
Effect of Motor Imagery Training on Motor Learning in Children and Adolescents: A Systematic Review and Meta-Analysis

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
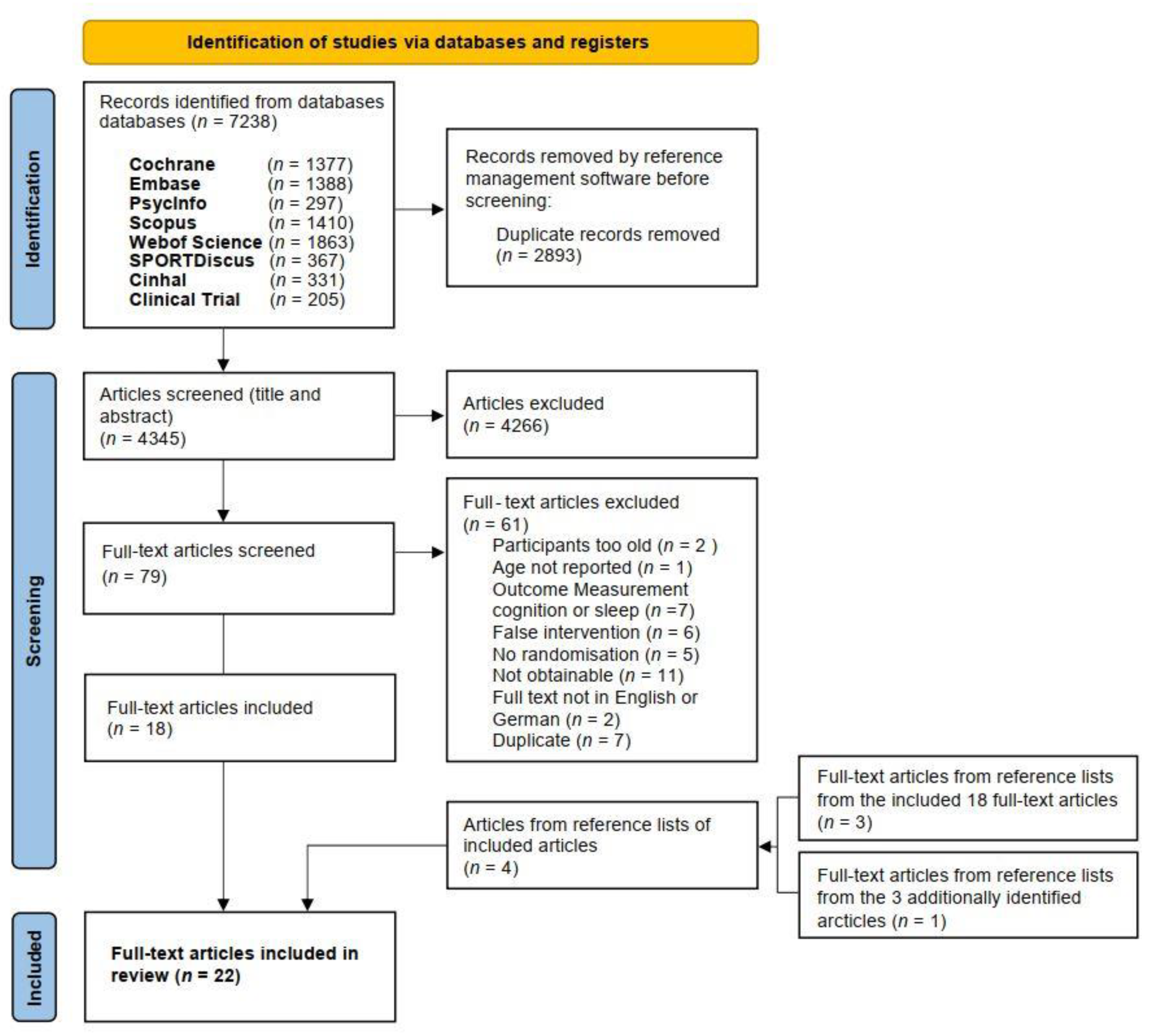
2.1. Search Strategy, Selection Criteria and Process
- Cochrane Library
- Embase
- PsycInfo
- Scopus
- Web of Science
- Cinhal
- Clinicaltrials.gov
2.2. Data Extraction
- (1)
- Trial-related information included: First author, year of publication, kind of randomization, blinding, sample size and study groups, age, and gender of participants, participants’ description, study setting, task to imagine, measurement events, outcomes and outcome measures, study results, number of dropouts, recognition of an included participant flow chart and the risk of bias evaluation.
- (2)
- MIT-related information included: MI experience, MI familiarization, MI manipulation check, PETTLEP (physical, environment, timing, task, learning, emotion, perspective) approach used, MIT intervention and control interventions descriptions, MIT session and order of MIT and physical practice, location of MIT and position of the individual during MI, MI supervision and instructions’ medium, instruction individualization yes/no, perspective (internal/external), mode (kinesthetic/visual), eyes open/closed and temporal parameters: number and frequency of MIT sessions and duration and number of MI trials (per session and total).
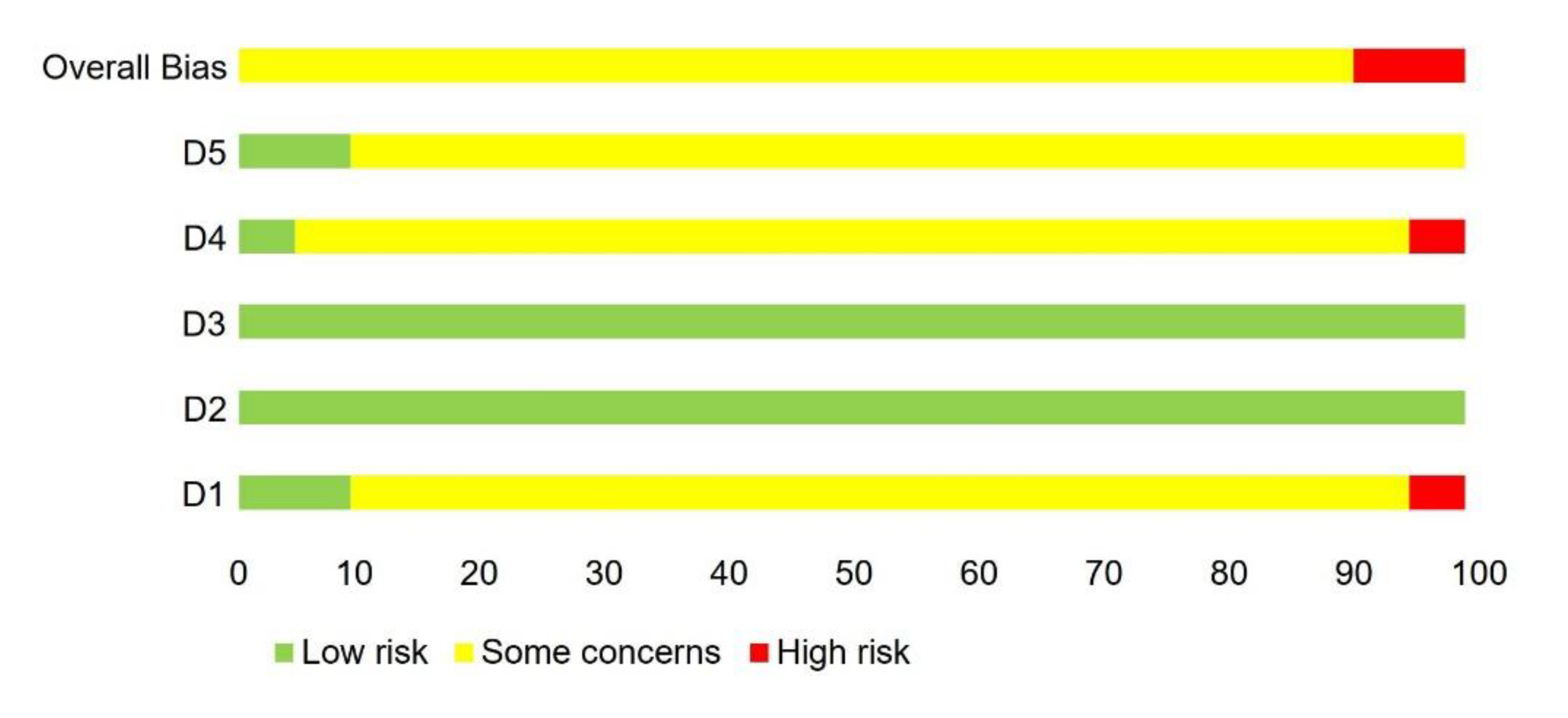
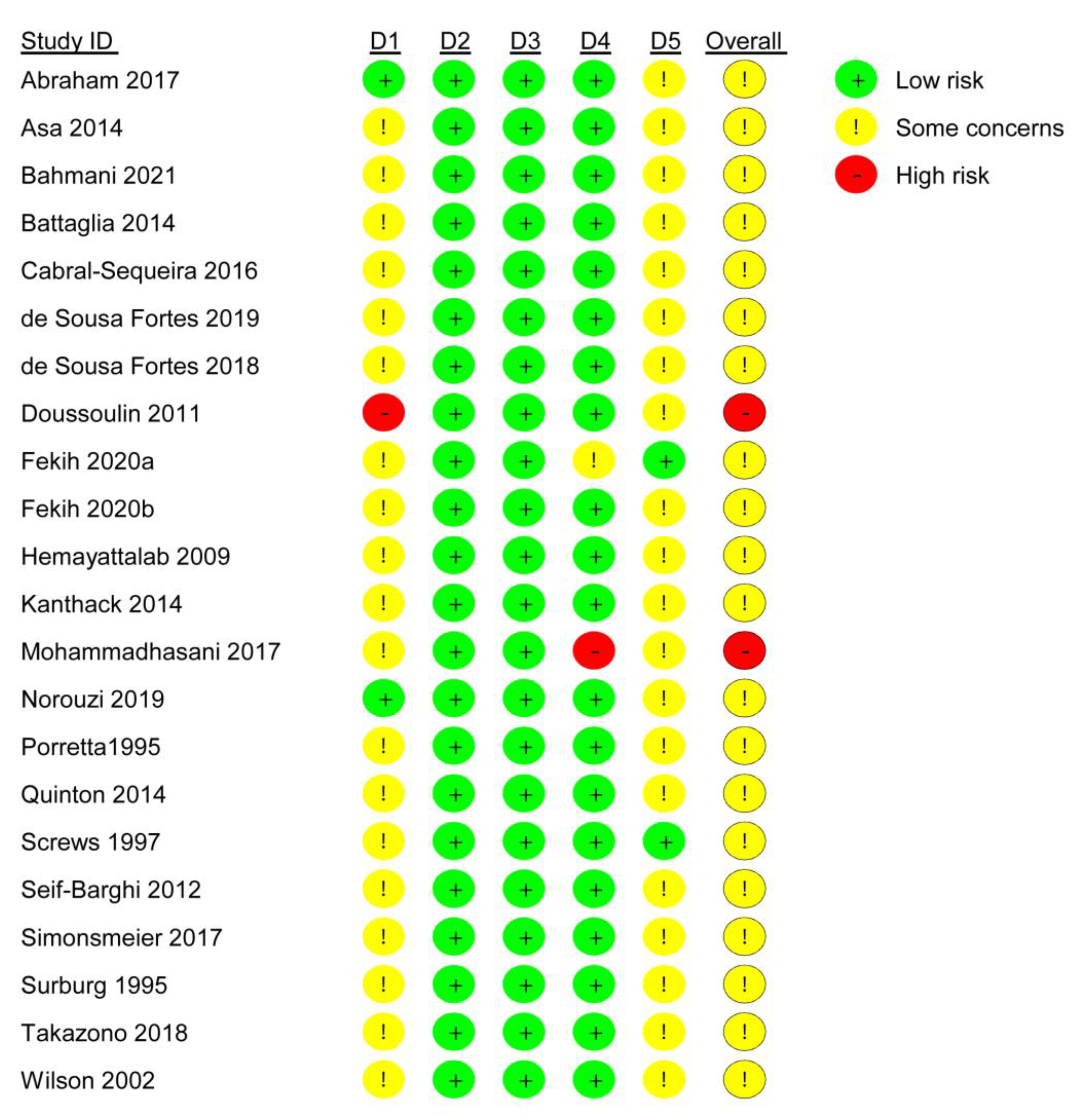
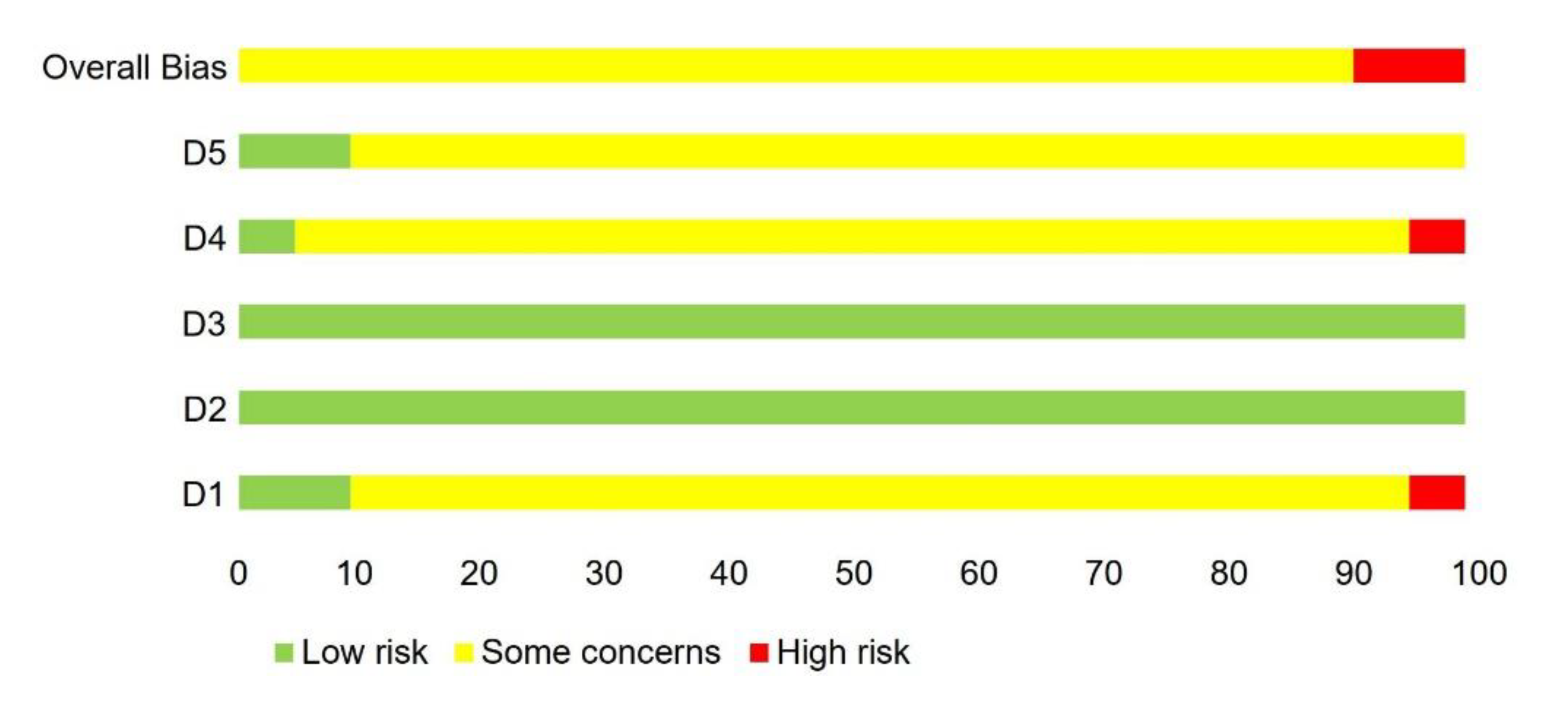
2.3. Assessment of Risk of Bias and GRADE

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author | Year | Country | Randomization and Kind of Randomization | Blinding | Study Groups | Number and Gender of Participants and per Group | Age of Participants and Per Group [Years] | Participants | Study Setting | Focus of Imagery | Measurement Events | Outcomes and Outcome Measures | Results EG vs. CG | Dropouts/ Flow Chart/ RoB Rating |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Abraham [73] | 2017 | IL | RCT, R. stratified for age and dancing level | Investigator and participants during pre-assessment | 2 | Total: 25 Females EG: 13 F CG: 12 | EG: 13.51 (± 0.49) CG: 13.63 (± 0.52) | Healthy dance students, at least 3 years of dancing experience | Dance studio | Elevé movement | Pretest Posttest | Ankle PF ROM in degrees Symmetry index in %: Kinematic data collected in 3-D using two digital video cameras Kinetic data were collected using the TETRAX© system MI ability: MIQ-R | No sign. between-group difference | Dropouts: 1 Flow chart: No RoB rating: SC |
| Asa [74] | 2014 | BRA | RCT, R. stratified for gender | N.R. | 3 | Total: 36 (F = 13, M = 23) MIT: 12 (F = 4, M = 8) PP: 12 (F = 5, M = 7) NP: 12 (F = 4, M = 8) | MIT: 9.9 ± 0.2; PP: 10 ± 0.5; NP: 9.9 ± 0.4 | Healthy, right-handed pupils from a private school, average education [years]: MIT and NP: 4.4 ± 0.3 PP: 4.5 ± 0.4 | N.R. | FOS: TS 4-3-2-1 | BL T1: Day 1 T2: Day 4 T3: Day 7 T4: Day 28 | Speed and accuracy of TS and URS: Number of correct sequences per min. recorded by a computer-monitored device attached to fingertips | MIT and PP equally effective in immediate and long-term learning, MIT leads to more efficient transfer to URS | Dropouts: N.R. Flow chart: No RoB rating: SC |
| Bahmani [75] | 2021 | IR | RCT, R. N.R. | N.R. | 2 | Total: 136 Males EMIT: 67 M IMIT: 71 F | Total: 10.13 ± 0.65 | Healthy boys, who were naïve to the purpose of the study | N.R. | Overarm tennis ball toss with non-dominant hand | Pretest: day 1 Posttest: day 2 | Tossing accuracy: Ratio of individual’s scoring for total score divided by number of completed trials MI ability: Persian MIQ-C | External imagery focus produced superior motor learning | Dropouts: No Flow chart: No RoB rating: SC |
| Battaglia [76] | 2014 | Italy | RCT, R. N.R. | Assessor | 2 | Total: 72 Females EG: 36 F CG: 36 F | EG: 13.8 ± 1.3 CG: 14.2 ± 1.7 | Female rhythmic gymnasts, competing at national level | Summer training camp | Vertical jumps | Pretest Posttest | Vertical jump performance (FT, CT, HT, DJ, Counter Movement Jump): Optojump system MI ability—MIQ-R | FT and CT jumping parameters of the HT and DJ tests improved significantly in MIT compared to PP only. | Dropouts: N.R. Flow chart: No RoB rating: SC |
| Cabral-Sequeira [77] | 2016 | BRA | RCT R. N.R. | N.R. | 4 | Total: 31 (F = 15, M = 16) EG: not reported CG: not reported | Total: 13.58 ± 1.74 EG: not reported, CG: not reported | Adolescents with mild cerebral palsy | N.R. | Aiming as fast and accurately as possible at a 2 cm diameter target | Day 1: Posttest 1 Day 2: Retention test, Posttest 2, Retention 2 | Movement time, Movement straightness, Frequency of sub-movement, Peak height, Average joint angular velocity, Radial error: Four opto-electronic cameras (Vicon, MX3+) | No effect associated with side of hemiparesis to achieve equivalent motor performance MIT induced faster and straighter movements in comparison with controls | Dropouts: 2 Flow chart: No RoB rating: SC |
| de Sousa Fortes [78] | 2019 | BRA | RCT, R. stratified for passing decision-making performance at BL | N.R. | 2 | Total: 33 Males EG: 17 CG: 16 | Total: 16 ± 0.6 EG: 15.6 ± 1.9 CG: 15.6 ± 1.8 | Volleyball players with at least 2 years of experience, training for 89.7 ± 4.5 min/day, 5×/week, enrolled in the U-17 Volleyball State Championship | Training site | Passing decision-making performance in volleyball | T1: 48 h before Intervention T2: 48 h after intervention | Decision-making performance—Game Performance Assessment Instrument and Decision-making index Heart rate—heart rate monitor Video recording of EG and CG sessions | Moderate positive effect of MIT on passing decision-making performance of the young volleyball players | Dropouts: N.R. Flow chart: No RoB rating: SC |
| de Sousa Fortes [79] | 2020 | BRA | RCT, R. stratified by website | Statistician | 2 | Total: 28 Males MIT: 14 CG: 14 | MIT: 15.37 ± 0.22 CG: 15.45 ± 0.33 | Tennis players (training 2 h/day, 4×/wk) enrolled in the State Tennis Championship | Tennis court | Tennis service performance | T1: 48 h before intervention T2: 48 h after intervention | Accuracy—total sum of achieved points Speed (km/h)—radar gun MI ability—MIQ- 3 | MIT might be an elective strategy to enhance tennis service performance among young male tennis players | Dropouts: No Flow chart: Yes RoB rating: SC |
| Doussoulin [80] | 2011 | CL | RCT R. N.R. | Assessor | 3 | Total: 64 (N.R.) EG: 22 CG1: 21 CG2: 21 | Total: 9–10 | Elementary school students, fourth grade classes, absence of motor and/or sensory disturbances | Urban elementary school from Temuco (Chile) | Run and throw a ball towards a distant target | BL: pretest during first session T1: posttest after sixth training session | Learning—Score of Standardized Basic and Combined Movements Scale Distance reached on each ball throwing—outcome measure not mentioned | All training forms were effective in improving motor task performance, MIT and modelling were more effective to obtain a significantly higher final performance than PP | Dropouts: N.R. Flow chart: No RoB rating: High |
| Fekih_a [81] | 2020 | TUN | RCT R. N.R. | N.R. | 2 | Total: 38 Males MIT: 18 CG: 20 | MIT: 16.9 ± 0.6 CG: 16.7 ± 0.8 | Young male tennis players, volunteered, training regularly in tennis clubs for 2 h/day, on average 3×/wk | Usual training session | Tennis service | T0: 48 h before Ramadan T1: end of first week of Ramadan T2: end of second week of Ramadan T3: end of fourth week of Ramadan | Tennis service performance as a product of accuracy and speed, measured with total scores of the Service Performance Test and radar gun MI ability with MIQ-RS | MIT could be effective strategy to optimize tennis service performance during Ramadan fasting, MIT could counteract/mitigate negative and detrimental effects of fasting on tennis service performance | Dropouts: N.R. Flow chart: No RoB rating: SC |
| Fekih_b [82] | 2020 | TUN | RCT R. N.R. | N.R. | 2 | Total: 27 Males | EG: 16.9 ± 0.64 CG: 16.7 ± 0.59 | Tennis players for at least 2 years who train in clubs for 2 h/day, 3×/wk | Tennis club sessions | Agility, speed, reaction time | T0: 48 h before Ramadan T1: end of first week of Ramadan T2: end of second week of Ramadan T3: end of fourth week of Ramadan | Agility—MAT- Agility Test Speed—ZIG-ZAG test Reaction time—video recordings MI ability—MIQ-RS for MITG only | Fasting during Ramadan reduced all performance outcomes. MIT after regular workouts may be an effective strategy to reduce the effect of fasting during Ramadan and stabilize physical performance outcomes in terms of agility, speed and reaction time for male tennis players. | Dropouts: N.R. Flow chart: No RoB rating: SC |
| Hemayattalab [83] | 2010 | IR | RCT, R. N.R. | N.R. | 5 | Total: 40 (N.R.) PP: 8 MIT: 8 PP + MIT: 8 MIT + PP: 8 CG: 8 | Total: 12–15 | Adolescents with mental retardation (AWMR) | School for mentally retarded pupils of Tehran | Basketball free throws | T1: pretest T2: posttest T3: retention test 10 days later | Basketball free throw performance: Free throw test (10 attempts) MI ability: EMG | In adolescents with mental retardation MIT by itself is less effective than PP for motor task learning enhancement, MIT + PP is more effective than MP alone | Dropouts: N.R. Flow chart: No RoB rating: SC |
| Kanthack [84] | 2014 | BRA | RCT, R. N.R: | N.R. | 2 | Total: 22 (N.R) EG: 11 CG:11 | EG: 17.6 ± 0.5 CG: 17.6 ± 0.5 | Young basketball players from one team in the junior league of the Federação Paulista de Basquete | Room near basket-ball court, and basketball court | Basket-ball free throws | T1: pretest T2: posttest | Basketball throwing performance: Scoring in 10 free throws Self-efficacy: General Perceived Self-Efficacy Scale Imagination level: customized scale ranging (0–3) | There was no significant difference between groups’ median SWC statistic indicated an 84% likelihood that MIT had a beneficial effect on performance in the first two free throws | Dropouts: N.R. Flow chart: No RoB rating: SC |
| Mohammadhasani [85] | 2017 | IR | RCT, R. N.R. | N.R. | 3 | Total: 36 Females MIT-CI: 11 PP-CI: 12 PP: 13 | Total: 12 years old | Sixth-grade elementary school pupils | A school of Shiraz city | Kata skill (the first kata: Taikyoku Sono Ichi) | T1: pretest T2: posttest = last training session T3: 48 h after last training session T4: in a competitive condition | Kata skill learning and performance: Kata evaluation form scores 0–20 | The systematic increase in the CI had highest effectiveness, MIT + PP with a systematic increase in CI had long-term positive effects on performance and learning a kata skill | Dropouts: N.R. Flow chart: No RoB rating: High |
| Norouzi [86] | 2019 | IR | RCT, R. computer-genera-ted random-number sequence | N.R. | 3 | Total: 45 Males MIT1: 15 MIT2: 15 CG:15 | Total: 14.65 ± 1.34 | Adolescent novice players in a summer camp | Football summer camp from Farhang Football School in Jahrom | Football pass skill performance | Pretest Posttest | Football pass skill performance: Mor and Christian’s test MI ability: MIQ | Among adolescent novice football players, external PETTLEP imagery led to the highest improvement in football passing skill performance | Dropouts: 0 Flow chart: No RoB rating: SC |
| Porretta [87] | 1995 | USA | RCT, R. N.R. | N.R. | 2 | Total: 32 (F = 17, M = 15) PP + MIT: 16 PP: 16 | PP + MIT: 15 years 4 months ± 1 year 8 months PP: 14 years 7 months ± 1 years 6 months | Adolescents with mild mental retardation | N.R. | Striking with a baseball bat | During each training session on 5 consecutive days (Monday to Friday) | Timing accuracy [ms] measured as discrepancy between arrival of light stimulus at a certain location and striking the string: Bassin Anticipation Timer | Participants using PP + MIT were significantly more accurate on the striking task than participants in the PP group | Dropouts: N.R. Flow chart: No RoB rating: SC |
| Quinton [88] | 2014 | UK | RCT (matched by age), R.N.R. | N.R. | 2 | Total: 36 (F = 2, M = 34) EG: 18 CG: 18 | Total: 9.72 ± 2.05 EG: N.R: CG: N.R. | Futsal player | Gymnasium | Dribbling and passing soccer task | Pretest Posttest | Players’ ball control and decision-making skills: Dribbling and passing soccer task MI ability: MIQ-C | MIT produced no significant improvements in imagery ability or motor task performance, Significant correlation at post-test for the MIT group between age and external visual and kinesthetic imagery ability | Dropouts: N.R. Flow chart: No RoB rating: SC |
| Screws [89] | 1997 | USA | RCT, R. N.R. | N.R. | 6 | Total: 30 (N.R.) EG: 10 (5 peg board; 5 pursuit rotor) PP: 10 (5 + 5) CG: 10 (5 + 5) | Total: 12.5 ± N.R. | Children with MMD | Rural School in Alabama | Cognitive-oriented task (peg board) + Skill on motoric-oriented task (pursuit rotor) | Pretest Posttest | Cognitive-oriented task: Correctly placed pegs on peg board Motoric-oriented task: Time on target for the pursuit rotor task | MIT enhanced motor performance of children with MMD on both the peg board test and the pursuit rotor task | Dropouts: N.R. Flow chart: No RoB rating: SC |
| Seif-Barghi [90] | 2012 | IR | RCT R. N.R. | Coaches | 2 | Total: 88 Males; U16:17; U19:18 EG: U16 = 9, U19 = 9 CG: U16 = 8, U19 = 9 | Total: 18.99 ± 4.24 U16: EG 15.04 ± 0.94, CG 14.93 ± 0.63; U19: EG 17.72 ± 1.16, CG 17.31 ± 1.46 | Soccer players affiliated with professional soccer clubs taking part in the national championship leagues in four age categories including U16, U19, U21 and over 21 | Soccer field; educational classes in their clubs in a private room | Soccer pass performance | Pretest Posttest | Successful passing performance: Rate index after dividing by total passing counts throughout the minutes of playing presented as percentile | Players in the MIT group could observe an increase in the successful pass rate compared to CG. | Dropouts: 19 Flow chart: Yes RoB rating: SC |
| Simonsmeier [91] | 2017 | GER | RCT, R. by software before BL assessment | Judges | 2 | Total: 56 Females MIT first: Low Expertise: 22 High Expertise: 9 MIT last: Low Expertise: 12 High Expertise: 13 | Total: 9.63 ± 2.43 | Gymnasts participating in their sport between 1 and 14 years between 3.5 and 25.5 h/week | Regular training session | The cast to handstand on bars | T1: prior to first training phase T2: between two training phases T3: after second training phase | The cast to handstand on bars performance: Coding system Mental representation: SDA-M Imagery ability: SIAQ | MIT had positive effects on performance only for the high-expertise athletes in MIT last condition | Dropouts: 2 Flow chart: No RoB rating: SC |
| Surburg [92] | 1995 | USA | RCT, R. N.R. | N.R. | 4 | Total: 40 (F = 22, M = 18) | Total: 15.65 ± 6.65 | Forty students with mild mental retardation (20 students from Indiana, 20 students from Ohio) | High school pupils | An under-hand baseball throwing task | N.R. | Successful execution of an underhand throwing task with the non-dominant arm | Two types of cognitive demands did not affect imagery MIT did improve motor performance of students with mild mental retardation | Dropouts: N.R. Flow chart: No RoB rating: SC |
| Takazono [93] | 2018 | BRA | RCT, R. N.R. | N.R. | 3 | Total:18 (both gender) PP: 6 PP + MIT: 6 CG: 6 | Total: 9.33 ± 0.49 | Right handed, healthy pupils | N.R. | Holding a plastic block and insert it in the support with the right hand | Pretest: before training Posttest: immediately after PP Retention test: 24 h after training) | Task performance: Movement time in sec reach, transport: commercial digital camera Imagery ability: MIQ-C | PP group achieved a persistent performance gain in the “transport”, but not in the “reaching” task PP + MIT group achieved persistent performance gains in both movement components No significant differences were found for CG | Dropouts: N.R. Flow chart: No RoB rating: SC |
| Wilson [94] | 2002 | AUS | RCT, R. blocked to ensure similar numbers of children within 4 percentile ranges of total impairment and similar age | Assessor | 3 | Total: 54 (N.R.) EG:18 PP: 18 NP: 18 | Total: Range 7–12 | Children with motor coordination difficulties | Six schools in Brisbane | Catching and throwing a tennis ball, Striking a softball, Jumping to a target using a two-leg take-off, balancing a ball on a bat while walking, placing objects using formboard | Pretest Posttest | Motor function: Movement Assessment Battery for Children | Imagery training, delivered in a multimedia format, can be equally effective to perceptual-motor training in developing the motor skills of children referred with coordination problems. | Dropouts: N.R. Flow chart: No RoB rating: SC |
| First Author | MI Experience, MI Familiarization and MI Manipulation Check | PETTLEP Approach and MI Intervention Description | Control Interventions | MIT Session and Order | Location and Position during MIT | MIT Supervision and MI Instructions | MI Mode, MI Perspective, Eyes | Number of MITS and Intervention Duration | Trials per MITS and Total Trials |
|---|---|---|---|---|---|---|---|---|---|
| Abraham | MI experience: N.R. MI familiarization: N.R. MI check:
| PETTLEP: yes MITG: Specific components of elevé performance, emphasis on ankle PF and foot movements, biomechanics, equal WBD Progression:
| PP: Upper body exercises with focus on postural awareness, joint mobility and strengthening of neck, shoulders, arm, elbows, wrists. No pelvic, abdominal or lower limbs exercises Progression: From 6. Session use of resistance bands and light balls | Session: N.R., probably group Order: N.R. | Location: Dance studio Position: MITG: Lying down supine on mattress CG: Sitting on a chair in a circle | Supervision: Yes Instructions: Live, detailed, descriptive with changing tones of voice, and using arousing mental images | Mode: Visual then kinesthetic Perspective: N.R. Eyes: Closed or open, according to personal preference | Total: 12 MITS = 2 MITS lasting 20–25 min each per week Duration: 6 weeks | Progressions: (1) Number of mental elevé 30–80, (2) tempo of performance: 20–40 movements per min. and for static elevé 8–14 s, (3) complexity of imagery environment |
| Asa | MI experience: N.R. MI familiarization: N.R. MI check: N.R. | PETTLEP: N.R. MITG: Kinesthetic imagery of the FOS trained sequence 4-3-2-1 | PP: Physical practice of FOS TS using the trained hand NP: No practice on any of the movement sequences, practiced a non-sequential painting task for the same length of time as PP and MIT | Session: N.R. probably individual Order: MIT only | Location: N.R. Position: Comfortably seated in front of a desk with supported elbows and forearms | Supervision: Yes Instructions: Live | Mode: Emphasized kinesthetic imagery and prevented use of visual imagery Perspective: N.R. Eyes: Closed | Total: 1 MITS lasting app. 25 min Duration: 1 day | MITS: Four blocks of 120 mental trials with rest intervals of 2 min between blocks Total trials: 120 |
| Bahmani | MI experience: No experience MI familiarization: N.R. MI check: Open-ended questions | PETTLEP: N.R. Two different MIT groups: MIT internal focus: Participants were asked ‘to focus on the tossing arm’ MIT external focus: Participants were instructed ‘to focus on the ball’ | Session: N.R. Order: PP before MIT | Location: N.R. Position: Standing, 6.1 m away from target | Supervision: N.R. Instructions: N.R. | Mode: N.R. Perspective: Internal and external Eyes: N.R. | Total: 1 MITS Duration: 1 day | MITS: Six blocks à 10 mental tosses Total trials: 60 | |
| Battaglia | MI experience: N.R. MI familiarization: N.R. MI check: 10 open-ended questions | PETTLEP: Yes MITG:
| CG: Light core training (abdominal muscle exercises) and active flexibility training + 3 min: 5 PP of each vertical jump | Session: N.R. Order: MIT before PP | Location: N.R., probably gym Position: N.R. | Supervision: N.R. Instructions: N.R. | Mode: Visual Perspective: N.R. Eyes: N.R. | Total: 12 Two MITS per day for 6 days/week Duration: 6 weeks | MITS: Five mental trials of each of the 3 vertical jumps = 15 MI trials Total trials: 180 |
| Cabral-Sequeira | MI experience: N.R. MI familiarization: N.R. MI check: Participants signaled initiation and end of trials by tapping their index finger of the resting (less affected) arm on supporting table | PETTLEP: N.R. MITG: Day 1: MIT of aiming task Day 2: PP of aiming task | CG: Day 1: Manipulation of a keyboard of a personal computer with less affected hand to play a game called ‘Tetris’ Day 2: PP of aiming task | Session: N.R. Order: PP before MIT | Location: Laboratory Position: Seating position on a height adjustable chair, hands relaxed and supported on table | Supervision: Yes Instructions: Live | Mode: N.R. Perspective: Internal Eyes: Closed | Total: 1 MITS lasting app. 34 min Duration: 2 days | MITS: Two sets of 5 × 10 mental trials with app. 10 min between sets Total trials: 100 |
| de Sousa Fortes | MI experience: Yes MI familiarization: N.R. MI check: N.R. | PETTLEP: N.R. MITG:
| CG: Watched videos of advertisements related to sports equipment (e.g., caps, t-shirts, and shorts). No communication allowed during sessions | Session: N.R. probably group Order: PP before MIT | Location: Quiet environment in gym, close to court, Participants wore competition outfits Position: N.R. | Supervision: N.R. Instructions: N.R. | Mode: N.R. Perspective: Internal Eyes: N.R. | Total: 24 Three MITS/wk lasting app. 10 min Duration: 8 weeks | MITS: N.R. Total trials: N.R. |
| de Sousa Fortes | MI experience: Yes MI familiarization: N.R. MI check: Participants were asked to provide information about the technique adopted and the magnitude of the perceived emotions Timer to control for MI trials | PETTLEP: N.R. MITG:
| CG: Watching videos about the history of the Olympics | Session: N.R. probably individual Order: PP before MIT | Location: Quiet environment close to the tennis court, participants wore competition outfits Position: N.R. | Supervision: Yes Instructions: N.R: | Mode: N.R. Perspective: Internal Eyes: N.R: | Total: 24 Three MITS/wk lasting app. 10 min Duration: 8 weeks | MITS: N.R. Total trials: N.R. |
| Doussoulin | MI experience: N.R. MI familiarization: N.R. MI check: N.R. | PETTLEP: N.R. MITG: MIT of the ball throwing while running task | CG1: Modeling condition: Watching a video recording of ball throwing performance while running being performed by an expert CG2: PP of ball throwing performance while running | Session: N.R. Order: PP before MIT | Location: N.R. Position: N.R. | Supervision: N.R. Instructions: N.R. | Mode: N.R. Perspective: N.R. Eyes: N.R. | Total: 6 MITS Duration: N.R. | MITS: Sixty mental trials Total trials: 60 |
| Fekih_a | MI experience: Yes MI familiarization: N.R. MI check: Chronometer for each athlete to control the duration of mental trials of the 10 tennis service | PETTLEP: N.R., probably partially MITG:
| CG: PP + watching videos about the history of the Olympic Games | Session: Individual Order: PP before MIT | Location: Quiet environment near the tennis court, participants wore competition outfits Position: N.R. | Supervision: Yes Instructions: N.R. | Mode: N.R. Perspective: Not clear: ‘first person situation’ Eyes: N.R. | Total: 12 Three MITS/wk lasting 10 min = app. 120 min Duration: 4 weeks | MITS: 10 mental trials Total trials: 120 |
| Fekih_b | MI experience: N.R. MI familiarization: N.R. MI check: Chronometer for each athlete to control the duration of mental trials of the 10 tennis service | PETTLEP: N.R. MITG:
| CG: PP + watching videos about the history of the Olympic Games | Session: N.R. Order: PP before MIT | Location: Quiet environment near the tennis court, Participants wore competition outfits Position: N.R. | Supervision: Yes Instructions: N.R. | Mode: Visual before kinesthetic Perspective: External before internal Eyes: N.R. | Total: 12 Three MITS/wk lasting 15 min= app. 180 min Duration: 4 weeks | MITS: Ten mental trials Total trials: 120 |
| Hemayattalab | MI experience: N.R. MI familiarization: Yes, 1 MI training session including internal kinesthetic imagery MI check: After pretest and before intervention a MIT training session including internal kinesthetic imagery and N.R. | PETTLEP: N.R. Three different MIT groups MITG:
PP followed by MIT: 12 TS PP of basketball free throw + 12 TS MIT basketball free throw MIT followed by PP: 12 TS MIT of basketball free throw + 12 TS PP basketball free throw | Two different control groups: PP: 30× physical practice of basketball free throw for 24 MITS CG: no training at all | Session: N.R. Order: Only MIT or PP in 1 TS | Location: N.R. Position: N.R. | Supervision: N.R. Instructions: N.R. | Mode: Kinesthetic Perspective: Internal Eyes: N.R. | Total: 24 30 min per MITS Duration: N.R. | MITS: 30 Total trials: MIT only: 720 PP followed by MIT: 360 MIT followed by PP: 360 |
| Kanthack | MI experience: No pervious MIT experience MI familiarization: N.R. MI check: Three open-ended questions | PETTLEP: N.R. MITG:
| CG: Participants were taken to another room for 4 min | Session: N.R. Order: MIT before PP | Location: Room off the basketball court, less than 20 m from the basket Position: Sitting | Supervision: Yes Instructions: N.R. | Mode: N.R. Perspective: N.R. Eyes: Closed | Total: 1 Duration: 3 min | MITS: N.R. Total trials: N.R. |
| Mohammadhasani | MI experience: N.R. MI familiarization: N.R. MI check: N.R. | PETTLEP: N.R. MITG:
| PP1: Participants physically practiced the kata skill with systematically increasing contextual interference for five sessions and five attempts each session in groups PP2: Participants practiced the kata skill for five sessions and five attempts each session in groups | Session: N.R. probably group Order: MIT before PP | Location: N.R. Position: Sitting on ground | Supervision: Yes Instructions: Live, acoustic Instructor loudly narrated the movement pattern of the kata skill step by step | Mode: N.R. Perspective: N.R. Eyes: Closed | Total: 5 Duration: N.R. | MITS: 5 Total trials: 25 |
| Norouzi | MI experience: N.R. MI familiarization: N.R. MI check: N.R. and 2 open-ended questions | PETTLEP: Yes If participants wished to modify their imagery activity, such modifications were incorporated in subsequent imagery sessions (learning). Two different MIT groups MIT1: Internal PETTLEP + PP MIT2: External PETTLEP + PP | PP: Participants practiced physically only | Session: Group Order: MIT before PP | Location: Football field Position: N.R. | Supervision: Yes, once a week Instructions: Verbal, audio | Mode: N.R. Perspective: N.R. Eyes: N.R. | Total: 12 3 MITS/wk lasting 10 × 2 min = 20 min Duration: 4 weeks | MITS: N.R. Total trials: N.R. |
| Porretta | MI experience: N. R. MI familiarization: Explanation until participants understood MIT and MIT for 4 trials MI check: Participants were asked how they actually imaged the task after familiarization and after each practice day | PETTLEP: N.R. MITG:
| PP: Participants were swinging the bat and hitting the string + were solving mathematical problems in between | Session: Individual Order: MIT before PP | Location: N.R. Position: N.R. | Supervision: N.R. Instructions: Live, acoustic | Mode: Visual and kinesthetic Perspective: N.R. Eyes: Closed | Total: 5 Duration: 5 days | MITS: 25 × 4 mental trials Total trials: 100 |
| Quinton | MI experience: N.R. MI familiarization: Participants were given a stimulus–response training in the first session to help them be more aware of what they were seeing and feeling during their imagination MI check: N.R. | PETTLEP: Yes, partially Participants were dressed in soccer kit, foot placed on the ball, usual environment (same gymnasium), changing session content MITG:
| CG: PP + participants received sport-specific nutritional advice | Session: N.R. Order: PP before MIT | Location: Gymnasium Position: Standing, foot placed on ball, dressed in soccer kit | Supervision: N.R. Instructions: Live, acoustic | Mode: according to personal preferences Perspective: according to personal preferences Eyes: according to personal preferences | Total: 10 Two MITS/wk Duration: 5 weeks | MITS: N.R. Total trials: N.R. |
| Screws | MI experience: N.R. MI familiarization: Imagery training orientation: Investigator discussed meaning of MIT and explained how to use MIT for motor task enhancement Participants were given MIT activities to acquaint them with MIT procedures. MI check: N.R. | PETTLEP: N.R. MITG:
| Two control groups: CG1: Participants physically practiced 20 trials on peg board or pursuit rotor game + made different geometric shapes CG2: no PP or MIT at any time, spent same amount of time with researcher | Session: N. R. Order: N. R. | Location: N. R. Position: N. R. | Supervision: N.R. Instructions: N. R. | Mode: N.R. Perspective: N.R. Eyes: N.R. | Total: 8 Five days/wk until prescribed number of sessions were completed Duration: 8 MITS, total 164 min | MITS: 20 Total trials: 160 |
| Seif-Barghi | MI experience: Little experience MI familiarization: Introduction session for defining and explanation of sport imagery, its application in soccer. Participants completed exercises to develop external and internal imagery, real time speeds of images and create images applying all senses. MI check: Feedback sessions at the end of each MITS Weekly interviews instantly before MIT Randomly asked questions about training course | PETTLEP: N.R. MITG:
| CG: N.R. = neutral task group’ + normal training and match activities | Session: N.R probably group Order: N.R. | Location: Quiet room in their football clubs Position: N.R. | Supervision: Yes Instructions: N.R. | Mode: N.R. Perspective: N.R. Eyes: Participants were recommended to start MIT with eyes closed. With increasing experience they could continue with eyes either open or closed | Total: 8 One MITS/wk lasting 10–15 min = 150 min MIT should be used on daily basis Duration: 8 weeks | MITS: N.R. Total trials: N.R. |
| Simonsmeier | MI experience: Assessed at BL MI familiarization: Athletes participated in a 20 min workshop, to facilitate understanding of MIT importance for motor learning Brief introduction to imagery script MI check: Four-item questionnaire post intervention, MIT diary for participants and trainers | PETTLEP: Yes MITG:
| CG: normal PP training | Session: N.R. probably individual Order: N.R. | Location: Regular training gym wearing regular clothes Position: N.R. | Supervision: N.R., probably unsupervised Instructions: Pre-recorded audio script | Mode: Visual and kinesthetic Perspective: Internal Eyes: N.R. | Total: 16 Four MITS/wk lasting 5 min = 80 min Duration: 4 weeks | MITS: Three mental trials Total trials: 48 |
| Surburg | MI experience: N. R. MI familiarization: Preparing subjects MIT with multiple trials of closing the eyes and rehearse task MI check: Questions regarding MIT content post-intervention | PETTLEP: N.R. MITG:
| Two different PP groups were participants practiced an underhand throw with the non-preferred hand: PP1: Low cognitive condition: experimenter stood next to the right side of the target PP2: High cognitive condition: experimenter served as base runner and participant had to toss the ball to the next base | Session: N.R. Order: MIT before PP | Location: N.R. Position: N.R. | Supervision: N. R. Instructions: N.R. | Mode: N. R. Perspective: N.R. Eyes: Closed | Total: N.R. Duration: 1 week | MITS: N.R. Total trials: N.R. |
| Takazono | MI experience: N.R. MI familiarization: N.R. MI check: N.R. | PETTLEP: N.R. MITG:
| Two different control groups PP: 240 physical trials of the experimental task CG: 180 mental trials of another visual rotation + 60 physical trials of the experimental task | Session: N.R., probably individual Order: MIT before PP | Location: N.R. Position: Seated in a chair in front of a table, starting with the palm of the right hand downwards resting on the starting point | Supervision: N. R., probably yes Instructions: Live, acoustic | Mode: N.R., ‘Imagine this movement, thinking of all the sensations it provides’ Perspective: N.R. Eyes: Closed | Total: 1 Duration: 1 day | MITS: 240 Total trials: 240 |
| Wilson | MI experience: N.R. MI familiarization: N.R. MI check: N.R. | PETTLEP: N.R. MITG: Software-based MIT Dynamic stimulus materials were presented in increasing complexity:
| Two different control groups PP: Traditional perceptual-motor training of the experimental task NP: wait-list control | Session: Individual Order: MIT before PP | Location: N.R. Position: N.R., probably sitting in front of a computer screen | Supervision: Yes Instructions: live | Mode: N.R., probably kinesthetic Perspective: External before internal Eyes: N.R. | Total: 5 1 MITS/wk Duration: 5 weeks | MITS: 50 Total trials: N.R., probably 250 |
2.4. Data Analysis
Primary Outcomes
3. Results
3.1. Characteristics of the Included Studies
3.2. Characteristics of Included Motor Imagery Training Interventions
- MIT as individual one-to-one session or group session was reported in four studies only (2 × group session, 2 × one-to-one session),
- A combination of MIT with PP was reported in 16 studies with an equal distribution whether MIT was performed before or after PP,
- Nine studies reported the location of the MIT and eight studies reported the position of the participant during MIT,
- Supervision during MIT session was reported and provided in eleven studies,
- Used instructions to guide the participants in their MIT was stated in ten studies using mainly live and acoustic instructions,
- The MI mode was described in seven studies reporting both visual and kinesthetic modes, which is similar to MI perspective. MI perspectives (internal, external) were described in nine studies. Both MIT session elements, mode and perspective, were used separately or in combination,
- Authors reported in ten studies whether participants had open or closed eyes during MIT,
- Surprisingly, participants were evaluated regarding their MI ability in twelve studies only. Authors used different standardized (MIQ, MIQ-R, MIQ-RS, MIQ-C) or customized MI ability questionnaires or EMG recordings,
- Temporal parameters regarding MIT sessions can be summarized as follows: Number of total MIT sessions varied between one and 24 with an intervention duration between one day and eight weeks. One MIT session took about three to 34 min, while between three and 80 MI trials were performed, summing up to 720 MI trials over one MIT intervention period.
3.3. Risk of Bias
3.4. Primary Outcomes-Effect of Motor Imagery Training Interventions
3.5. GRADE Evidence Profile Table
3.6. Further Analyses
4. Discussion
4.1. Motor Imagery Training Interventions
4.2. Methodology of the Included Studies
4.3. Strengths and Limitations
4.4. Implications for Further Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schott, N.; Haibach-Beach, P.; Knöpfle, I.; Neuberger, V. The effects of visual impairment on motor imagery in children and adolescents. Res. Dev. Disabil. 2021, 109, 103835. [Google Scholar] [CrossRef]
- Guillot, A.; Di Rienzo, F.; MacIntyre, T.; Moran, A.P.; Collet, C. Imagining is Not Doing but Involves Specific Motor Commands: A Review of Experimental Data Related to Motor Inhibition. Front. Hum. Neurosci. 2012, 6, 247. [Google Scholar] [CrossRef] [Green Version]
- Munzert, J.; Lorey, B.; Zentgraf, K. Cognitive motor processes: The role of motor imagery in the study of motor representations. Brain Res. Rev. 2009, 60, 306–326. [Google Scholar] [CrossRef] [PubMed]
- Conson, M.; Mazzarella, E.; Trojano, L. Developmental changes of the biomechanical effect in motor imagery. Exp. Brain Res. 2013, 226, 441–449. [Google Scholar] [CrossRef]
- Jackson, P.; Lafleur, M.F.; Malouin, F.; Richards, C.L.; Doyon, J. Potential role of mental practice using motor imagery in neurologic rehabilitation. Arch. Phys. Med. Rehabil. 2001, 82, 1133–1141. [Google Scholar] [CrossRef]
- Jeannerod, M. Motor representations and reality. Behav. Brain Sci. 1994, 17, 229–245. [Google Scholar] [CrossRef]
- Sharma, N.; Pomeroy, V.; Baron, J.-C. Motor Imagery: A backdoor to the motor system after stroke? Stroke 2006, 37, 1941–1952. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kilteni, K.; Andersson, B.J.; Houborg, C.; Ehrsson, H.H. Motor imagery involves predicting the sensory consequences of the imagined movement. Nat. Commun. 2018, 9, 1617. [Google Scholar] [CrossRef] [Green Version]
- Ridderinkhof, K.R.; Brass, M. How Kinesthetic Motor Imagery works: A predictive-processing theory of visualization in sports and motor expertise. J. Physiol. 2015, 109, 53–63. [Google Scholar] [CrossRef] [PubMed]
- Decety, J.; Perani, D.; Jeannerod, M.; Bettinardi, V.; Tadary, B.; Woods, R.; Mazziotta, J.C.; Fazio, F. Mapping motor representations with positron emission tomography. Nat. Cell Biol. 1994, 371, 600–602. [Google Scholar] [CrossRef]
- Decety, J. The neurophysiological basis of motor imagery. Behav. Brain Res. 1996, 77, 45–52. [Google Scholar] [CrossRef]
- Roth, M.; Decety, J.; Raybaudi, M.; Massarelli, R.; Delon-Martin, C.; Segebarth, C.; Morand, S.; Gemignani, A.; Décorps, M.; Jeannerod, M. Possible involvement of primary motor cortex in mentally simulated movement. NeuroReport 1996, 7, 1280–1284. [Google Scholar] [CrossRef] [PubMed]
- Fleming, M.; Stinear, C.; Byblow, W. Bilateral parietal cortex function during motor imagery. Exp. Brain Res. 2009, 201, 499–508. [Google Scholar] [CrossRef] [PubMed]
- Grosprêtre, S.; Lebon, F.; Papaxanthis, C.; Martin, A. New evidence of corticospinal network modulation induced by motor imagery. J. Neurophysiol. 2016, 115, 1279–1288. [Google Scholar] [CrossRef]
- Cumming, R.R.J. Imagery Intervention in Sport. In Advances in Applied Sport Psychology: A Review; Routledge: London, UK, 2009. [Google Scholar]
- Simonsmeier, B.A.; Androniea, M.; Buecker, S.; Frank, C. The effects of imagery interventions in sports: A meta-analysis. Int. Rev. Sport Exerc. Psychol. 2020, 1–22. [Google Scholar] [CrossRef]
- Driediger, M.; Hall, C.; Callow, N. Imagery use by injured athletes: A qualitative analysis. J. Sports Sci. 2006, 24, 261–272. [Google Scholar] [CrossRef] [PubMed]
- Schuster, C.; Glässel, A.; Scheidhauer, A.; Ettlin, T.; Butler, J. Motor Imagery Experiences and Use: Asking Patients after Stroke Where, When, What, Why, and How They Use Imagery: A Qualitative Investigation. Stroke Res. Treat. 2012, 2012, 503190. [Google Scholar] [CrossRef]
- Braun, S.; Kleynen, M.; Van Heel, T.; Kruithof, N.; Wade, D.; Beurskens, A. The effects of mental practice in neurological rehabilitation; a systematic review and meta-analysis. Front. Hum. Neurosci. 2013, 7, 390. [Google Scholar] [CrossRef] [Green Version]
- Zimmermann-Schlatter, A.; Schuster, C.; Puhan, M.A.; Siekierka, E.; Steurer, J. Efficacy of motor imagery in post-stroke rehabilitation: A systematic review. J. Neuroeng. Rehabil. 2008, 5, 8. [Google Scholar] [CrossRef] [Green Version]
- Cramer, S.C.; Orr, E.L.R.; Cohen, M.J.; LaCourse, M.G. Effects of motor imagery training after chronic, complete spinal cord injury. Exp. Brain Res. 2006, 177, 233–242. [Google Scholar] [CrossRef] [Green Version]
- Lebon, F.; Guillot, A.; Collet, C. Increased Muscle Activation Following Motor Imagery During the Rehabilitation of the Anterior Cruciate Ligament. Appl. Psychophysiol. Biofeedback 2011, 37, 45–51. [Google Scholar] [CrossRef]
- Marusic, U.; Grosprêtre, S.; Paravlic, A.; Kovač, S.; Pišot, R.; Taube, W. Motor Imagery during Action Observation of Locomotor Tasks Improves Rehabilitation Outcome in Older Adults after Total Hip Arthroplasty. Neural Plast. 2018, 2018, 5651391. [Google Scholar] [CrossRef] [PubMed]
- Cupal, D.D.; Brewer, B.W. Effects of relaxation and guided imagery on knee strength, reinjury anxiety, and pain following anterior cruciate ligament reconstruction. Rehabil. Psychol. 2001, 46, 28–43. [Google Scholar] [CrossRef]
- Christakou, A.; Zervas, Y.; Lavallee, D. The adjunctive role of imagery on the functional rehabilitation of a grade II ankle sprain. Hum. Mov. Sci. 2007, 26, 141–154. [Google Scholar] [CrossRef]
- Sordoni, C.; Hall, C.; Forwell, L. The Use of Imagery by Athletes during Injury Rehabilitation. J. Sport Rehabil. 2000, 9, 329–338. [Google Scholar] [CrossRef]
- Bucher, L. The Effects of Imagery Abilities and Mental Rehearsal on Learning a Nursing Skill. J. Nurs. Educ. 1993, 32, 318–324. [Google Scholar] [CrossRef] [PubMed]
- Doheny, M.O. Effects of Mental Practice on Psychomotor Skills with Baccalaureate Nursing Students. Doctoral Dissertation, Kent State University, St. Kent, OH, USA, 1989. [Google Scholar]
- Immenroth, M.; Bürger, T.; Brenner, J.; Nagelschmidt, M.; Eberspächer, H.; Troidl, H. Mental Training in Surgical Education. Ann. Surg. 2007, 245, 385–391. [Google Scholar] [CrossRef]
- Fairweather, M.M.; Sidaway, B. Ideokinetic Imagery as a Postural Development Technique. Res. Q. Exerc. Sport 1993, 64, 385–392. [Google Scholar] [CrossRef]
- Silva, S.; Borges, L.R.; Santiago, L.; Lucena, L.; Lindquist, A.R.; Ribeiro, T. Motor imagery for gait rehabilitation after stroke. Cochrane Database Syst. Rev. 2020, 2020. [Google Scholar] [CrossRef]
- Di Rienzo, F.; Debarnot, U.; Daligault, S.; Saruco, E.; Delpuech, C.; Doyon, J.; Collet, C.; Guillot, A. Online and Offline Performance Gains Following Motor Imagery Practice: A Comprehensive Review of Behavioral and Neuroimaging Studies. Front. Hum. Neurosci. 2016, 10, 315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Féry, Y.-A. Differentiating visual and kinesthetic imagery in mental practice. Can. J. Exp. Psychol. Rev. Can. Psychol. Exp. 2003, 57, 1–10. [Google Scholar] [CrossRef]
- Guillot, A.; Collet, C.; Dittmar, A. Relationship Between Visual and Kinesthetic Imagery, Field Dependence-Independence, and Complex Motor Skills. J. Psychophysiol. 2004, 18, 190–198. [Google Scholar] [CrossRef]
- Guillot, A.; Collet, C.; Nguyen, V.A.; Malouin, F.; Richards, C.L.; Doyon, J. Brain activity during visual versus kinesthetic imagery: An fMRI study. Hum. Brain Mapp. 2009, 30, 2157–2172. [Google Scholar] [CrossRef] [PubMed]
- Callow, N.; Roberts, R.; Hardy, L.; Jiang, D.; Edwards, M.G. Performance improvements from imagery: Evidence that internal visual imagery is superior to external visual imagery for slalom performance. Front. Hum. Neurosci. 2013, 7, 697. [Google Scholar] [CrossRef] [Green Version]
- Wakefield, C.; Smith, D. Perfecting Practice: Applying the PETTLEP Model of Motor Imagery. J. Sport Psychol. Action 2012, 3, 1–11. [Google Scholar] [CrossRef]
- Cumming, J.; Williams, S. The Role of Imagery in Performance. In The Role of Imagery in Performance; Oxford University Press: New York, NY, USA, 2012. [Google Scholar]
- Goss, S.; Hall, C.; Buckolz, E.; Fishburne, G. Imagery ability and the acquisition and retention of movements. Mem. Cogn. 1986, 14, 469–477. [Google Scholar] [CrossRef] [Green Version]
- Mizuguchi, N.; Nakata, H.; Uchida, Y.; Kanosue, K. Motor imagery and sport performance. J. Phys. Fit. Sports Med. 2012, 1, 103–111. [Google Scholar] [CrossRef] [Green Version]
- Williams, J.; Thomas, P.R.; Maruff, P.; Wilson, P. The link between motor impairment level and motor imagery ability in children with developmental coordination disorder. Hum. Mov. Sci. 2008, 27, 270–285. [Google Scholar] [CrossRef]
- Spruijt, S.; van der Kamp, J.; Steenbergen, B. Current insights in the development of children’s motor imagery ability. Front. Psychol. 2015, 6, 787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butson, M.L.; Hyde, C.; Steenbergen, B.; Williams, J. Assessing motor imagery using the hand rotation task: Does performance change across childhood? Hum. Mov. Sci. 2014, 35, 50–65. [Google Scholar] [CrossRef] [PubMed]
- Spruijt, S.; van der Kamp, J.; Steenbergen, B. The ability of 6- to 8-year-old children to use motor imagery in a goal-directed pointing task. J. Exp. Child Psychol. 2015, 139, 221–233. [Google Scholar] [CrossRef]
- Molina, M.; Tijus, C.; Jouen, F. The emergence of motor imagery in children. J. Exp. Child Psychol. 2008, 99, 196–209. [Google Scholar] [CrossRef]
- Estes, D. Young Children’s Awareness of Their Mental Activity: The Case of Mental Rotation. Child Dev. 2008, 69, 1345–1360. [Google Scholar] [CrossRef]
- Cheng, Y.-L.; Mix, K.S. Spatial Training Improves Children’s Mathematics Ability. J. Cogn. Dev. 2014, 15, 2–11. [Google Scholar] [CrossRef]
- Hawes, Z.; Moss, J.; Caswell, B.; Poliszczuk, D. Effects of mental rotation training on children’s spatial and mathematics performance: A randomized controlled study. Trends Neurosci. Educ. 2015, 4, 60–68. [Google Scholar] [CrossRef]
- Funk, M.; Brugger, P.; Wilkening, F. Motor processes in children’s imagery: The case of mental rotation of hands. Dev. Sci. 2005, 8, 402–408. [Google Scholar] [CrossRef] [PubMed]
- Souto, D.O.; Cruz, T.K.F.; Fontes, P.L.B.; Batista, R.C.; Haase, V.G. Motor Imagery Development in Children: Changes in Speed and Accuracy with Increasing Age. Front. Pediatr. 2020, 8, 100. [Google Scholar] [CrossRef] [Green Version]
- Bhoyroo, R.; Hands, B.; Wilmut, K.; Hyde, C.; Wigley, A. Motor planning with and without motor imagery in children with Developmental Coordination Disorder. Acta Psychol. 2019, 199, 102902. [Google Scholar] [CrossRef]
- Adams, I.L.J.; Steenbergen, B.; Lust, J.M. Development of motor imagery ability in children with developmental coordination disorder—A goal-directed pointing task. Br. J. Psychol. 2018, 109, 187–203. [Google Scholar] [CrossRef] [Green Version]
- Adams, I.L.J.; Smits-Engelsman, B.; Lust, J.M.; Wilson, P.; Steenbergen, B. Feasibility of Motor Imagery Training for Children with Developmental Coordination Disorder—A Pilot Study. Front. Psychol. 2017, 8, 1271. [Google Scholar] [CrossRef] [Green Version]
- Errante, A.; Bozzetti, F.; Sghedoni, S.; Bressi, B.; Costi, S.; Crisi, G.; Ferrari, A.; Fogassi, L. Explicit Motor Imagery for Grasping Actions in Children with Spastic Unilateral Cerebral Palsy. Front. Neurol. 2019, 10, 837. [Google Scholar] [CrossRef] [Green Version]
- American Psychatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Publishing: Washington, DC, USA, 2013. [Google Scholar]
- Deconinck, F.J.A.; De Clercq, D.; Savelsbergh, G.J.P.; Van Coster, R.; Oostra, A.; Dewitte, G.; Lenoir, M. Visual contribution to walking in children with Developmental Coordination Disorder. Child Care Health Dev. 2006, 32, 711–722. [Google Scholar] [CrossRef] [PubMed]
- Wilson, P.H.; Ruddock, S.; Smits-Engelsman, B.; Polatajko, H.; Blank, R. Understanding performance deficits in developmental coordination disorder: A meta-analysis of recent research. Dev. Med. Child Neurol. 2012, 55, 217–228. [Google Scholar] [CrossRef] [PubMed]
- Adams, I.L.; Lust, J.M.; Wilson, P.; Steenbergen, B. Compromised motor control in children with DCD: A deficit in the internal model?—A systematic review. Neurosci. Biobehav. Rev. 2014, 47, 225–244. [Google Scholar] [CrossRef] [PubMed]
- Gabbard, C.; Bobbio, T. The Inability to Mentally Represent Action May Be Associated with Performance Deficits in Children With Developmental Coordination Disorder. Int. J. Neurosci. 2010, 121, 113–120. [Google Scholar] [CrossRef]
- Williams, J.; Thomas, P.R.; Maruff, P.; Butson, M.; Wilson, P.H. Motor, visual and egocentric transformations in children with Developmental Coordination Disorder. Child Care Health Dev. 2006, 32, 633–647. [Google Scholar] [CrossRef] [PubMed]
- Hyde, C.; Fuelscher, I.; Buckthought, K.; Enticott, P.; Gitay, M.A.; Williams, J. Motor imagery is less efficient in adults with probable developmental coordination disorder: Evidence from the hand rotation task. Res. Dev. Disabil. 2014, 35, 3062–3070. [Google Scholar] [CrossRef]
- Deconinck, F.J.A.; Spitaels, L.; Fias, W.; Lenoir, M. Is developmental coordination disorder a motor imagery deficit? J. Clin. Exp. Neuropsychol. 2009, 31, 720–730. [Google Scholar] [CrossRef]
- Reynolds, J.E.; Licari, M.K.; Elliott, C.; Lay, B.S.; Williams, J. Motor imagery ability and internal representation of movement in children with probable developmental coordination disorder. Hum. Mov. Sci. 2015, 44, 287–298. [Google Scholar] [CrossRef]
- Crajé, C.; van Elk, M.; Beeren, M.; van Schie, H.T.; Bekkering, H.; Steenbergen, B. Compromised motor planning and Motor Imagery in right Hemiparetic Cerebral Palsy. Res. Dev. Disabil. 2010, 31, 1313–1322. [Google Scholar] [CrossRef]
- Mutsaarts, M.; Steenbergen, B.; Bekkering, H. Anticipatory planning deficits and task context effects in hemiparetic cerebral palsy. Exp. Brain Res. 2006, 172, 151–162. [Google Scholar] [CrossRef]
- Barclay, R.E.; Stevenson, T.J.; Poluha, W.; Thalman, L. Mental practice for treating upper extremity deficits in individuals with hemiparesis after stroke. Cochrane Database Syst. Rev. 2011, 2011, CD005950. [Google Scholar] [CrossRef]
- Suica, Z.; Platteau-Waldmeier, P.; Koppel, S.; Schmidt-Trucksaess, A.; Ettlin, T.; Schuster-Amft, C. Motor imagery ability assessments in four disciplines: Protocol for a systematic review. BMJ Open 2018, 8, e023439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lefebvre, C.; Glanville, J.; Briscoe, S.; Littlewood, A.; Marshall, C.; Metzendorf, M.; Noel-Storr, A.; Rader, T.; Shokraneh, F.; Thomas, J.; et al. Chapter 4: Searching for and selecting studies. In Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (Updated February 2021); Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Cochrane: London, UK, 2021. [Google Scholar]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schuster, C.; Hilfiker, R.; Amft, O.; Scheidhauer, A.; Andrews, B.; Butler, J.; Kischka, U.; Ettlin, T. Best practice for motor imagery: A systematic literature review on motor imagery training elements in five different disciplines. BMC Med. 2011, 9, 75. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Ryan, R.; Hill, S. How to GRADE. Cochrane Consum. Commun. La Trobe Univ. 2018. [Google Scholar] [CrossRef]
- Abraham, A.; Dunsky, A.; Dickstein, R. The Effect of Motor Imagery Practice on Elevé Performance in Adolescent Female Dance Students: A Randomized Controlled Trial. J. Imag. Res. Sport Phys. Act. 2017, 12. [Google Scholar] [CrossRef]
- Asa, S.K.D.P.; Melo, M.C.S.; Piemonte, M.E.P. Effects of Mental and Physical Practice on a Finger Opposition Task among Children. Res. Q. Exerc. Sport 2014, 85, 308–315. [Google Scholar] [CrossRef]
- Bahmani, M.; Babak, M.; Land, W.M.; Howard, J.T.; Diekfuss, J.A.; Abdollahipour, R. Children’s motor imagery modality dominance modulates the role of attentional focus in motor skill learning. Hum. Mov. Sci. 2021, 75, 102742. [Google Scholar] [CrossRef]
- Battaglia, C.; D’Artibale, E.; Fiorilli, G.; Piazza, M.; Tsopani, D.; Giombini, A.; Calcagno, G.; di Cagno, A. Use of video observation and motor imagery on jumping performance in national rhythmic gymnastics athletes. Hum. Mov. Sci. 2014, 38, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Cabral-Sequeira, A.S.; Coelho, D.B.; Teixeira, L.A. Motor imagery training promotes motor learning in adolescents with cerebral palsy: Comparison between left and right hemiparesis. Exp. Brain Res. 2016, 234, 1515–1524. [Google Scholar] [CrossRef] [PubMed]
- Fortes, L.D.; Almeida, S.S.; Nascimento Junior, J.R.; Vieira, L.F.; Lima-Júnior, D.; Ferreira, M.E. Effect of motor imagery training on tennis service performance in young tennis athletes. Rev. Psicol. Deporte 2019, 28, 157–168. [Google Scholar]
- Fortes, L.; Freitas-Júnior, C.G.; Paes, P.P.; Vieira, L.F.; Junior, J.R.N.; de Lima-Junior, D.; Ferreira, M.E.C. Effect of an eight-week imagery training programme on passing decision-making of young volleyball players. Int. J. Sport Exerc. Psychol. 2020, 18, 120–128. [Google Scholar] [CrossRef]
- Doussoulin, A.; Rehbein, L. Motor imagery as a tool for motor skill training in children. Motricidade 2011, 7, 37–43. [Google Scholar] [CrossRef]
- Fekih, S.; Zguira, M.S.; Koubaa, A.; Ghariani, I.; Zguira, H.; Bragazzi, N.L.; Jarraya, M. The Impact of a Motor Imagery-Based Training Program on Agility, Speed, and Reaction Time in a Sample of Young Tennis Athletes during Ramadan Fasting: Insights and Implications from a Randomized, Controlled Experimental Trial. Nutrients 2020, 12, 3306. [Google Scholar] [CrossRef]
- Fekih, S.; Zguira, M.S.; Koubaa, A.; Masmoudi, L.; Bragazzi, N.L.; Jarraya, M. Effects of Motor Mental Imagery Training on Tennis Service Performance during the Ramadan Fasting: A Randomized, Controlled Trial. Nutrients 2020, 12, 1035. [Google Scholar] [CrossRef] [Green Version]
- Hemayattalab, R.; Movahedi, A. Effects of different variations of mental and physical practice on sport skill learning in adolescents with mental retardation. Res. Dev. Disabil. 2010, 31, 81–86. [Google Scholar] [CrossRef]
- Kanthack, T.F.D.; Bigliassi, M.; Vieira, L.F.; Altimari, L.R. Efeito agudo da imagética no desempenho de lances livres e percepção de autoeficácia em atletas. Braz. J. Kinanthropometry Hum. Perform. 2013, 16, 47–57. [Google Scholar] [CrossRef] [Green Version]
- Mohammadhasani, F.; Rostami, R.; Cheric, M.C. The Effect of a Combined Practice Course of Mental and Physical Practice with Systematic Increase in Contextual Interference on Learning a Kata Skill. Ann. Appl. Sport Sci. 2017, 5, 73–80. [Google Scholar] [CrossRef] [Green Version]
- Norouzi, E.; Hossini, R.N.S.; Afroozeh, M.S.; Vaezmosavi, M.; Gerber, M.; Puehse, U.; Brand, S. Examining the Effectiveness of a PETTLEP Imagery Intervention on the Football Skill Performance of Novice Athletes. J. Imag. Res. Sport Phys. Act. 2019, 14. [Google Scholar] [CrossRef]
- Porretta, D.L.; Surburg, P.R. Imagery and Physical Practice in the Acquisition of Gross Motor Timing of Coincidence by Adolescents with Mild Mental Retardation. Percept. Mot. Ski. 1995, 80, 1171–1183. [Google Scholar] [CrossRef]
- Quinton, M.L.; Cumming, J.; Gray, R.; Geeson, J.R.; Cooper, A.; Crowley, H.; Williams, S.E. A PETTLEP Imagery Intervention with Young Athletes. J. Imag. Res. Sport Phys. Act. 2014, 9. [Google Scholar] [CrossRef]
- Screws, D.P.; Surburg, P.R. Motor Performance of Children with Mild Mental Disabilities after Using Mental Imagery. Adapt. Phys. Act. Q. 1997, 14, 119–130. [Google Scholar] [CrossRef]
- Seif-Barghi, T.; Kordi, R.; Memari, A.-H.; Mansournia, M.A.; Jalali-Ghomi, M. The Effect of an Ecological Imagery Program on Soccer Performance of Elite Players. Asian J. Sports Med. 2012, 3, 81–89. [Google Scholar] [CrossRef] [Green Version]
- Simonsmeier, B.A.; Frank, C.; Gubelmann, H.; Schneider, M. The effects of motor imagery training on performance and mental representation of 7- to 15-year-old gymnasts of different levels of expertise. Sport Exerc. Perform. Psychol. 2018, 7, 155–168. [Google Scholar] [CrossRef]
- Surburg, P.R.; Porretta, D.L.; Sutlive, V. Use of Imagery Practice for Improving a Motor Skill. Adapt. Phys. Act. Q. 1995, 12, 217–227. [Google Scholar] [CrossRef]
- Takazono, P.S.; Teixeira, L.A. Efeito da associação de prática imagética e física na aprendizagem motora em crianças. Braz. J. Kinanthropometry Hum. Perform. 2018, 20, 363–372. [Google Scholar] [CrossRef] [Green Version]
- Wilson, P.H.; Thomas, P.R.; Maruff, P. Motor Imagery Training Ameliorates Motor Clumsiness in Children. J. Child Neurol. 2002, 17, 491–498. [Google Scholar] [CrossRef]
- Review Manager Web (RevMan 5); The Cochrane Collaboration: London, UK, 2020.
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 11. [Google Scholar] [CrossRef]
- GRADEpro GDT: GRADEpro Guideline Development Tool; McMaster University (Developed by Evidence Prime, Inc.): Hamilton, ON, Canada, 2020.
- Grezes, J.; Decety, J. Functional anatomy of execution, mental simulation, observation, and verb generation of actions: A meta-analysis. Hum. Brain Mapp. 2001, 12, 1–19. [Google Scholar] [CrossRef]
- Gerardin, E.; Sirigu, A.; Lehéricy, S.; Poline, J.-B.; Gaymard, B.; Marsault, C.; Agid, Y.; Le Bihan, D. Partially Overlapping Neural Networks for Real and Imagined Hand Movements. Cereb. Cortex 2000, 10, 1093–1104. [Google Scholar] [CrossRef]
- Marshall, B.; Wright, D.; Holmes, P.; Williams, J.; Wood, G. Combined action observation and motor imagery facilitates visuomotor adaptation in children with developmental coordination disorder. Res. Dev. Disabil. 2020, 98, 103570. [Google Scholar] [CrossRef]
- Scott, M.W.; Emerson, J.R.; Dixon, J.; Tayler, M.A.; Eaves, D.L. Motor imagery during action observation enhances imitation of everyday rhythmical actions in children with and without developmental coordination disorder. Hum. Mov. Sci. 2020, 71, 102620. [Google Scholar] [CrossRef] [PubMed]
- Holmes, P.S.; Collins, D.J. The PETTLEP Approach to Motor Imagery: A Functional Equivalence Model for Sport Psychologists. J. Appl. Sport Psychol. 2001, 13, 60–83. [Google Scholar] [CrossRef]
- Guerra, Z.F.; Lucchetti, A.L.G.; Lucchetti, G. Motor Imagery Training After Stroke: A Systematic Review and Meta-analysis of Randomized Controlled Trials. J. Neurol. Phys. Ther. 2017, 41, 205–214. [Google Scholar] [CrossRef]
- Caeyenberghs, K.; Tsoupas, J.; Wilson, P.; Smits-Engelsman, B.C.M. Motor Imagery Development in Primary School Children. Dev. Neuropsychol. 2009, 34, 103–121. [Google Scholar] [CrossRef]
- Mulder, T.; Hochstenbach, J.; van Heuvelen, M.; Otter, A.D. Motor imagery: The relation between age and imagery capacity. Hum. Mov. Sci. 2007, 26, 203–211. [Google Scholar] [CrossRef]
- Collet, C.; Guillot, A.; Lebon, F.; MacIntyre, T.; Moran, A. Measuring Motor Imagery Using Psychometric, Behavioral, and Psychophysiological Tools. Exerc. Sport Sci. Rev. 2011, 39, 85–92. [Google Scholar] [CrossRef] [Green Version]
- Lequerica, A.; Rapport, L.; Axelrod, B.N.; Telmet, K.; Whitman, R.D. Subjective and Objective Assessment Methods of Mental Imagery Control: Construct Validations of Self-Report Measures. J. Clin. Exp. Neuropsychol. 2002, 24, 1103–1116. [Google Scholar] [CrossRef]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 explanation and elaboration: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c869. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, T.C.; Glasziou, P.P.; Boutron, I.; Milne, R.; Perera, R.; Moher, D.; Altman, D.G.; Barbour, V.; Macdonald, H.; Johnston, M.; et al. Better reporting of interventions: Template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014, 348. [Google Scholar] [CrossRef] [Green Version]
- Von Hippel, P.T. The heterogeneity statistic I2 can be biased in small meta-analyses. BMC Med Res. Methodol. 2015, 15, 35. [Google Scholar] [CrossRef] [Green Version]




| No. | Query | Results |
|---|---|---|
| #5 | #1 AND #2 AND #3 NOT [conference abstract]/lim NOT ([animals]/lim NOT [humans]/lim) | 1388 |
| #4 | #1 AND #2 AND #3 | 1695 |
| #3 | ‘controlled clinical trial’/exp OR crossover*:ti,ab,kw OR ‘cross-over*’:ti,ab,kw OR placebo*:ti,ab,kw OR sham:ti,ab,kw OR (((single OR double) NEAR/2 blind*):ti,ab,kw) OR random*:ti,ab,kw OR allocat*:ti,ab,kw OR factorial*:ti,ab,kw OR assign*:ti,ab,kw OR (((clinical OR controlled) NEAR/2 (trial* OR stud*)):ti,ab,kw) OR trial:ti | 3,145,824 |
| #2 | ‘motor imagery’/exp OR ‘motor imagery training’/exp OR ‘imagery’/exp OR ‘imagination’/exp OR (((motor OR locomot* OR mental OR kinesthetic* OR kinaesthetic* OR movement*) NEAR/2 (imag*OR simulation* OR ideation* OR visual*)):ti,ab,kw) OR (((mental* OR cognitive* OR covert*) NEAR/2 (movement* OR rehears* OR imag* OR practic* OR practis* OR training* OR represent*OR stimulation* OR ideation* OR visual*)):ti,ab,kw) OR imagery:ti,ab,kw OR imagining:ti,ab,kw OR imagination*:ti,ab,kw | 64,715 |
| #1 | ‘child’/exp OR ‘adolescent’/exp OR ‘pediatrics’/exp OR ‘cerebral palsy’/exp OR ‘developmental coordination disorder’/exp OR child*:ti,ab,kw OR boy:ti,ab,kw OR boys:ti,ab,kw OR girl*:ti,ab,kw OR pediatric*:ti,ab,kw OR paediatric*:ti,ab,kw OR adoles*:ti,ab,kw OR teen*:ti,ab,kw OR ‘preschool*’:ti,ab,kw OR (((cerebral OR brain OR spastic) NEAR/2 (palsy OR paralys* OR pares* OR diplegia)):ti,ab,kw) OR ‘developmental coordination disorder*’:ti,ab,kw OR dcd:ti,ab,kw | 4,523,492 |
| Certainty Assessment | No. of Patients | Effect | Quality of Evidence | Importance | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. of Studies | Study Design | Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | MI | Control | Relative (95% CI) | Absolute (95% CI) | ||
| Accuracy (Follow-up range 3 to 4 weeks) | ||||||||||||
| 2 | RCT | serious a | not serious | not serious b | serious c | none | 32 | 34 | - | SMD 1.05 (0.53, 1.57) | ⨁⨁◯◯ LOW | not important |
| Ball stroke speed (Follow-up range 3 to 4 weeks) | ||||||||||||
| 2 | RCT | serious a | not serious | not serious b | serious c | none | 32 | 34 | - | SMD 0.83 (0.33, 1.34) | ⨁⨁◯◯ LOW | not important |
| Tennis service performance (Follow-up range 3 to 4 weeks) | ||||||||||||
| 2 | RCT | serious a | serious d | not serious b | serious c | none | 32 | 34 | - | SMD 1.87 (0.64, 3.10) | ⨁◯◯◯ VERY LOW | not important |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Behrendt, F.; Zumbrunnen, V.; Brem, L.; Suica, Z.; Gäumann, S.; Ziller, C.; Gerth, U.; Schuster-Amft, C. Effect of Motor Imagery Training on Motor Learning in Children and Adolescents: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 9467. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18189467
Behrendt F, Zumbrunnen V, Brem L, Suica Z, Gäumann S, Ziller C, Gerth U, Schuster-Amft C. Effect of Motor Imagery Training on Motor Learning in Children and Adolescents: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(18):9467. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18189467
Chicago/Turabian StyleBehrendt, Frank, Valerie Zumbrunnen, Lynn Brem, Zorica Suica, Szabina Gäumann, Carina Ziller, Ulrich Gerth, and Corina Schuster-Amft. 2021. "Effect of Motor Imagery Training on Motor Learning in Children and Adolescents: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 18: 9467. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18189467