
No Obvious Role for Suspicious Oral Pathogens in Arthritis Development

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Subgingival Microbial Sampling
2.3. DNA Extraction and 16S rRNA Gene Sequencing
2.4. Antibody Measurements in Serum
2.5. Statistics
3. Results
3.1. Patients
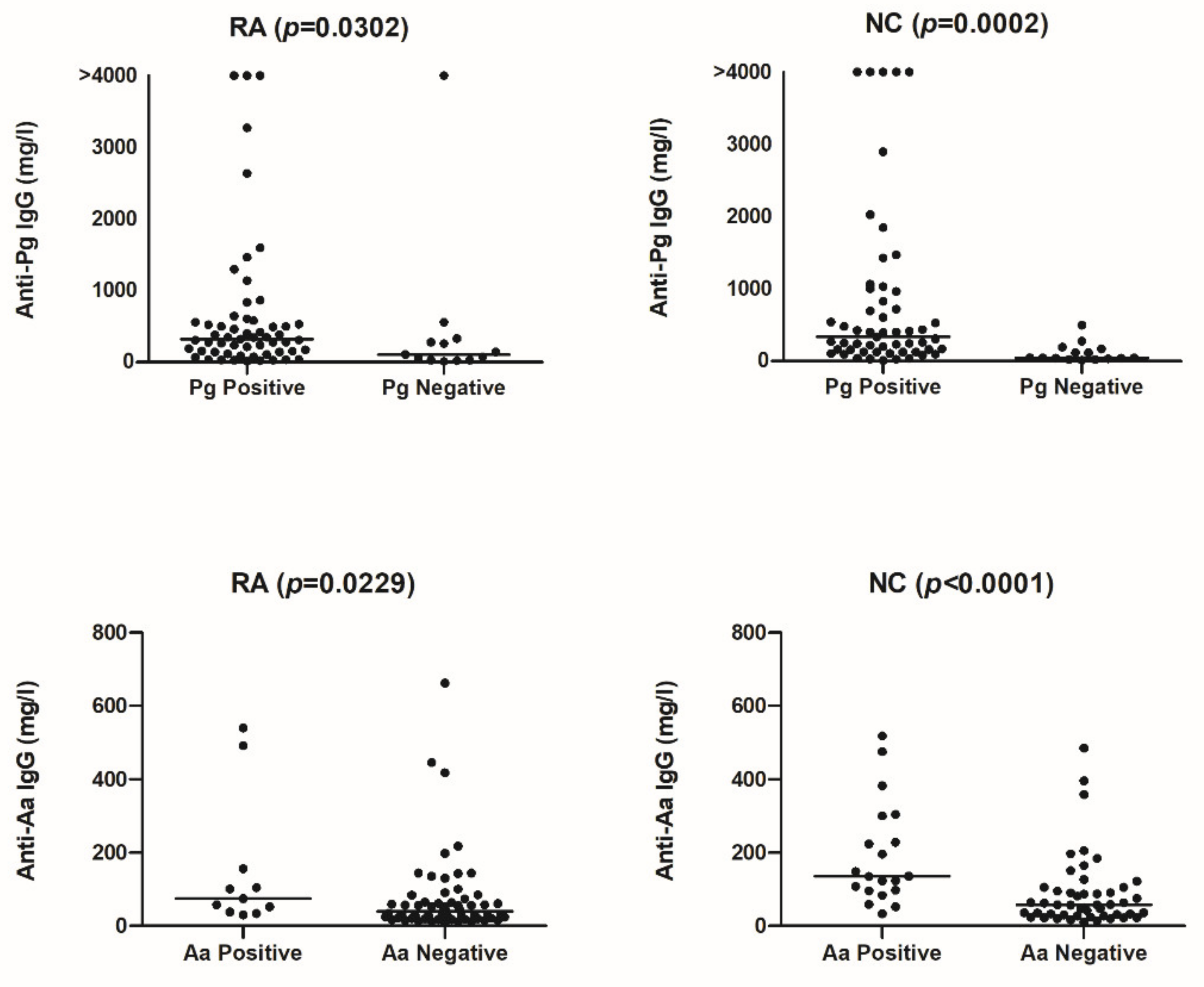
3.2. Correlations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lopez-Oliva, I.; De Pablo, P.; Dietrich, T.; Chapple, I. Gums and joints: Is there a connection? Part one: Epidemiological and clinical links. Br. Dent. J. 2019, 227, 605–609. [Google Scholar] [CrossRef]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.; Bingham, C.O., III; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010, 62, 2569–2581. [Google Scholar] [CrossRef] [PubMed]
- Rosenstein, E.D.; Greenwald, R.A.; Kushner, L.J.; Weissmann, G. Hypothesis: The Humoral Immune Response to Oral Bacteria Provides a Stimulus for the Development of Rheumatoid Arthritis. Inflammation 2004, 28, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Lundberg, K.; Wegner, N.; Yucel-Lindberg, T.; Venables, P.J. Periodontitis in RA—the citrullinated enolase connection. Nat. Rev. Rheumatol. 2010, 6, 727–730. [Google Scholar] [CrossRef]
- Catrina, A.I.; Deane, K.D.; Scher, J.U. Gene, environment, microbiome and mucosal immune tolerance in rheumatoid arthritis. Rheumatology 2016, 55, 391–402. [Google Scholar] [CrossRef] [Green Version]
- Wegner, N.; Wait, R.; Sroka, A.; Eick, S.; Nguyen, K.-A.; Lundberg, K.; Kinloch, A.; Culshaw, S.; Potempa, J.; Venables, P.J. Peptidylarginine deiminase from Porphyromonas gingivalis citrullinates human fibrinogen and α-enolase: Implications for autoimmunity in rheumatoid arthritis. Arthritis Rheum. 2010, 62, 2662–2672. [Google Scholar] [CrossRef] [PubMed]
- Stobernack, T.; Espina, M.D.T.; Mulder, L.M.; Medina, L.M.P.; Piebenga, D.R.; Gabarrini, G.; Zhao, X.; Janssen, K.M.J.; Hulzebos, J.; Brouwer, E.; et al. A Secreted Bacterial Peptidylarginine Deiminase Can Neutralize Human Innate Immune Defenses. MBio 2018, 9, e01704-18. [Google Scholar] [CrossRef] [Green Version]
- Gabarrini, G.; Grasso, S.; van Winkelhoff, A.J.; van Dijl, J.M. Gingimaps: Protein Localization in the Oral Pathogen Porphyromonas gingivalis. Microbiol. Mol. Biol. Rev. 2020, 84, e00032-19. [Google Scholar] [CrossRef]
- Potempa, J.; Mydel, P.; Koziel, J. The case for periodontitis in the pathogenesis of rheumatoid arthritis. Nat. Rev. Rheumatol. 2017, 13, 606–620. [Google Scholar] [CrossRef] [PubMed]
- Konig, M.F.; Abusleme, L.; Reinholdt, J.; Palmer, R.J.; Teles, R.P.; Sampson, K.; Rosen, A.; Nigrovic, P.A.; Sokolove, J.; Giles, J.T.; et al. Aggregatibacter actinomycetemcomitans-induced hypercitrullination links periodontal infection to autoimmunity in rheumatoid arthritis. Sci. Transl. Med. 2016, 8, 369ra176. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, R.D.O.; Silva, R.D.B.; Magno, M.B.; Almeida, A.P.C.P.S.C.; Fagundes, N.C.F.; Maia, L.; Lima, R.R. Does periodontitis represent a risk factor for rheumatoid arthritis? A systematic review and meta-analysis. Ther. Adv. Musculoskelet. Dis. 2019, 11. [Google Scholar] [CrossRef]
- Johansson, L.; Sherina, N.; Kharlamova, N.; Potempa, B.; Larsson, B.; Israelsson, L.; Potempa, J.; Rantapää-Dahlqvist, S.; Lundberg, K. Concentration of antibodies against Porphyromonas gingivalis is increased before the onset of symptoms of rheumatoid arthritis. Arthritis Res. 2016, 18, 201. [Google Scholar] [CrossRef] [Green Version]
- Rahajoe, P.S.; De Smit, M.; Schuurmans, G.; Raveling-Eelsing, E.; Kertia, N.; Vissink, A.; Westra, J. Increased IgA anti-citrullinated protein antibodies in the periodontal inflammatory exudate of healthy individuals compared to rheumatoid arthritis patients. J. Clin. Periodontol. 2020, 47, 552–560. [Google Scholar] [CrossRef]
- Nesse, W.; Abbas, F.; Van Der Ploeg, I.; Spijkervet, F.K.L.; Dijkstra, P.U.; Vissink, A. Periodontal inflamed surface area: Quantifying inflammatory burden. J. Clin. Periodontol. 2008, 35, 668–673. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heida, F.H.; Van Zoonen, A.G.J.F.; Hulscher, J.B.F.; Kiefte, B.J.C.T.; Wessels, R.; Kooi, E.M.W.; Bos, A.F.; Harmsen, H.J.M.; de Goffau, M. A Necrotizing Enterocolitis-Associated Gut Microbiota Is Present in the Meconium: Results of a Prospective Study. Clin. Infect. Dis. 2016, 62, 863–870. [Google Scholar] [CrossRef] [Green Version]
- Bartram, A.K.; Lynch, M.D.J.; Stearns, J.C.; Moreno-Hagelsieb, G.; Neufeld, J.D. Generation of Multimillion-Sequence 16S rRNA Gene Libraries from Complex Microbial Communities by Assembling Paired-End Illumina Reads. Appl. Environ. Microbiol. 2011, 77, 3846–3852. [Google Scholar] [CrossRef] [Green Version]
- Ludwig, W.; Strunk, O.; Westram, R.; Richter, L.; Meier, H.; Yadhukumar, A.; Buchner, A.; Lai, T.; Steppi, S.; Jobb, G.; et al. ARB: A software environment for sequence data. Nucleic Acids Res. 2004, 32, 1363–1371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masella, A.P.; Bartram, A.K.; Truszkowski, J.M.; Brown, D.G.; Neufeld, J.D. PANDAseq: Paired-end assembler for illumina sequences. BMC Bioinform. 2012, 13, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veloo, A.; Elgersma, P.; Friedrich, A.; Nagy, E.; van Winkelhoff, A. The influence of incubation time, sample preparation and exposure to oxygen on the quality of the MALDI-TOF MS spectrum of anaerobic bacteria. Clin. Microbiol. Infect. 2014, 20, O1091–O1097. [Google Scholar] [CrossRef] [Green Version]
- De Smit, M.; Westra, J.; Vissink, A.; Der Meer, B.D.-V.; Brouwer, E.; Van Winkelhoff, A.J. Periodontitis in established rheumatoid arthritis patients: A cross-sectional clinical, microbiological and serological study. Arthritis Res. Ther. 2012, 14, R222. [Google Scholar] [CrossRef] [Green Version]
- Van Leeuwen, M.A.; Westra, J.; Van Riel, P.; Limburg, P.C.; Van Rijswijk, M.H. IgM, IgA, and IgG Rheumatoid Factors in Early Rheumatoid Arthritis Predictive of Radiological Progression? Scand. J. Rheumatol. 1995, 24, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Westra, J.; Brouwer, E.; Raveling-Eelsing, E.; Arends, S.; Abdulle, A.E.; Roozendaal, C.; Delft, M.A.M.V.; Toes, R.E.M.; Trouw, L.A.; Vissink, A.; et al. Arthritis autoantibodies in individuals without rheumatoid arthritis: Follow-up data from a Dutch population-based cohort (Lifelines). Rheumatology 2020, 60, 658–666. [Google Scholar] [CrossRef]
- Scher, J.U.; Ubeda, C.; Equinda, M.; Khanin, R.; Buischi, Y.; Viale, A.; Lipuma, L.; Attur, M.; Pillinger, M.; Weissmann, G.; et al. Periodontal disease and the oral microbiota in new-onset rheumatoid arthritis. Arthritis Rheum. 2012, 64, 3083–3094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leira, Y.; Martín-Lancharro, P.; Blanco, J. Periodontal inflamed surface area and periodontal case definition classification. Acta Odontol. Scand. 2017, 76, 195–198. [Google Scholar] [CrossRef]
- Lakio, L.; Antinheimo, J.; Paju, S.; Buhlin, K.; Pussinen, P.J.; Alfthan, G. Tracking of plasma antibodies against Aggregatibacter actinomycetemcomitans and Porphyromonas gingivalis during 15 years. J. Oral Microbiol. 2009, 1, 1979. [Google Scholar] [CrossRef] [PubMed]
- Mikuls, T.R.; Payne, J.; Yu, F.; Thiele, G.; Reynolds, R.J.; Cannon, G.W.; Markt, J.; McGowan, D.; Kerr, G.S.; Redman, R.S.; et al. Periodontitis and Porphyromonas gingivalisin Patients with Rheumatoid Arthritis. Arthritis Rheumatol. 2014, 66, 1090–1100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmickler, J.; Rupprecht, A.; Patschan, S.; Patschan, D.; Müller, G.A.; Haak, R.; Mausberg, R.F.; Schmalz, G.; Kottmann, T.; Ziebolz, D. Cross-Sectional Evaluation of Periodontal Status and Microbiologic and Rheumatoid Parameters in a Large Cohort of Patients with Rheumatoid Arthritis. J. Periodontol. 2017, 88, 368–379. [Google Scholar] [CrossRef]
- Beyer, K.; Zaura, E.; Brandt, B.W.; Buijs, M.J.; Brun, J.G.; Crielaard, W.; Bolstad, A.I. Subgingival microbiome of rheumatoid arthritis patients in relation to their disease status and periodontal health. PLoS ONE 2018, 13, e0202278. [Google Scholar] [CrossRef] [Green Version]
- Bae, S.-C.; Lee, Y.H. Association between anti-Porphyromonas gingivalis antibody, anti-citrullinated protein antibodies, and rheumatoid arthritis. Z. Rheumatol. 2017, 77, 522–532. [Google Scholar] [CrossRef]
- Volkov, M.; Dekkers, J.; Loos, B.G.; Bizzarro, S.; Huizinga, T.W.J.; Praetorius, H.A.; Toes, R.; Van Der Woude, D. Comment on “Aggregatibacter actinomycetemcomitans–induced hypercitrullination links periodontal infection to autoimmunity in rheumatoid arthritis”. Sci. Transl. Med. 2018, 10, eaan8349. [Google Scholar] [CrossRef] [Green Version]
- Susanto, H.; Nesse, W.; Kertia, N.; Soeroso, J.; Van Reenen, Y.H.; Hoedemaker, E.; Agustina, D.; Vissink, A.; Abbas, F.; Dijkstra, P.U. Prevalence and Severity of Periodontitis in Indonesian Patients with Rheumatoid Arthritis. J. Periodontol. 2013, 84, 1067–1074. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yahya, A.; Bengtsson, C.; Lai, T.C.; Larsson, P.T.; Mustafa, A.N.; Abdullah, N.A.; Muhamad, N.; Hussein, H.; Klareskog, L.; Alfredsson, L.; et al. Smoking is associated with an increased risk of developing ACPA-positive but not ACPA-negative rheumatoid arthritis in Asian populations: Evidence from the Malaysian My EIRA case–control study. Mod. Rheumatol. 2011, 22, 524–531. [Google Scholar] [CrossRef] [PubMed]
- Fia, F.; Westra, J. Overview of rheumatoid arthritis therapy: Management options in Indonesia. Tarumanagara Med. J. 2018, 1, 208–220. [Google Scholar]
- Äyräväinen, L.; Leirisalo-Repo, M.; Kuuliala, A.; Ahola, K.; Koivuniemi, R.; Meurman, J.H.; Heikkinen, A.M. Periodontitis in early and chronic rheumatoid arthritis: A prospective follow-up study in Finnish population. BMJ Open 2017, 7, e011916. [Google Scholar] [CrossRef] [Green Version]
- De Smit, M.; Westra, J.; Posthumus, M.; Springer, G.; van Winkelhoff, A.; Vissink, A.; Brouwer, E.; Bijl, M. Effect of Anti-Rheumatic Treatment on the Periodontal Condition of Rheumatoid Arthritis Patients. Int. J. Environ. Res. Public Health 2021, 18, 2529. [Google Scholar] [CrossRef]
- De Smit, M.; Van De Stadt, L.A.; Janssen, K.M.J.; Der Meer, B.D.-V.; Vissink, A.; Van Winkelhoff, A.J.; Brouwer, E.; Westra, J.; Van Schaardenburg, D. Antibodies against Porphyromonas gingivalisin seropositive arthralgia patients do not predict development of rheumatoid arthritis. Ann. Rheum. Dis. 2014, 73, 1277–1279. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Subject Characteristics | RA (n = 70) | NC (n = 70) | p Value |
|---|---|---|---|
| Age (mean, SD) | 47.3 (11.1) | 46.7 (11.9) | 0.753 |
| Female (n) (%) | 62 (88.6) | 62 (88.6) | 1 |
| Current smoking (n) (%) | 2 (2.9) | 1 (1.4) | 1 |
| Never smoking (n) (%) | 7 (10.00) | 6 (8.6) | 1 |
| Co-morbidity (n) (%): | |||
| Asthma (+bronchodilator) | 0 (0) | 3 (4.3) | 0.245 |
| Hypertension (+medication) | 7 (10.0) | 4 (5.7) | 0.532 |
| Medication for hypertension, also combinations (n): | |||
| Calcium channel blocker | 4 | 2 | |
| ACE inhibitor | 2 | 2 | |
| Angiotensin receptor blocker | 2 | 0 | |
| RA patient characteristics: | |||
| Disease duration in months (median, IQR) | 24 (6–48) | ||
| DAS28 (mean, SD) | 5.1 (1.1) | ||
| Disease remission (DAS28 < 2.6) (n) (%) | 0 (0) | ||
| Low activity (DAS28 ≥ 2.6 < 3.2) (n) (%) | 3 (4.3) | ||
| Moderate activity (DAS28 ≥ 3.2 < 5.1) (n) (%) | 25 (35.7) | ||
| High activity (DAS28 ≥ 5.1) (n) (%) | 42 (60.0) | ||
| Medication for RA (n) (%), also combinations: | |||
| None | 8 (11.4) | ||
| Herbal | 5 (7.1) | ||
| NSAID | 44 (62.9) | ||
| Steroid | 55 (78.6) | ||
| DMARD total | 40 (57.1) | ||
| DMARD specific (n): | |||
| Methotrexate | 32 | ||
| Leflunomide | 2 | ||
| Chloroquine | 2 | ||
| Sulfasalazine | 11 | ||
| ACPA seropositive (n) (%): | |||
| IgG (>10 U/mL) | 29 (41.4) | 0 (0) | <0.000 |
| IgA † (>1.26 U/mL) | 27 (38.6) | 3 (4.3) | <0.000 |
| RF seropositive (n) (%): | |||
| IgM (>5 IU/mL) | 34 (48.6) | 1 (1.4) | <0.000 |
| IgA (>25 IU/mL) | 25 (35.7) | 0 (0) | <0.000 |
| RA | RA-nonPD | RA-PD | NC | NC-nonPD | NC-PD | p Value | |
|---|---|---|---|---|---|---|---|
| N (%) | 70 (100) | 55 (78.6) | 15 (21.4) | 70 (100) | 53 (75.7) | 17 (24.3) | RA-NC |
| Number of teeth (median, IQR) | 26 (22–28) | 26 (22–28) | 26 (22–29) | 27 (24–30) | 28 (23–31) | 27 (25–28) | 0.072 |
| PISA in mm2 (median, range) | 4.9 (0–1319) | 0.3 (0–126) | 304 (158–1319) | 8.0 (0–1897) | 0 (0–94) | 509 (133–18,970) | 0.635 |
| % of sites with pocket probing depth 1–2 mm | 96 (74–99) | 56 (42–71) | 97 (94–99) | 93 (75–100) | 54 (34–63) | 97 (89–100) | |
| (median, IQR) | |||||||
| % of sites with pocket probing depth 3–4 mm | 4.7 (0.7–24.3) | 41 (27–44) | 2.3 (0.6–6.1) | 5.6 (0–19.4) | 37 (22–43) | 2.1 (0–8.1) | |
| (median, IQR) | |||||||
| % of sites with pocket probing depth ≥5 mm | 0 (0–0.8) | 3.8 (1.1–13) | 0 (0–0) | 0 (0–2.6) | 6.2 (2.0–23) | 0 (0–0) | |
| (median, IQR) | |||||||
| % of sites with bleeding on probing | 1.1 (0–11) | 35 (18–57) | 0.6 (0–2.2) | 1.1 (0–10) | 30 (12–46) | 0 (0–2.8) | |
| (median, IQR) | |||||||
| Periodontal pathogens detected: | |||||||
| P. gingivalis (Pg) (n) (%) | 57 (81.4) | 45 (81.8) | 12 (80.0) | 55 (78.6) | 43 (81.1) | 13 (76.5) | 0.834 |
| A. actinomycetemcomitans (Aa) (n) (%) | 11 (15.7) | 9 (16.4) | 2 (13.3) | 21 (30.0) | 14 (26.4) | 7 (41.2) | 0.070 |
| Pg + Aa (n) (%) | 10 (14.3) | 8 (14.5) | 2 (13.3) | 19 (27.1) | 12(22.6) | 7 (41.2) | 0.094 |
| Correlations | RA (n = 70) | NC (n = 70) | ||
|---|---|---|---|---|
| with anti-Pg | ρ | p-value | ρ | p-value |
| Pg relative abundance | 0.384 | 0.001 | 0.35 | 0.003 |
| PISA | −0.087 | 0.472 | 0.179 | 0.138 |
| ACPA IgG | 0.137 | 0.259 | −0.074 | 0.542 |
| ACPA IgA | 0.207 | 0.086 | −0.054 | 0.659 |
| RF IgM | 0.132 | 0.276 | −0.048 | 0.691 |
| RF IgA | 0.11 | 0.227 | 0.058 | 0.632 |
| with anti-Aa | ρ | p-value | ρ | p-value |
| Aa relative abundance | 0.292 | 0.014 | 0.524 | <0.000 |
| PISA | −0.117 | 0.335 | 0.117 | 0.333 |
| ACPA IgG | 0.011 | 0.929 | 0.271 | 0.024 |
| ACPA IgA | −0.111 | 0.36 | 0.111 | 0.362 |
| RF IgM | 0.028 | 0.816 | 0.043 | 0.729 |
| RF IgA | 0.056 | 0.647 | 0.056 | 0.645 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rahajoe, P.S.; de Smit, M.J.; Raveling-Eelsing, E.; du Teil Espina, M.; Stobernack, T.; Lisotto, P.; Harmsen, H.J.M.; van Dijl, J.M.; Kertia, N.; Vissink, A.; et al. No Obvious Role for Suspicious Oral Pathogens in Arthritis Development. Int. J. Environ. Res. Public Health 2021, 18, 9560. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18189560
Rahajoe PS, de Smit MJ, Raveling-Eelsing E, du Teil Espina M, Stobernack T, Lisotto P, Harmsen HJM, van Dijl JM, Kertia N, Vissink A, et al. No Obvious Role for Suspicious Oral Pathogens in Arthritis Development. International Journal of Environmental Research and Public Health. 2021; 18(18):9560. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18189560
Chicago/Turabian StyleRahajoe, Poerwati S., Menke J. de Smit, Elisabeth Raveling-Eelsing, Marines du Teil Espina, Tim Stobernack, Paola Lisotto, Hermie J. M. Harmsen, Jan Maarten van Dijl, Nyoman Kertia, Arjan Vissink, and et al. 2021. "No Obvious Role for Suspicious Oral Pathogens in Arthritis Development" International Journal of Environmental Research and Public Health 18, no. 18: 9560. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18189560