
Suicidology Post Graduate Curriculum: Priority Topics and Delivery Mechanisms for Suicide Prevention Education

 , , , and
, , , and 
{kind=link}
Abstract
:1. Introduction
2. Overview
2.1. Review of the Need for Suicide Prevention Education
2.2. Type of Suicide Prevention Education
2.2.1. Gatekeeper Training
2.2.2. Specialized Professional Training
2.2.3. Curriculum-Based Tertiary Education
2.3. Suicidology Tertiary Education in Australia
Tertiary Education: Content and Delivery Modes in a Changing Learning Environment
3. Materials and Methods
3.1. Participants and Recruitment
3.2. Questionnaire
3.3. Analyses
4. Results
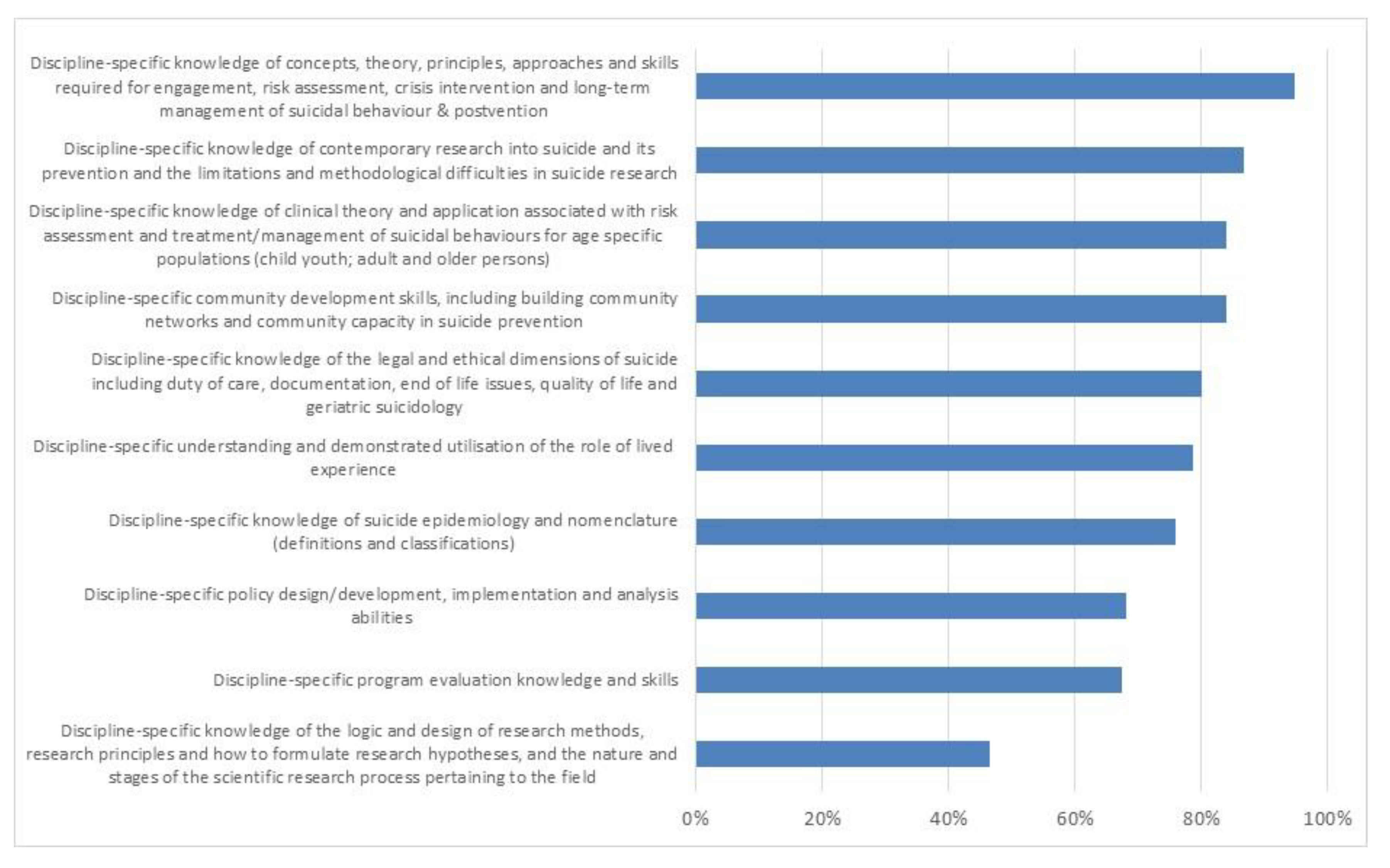
4.1. Importance of Key Learning Domains
4.2. Relevant Qualifications and Preferred Mode of Delivery
4.3. Stakeholder Preference and Willingness to Support Professional Development
5. Discussion
5.1. Limitations
5.2. Implications
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Suicide Worldwide in 2019: Global Health Estimates; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Fitzpatrick, K.M.; Harris, C.; Drawve, G. How bad is it? Suicidality in the middle of the COVID-19 pandemic. Suicide Life Threat. Behav. 2020, 50, 1241–1249. [Google Scholar] [CrossRef]
- Reger, M.A.; Stanley, I.H.; Joiner, T.E. Suicide mortality and coronavirus disease 2019—A perfect storm? JAMA Psychiatry 2020, 77, 1093–1094. [Google Scholar] [CrossRef] [Green Version]
- Pirkis, J.; John, A.; Shin, S.; DelPozo-Banos, M.; Arya, V.; Analuisa-Aguilar, P.; Appleby, L.; Arensman, E.; Bantjes, J.; Baran, A.; et al. Suicide trends in the early months of the COVID-19 pandemic: An interrupted time-series analysis of preliminary data from 21 countries. Lancet Psychiatry 2021, 8, 579–588. [Google Scholar] [CrossRef]
- Gunnell, D.; Appleby, L.; Arensman, E.; Hawton, K.; John, A.; Kapur, N.; Khan, M.; O’Connor, R.C.; Pirkis, J.; Caine, E.D.; et al. Suicide risk and prevention during the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 468–471. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. Causes of Death, Australia, 2019. (Cat. No. 3303.0); Australian Bureau of Statistics, Australian Government: Canberra, Australia, 2020.
- Australian Institute for Health and Welfare. Suicide and Self-harm Monitoring. Intentional Self-Harm Hospitalisations. Available online: https://www.aihw.gov.au/suicide-self-harm-monitoring/data/intentional-self-harm-hospitalisations/intentional-self-harm-hospitalisations-by-states (accessed on 28 July 2021).
- World Health Organization. Preventing Suicide: A Global Imperative; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Platt, S.; Niederkrotenthaler, T. Suicide prevention programs. Crisis 2020, 41, S99–S124. [Google Scholar] [CrossRef] [PubMed]
- Platt, S.; Arensman, E.; Rezaeian, M. National Suicide Prevention Strategies—Progress and Challenges. Crisis 2019, 40, 75–82. [Google Scholar] [CrossRef]
- Council of Australian Governments Health Council. The Fifth National Mental Health and Suicide Prevention Plan; COAG Health Council: Canberra, Australia, 2017.
- Pompili, M.; Baldessarini, R.J.; Berman, A.L.; Lester, D.; Wasserman, D.; De Leo, D.; Girardi, P. Integration of suicidology with general medicine: An obligation to society. Patient Educ. Couns. 2011, 85, 127–128. [Google Scholar] [CrossRef] [PubMed]
- Hawgood, J.L.; Krysinska, K.E.; Ide, N.; De Leo, D. Is suicide prevention properly taught in medical schools? Med. Teach. 2008, 30, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Mughal, F.; Troya, M.I.; Dikomitis, L.; A Chew-Graham, C.; Corp, N.; O Babatunde, O. Role of the GP in the management of patients with self-harm behaviour: A systematic review. Br. J. Gen. Pr. 2020, 70, e364–e373. [Google Scholar] [CrossRef]
- Palmieri, G.; Forghieri, M.; Ferrari, S.; Pingani, L.; Coppola, P.; Colombini, N.; Rigatelli, M.; Neimeyer, R.A. Suicide intervention skills in health professionals: A multidisciplinary comparison. Arch. Suicide Res. 2008, 12, 232–237. [Google Scholar] [CrossRef]
- Puntil, C.; York, J.; Limandri, B.; Greene, P.; Arauz, E.; Hobbs, D. Competency-based training for PMH nurse generalists: Inpatient intervention and prevention of suicide. J. Am. Psychiat. Nurses Assos. 2013, 19, 205–210. [Google Scholar] [CrossRef]
- Schoen, L.E.; Bogetz, A.L.; Hom, M.A.; Bernert, R.A. Suicide risk assessment and management training practices in pediatric residency programs: A nationwide needs assessment survey. J. Adolesc. Health 2019, 65, 280–288. [Google Scholar] [CrossRef]
- Monahan, M.F.; Karver, M.S. Are they ready yet? A theory-driven evaluation of suicide risk assessment trainings in psychology graduate programs. J. Clin. Psychol. 2021, 77, 1614–1628. [Google Scholar] [CrossRef]
- Cramer, R.J.; Johnson, S.M.; McLaughlin, J.; Rausch, E.M.; Conroy, M.A. Suicide risk assessment training for psychology doctoral programs: Core competencies and a framework for training. Train. Educ. Prof. Psychol. 2013, 7, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Cramer, R.; La Guardia, A.C.; Wright-Berryman, J.; Long, M.M.; Tufts, K.A. Integrating interprofessional education into suicide prevention training: Results from a pilot evaluation. Soc. Work Public Health 2019, 34, 628–636. [Google Scholar] [CrossRef] [PubMed]
- Almeida, J.; O’Brien, K.H.M.; Gironda, C.M.; Gross, E.B. Development, implementation, and evaluation of a comprehensive course on suicide in a Master’s of social work program. J. Soc. Work Educ. 2017, 53, 727–736. [Google Scholar] [CrossRef]
- Feldman, B.N.; Freedenthal, S. Social work education in suicide intervention and prevention: An unmet need? Suicide Life Threat. Behav. 2006, 36, 480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kourgiantakis, T.; Sewell, K.M.; McNeil, S.; Lee, E.; Logan, J.; Kuehl, D.; McCormick, M.; Adamson, K.; Kirvan, A. Social work education and training in mental health, addictions, and suicide: A scoping review. J. Soc. Work Educ. 2020, 1–27. [Google Scholar] [CrossRef]
- Scott, M. Teaching note: Understanding of suicide prevention, intervention, and postvention: Curriculum for MSW students. J. Soc. Work Educ. 2015, 51, 185. [Google Scholar] [CrossRef]
- Dexter-Mazza, E.T.; Freeman, K.A. Graduate training and the treatment of suicidal clients: The students’ perspective. Suicide Life Threat. Behav. 2003, 33, 211–218. [Google Scholar] [CrossRef]
- Jahn, D.R.; Drapeau, C.W.; Wacha-Montes, A.; Grant, B.L.; Nadorff, M.R.; Pusateri, M.J., Jr.; Hannah, D.J.; Bryant, G.; Cukrowicz, K.C. Character-istics of and barriers to suicidology training in undergraduate and clinically-oriented graduate-level psychology programs. Suicidol. Online 2017, 8, 74–83. [Google Scholar]
- Wakai, S.; Schilling, E.A.; Aseltine, R.H., Jr.; Blair, E.W.; Bourbeau, J.; Duarte, A.; Durst, L.S.; Graham, P.; Hubbard, N.; Hughey, K.; et al. Suicide prevention skills, confidence and training: Results from the Zero Suicide Workforce Survey of behavioral health care professionals. SAGE Open Med. 2020, 8, 2050312120933152. [Google Scholar] [CrossRef] [PubMed]
- Hawgood, J.; Woodward, A.; Quinnett, P.; De Leo, D. Gatekeeper training and minimum standards of competency. Crisis 2021. [Google Scholar] [CrossRef]
- Osteen, P.J.; Frey, J.J.; Ko, J. Advancing training to identify, intervene, and follow up with individuals at risk for suicide through research. Am. J. Prev. Med. 2014, 47, S216–S221. [Google Scholar] [CrossRef] [PubMed]
- Elston, N.C.; Rogers, J.L.; Gilbride, D.D.; Shannonhouse, L.R. Counselors in training identifying and responding to suicidal clients: A matched-control study. J. Couns. Leadersh. Advocacy 2019, 7, 1–14. [Google Scholar] [CrossRef]
- Isaac, M.; Elias, B.; Katz, L.Y.; Belik, S.-L.; Deane, F.P.; Enns, M.W.; Sareen, J. Gatekeeper training as a preventative intervention for suicide: A systematic review. Can. J. Psychiatry 2009, 54, 260–268. [Google Scholar] [CrossRef] [Green Version]
- Zimitat, C.; De Silva, E.; Bowerman, L. A suicide awareness and intervention program for health professional students. Educ. Health Chang. Learn. Pr. 2015, 28, 201. [Google Scholar] [CrossRef]
- Yonemoto, N.; Kawashima, Y.; Endo, K.; Yamada, M. Gatekeeper training for suicidal behaviors: A systematic review. J. Affect. Disord. 2018, 246, 506–514. [Google Scholar] [CrossRef]
- Holmes, G.; Clacy, A.; Hermens, D.F.; Lagopoulos, J. The long-term efficacy of suicide prevention gatekeeper training: A systematic review. Arch. Suicide Res. 2019, 25, 177–207. [Google Scholar] [CrossRef]
- Holmes, G.; Clacy, A.; Hermens, D.F.; Lagopoulos, J. Evaluating the longitudinal efficacy of SafeTALK suicide prevention gatekeeper training in a general community sample. Suicide Life Threat. Behav. 2021. [Google Scholar] [CrossRef] [PubMed]
- Burnette, C.; Ramchand, R.; Ayer, L. Gatekeeper training for suicide prevention a theoretical model and review of the empirical literature. Rand. Health Q. 2015, 5, 16. [Google Scholar] [PubMed]
- Mann, J.J.; Apter, A.; Bertolote, J.; Beautrais, A.; Currier, D.; Haas, A.; Hegerl, U.; Lonnqvist, J.; Malone, K.; Marusic, A.; et al. Suicide prevention strategies: A systematic review. JAMA 2005, 294, 2064–2074. [Google Scholar] [CrossRef]
- Zalsman, G.; Hawton, K.; Wasserman, D.; van Heeringen, K.; Arensman, E.; Sarchiapone, M.; Carli, V.; Höschl, C.; Barzilay, R.; Balazs, J.; et al. Suicide pre-vention strategies revisited: 10-year systematic review. Lancet Psychiat. 2016, 3, 646–659. [Google Scholar] [CrossRef]
- Cramer, R.J.; Bryson, C.N.; Eichorst, M.K.; Keyes, L.N.; Ridge, B.E. Conceptualization and pilot testing of a core competency-based training workshop in suicide risk assessment and management: Notes from the field. J. Clin. Psychol. 2016, 73, 233–238. [Google Scholar] [CrossRef] [PubMed]
- Cramer, R.J.; Long, M.M. Competency-based suicide prevention education: Implementation of a pilot course for under-graduate health professions students. Acad. Psychiatr. 2018, 42, 857–861. [Google Scholar] [CrossRef] [PubMed]
- Oordt, M.S.; Jobes, D.A.; Fonseca, V.P.; Schmidt, S.M. Training mental health professionals to assess and manage suicidal behavior: Can provider confidence and practice behaviors be altered? Suicide Life Threat. Behav. 2009, 39, 21–32. [Google Scholar] [CrossRef]
- Pisani, A.R.; Cross, W.F.; Watts, A.; Conner, K. Evaluation of the commitment to living (CTL) curriculum. Crisis 2012, 33, 30–38. [Google Scholar] [CrossRef]
- Liebling-Boccio, D.E.; Jennings, H.R. The current status of graduate training in suicide risk assessment. Psychol. Sch. 2012, 50, 72–86. [Google Scholar] [CrossRef]
- Chuop, M.; Michel, Z.; Shah, R.; Chen, J.I.; Black, W. From screening to interventions: Teaching clinical suicide prevention skills to medical students. Acad. Psychiatry 2020, 45, 292–296. [Google Scholar] [CrossRef]
- Mospan, C.M.; Hess, R.; Blackwelder, R.; Grover, S.; Dula, C. A two-year review of suicide ideation assessments among medical, nursing, and pharmacy students. J. Interprof. Care 2017, 31, 537–539. [Google Scholar] [CrossRef]
- Kourgiantakis, T.; Sewell, K.M.; Lee, E.; Adamson, K.; McCormick, M.; Kuehl, D.; Bogo, M. Teaching note-enhancing social work education in mental health, addictions, and suicide risk assessment. J. Soc. Work Educ. 2020, 56, 587–594. [Google Scholar] [CrossRef]
- Muehlenkamp, J.J.; Thoen, S.K. Short- and long-term impact of an undergraduate suicidology course. Suicide Life Threat. Behav. 2019, 49, 1573–1586. [Google Scholar] [CrossRef] [PubMed]
- Yousuf, S.; Beh, S.L.; Wong, P.W. Attitudes towards suicide following an undergraduate suicide prevention module: Expe-rience of medical students in Hong Kong. Hong Kong Med. J. 2013, 19, 377–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Griffith University. Master of Suicidology. Available online: https://www.griffith.edu.au/study/degrees/master-of-suicidology-5666 (accessed on 28 July 2021).
- Griffith University. Graduate Certificate in Suicidology. Available online: https://www.griffith.edu.au/study/degrees/graduate-certificate-in-suicidology-3382 (accessed on 28 July 2021).
- Happell, B.; Waks, S.; Bocking, J.; Horgan, A.; Manning, F.; Greaney, S.; Goodwin, J.; Scholz, B.; van der Vaart, K.J.; Allon, J.; et al. There’s more to a person than what’s in front of you: Nursing students’ experiences of consumer taught mental health education. Int. J. Ment. Health Nur. 2019, 28, 950–959. [Google Scholar] [CrossRef]
- Chang, V. Review and discussion: E-learning for academia and industry. Int. J. Inf. Manag. 2016, 36, 476–485. [Google Scholar] [CrossRef] [Green Version]
- Sun, P.-C.; Tsai, R.J.; Finger, G.; Chen, Y.-Y.; Yeh, D. What drives a successful e-Learning? An empirical investigation of the critical factors influencing learner satisfaction. Comput. Educ. 2008, 50, 1183–1202. [Google Scholar] [CrossRef]
- Lorenza, L.; Carter, D. Emergency online teaching during COVID-19: A case study of Australian tertiary students in teacher education and creative arts. Int. J. Educ. Res. Open 2021, 2-2, 100057. [Google Scholar] [CrossRef]
- Bayer, C.R.; Respress, E.; Willock, R.J.; Heiman, H.J. Curriculum mapping and needs assessment to inform the training of health policy leaders. Ethn. Dis. 2019, 29, 413–420. [Google Scholar] [CrossRef]
- Australian Government. Australian Government Response to Contributing Lives, Thriving—Review of Mental Health Programs and Services; Australian Government: Canberra, Australia, 2015.
- Australian Institute for Health and Welfare. Suicide and Self-harm Monitoring. Deaths by suicide by Remoteness Areas. Available online: https://www.aihw.gov.au/suicide-self-harm-monitoring/data/geography/suicide-by-remoteness-areas (accessed on 28 July 2021).
- National Suicide Prevention Taskforce. Compassion First: Designing our National Approach from the Lived Experience of Suicidal Behaviour; National Suicide Prevention Taskforce: Canberra, Australia, 2020. [Google Scholar]
- Miller, L.G.; McGLOTHLIN, J.M.; West, J.D. Taking the fear out of suicide assessment and intervention: A pedagogical and humanistic practice. J. Humanist. Couns. 2013, 52, 106–121. [Google Scholar] [CrossRef]
- Kang, K.I.; Joung, J. Outcomes of consumer involvement in mental health nursing education: An integrative review. Int. J. Environ. Res. Public Health 2020, 17, 6756. [Google Scholar] [CrossRef]
- Pearce, T.; Maple, M.; Wayland, S.; McKay, K.; Shakeshaft, A. What is the co-creation of new knowledge? A proposed definition. Int. J. Environ. Res. Public Health 2020, 17, 2229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grey, F.; Roper, C.; Cadogan, E. Co-production: Putting Principles into Practice in Mental Health Contexts. 2018. Available online: https://healthsciences.unimelb.edu.au/data/assets/pdf_file/0007/3392215/Coproduction_putting-principles-into-practice.pdf (accessed on 28 July 2021).
- National Collaborating Centre for Mental Health. Self-Harm and Suicide Prevention Competence Framework: Community and Public Health; NHS Health: London, UK, 2018. [Google Scholar]
- Gryglewicz, K.; Monahan, M.F.; Chen, J.I.; Bozzay, M.; Bender, A.; Gleason, L.L.; Witmeier, M.; Karver, M.S. Examining the effects of role play practice in enhancing clinical skills to assess and manage suicide risk. J. Ment. Health 2019, 29, 549–557. [Google Scholar] [CrossRef] [PubMed]
- Millar, S.L.; Chambers, M.; Giles, M. Service user involvement in mental health care: An evolutionary concept analysis. Health Expect. 2015, 19, 209–221. [Google Scholar] [CrossRef] [Green Version]
- Berman, A.L.; Silverman, M.M.; De Leo, D.; Reidenberg, D. Defining suicidology and the titling of suicidologist? Crisis 2021, 42, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Shneidman, E.S.; Swenson, D.D. Bulletin of Suicidology; U.S. Government Printing Office: Washington, DC, USA, 1967.
- Bernert, R.A.; Hom, M.A.; Roberts, L.W. A Review of multidisciplinary clinical practice guidelines in suicide prevention: Toward an emerging standard in suicide risk assessment and management, training and practice. Acad. Psychiatry 2014, 38, 585–592. [Google Scholar] [CrossRef]
- Graves, J.M.; Mackelprang, J.L.; Van Natta, S.E.; Holliday, C. Suicide prevention training: Policies for health care profes-sionals across the United States as of October 2017. Am. J. Public Health 2018, 108, 760–768. [Google Scholar] [CrossRef]
- OECD. Tackling the Mental Health Impact of the COVID-19 Crisis: An Integrated, Whole-of-Society Response. OECD, 2021. Available online: https://www.oecd.org/coronavirus/policy-responses/tackling-the-mental-health-impact-of-the-covid-19-crisis-an-integrated-whole-of-society-response-0ccafa0b/ (accessed on 13 September 2021).

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hawgood, J.; Krysinska, K.; Mooney, M.; Ozols, I.; Andriessen, K.; Betterridge, C.; De Leo, D.; Kõlves, K. Suicidology Post Graduate Curriculum: Priority Topics and Delivery Mechanisms for Suicide Prevention Education. Int. J. Environ. Res. Public Health 2021, 18, 9926. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18189926
Hawgood J, Krysinska K, Mooney M, Ozols I, Andriessen K, Betterridge C, De Leo D, Kõlves K. Suicidology Post Graduate Curriculum: Priority Topics and Delivery Mechanisms for Suicide Prevention Education. International Journal of Environmental Research and Public Health. 2021; 18(18):9926. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18189926
Chicago/Turabian StyleHawgood, Jacinta, Karolina Krysinska, Maddeline Mooney, Ingrid Ozols, Karl Andriessen, Carmen Betterridge, Diego De Leo, and Kairi Kõlves. 2021. "Suicidology Post Graduate Curriculum: Priority Topics and Delivery Mechanisms for Suicide Prevention Education" International Journal of Environmental Research and Public Health 18, no. 18: 9926. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18189926