL-C): male < 1.0 mmol/L, female < 1.3 mmol/L or on treatment for dyslipidaemia); (f) were able to read and understand the Malay language and (g) willing to participate in the study.
The following patients were excluded from the study: (a) diagnosed with circulatory disorders requiring secondary care over the past year (e.g., acute coronary syndrome, stroke, transient ischemic attacks, peripheral vascular disease); (b) on renal dialysis; (c) presented with severe HTN (systolic BP > 180 mmHg and/or diastolic BP > 110 mmHg); (d) on radiotherapy/chemotherapy or palliative care; (e) had any form of mental disorder or cognitive impairment that would affect the ability to answer the questionnaire, for example, dementia or mental retardation; (f) pregnant; and (g) unable to give informed consent.
2.2. Study Tool
The E-SUQ in this study was adapted from SKAMA to assess the level of usability of the EMPOWER-SUSTAIN Global CV Risks Self-Management Booklet
©. SKAMA is a 10-item questionnaire in the Malay language which assesses the usability of mobile apps, in which the response score is calculated using the 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). The item score on the positively phrased statements is subtracted by 1 (x − 1) and the item score on the negatively phrased statements is calculated by subtracting the score from 5 (5 − x) [
22]. The overall score is computed as the summation of all item scores multiplied by 2.5, which gives the overall score that ranged from 0 (extremely poor usability) to 100 (excellent usability). The score value of > 68 is recommended by the original author to indicate the cut-off point for good usability of an app [
23]. Permission to adapt and validate SKAMA into E-SUQ was obtained from the researchers.
2.3. Phase 1: Adaptation and Content Validation
The SKAMA underwent a process of adaptation into E-SUQ. Each item in the questionnaire which assessed the usability of mobile application was adapted to assess the usability of the self-management booklet. The word “mobile application” was substituted with “self-management booklet” in the Malay version.
Content validation was conducted through an online survey by seven family medicine specialists who are experts in questionnaire validation. They are clinical experts with a special interest in patient empowerment and chronic disease management. According to the literature, content validation should include at least five experts to have sufficient control over chance agreement [
24]. The original 10-item SKAMA was critically reviewed by the panels for clarity and relevance to the conceptual framework. The items were rated on a scale from 1 to 4 (1 = not relevant, 2 = somewhat relevant, 3 = quite relevant, 4 = highly relevant). The item level content validity index (I-CVI) was computed for each item by dichotomizing the 4-point scale. Items with a score of either 1 or 2 were recategorized into “not relevant” with 0 point. Items with a score of either 3 or 4 were recategorized into “relevant” with 1 point. The values (0 or 1) for each item were added up and then the total value was divided by the total number of experts [
25]. An I-CVI value of at least 0.83 determined that the items were relevant and to be retained in the questionnaire [
26]. Two rounds of content validity were conducted in this study because a major revision was required for item 5. After the second round, the scale level content validity index based on the average method (S-CVI/Ave) was computed to evaluate the relevance of the revised questionnaire. S-CVI/Ave is the average of the I-CVI scores for all items on the scale or the average of proportion relevance judged by all experts [
25]. S-CVI/Ave value of >0.90 indicates that the item should be retained [
27].
2.4. Phase 2: Face Validation
The face validation process was done through a face-to-face interview on a sample of 10 patients who met the inclusion and exclusion criteria. They were asked to comment on the questionnaire’s instructions, contents, terminology, comprehensibility and overall structure. Correction and fine-tuning of the E-SUQ were conducted by the research team based on the patient’s feedback. Face validity index (FVI) was used to evaluate the items in the form of clarity and comprehensibility of language and instructions used in the questionnaire [
28]. The participants were requested to rate the comprehensibility of each item to the conceptual framework on a scale from 1 to 4 (1 = not understandable, 2 = somewhat understandable, 3 = understandable, 4 = very understandable). The item level-FVI (I-FVI) was computed for each item by dichotomizing the 4-point scale, with items scoring either 1 or 2 being recoded as 0 and items with a score of either 3 or 4 being recoded as 1 [
29]. The values (0 or 1) for each item were added up and then the total value was divided by the total number of experts. Marzuki et al. suggested that if the number of raters is 10, the acceptable cut-off score of FVI is at least 0.83 [
19]. This process produced the refined E-SUQ, which was ready to undergo the psychometric evaluation.
2.5. Phase 3: Field Testing and Psychometric Evaluation
In the final phase, the E-SUQ went through field testing for psychometric evaluation. The same inclusion and exclusion criteria were applied to the recruited participants. However, participants who were involved in Phase 2 were not included in Phase 3 of this study.
2.5.1. Sample Size Determination
The sample size for the psychometric evaluation was calculated using the sample-to-variable ratio (SVR) of 20:1 [
30]. The E-SUQ contains 10 items; therefore, a minimum sample size of 200 patients was required. After taking into consideration a 10% non-responder and non-eligibility rate, the study aimed to approach 220 patients.
2.5.2. Sampling Method, Patient Recruitment and Data Collection
The EMPOWER-SUSTAIN Global CV Risks Self-Management Booklet© was distributed to patients with MetS at the university primary care clinic from October 2019 to March 2020, to ensure that the patients had the booklet for at least 6 months prior to the usability data collection.
Patients were recruited over four months from December 2020 to March 2021 when they attended the clinic for their follow-up appointment. The data collection was conducted by a trained research assistant to maintain a consistent method of collecting the data. Patients who were identified to have the booklet were approached in the nurse assessment room on the day of their follow-up appointment. They were briefed about the study and were invited to participate. A patient information sheet was given to participants to provide further details regarding the study, and their right for confidentiality was explained. Those who agreed to participate were screened for eligibility according to the inclusion and exclusion criteria. The patient’s eligibility was screened by reviewing the electronic medical record. A written informed consent was obtained from participants who agreed and were eligible to participate in the study.
The usability data were collected using E-SUQ, which was distributed to participants to be self-administered. Clear verbal instructions were provided on how to complete the questionnaire without assistance. The participants were advised to seek clarification from the researcher for any questions. Participants took approximately 15 minutes to complete the questionnaire. Following completion, participants were asked to return the questionnaire to the researcher to be checked for completeness.
2.5.3. Data Collection for Test-Retest
Thirty participants were recruited for the test-retest of E-SUQ. A date was given for them to come back to the clinic within 2–4 weeks to answer the same questionnaire. Participants were called one day before to remind them about the appointment.
2.6. Statistical Analysis
Data entry and statistical analysis were performed using the latest IBM SPSS Statistics Program Version 25. During the data entry, the responses for negative statements (item 2, 4, 6, 8 and 10) were reversed. Data quality was examined using the percentage of missing data and mean score of E-SUQ with standard deviation (±SD) was calculated using the formula recommended by the SUS author [
22]. Descriptive analysis was presented as frequency and percentage for categorical data. Normally distributed continuous data were expressed as mean with ±SD and non-normally distributed data were expressed as median with interquartile range (IQR).
Psychometric elements of E-SUQ were examined in three parts. Firstly, the factorability of the 10 items was examined to determine the suitability of the data to undergo factor analysis. The sampling adequacy was assessed using the Kaiser-Meyer-Olkin (KMO), whereas the appropriateness of data was conducted using Bartlett’s test of sphericity. The data are considered to be suitable for factor analysis when the KMO value is >0.50 [
31] and if the p-value of Bartlett’s test of sphericity is <0.05 [
32].
Secondly, factor extraction using principal component analysis (PCA) was conducted to identify the dimensionality of the 10 items of E-SUQ. The number of factors to retain was determined using the following tests: the rule of eigenvalue >1 according to Kaiser’s Criteria, >50% cumulative percentage of variance and the scree plot [
33]. The retained factors were then rotated using varimax rotation with the factor loading significance set at >0.4 [
34].
Thirdly, the internal consistency and test-retest reliability analyses were conducted to determine the reliability of E-SUQ. A Cronbach α coefficient and corrected item-total correlation (CITC) were used to measure internal consistency. A minimum value of Cronbach’s α coefficient of 0.7 [
35] and a minimum CITC range (r) of 0.3 were considered as reliable [
36]. The test-retest reliability was examined using the intra-class correlation coefficient (ICC) to assess the temporal stability of the item. The ICC estimates and their 95% confidence intervals were calculated based on the mean rating (k = 30), absolute agreement and two-way mixed-effect model (ICC [2,k]). The ICC values <0.5 indicate poor reproducibility, between 0.5 and 0.75 indicate moderate reproducibility, between 0.75 and 0.9 indicate good reproducibility, and values >0.90 indicate excellent reproducibility [
37].
4. Discussion
To the best of our knowledge, there is no published study on the validation of a usability questionnaire to assess a self-management booklet. Our study is the first to demonstrate that E-SUQ is a valid and reliable tool to assess the usability of the EMPOWER-SUSTAIN Global CV Risks Self-Management Booklet
©. E-SUQ also underwent a thorough adaptation and validation process based on the recommended guidelines [
20].
The data set of our study is of good quality as there were no missing values. The mean score of E-SUQ among patients with MetS was 77.3 (SD ± 13.8). Direct comparison with other studies assessing usability of the self-management booklet could not be made as there was no published literature in this area. Our findings can be compared with usability of mobile apps as there is numerous published evidence in this area. The mean score in our study is comparable to the mean score of SKAMA (72.9 (SD ± 11.5)) which was used to assess a colorectal community education mobile app in Malaysia [
38]. Other validation studies that used the original SUS had reported higher mean scores. These include studies among patients with type 2 diabetes mellitus in Utah which showed a mean score of 80.5 (SD ± 11.5) [
39] and among patients living with chronic pain in Norway which showed mean score of 85.7 (SD ± 12.9) [
40]. In contrast, a usability study of a cognitive behavioural therapy app using SUS among mental healthcare providers in six European countries yielded a lower mean score of 67.9 (SD ± 18.8) [
41]. This might be due to comprehension problems as there was no translation of SUS to the local language in these European countries.
Content validation was conducted twice in our study due to the need to improve clarity and relevance for item 5. Several studies supported multiple iterations in the process of content validation to improve the clarity and relevance of the items representing the underlying construct [
26,
42,
43]. With regards to face validity, ESUQ was found to be clear and comprehensible with I-FVI ranged between 0.9 and 1.0. Our finding is comparable to the I-FVI of SKAMA which ranged between 0.8 and 1.0 [
19].
Factor analysis in this study revealed a two-factor solution in which items 1, 3, 5, 7 and 9 loaded onto Factor 1 (“Positive Tone”) and items 2, 4, 6, 8 and 10 loaded onto Factor 2 (“Negative Tone”). This is known as the tone model, which has been described in various other studies [
41,
44,
45,
46]. However, two studies did not support the tone model as it was of limited theoretical interest in relation to usability [
44,
45]. They recommended to interpret SUS as a unidimensional measure of perceived usability [
44,
45]. A more recent study using confirmatory factor analysis (CFA) supported a two-factor model of “Usability” and “Learnability” as the best fitted model compared to the unidimensional or the tone model [
41].
The overall Cronbach’s α coefficient found in our study was 0.77, which indicates that E-SUQ is reliable to assess the usability of a self-management booklet. This finding is comparable to SKAMA, which has a Cronbach α of 0.85 [
19]. Likewise, our finding is also comparable to the reliability of the SUS in other studies which showed Cronbach’s α of 0.91 [
41] and 0.88 [
46].
In terms of test-retest reliability, our study demonstrates an overall value of 0.85, indicating good reproducibility. This finding is comparable to the Persian version of SUS, where the value of overall ICC was 0.96 [
47]. In contrast, the Portuguese version of SUS showed a weak overall ICC value of 0.36 [
48].
4.1. Strength and Limitation
The strengths of this study include having a good quality data set as there was no missing value and the mean score showed good usability at 77.3 (SD ± 13.8). Another strength of this study was the high response rate of 97.6%. Our study is the first to demonstrate that E-SUQ is a valid and reliable tool to assess the usability of a self-management booklet. To date, there is no other published questionnaire available that can be regarded as an “anchor tool” or “gold standard”. Therefore, convergent validity could not be performed. There were also limitations in this study. Firstly, the population was from a university primary care clinic with Malay ethnicity (88.3%) constituting the vast majority of participants. As a result, the outcome of this validation study may not be generalizable to other primary care clinics in Malaysia with multiracial populations such as Chinese and Indian. Secondly, patients with MetS who were given the EMPOWER-SUSTAIN Global CV Risks Self-Management Booklet© were chosen conveniently. This may introduce sampling bias. To minimize this, all patients who were identified to have the booklet on their appointment day were invited to participate in the study. Thirdly, CFA could not be conducted to confirm the dimensionality of the item as it requires a larger sample size of at least 300. This was not feasible considering the limited time frame given to complete this study. The COVID-19 pandemic also had an impact on the number of patients coming to our clinic, resulting in a longer time taken to collect the data. Lastly, the validated E-SUQ questionnaire can only be utilized by those who can read and understand the Malay language.
4.2. Implication for Further Research and Clinical Practice
This study has proven that E-SUQ is a valid and reliable questionnaire to assess the level of usability of the EMPOWER-SUSTAIN Global CV Risks Self-Management Booklet© among patients with MetS attending a university primary care clinic. Further validation study involving patients from other primary care clinics in Malaysia is recommended to improve its generalizability. ESUQ should also be translated into Mandarin and Tamil so that the level of usability can be assessed among other major ethnic groups in Malaysia such as Chinese and Indian. As there were many controversies with the factor structure of the original SUS, future studies using CFA should be performed to confirm the dimensionality of E-SUQ. Further research to determine the factors associated with usability of the booklet is also recommended to support its widespread use among patients with MetS.




{kind=link}
