
Clinical Presentations of Adolescents Aged 16–18 Years in the Adult Emergency Department

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Collection and Extraction
2.3. Statistical Analysis
3. Results
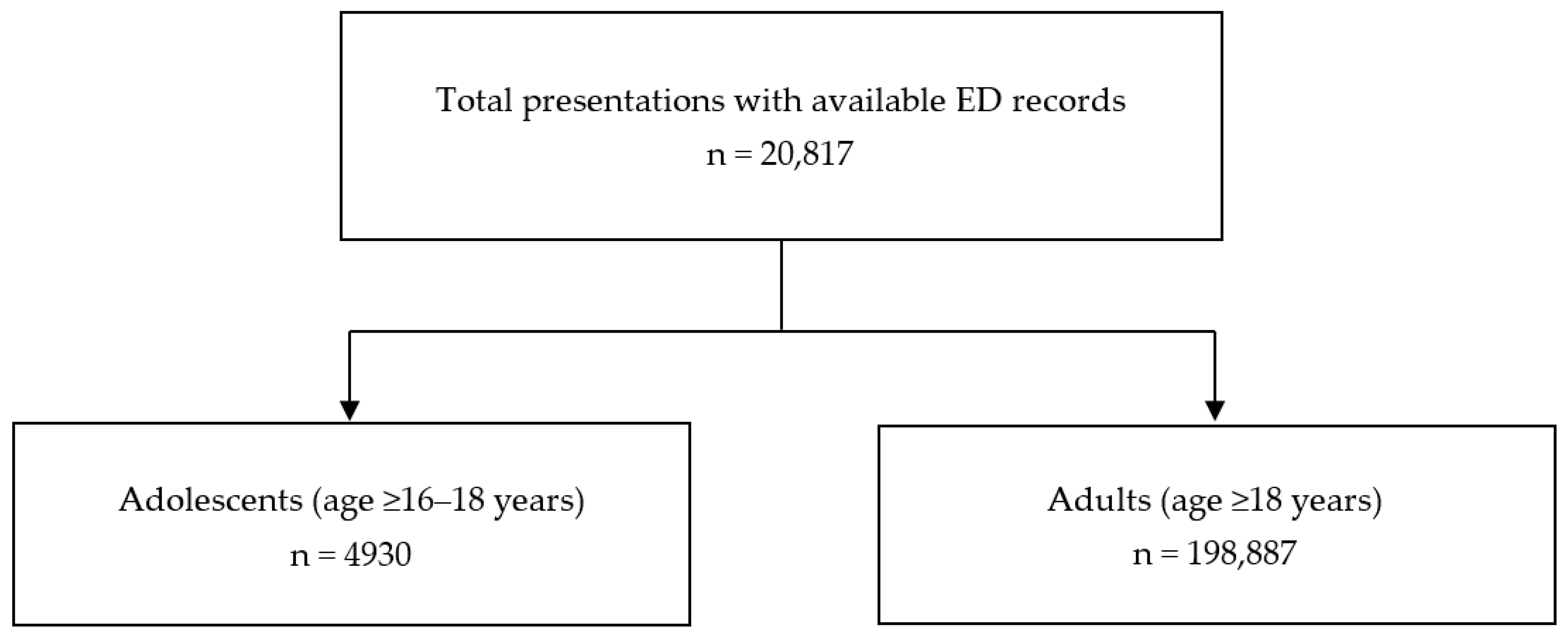
3.1. Study Population
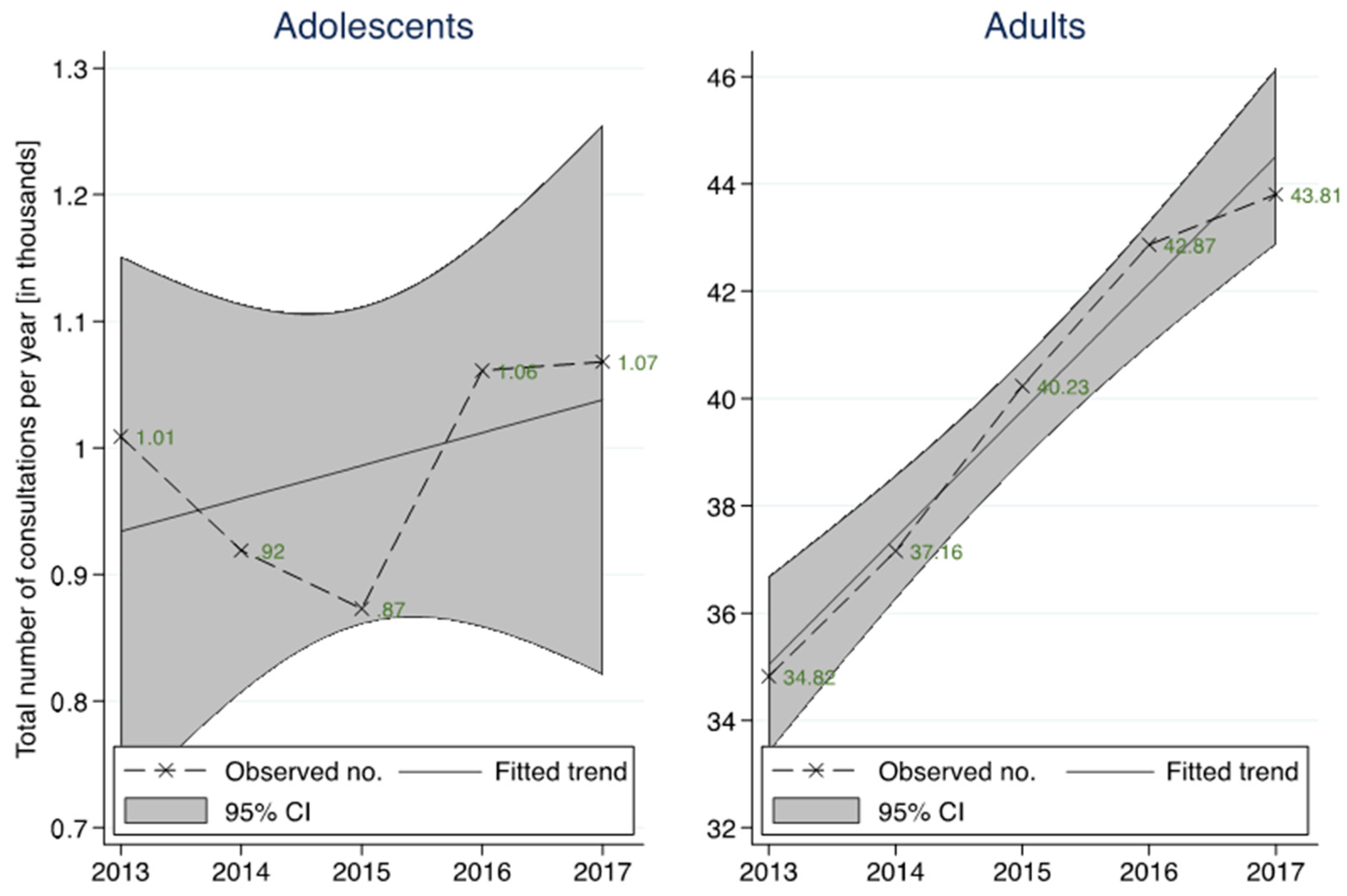
3.2. Annual Changes
3.3. Presentation Characteristics
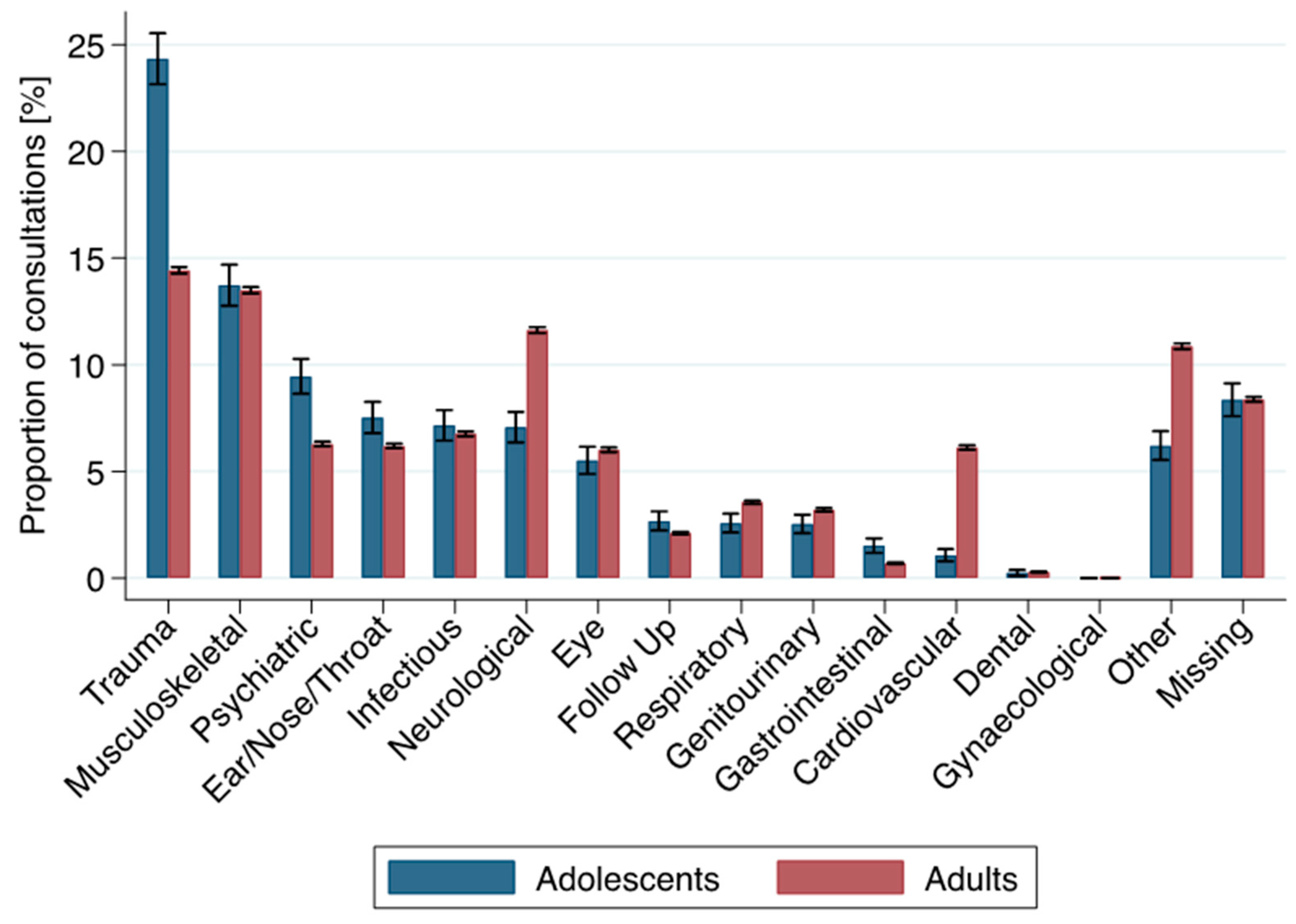
3.4. Principle Complaint Groups
3.5. Discharge
3.6. Sensitivity Analysis
4. Discussion
4.1. Summary of Findings
4.2. Comparison with Other Studies
4.3. Strengths and Limitations
4.4. Relevance/Discussion of the Findings
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Volans, A.; Blatchford, O.; Capewell, S. Trends in emergency admissions. Br. Med. J. 1999, 319, 1201. [Google Scholar] [CrossRef]
- Tang, N.; Stein, J.; Hsia, R.Y.; Maselli, J.H.; Gonzales, R. Trends and Characteristics of US Emergency Department Visits, 1997-2007. J. Am. Med. Assoc. 2010, 304, 664–670. [Google Scholar] [CrossRef] [Green Version]
- Weiss, A.J.; Wier, L.M.; Stocks, C.; Blanchard, J. Overview of Emergency Department Visits in the United States. Available online: https://pubmed.ncbi.nlm.nih.gov/25144109/ (accessed on 11 September 2021).
- Müller, M.; Schechter, C.B.; Hautz, W.E.; Sauter, T.C.; Exadaktylos, A.K.; Stock, S.; Birrenbach, T. The development and validation of a resource consumption score of an emergency department consultation. PLoS ONE 2021, 16, e0247244. [Google Scholar] [CrossRef]
- Zahlen und Fakten Universitäres Notfallzentrum 2013–2019. Available online: http://www.notfallzentrum.insel.ch/de/ueber-uns/ueber-die-klinik/zahlen-und-fakten/ (accessed on 1 June 2021).
- Sands, R.; Shanmugavadivel, D.; Stephenson, T.; Wood, D. Medical problems presenting to paediatric emergency departments: 10 years on. Emerg. Med. J. 2011, 29, 379–382. [Google Scholar] [CrossRef]
- Shanmugavadivel, D.; Sands, R.; Wood, D. Common Presenting Problems for Young People Attending the Emergency Department. Adv. Emerg. Med. 2014, 2014, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Sawyer, S.M.; Patton, G.C. Why are so many more adolescents presenting to our emergency departments with mental health problems? Med. J. Aust. 2018, 208, 339–340. [Google Scholar] [CrossRef] [PubMed]
- Sawyer, S.M.; Azzopardi, P.S.; Wickremarathne, D.; Patton, G.C. The age of adolescence. Lancet Child Adolesc. Health 2018, 2, 223–228. [Google Scholar] [CrossRef]
- Akré, C.; Chamay-Weber, C.; Haller-Hester, D.; Eggimann, S.H.; Hutter, I.; Pizzagalli, C.; Rutishauser, C.; Schlumbom, V. Obere Altersgrenze für Kinderkliniken in der Schweiz. Paediatrica 2014, 25, 7–8. [Google Scholar] [CrossRef]
- United Nations International Children’s Emergency Fund. The State of the World’s Children; United Nations International Children’s Emergency Fund: New York, NY, USA, 1985; Volume 17. [Google Scholar]
- Kinderspital Zürich. Available online: https://www.kispi.uzh.ch/de/zuweiser/fachbereiche/notfallstation/Seiten/default.aspx#a=akk3 (accessed on 1 June 2021).
- Universitättsspital Basel. Available online: https://www.gesundheit.bs.ch/schulgesundheit/beratungen-abklaerungen/notfall-erste-hilfe.html (accessed on 1 June 2021).
- Kantonasspital Luzern. Available online: https://www.luks.ch/standorte/standort-luzern/kinderspital (accessed on 1 June 2021).
- Hôpital Universitaire Genève. Available online: https://www.hug.ch/de/kinderspital (accessed on 1 June 2021).
- Kinderspital Winterthur. Available online: https://www.ksw.ch/klinik/kinder-und-jugendmedizin/angebot/notfallstation/ (accessed on 1 June 2021).
- Kantonsspital Aarau. Available online: https://www.ksa.ch/zentren-kliniken/klinik-fuer-kinder-und-jugendliche/leistungsangebot (accessed on 1 June 2021).
- Burns, C.; Wang, N.E.; Goldstein, B.A.; Hernandez-Boussard, T. Characterization of Young Adult Emergency Department Users: Evidence to Guide Policy. J. Adolesc. Health 2016, 59, 654–661. [Google Scholar] [CrossRef] [Green Version]
- Montalbano, A.; Rodean, J.; Kangas, J.; Lee, B.; Hall, M. Urgent care and emergency department visits in the pediatric medicaid population. Pediatrics 2016, 137, e20153100. [Google Scholar] [CrossRef] [Green Version]
- Rhine, T.; Gittelman, M.; Timm, N. Prevalence and Trends of the Adult Patient Population in a Pediatric Emergency Department. Pediatr. Emerg. Care 2012, 28, 141–144. [Google Scholar] [CrossRef]
- Fortuna, R.J.; Robbins, B.W.; Mani, N.; Halterman, J.S. Dependence on Emergency Care among Young Adults in the United States. J. Gen. Intern. Med. 2010, 25, 663–669. [Google Scholar] [CrossRef] [Green Version]
- McDermott, K.W.; Stocks, C.; Freeman, W.J. Overview of Pediatric Emergency Department Visits, 2015: Statistical Brief #242. Healthc. Cost Util. Proj. Stat. Briefs 2018, 39, 1–17. [Google Scholar]
- Venkatesh, A.K.; Dai, Y.; Ross, J.S.; Schuur, J.D.; Capp, R.; Krumholz, H.M. Variation in US Hospital Emergency Department Admission Rates by Clinical Condition. Med. Care 2015, 53, 237–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- A Lowthian, J.; Curtis, A.; Cameron, P.; Stoelwinder, J.U.; Cooke, M.W.; McNeil, J. Systematic review of trends in emergency department attendances: An Australian perspective. Emerg. Med. J. 2010, 28, 373–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bayerl, C. Kinder sind keine kleinen Erwachsenen. Aktuel Dermatol. 2013, 39, 63. [Google Scholar] [CrossRef]
- Kalb, L.G.; Stapp, E.K.; Ballard, E.D.; Holingue, C.; Keefer, A.; Riley, A. Trends in Psychiatric Emergency Department Visits among Youth and Young Adults in the US. Pediatrics 2019, 143, e20182192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiscock, H.; Neely, R.J.; Lei, S.; Freed, G. Paediatric mental and physical health presentations to emergency departments, Victoria, 2008–15. Med. J. Aust. 2018, 208, 343–348. [Google Scholar] [CrossRef]
- Torio, C.M.; Encinosa, W.; Berdahl, T.; McCormick, M.C.; Simpson, L.A. Annual Report on Health Care for Children and Youth in the United States: National Estimates of Cost, Utilization and Expenditures for Children with Mental Health Conditions. Acad. Pediatr. 2015, 15, 19–35. [Google Scholar] [CrossRef]
- Leeb, R.T.; Bitsko, R.H.; Radhakrishnan, L.; Martinez, P.; Njai, R.; Holland, K.M. Mental Health–Related Emergency Department Visits Among Children Aged < 18 Years during the COVID-19 Pandemic—United States, January 1–October 17, 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 1680. [Google Scholar]
- Tolentino, A.; Symington, L.; Jordan, F.; Kinnear, F.; Jarvis, M. Mental health presentations to a paediatric emergency department. Emerg. Med. Australas. 2020, 33, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Hautz, W.E.; Sauter, T.C.; Exadakytlos, A.K.; Krummrey, G.; Schauber, S.; Müller, M. Barriers to seeking emergency care during the COVID-19 pandemic may lead to higher morbidity and mortality—A retrospective study from a Swiss university hospital. Swiss Med. Wkly. 2020, 150, w20331. [Google Scholar] [CrossRef]
- Remick, K.; Gausche-Hill, M.; Joseph, M.M.; Brown, K.; Snow, S.K.; Wright, J.L. Pediatric readiness in the emergency department. Pediatrics 2018, 142, e20182459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klenk, L.; Von Rütte, C.; Henssler, J.; Sauter, T.C.; Hautz, W.E.; Exadaktylos, A.K.; Müller, M. Resource consumption of multi-substance users in the emergency room: A neglected patient group. PLoS ONE 2019, 14, e0223118. [Google Scholar] [CrossRef] [PubMed]
- Müller, M.; E Ricklin, M.; Weiler, S.; Exadaktylos, A.K.; Arampatzis, S. Emergency medicine in the extreme geriatric era: A retrospective analysis of patients aged in their mid 90s and older in the emergency department. Geriatr. Gerontol. Int. 2017, 18, 415–420. [Google Scholar] [CrossRef]
- E Hautz, W.; Sauter, T.C.; Hautz, S.C.; E Kämmer, J.; Schauber, S.K.; Birrenbach, T.; Exadaktylos, A.K.; Stock, S.; Müller, M. What determines diagnostic resource consumption in emergency medicine: Patients, physicians or context? Emerg. Med. J. 2020, 37, 546–551. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Hospital | Paediatric ED Age Limit (years) |
|---|---|
| Aarau | 18 |
| Basel University | 18 |
| Geneva | 16 1 |
| Lucerne | 16 2 |
| Winterthur | 16 |
| Zurich University | 16 |
| Category | Adolescents 16–18 (n = 4930) | Adults ≥18 (n = 198,887) | p | ||
|---|---|---|---|---|---|
| Year, n (%) | <0.001 | ||||
| 2013 | 1009 | (20.5) | 34,821 | (17.5) | |
| 2014 | 919 | (18.6) | 37,159 | (18.7) | |
| 2015 | 873 | (17.7) | 40,234 | (20.2) | |
| 2016 | 1061 | (21.5) | 42,867 | (21.6) | |
| 2017 | 1068 | (21.7) | 43,806 | (22.0) | |
| Presentation Date and Time | |||||
| Saturday or Sunday admission (00:00–23:59), n (%) | 1497 | (30.4) | 58,061 | (29.2) | 0.074 |
| Public and cantonal (Bern) holidays, n (%) | 98 | (2.0) | 4009 | (2.0) | 0.891 |
| Night-time admissions (19:00–06:59), n (%) | 1929 | (39.1) | 62,670 | (31.5) | <0.001 |
| Day of the week, n (%) | 0.331 | ||||
| Monday | 712 | (14.4) | 29,725 | (14.9) | |
| Tuesday | 666 | (13.5) | 27,113 | (13.6) | |
| Wednesday | 675 | (13.7) | 27,296 | (13.7) | |
| Thursday | 663 | (13.4) | 27,524 | (13.8) | |
| Friday | 717 | (14.5) | 29,168 | (14.7) | |
| Saturday | 737 | (14.9) | 29,912 | (15.0) | |
| Sunday | 760 | (15.4) | 28,149 | (14.2) | |
| Type of Admission, n (%) | <0.001 | ||||
| Ambulance | 506 | (10.3) | 29,224 | (14.7) | |
| General practitioner | 170 | (3.4) | 10,969 | (5.5) | |
| External hospital | 243 | (4.9) | 15,231 | (7.7) | |
| Police | 73 | (1.5) | 2154 | (1.1) | |
| Air rescue | 65 | (1.3) | 2465 | (1.2) | |
| Repatriation | 5 | (0.1) | 319 | (0.2) | |
| Walk-in | 2674 | (54.2) | 89,254 | (44.9) | |
| Internal referral | 180 | (3.7) | 8238 | (4.1) | |
| Urgent care centre/doctor | 49 | (1.0) | 1787 | (0.9) | |
| Other | 12 | (0.2) | 769 | (0.4) | |
| Missing information | 953 | (19.3) | 38,477 | (19.3) | |
| Triage, n (%) | <0.001 | ||||
| Life-threatening | 148 | (3.0) | 15,564 | (7.8) | |
| Highly urgent | 889 | (18.0) | 46,193 | (23.2) | |
| Urgent | 3217 | (65.3) | 115,820 | (58.2) | |
| Semi-urgent | 448 | (9.1) | 13,746 | (6.9) | |
| Non-urgent | 125 | (2.5) | 3209 | (1.6) | |
| Missing Information | 103 | (2.1) | 4355 | (2.2) | |
| Resuscitation room treatment, n (%) | 0.001 | ||||
| No | 4704 | (95.4) | 187,573 | (94.3) | |
| Yes | 226 | (4.6) | 11,312 | (5.7) | |
| Principle complaint, n (%) | <0.001 | ||||
| Psychiatric problem (including self-harm) | 466 | (9.5) | 12,494 | (6.3) | |
| Musculoskeletal + rheumatologic problems | 677 | (13.7) | 26,818 | (13.5) | |
| Gastrointestinal problems | 75 | (1.5) | 1389 | (0.7) | |
| Respiratory problems | 127 | (2.6) | 7061 | (3.6) | |
| Neurological problems | 349 | (7.1) | 23,108 | (11.6) | |
| Cardiovascular problems | 53 | (1.1) | 12,174 | (6.1) | |
| Infectious disease, including skin problems | 353 | (7.2) | 13,447 | (6.8) | |
| Obstetric or gynaecological problems | 0 | (0.0) | 26 | (0.0) | |
| Dental problems | 12 | (0.2) | 580 | (0.3) | |
| Eye problems | 272 | (5.5) | 11,963 | (6.0) | |
| Other | 306 | (6.2) | 21,610 | (10.9) | |
| Trauma | 1200 | (24.3) | 28,685 | (14.4) | |
| Genitourinary problems | 125 | (2.5) | 6359 | (3.2) | |
| Ear/nose/throat problems | 371 | (7.5) | 12,311 | (6.2) | |
| Follow-up | 132 | (2.7) | 4205 | (2.1) | |
| Missing information | 412 | (8.4) | 16,657 | (8.4) | |
| Discharge, n (%) | <0.001 | ||||
| Death | 0 | (0.0) | 332 | (0.2) | |
| Discharge home | 3490 | (70.8) | 103,880 | (52.2) | |
| Hospital admission | 562 | (11.4) | 55,805 | (28.1) | |
| Transfer to external hospital | 320 | (6.5) | 17,426 | (8.8) | |
| Other | 44 | (0.9) | 1711 | (0.9) | |
| Not specified | 514 | (10.4) | 19,724 | (9.9) | |
| Missing information | 0 | (0.0) | 9 | (0.0) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brockhus, L.A.; Bärtsch, M.; Exadaktylos, A.K.; Keitel, K.; Klukowska-Rötzler, J.; Müller, M. Clinical Presentations of Adolescents Aged 16–18 Years in the Adult Emergency Department. Int. J. Environ. Res. Public Health 2021, 18, 9578. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18189578
Brockhus LA, Bärtsch M, Exadaktylos AK, Keitel K, Klukowska-Rötzler J, Müller M. Clinical Presentations of Adolescents Aged 16–18 Years in the Adult Emergency Department. International Journal of Environmental Research and Public Health. 2021; 18(18):9578. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18189578
Chicago/Turabian StyleBrockhus, Lara Aurora, Martina Bärtsch, Aristomenis K. Exadaktylos, Kristina Keitel, Jolanta Klukowska-Rötzler, and Martin Müller. 2021. "Clinical Presentations of Adolescents Aged 16–18 Years in the Adult Emergency Department" International Journal of Environmental Research and Public Health 18, no. 18: 9578. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18189578