
Palliative Care Consultation Services on Terminally Ill Cancer Patients and Non-Cancer Patients: Trend Analysis from a 9-Year-Long Observational Study in Taiwan


Abstract
:1. Introduction
2. Materials and Methods
Statistical Analyses
3. Results
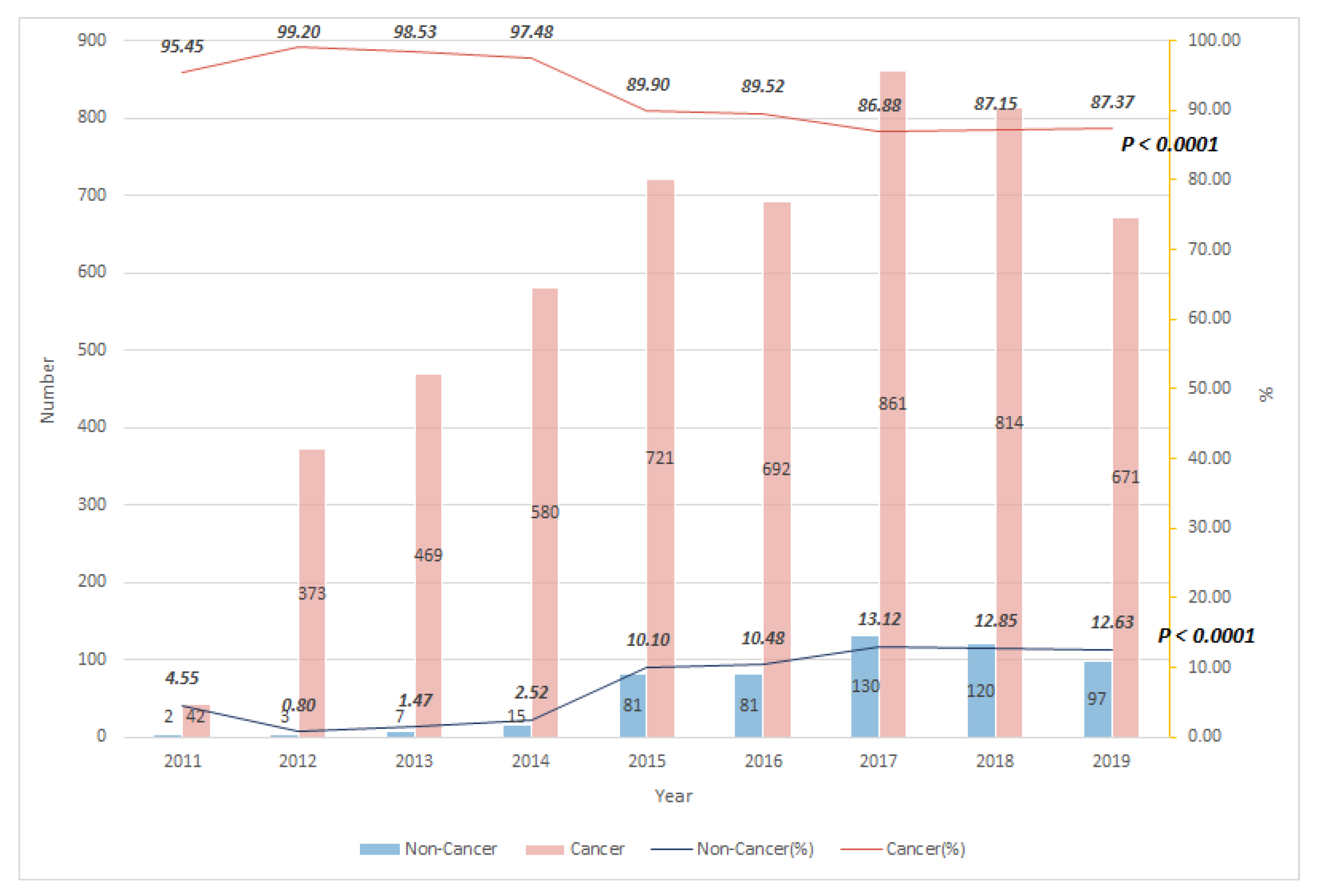
3.1. Trend of Cancer and Non-Cancer Patients Receiving PCCS
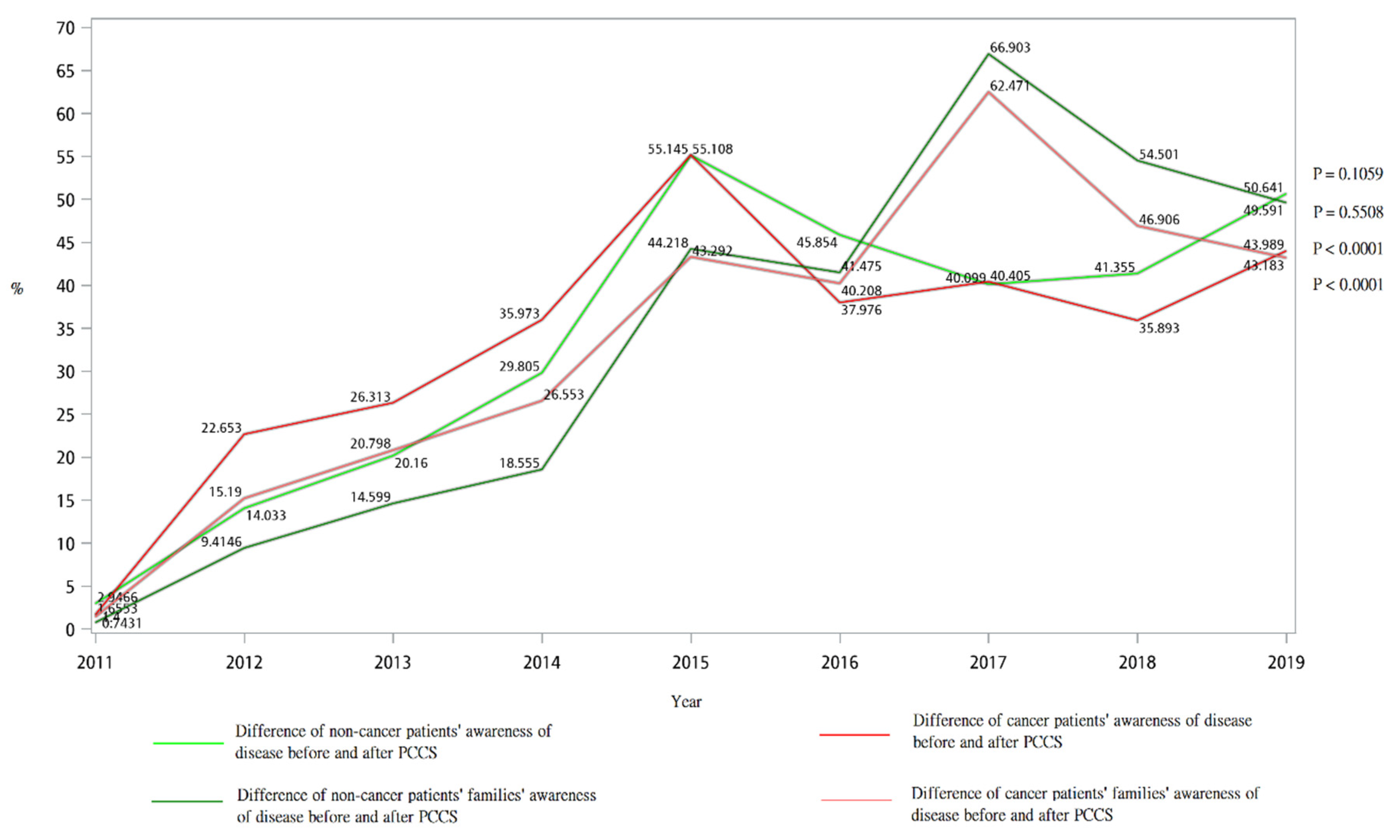
3.2. Awareness of Cancer Patients and Non-Cancer Patients and Their Families before and after PCCS
3.3. Trend of DNR Declaration among Cancer and Non-Cancer Patients Receiving PCCS from 2011 to 2019
3.4. Determinants of Late Referral to PCCS among Cancer and Non-Cancer Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Roth, A.R.; Canedo, A.R. Introduction to Hospice and Palliative Care. Prim. Care Clin. Off. Pr. 2019, 46, 287–302. [Google Scholar] [CrossRef]
- Hui, D.; Bruera, E. Models of Palliative Care Delivery for Patients with Cancer. J. Clin. Oncol. 2020, 38, 852–865. [Google Scholar] [CrossRef]
- Mounsey, L.; Ferres, M.; Eastman, P. Palliative care for the patient without cancer. Aust. J. Gen. Pr. 2018, 47, 765–769. [Google Scholar] [CrossRef] [Green Version]
- Singer, A.E.; Goebel, J.; Kim, Y.S.; Dy, S.M.; Ahluwalia, S.C.; Clifford, M.; Dzeng, E.; O’Hanlon, C.E.; Motala, A.; Walling, A.M.; et al. Populations and Interventions for Palliative and End-of-Life Care: A Systematic Review. J. Palliat. Med. 2016, 19, 995–1008. [Google Scholar] [CrossRef] [Green Version]
- Moens, K.; Higginson, I.J.; Harding, R.; Brearley, S.; Caraceni, A.; Cohen, J.; Costantini, M.; Deliens, L.; Francke, A.L.; Kaasa, S.; et al. Are There Differences in the Prevalence of Palliative Care-Related Problems in People Living with Advanced Cancer and Eight Non-Cancer Conditions? A Systematic Review. J. Pain Symptom Manag. 2014, 48, 660–677. [Google Scholar] [CrossRef]
- Tang, W.-R.; Hong, J.-H.; Rau, K.; Wang, C.; Juang, Y.-Y.; Lai, C.-H.; Fujimori, M.; Fang, C.-K. Truth telling in Taiwanese cancer care: Patients’ and families’ preferences and their experiences of doctors’ practices. Psycho-Oncology 2016, 26, 999–1005. [Google Scholar] [CrossRef]
- Kassianos, A.P.; Ioannou, M.; Koutsantoni, M.; Charalambous, H. The impact of specialized palliative care on cancer patients’ health-related quality of life: A systematic review and meta-analysis. Support. Care Cancer 2018, 26, 61–79. [Google Scholar] [CrossRef] [PubMed]
- Yates, P. Symptom Management and Palliative Care for Patients with Cancer. Nurs. Clin. N. Am. 2017, 52, 179–191. [Google Scholar] [CrossRef]
- Akgün, K.M. Palliative and End-of-Life Care for Patients with Malignancy. Clin. Chest Med. 2017, 38, 363–376. [Google Scholar] [CrossRef] [PubMed]
- Nichols, E.; Szoeke, C.E.; Vollset, S.E.; Abbasi, N.; Abd-Allah, F.; Abdela, J.; Aichour, M.T.E.; Akinyemi, R.O.; Alahdab, F.; Asgedom, S.W.; et al. Global, regional, and national burden of Alzheimer’s disease and other dementias, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 88–106. [Google Scholar] [CrossRef] [Green Version]
- Jha, V.; Garcia, G.G.; Iseki, K.; Li, Z.; Naicker, S.; Plattner, B.; Saran, R.; Wang, A.Y.-M.; Yang, C.-W. Chronic kidney disease: Global dimension and perspectives. Lancet 2013, 382, 260–272. [Google Scholar] [CrossRef]
- Wysham, N.G.; Cox, C.E.; Wolf, S.P.; Kamal, A.H. Symptom Burden of Chronic Lung Disease Compared with Lung Cancer at Time of Referral for Palliative Care Consultation. Ann. Am. Thorac. Soc. 2015, 12, 1294–1301. [Google Scholar] [CrossRef] [PubMed]
- Oskoui, T.; Pandya, R.; Weiner, D.E.; Wong, J.B.; Koch-Weser, S.; Ladin, K. Advance Care Planning Among Older Adults with Advanced Non–Dialysis-Dependent CKD and Their Care Partners: Perceptions Versus Reality? Kidney Med. 2020, 2, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Murray, L.; Butow, P.N.; White, K.; Kiernan, M.C.; D’Abrew, N.; Herz, H. Advance care planning in motor neuron disease: A qualitative study of caregiver perspectives. Palliat. Med. 2016, 30, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Oishi, A.; Murtagh, F. The challenges of uncertainty and interprofessional collaboration in palliative care for non-cancer patients in the community: A systematic review of views from patients, carers and health-care professionals. Palliat. Med. 2014, 28, 1081–1098. [Google Scholar] [CrossRef] [Green Version]
- Alexander, K.; Goldberg, J.; Korc-Grodzicki, B. Palliative Care and Symptom Management in Older Patients with Cancer. Clin. Geriatr. Med. 2016, 32, 45–62. [Google Scholar] [CrossRef] [Green Version]
- Greer, J.A.; Applebaum, A.J.; Jacobsen, J.C.; Temel, J.S.; Jackson, V.A. Understanding and Addressing the Role of Coping in Palliative Care for Patients with Advanced Cancer. J. Clin. Oncol. 2020, 38, 915–925. [Google Scholar] [CrossRef]
- Haun, M.W.; Estel, S.; Rücker, G.; Friederich, H.-C.; Villalobos, M.; Thomas, M.; Hartmann, M. Early palliative care for adults with advanced cancer. Cochrane Database Syst. Rev. 2017, 2017, CD011129. [Google Scholar] [CrossRef]
- Ullrich, A.; Ascherfeld, L.; Marx, G.; Bokemeyer, C.; Bergelt, C.; Oechsle, K. Quality of life, psychological burden, needs, and satisfaction during specialized inpatient palliative care in family caregivers of advanced cancer patients. BMC Palliat. Care 2017, 16, 1–10. [Google Scholar] [CrossRef]
- Higginson, I.J.; Bausewein, C.; Reilly, C.; Gao, W.; Gysels, M.; Dzingina, M.D.; McCrone, P.; Booth, S.; Jolley, C.J.; Moxham, J. An integrated palliative and respiratory care service for patients with advanced disease and refractory breathlessness: A randomised controlled trial. Lancet Respir. Med. 2014, 2, 979–987. [Google Scholar] [CrossRef] [Green Version]
- Hung, Y.-S.; Chen, C.-H.; Yeh, K.-Y.; Chang, H.; Huang, Y.-C.; Chang, C.-L.; Wu, W.-S.; Hsu, H.-P.; Lin, J.-C.; Chou, W.-C. Potential benefits of palliative care for polysymptomatic patients with late-stage nonmalignant disease in Taiwan. J. Formos. Med. Assoc. 2013, 112, 406–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, L.-F.; Chu, C.; Chen, Y.-G.; Ho, C.-L.; Pan, H.-H. Relationship between palliative care consultation service and end-of-life outcomes. Support. Care Cancer 2016, 24, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.-F.; Lin, C.; Hung, Y.-C.; Chang, L.-F.; Ho, C.-L.; Pan, H.-H. Effectiveness of palliative care consultation service on caregiver burden over time between terminally ill cancer and non-cancer family caregivers. Support. Care Cancer 2020, 28, 6045–6055. [Google Scholar] [CrossRef]
- Lu, C.Y.; Shen, W.C.; Kao, C.Y.; Wang, H.M.; Tang, S.C.; Chin, T.L.; Chi, C.C.; Yang, J.M.; Chang, C.W.; Lai, Y.F.; et al. Impact of Palliative Care Consultation Service on Terminally Ill Cancer Patients: A 9-Year Observational Cohort Study in Taiwan. Medicine 2016, 95, e2981. [Google Scholar] [CrossRef]
- Basedow-Rajwich, B.; Montag, T.; Duckert, A.; Schulz, C.; Rajwich, G.; Kleiter, I.; Koehler, J.; Lindena, G. Mobile Palliative Care Consultation Service (PCCS): Overview of Hospice and Palliative Care Evaluation (HOPE) Data on In-Patients with End-Stage Cancer, Multiple Sclerosis, and Noncancer, Nonneurological Disease From 4 PCCS Centers in Germany in 2013. Palliat. Care: Res. Treat. 2018, 11, 1178224218785139. [Google Scholar] [CrossRef]
- Maddison, A.R.; Malik, S.; Smaggus, A. Inpatient Palliative Care Consultations from a Canadian Clinical Teaching Unit: Who is Referred and When? J. Palliat. Care 2018, 33, 204–208. [Google Scholar] [CrossRef] [PubMed]
- Shih, T.-C.; Chang, H.-T.; Lin, M.-H.; Chen, C.-K.; Chen, T.-J.; Hwang, S.-J. Differences in do-not-resuscitate orders, hospice care utilization, and late referral to hospice care between cancer and non-cancer decedents in a tertiary Hospital in Taiwan between 2010 and 2015: A hospital-based observational study. BMC Palliat. Care 2018, 17, 1–7. [Google Scholar] [CrossRef]
- Hess, S.; Stiel, S.; Hofmann, S.; Klein, C.; Lindena, G.; Ostgathe, C. Trends in specialized palliative care for non-cancer patients in Germany—Data from the National Hospice and Palliative Care Evaluation (HOPE). Eur. J. Intern. Med. 2014, 25, 187–192. [Google Scholar] [CrossRef]
- Gadoud, A.; Kane, E.; Oliver, S.E.; Johnson, M.J.; MacLeod, U.; Allgar, V. Palliative care for non-cancer conditions in primary care: A time trend analysis in the UK (2009–2014). BMJ Support. Palliat. Care 2020. [Google Scholar] [CrossRef]
- Hung, Y.-S.; Lee, S.-H.; Hung, C.-Y.; Wang, C.-H.; Kao, C.-Y.; Wang, H.-M.; Chou, W.-C. Clinical characteristics and survival outcomes of terminally ill patients undergoing withdrawal of mechanical ventilation. J. Formos. Med. Assoc. 2018, 117, 798–805. [Google Scholar] [CrossRef]
- Chang, H.-T.; Lin, M.-H.; Chen, C.-K.; Chen, T.-J.; Hwang, S.-J. Aggressive End-of-Life Care and Symptom Relief Treatments in Terminally Ill Patients Who Had Discussed Withdrawal of Mechanical Ventilation: A Hospital-Based Observational Study. Am. J. Hosp. Palliat. Med. 2020, 37, 897–903. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.Y.; Wu, M.S. Taiwan renal care system: A learning health-care system. Nephrology 2018, 23 (Suppl. 4), 112–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hung, Y.-S.; Chang, H.; Wu, W.-S.; Chen, J.-S.; Chou, W.-C. A Comparison of Cancer and Noncancer Patients Who Receive Palliative Care Consultation Services. Am. J. Hosp. Palliat. Med. 2012, 30, 558–565. [Google Scholar] [CrossRef] [PubMed]
- Fujimoto, K.; Minami, S.; Yamamoto, S.; Ogata, Y.; Koba, T.; Futami, S.; Nishijima, Y.; Yaga, M.; Masuhiro, K.; Komuta, K. Comparison of timing and decision-makers of do-not-resuscitate orders between thoracic cancer and non-cancer respiratory disease patients dying in a Japanese acute care hospital. Support. Care Cancer 2014, 22, 1485–1492. [Google Scholar] [CrossRef] [PubMed]
- Abe, A.; Kobayashi, M.; Kohno, T.; Takeuchi, M.; Hashiguchi, S.; Mimura, M.; Fujisawa, D. Patient participation and associated factors in the discussions on do-not-attempt-resuscitation and end-of-life disclosure: A retrospective chart review study. BMC Palliat. Care 2021, 20, 1–10. [Google Scholar] [CrossRef]
- Kao, C.-Y.; Wang, H.-M.; Tang, S.-C.; Huang, K.-G.; Jaing, T.-H.; Liu, C.-Y.; Liu, K.-H.; Shen, W.-C.; Wu, J.-H.; Hung, Y.-S.; et al. Predictive Factors for Do-Not-Resuscitate Designation Among Terminally Ill Cancer Patients Receiving Care from a Palliative Care Consultation Service. J. Pain Symptom Manag. 2014, 47, 271–282. [Google Scholar] [CrossRef]
- Wang, C.-L.; Lin, C.-Y.; Huang, C.-C.; Lin, C.-S.; Hu, C.-C.; Hwang, S.-F.; Yen, T.-T.; Liou, Y.-S.; Lee, L.-C. Do-not-resuscitate status is correlated with the prescribed use of systemic strong opioid analgesics in patients with terminal cancer: An observational study. Support. Care Cancer 2019, 27, 4507–4513. [Google Scholar] [CrossRef]
- Bandeali, S.; Ordons, A.R.D.; Sinnarajah, A. Comparing the physical, psychological, social, and spiritual needs of patients with non-cancer and cancer diagnoses in a tertiary palliative care setting. Palliat. Support. Care 2020, 18, 513–518. [Google Scholar] [CrossRef]
- Allsop, M.J.; Ziegler, L.E.; Mulvey, M.R.; Russell, S.; Taylor, R.; Bennett, M. Duration and determinants of hospice-based specialist palliative care: A national retrospective cohort study. Palliat. Med. 2018, 32, 1322–1333. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total | 2011 | 2012 | 2013 | 2014 | ||||||||||||||||||||
| Non-Cancer n = 536 | Cancer n = 5223 | p | Non-Cancer n = 2 | Cancer n = 42 | p | Non-Cancer n = 3 | Cancer n = 373 | p | Non-Cancer n = 7 | Cancer n = 469 | p | Non-Cancer n = 15 | Cancer n = 580 | p | |||||||||||
| Gender, n (%) | 0.6805 | 0.2284 | 0.305 | 0.1453 | 0.446 | ||||||||||||||||||||
| Men | 323 | (60) | 3195 | (61) | 2 | (100) | 24 | (57) | 1 | (33) | 232 | (62) | 6 | (86) | 274 | (58) | 7 | (47) | 328 | (57) | |||||
| Women | 213 | (40) | 2028 | (39) | 0 | (0) | 18 | (43) | 2 | (67) | 141 | (38) | 1 | (14) | 195 | (42) | 8 | (53) | 252 | (43) | |||||
| Age, MEDIAN (Q1–Q3) | 74 | (62–85) | 63 | (54–74) | <0.0001 | 53.5 | (49–58) | 64.5 | (54–76) | 0.2364 | 62 | (60–85) | 61 | (53–73) | 0.3845 | 78 | (54–82) | 62 | (53–74) | 0.2409 | 74 | (61–89) | 62 | (53–74) | 0.0046 |
| Duration of PCCS, MEDIAN (Q1–Q3) | 10 | (4–26) | 12 | (4–26) | 0.01 | 14 | (8–20) | 10 | (4–22) | 0.7343 | 16 | (2–42) | 12 | (4–24) | 0.8328 | 6 | (2–8) | 12 | (4–26) | 0.0443 | 20 | (6–26) | 14 | (6–30.5) | 0.7525 |
| DNR declaration, n (%) | <0.0001 | 0.3842 | 0.0231 | ||||||||||||||||||||||
| Not signed | 11 | (2) | 930 | (18) | 0 | (0) | 5 | (12) | 0 | (0) | 59 | (16) | 0 | (0) | 80 | (17) | 0 | (0) | 140 | (24) | |||||
| Signed before PCCS | 444 | (83) | 2507 | (48) | 2 | (100) | 21 | (50) | 2 | (67) | 201 | (54) | 7 | (100) | 224 | (48) | 9 | (60) | 209 | (36) | |||||
| Signed after PCCS | 81 | (15) | 1786 | (34) | 0 | (0) | 16 | (38) | 1 | (33) | 113 | (30) | 0 | (0) | 165 | (35) | 6 | (40) | 231 | (40) | |||||
| Status of PCCS Termination | <0.0001 | 0.0823 | 0.1707 | 0.8755 | 0.2705 | ||||||||||||||||||||
| Discharge | 54 | (10) | 813 | (16) | 0 | (0) | 4 | (10) | 0 | (0) | 36 | (10) | 0 | (0) | 70 | (15) | 1 | (7) | 97 | (17) | |||||
| impending Death discharge | 114 | (21) | 1265 | (24) | 1 | (50) | 12 | (29) | 0 | (0) | 90 | (24) | 2 | (29) | 122 | (26) | 5 | (33) | 160 | (28) | |||||
| Refer to palliative home care | 44 | (8) | 638 | (12) | 0 | (0) | 8 | (19) | 1 | (33) | 59 | (16) | 1 | (14) | 51 | (11) | 0 | (0) | 63 | (11) | |||||
| Refer to palliative care unit | 60 | (11) | 885 | (17) | 0 | (0) | 7 | (17) | 0 | (0) | 92 | (25) | 1 | (14) | 93 | (20) | 1 | (7) | 104 | (18) | |||||
| Refer to ICU | 0 | (0) | 3 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 1 | (0) | 0 | (0) | 1 | (0) | 0 | (0) | 0 | (0) | |||||
| Refer to home care service | 4 | (1) | 9 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 1 | (0) | 0 | (0) | 1 | (0) | 0 | (0) | 0 | (0) | |||||
| Refusal by patient | 0 | (0) | 1 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | |||||
| Refusal by family | 0 | (0) | 5 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | |||||
| Improved condition | 8 | (1) | 71 | (1) | 0 | (0) | 1 | (2) | 1 | (33) | 11 | (3) | 0 | (0) | 15 | (3) | 1 | (7) | 16 | (3) | |||||
| Death | 204 | (38) | 1266 | (24) | 0 | (0) | 9 | (21) | 1 | (33) | 63 | (17) | 3 | (43) | 91 | (19) | 6 | (40) | 117 | (20) | |||||
| Others | 48 | (9) | 267 | (5) | 1 | (50) | 1 | (2) | 0 | (0) | 20 | (5) | 0 | (0) | 25 | (5) | 1 | (7) | 23 | (4) | |||||
| Characteristics | 2015 | 2016 | 2017 | 2018 | 2019 | ||||||||||||||||||||
| Non-Cancer n = 81 | Cancer n = 721 | p | Non-Cancer n = 81 | Cancer n = 692 | p | Non-Cancer n = 130 | Cancer n = 861 | p | Non-Cancer n = 120 | Cancer n = 814 | p | Non-Cancer n = 97 | Cancer n = 671 | p | |||||||||||
| Gender, n (%) | 0.6985 | 0.4363 | 0.5074 | 0.0836 | 0.0623 | ||||||||||||||||||||
| Men | 51 | (63) | 438 | (61) | 53 | (65) | 422 | (61) | 85 | (65) | 537 | (62) | 67 | (56) | 521 | (64) | 51 | (53) | 419 | (62) | |||||
| Women | 30 | (37) | 283 | (39) | 28 | (35) | 270 | (39) | 45 | (35) | 324 | (38) | 53 | (44) | 293 | (36) | 46 | (47) | 252 | (38) | |||||
| Age, MEDIAN (Q1–Q3) | 69 | (58–84) | 64 | (53–75) | 0.0036 | 73 | (62–83) | 63 | (54–74) | 0.0005 | 71.5 | (61–83) | 63 | (53–74) | <0.0001 | 76 | (64–86) | 65 | (56–75) | <0.0001 | 79 | (69–89) | 64 | (56–74) | <0.0001 |
| Duration of PCCS, MEDIAN (Q1–Q3) | 12 | (4–32) | 12 | (4–24) | 0.5987 | 12 | (4–26) | 12 | (4–24) | 0.4452 | 10 | (4–26) | 12 | (5–26) | 0.2717 | 9 | (4–26) | 12 | (5–26) | 0.1174 | 10 | (4–18) | 14 | (6–24) | 0.0275 |
| DNR declaration, n (%) | <0.0001 | <0.0001 | <0.0001 | <0.0001 | <0.0001 | ||||||||||||||||||||
| Not signed | 4 | (5) | 154 | (21) | 3 | (4) | 149 | (22) | 1 | (1) | 138 | (16) | 3 | (3) | 116 | (14) | 0 | (0) | 89 | (13) | |||||
| Signed before PCCS | 57 | (70) | 300 | (42) | 68 | (84) | 322 | (47) | 108 | (83) | 428 | (50) | 101 | (84) | 431 | (53) | 90 | (93) | 371 | (55) | |||||
| Signed after PCCS | 20 | (25) | 267 | (37) | 10 | (12) | 221 | (32) | 21 | (16) | 295 | (34) | 16 | (13) | 267 | (33) | 7 | (7) | 211 | (31) | |||||
| Status of PCCS termination | <0.0001 | 0.3145 | <0.0001 | 0.0001 | 0.0021 | ||||||||||||||||||||
| Discharge | 12 | (15) | 128 | (18) | 9 | (11) | 117 | (17) | 16 | (12) | 137 | (16) | 10 | (8) | 121 | (15) | 6 | (6) | 103 | (15) | |||||
| impending Death discharge | 28 | (35) | 203 | (28) | 22 | (27) | 162 | (23) | 30 | (23) | 213 | (25) | 12 | (10) | 159 | (20) | 14 | (14) | 144 | (21) | |||||
| Refer to palliative home care | 3 | (4) | 87 | (12) | 8 | (10) | 97 | (14) | 4 | (3) | 97 | (11) | 12 | (10) | 90 | (11) | 15 | (15) | 86 | (13) | |||||
| Refer to palliative care unit | 2 | (2) | 105 | (15) | 8 | (10) | 103 | (15) | 10 | (8) | 144 | (17) | 22 | (18) | 137 | (17) | 16 | (16) | 100 | (15) | |||||
| Refer to ICU | 1 | (1) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 1 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | |||||
| Refer to home care service | 0 | (0) | 0 | (0) | 0 | (0) | 3 | (0) | 1 | (1) | 0 | (0) | 2 | (2) | 3 | (0) | 0 | (0) | 1 | (0) | |||||
| Refusal by patient | 0 | (0) | 1 | (0) | 0 | (0) | 1 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | |||||
| Refusal by family | 0 | (0) | 0 | (0) | 0 | (0) | 2 | (0) | 0 | (0) | 1 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 1 | (0) | |||||
| Improved condition | 1 | (1) | 8 | (1) | 0 | (0) | 10 | (1) | 1 | (1) | 10 | (1) | 2 | (2) | 0 | (0) | 2 | (2) | 0 | (0) | |||||
| Death | 27 | (33) | 173 | (24) | 28 | (35) | 165 | (24) | 52 | (40) | 200 | (23) | 49 | (41) | 248 | (30) | 38 | (39) | 200 | (30) | |||||
| Others | 7 | (9) | 16 | (2) | 6 | (7) | 32 | (5) | 16 | (12) | 58 | (7) | 11 | (9) | 56 | (7) | 6 | (6) | 36 | (5) | |||||
| Characteristics | Total | 2011 | 2012 | 2013 | 2014 | ||||||||||
| Non-Cancer | Cancer | p | Non-Cancer | Cancer | p | Non-Cancer | Cancer | p | Non-Cancer | Cancer | p | Non-Cancer | Cancer | p | |
| Patients’ awareness of disease before PCCS | 35.1 | 37.6 | 0.5667 | 100.0 | 61.1 | 0.2671 | 0.0 | 41.3 | 0.1471 | 50.0 | 24.3 | 0.2347 | 11.1 | 21.1 | 0.4643 |
| Families’ awareness of disease before PCCS | 72.2 | 62.7 | <0.0001 | 100.0 | 90.5 | 0.6471 | 66.7 | 56.9 | 0.7337 | 71.4 | 51.6 | 0.2978 | 66.7 | 58.7 | 0.5364 |
| Patients’ awareness of disease after PCCS | 75.5 | 79.8 | 0.1877 | 100.0 | 76.3 | 0.4343 | 100.0 | 82.4 | 0.4239 | 100.0 | 76.2 | 0.2642 | 66.7 | 68.7 | 0.8955 |
| Families’ awareness of disease after PCCS | 99.6 | 99.5 | 0.7773 | 100.0 | 100.0 | - | 100.0 | 100.0 | - | 100.0 | 99.6 | 0.8625 | 100.0 | 99.3 | 0.7463 |
| Characteristics | 2015 | 2016 | 2017 | 2018 | 2019 | ||||||||||
| Non-Cancer | Cancer | p | Non- Cancer | Cancer | p | Non-Cancer | Cancer | p | Non-Cancer | Cancer | p | Non-Cancer | Cancer | p | |
| Patients’ awareness of disease before PCCS | 8.0 | 27.7 | 0.0298 | 29.2 | 36.3 | 0.4762 | 50.0 | 54.2 | 0.7107 | 55.0 | 49.4 | 0.6203 | 45.8 | 43.0 | 0.7809 |
| Families’ awareness of disease before PCCS | 71.8 | 62.9 | 0.1225 | 74.4 | 66.1 | 0.1432 | 64.8 | 68.1 | 0.4626 | 78.3 | 66.3 | 0.0105 | 73.7 | 60.3 | 0.0124 |
| Patients’ awareness of disease after PCCS | 64.3 | 74.2 | 0.2431 | 57.1 | 70.8 | 0.1217 | 86.7 | 91.9 | 0.3072 | 73.1 | 86.2 | 0.0624 | 89.7 | 87.9 | 0.7815 |
| Families’ awareness of disease after PCCS | 100.0 | 99.7 | 0.6365 | 100.0 | 99.3 | 0.4439 | 99.2 | 99.6 | 0.4857 | 99.2 | 99.1 | 0.9798 | 100.0 | 99.8 | 0.7019 |
| Characteristics | Crude | Adjusted | ||||
|---|---|---|---|---|---|---|
| OR | 95%CI | p-Value | OR | 95%CI | p-Value | |
| Age | 0.9930 | (0.99–0.997) | 0.0004 | 0.9920 | (0.987–0.996) | 0.0005 * |
| Gender | ||||||
| Men | - | - | - | - | - | - |
| Women | 1.0820 | (0.966–1.211) | 0.1741 | 1.0630 | (0.93–1.216) | 0.3696 |
| Disease | ||||||
| Non-cancer | - | - | - | - | - | - |
| Cancer | 1.3670 | (1.139–1.641) | 0.0008 | 1.2230 | (0.87–1.719) | 0.2460 |
| DNR declaration | ||||||
| Not signed | - | - | - | - | - | - |
| Signed before PCCS | 0.9010 | (0.772–1.051) | 0.1829 | 1.1600 | (0.946–1.422) | 0.1528 |
| Signed after PCCS | 1.5330 | (1.293–1.817) | <0.0001 | 1.9670 | (1.574–2.458) | <0.0001 * |
| Awareness | ||||||
| Patients’ awareness of disease before PCCS | ||||||
| No | - | - | - | - | - | - |
| Yes | 0.910 | (0.796–1.04) | 0.168 | - | - | - |
| Patients’ awareness of disease after PCCS | ||||||
| No | - | - | - | - | - | - |
| Yes | 0.843 | (0.717–0.991) | 0.039 | 0.754 | (0.635–0.895) | 0.001 * |
| Families’ awareness of disease before PCCS | ||||||
| No | - | - | - | - | - | - |
| Yes | 1.101 | (0.982–1.236) | 0.100 | - | - | - |
| Families’ awareness of disease after PCCS | ||||||
| No | - | - | - | - | - | - |
| Yes | 0.485 | (0.183–1.288) | 0.146 | - | - | - |
| Status of PCCS termination | ||||||
| Discharge | - | - | - | - | - | - |
| Impending death discharge | 0.8210 | (0.684–0.986) | 0.0350 | 0.763 | (0.606–0.962) | 0.022 * |
| Refer to palliative home care | 0.7900 | (0.637–0.978) | 0.0307 | 0.716 | (0.563–0.91) | 0.006 * |
| Refer to palliative care unit | 0.7760 | (0.637–0.945) | 0.0116 | 0.630 | (0.493–0.804) | 0.000 * |
| Refer to ICU | 0.8520 | (0.077–9.437) | 0.8961 | >999.999 | (<0.001–>999.999) | 0.983 |
| Refer to home care service | 2.3430 | (0.516–10.644) | 0.2703 | >999.999 | (<0.001–>999.999) | 0.970 |
| Refusal by patient | >999.999 | (<0.001–>999.999) | 0.9811 | >999.999 | (<0.001–>999.999) | 0.988 |
| Refusal by family | >999.999 | (<0.001–>999.999) | 0.9577 | >999.999 | (<0.001–>999.999) | 0.979 |
| Improved condition | 16.4000 | (3.999–67.263) | 0.0001 | 12.245 | (2.964–50.584) | 0.001 * |
| Death | 0.7760 | (0.648–0.929) | 0.0059 | 0.811 | (0.642–1.026) | 0.081 |
| Others | 1.7040 | (1.247–2.328) | 0.0008 | 1.375 | (0.965–1.959) | 0.078 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, L.-H.; Lin, L.-S.; Wang, C.-L.; Chang, Y.-C.; Lee, L.-C.; Hu, C.-C.; Hsu, P.-S.; Chu, W.-M. Palliative Care Consultation Services on Terminally Ill Cancer Patients and Non-Cancer Patients: Trend Analysis from a 9-Year-Long Observational Study in Taiwan. Int. J. Environ. Res. Public Health 2021, 18, 9882. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18189882
Huang L-H, Lin L-S, Wang C-L, Chang Y-C, Lee L-C, Hu C-C, Hsu P-S, Chu W-M. Palliative Care Consultation Services on Terminally Ill Cancer Patients and Non-Cancer Patients: Trend Analysis from a 9-Year-Long Observational Study in Taiwan. International Journal of Environmental Research and Public Health. 2021; 18(18):9882. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18189882
Chicago/Turabian StyleHuang, Ling-Hui, Lian-Shin Lin, Chun-Li Wang, Yu-Chen Chang, Lung-Chun Lee, Chung-Chieh Hu, Pi-Shan Hsu, and Wei-Min Chu. 2021. "Palliative Care Consultation Services on Terminally Ill Cancer Patients and Non-Cancer Patients: Trend Analysis from a 9-Year-Long Observational Study in Taiwan" International Journal of Environmental Research and Public Health 18, no. 18: 9882. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18189882