
Health-Related Quality of Life (HRQoL) Outcomes Following Injury in Childhood and Adolescence Using EuroQol (EQ-5D) Responses with Pooled Longitudinal Data

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials
Patient Cohorts
- The Victorian State Trauma Registry (VSTR) is a population-based trauma registry that captures data about all major trauma patients in the state of Victoria in Australia [9];
- The Victorian Orthopedic Trauma Outcomes Registry (VOTOR) is a clinical registry of orthopedic injuries, treatment, complications and outcomes based on admissions to four Australian centres [10].
- The US Children’s Health After Injury (CHAI) study included children with mild, moderate and severe traumatic brain injury (TBI) or with upper extremity injuries who presented to a set of US hospitals [11].
- The United Kingdom Burden of Injury (UKBOI) was a study of injured individuals with children recruited from emergency department (ED) presentations and hospital admissions in four UK centers [12].
- The British Columbia Children’s Hospital Longitudinal Injury Outcomes (BCCH-LIO) study included children who attended the British Columbia Children’s Hospital in Canada for an injury [13].
3. Methods
3.1. Measures
3.1.1. Demographic and Injury Characteristics
3.1.2. EQ-5D
3.1.3. Time Points
3.2. Statistical Analysis
3.3. Ethics
4. Results
4.1. Pooled Cohort Overview
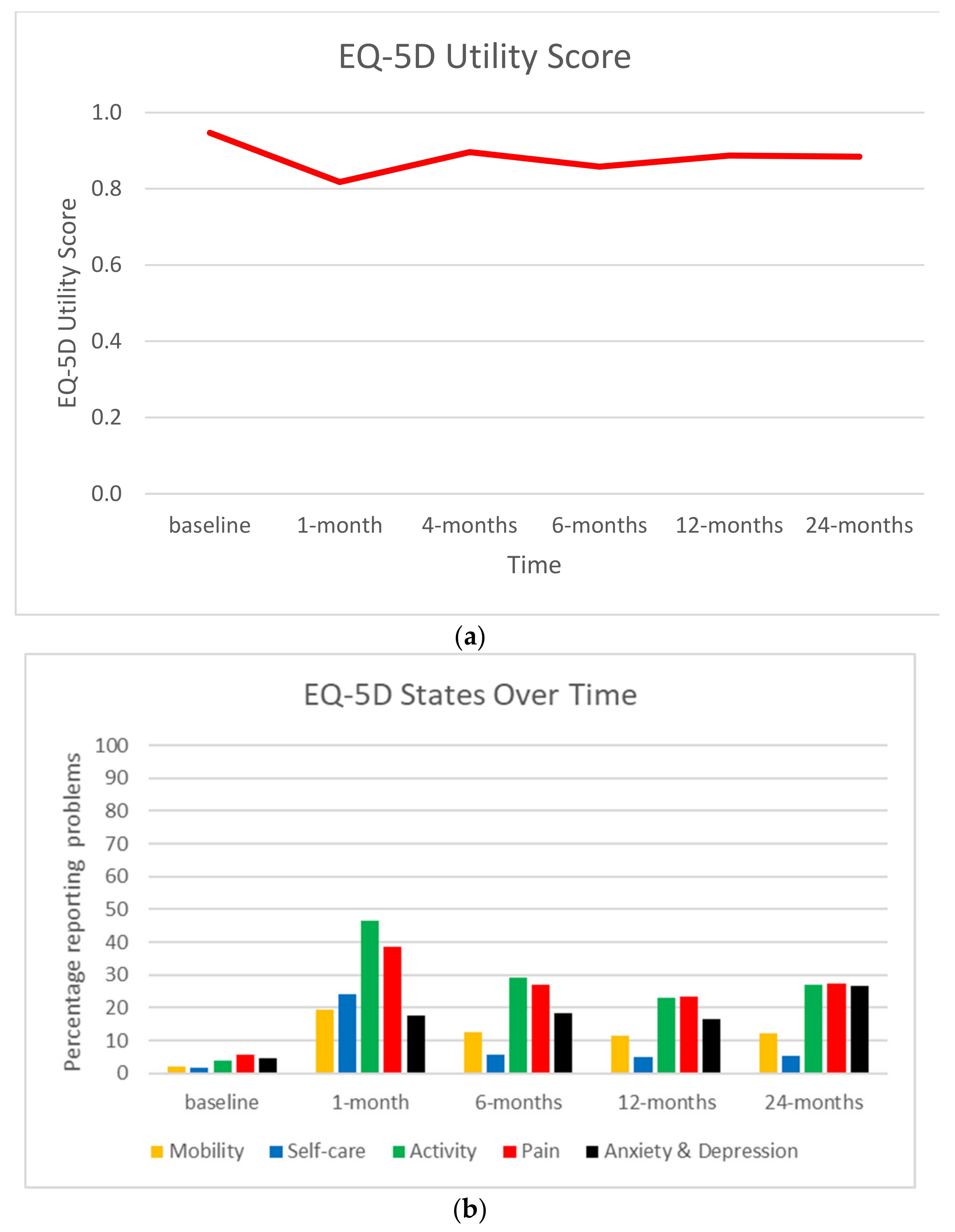
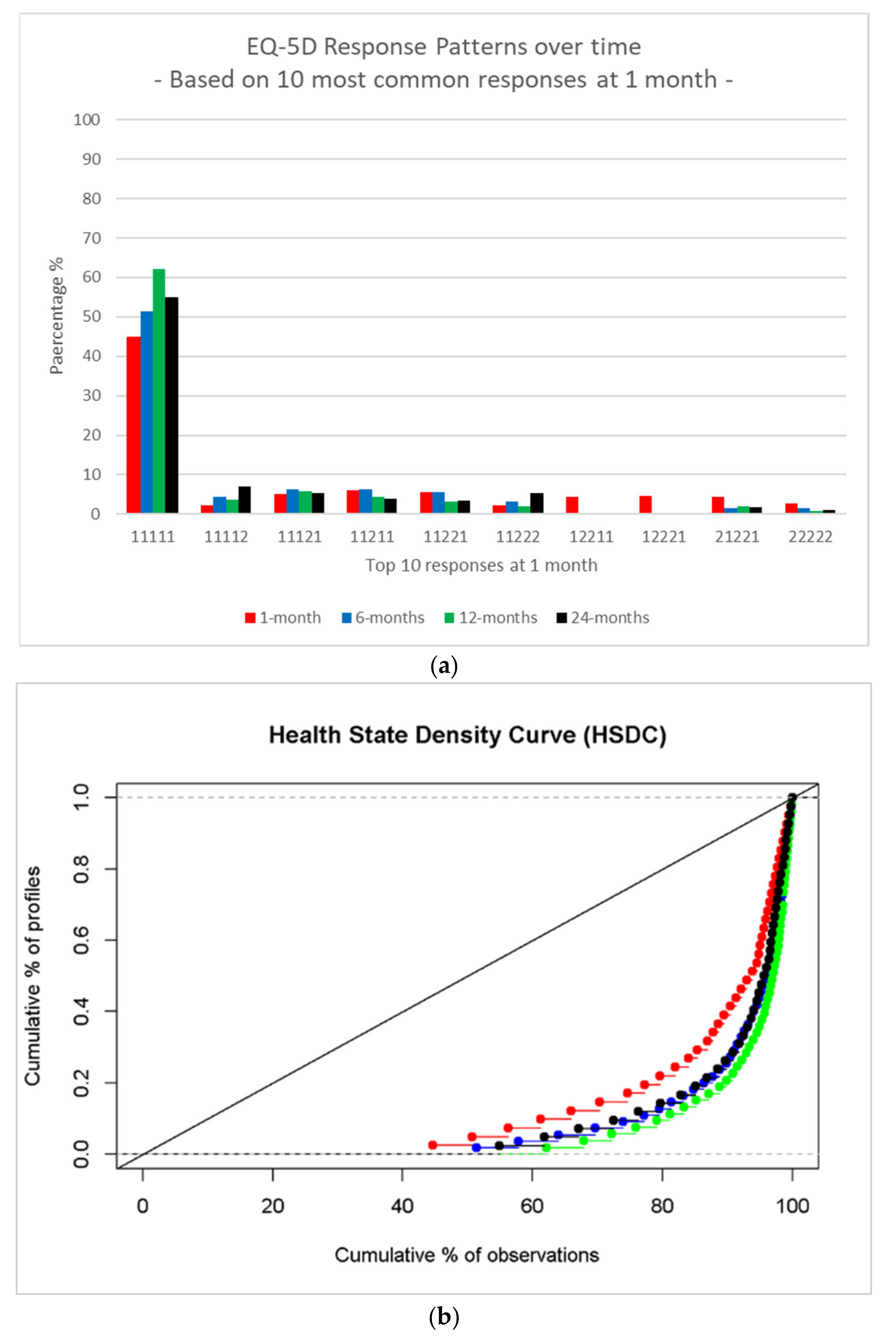
4.2. EQ-5D
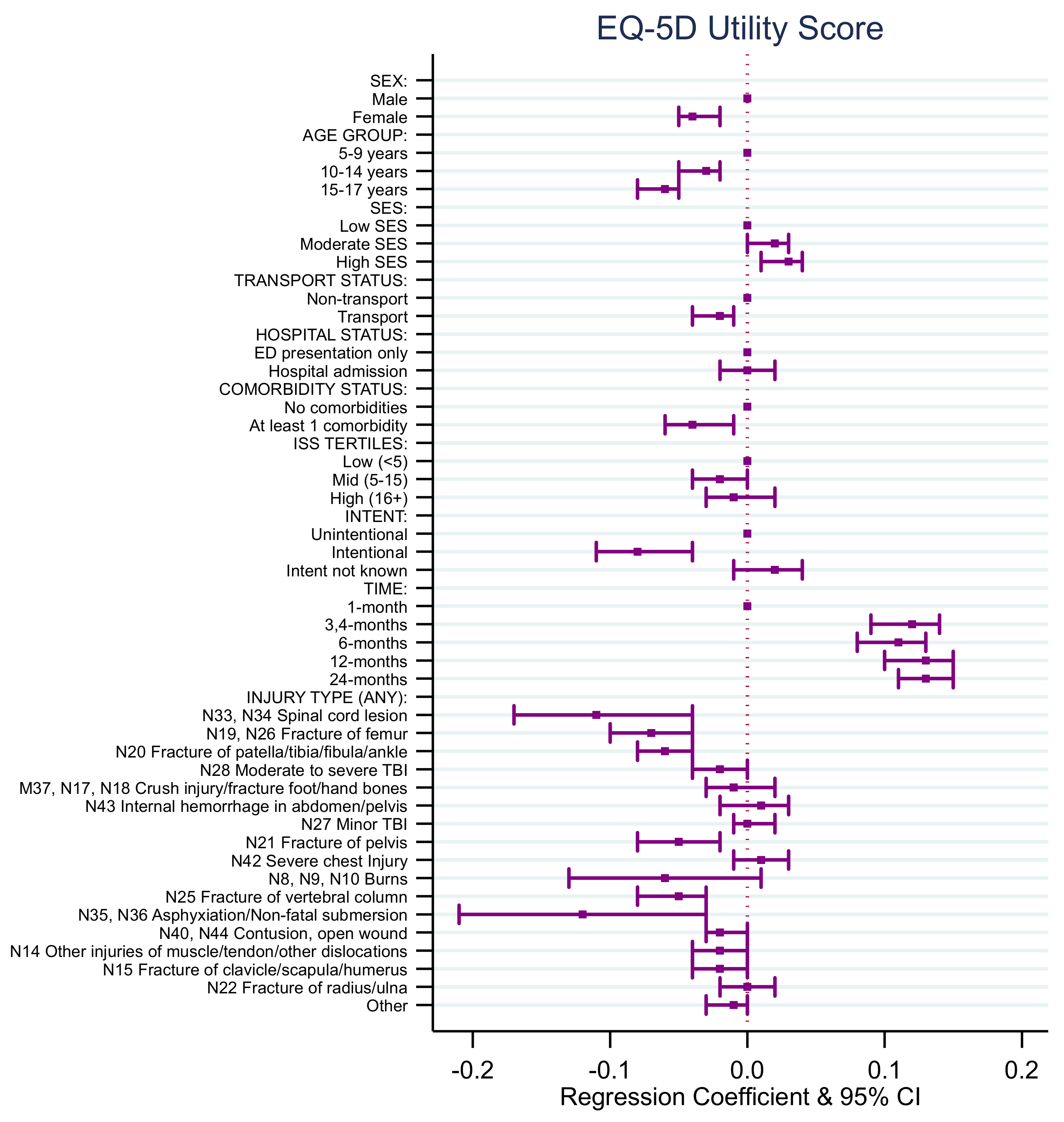
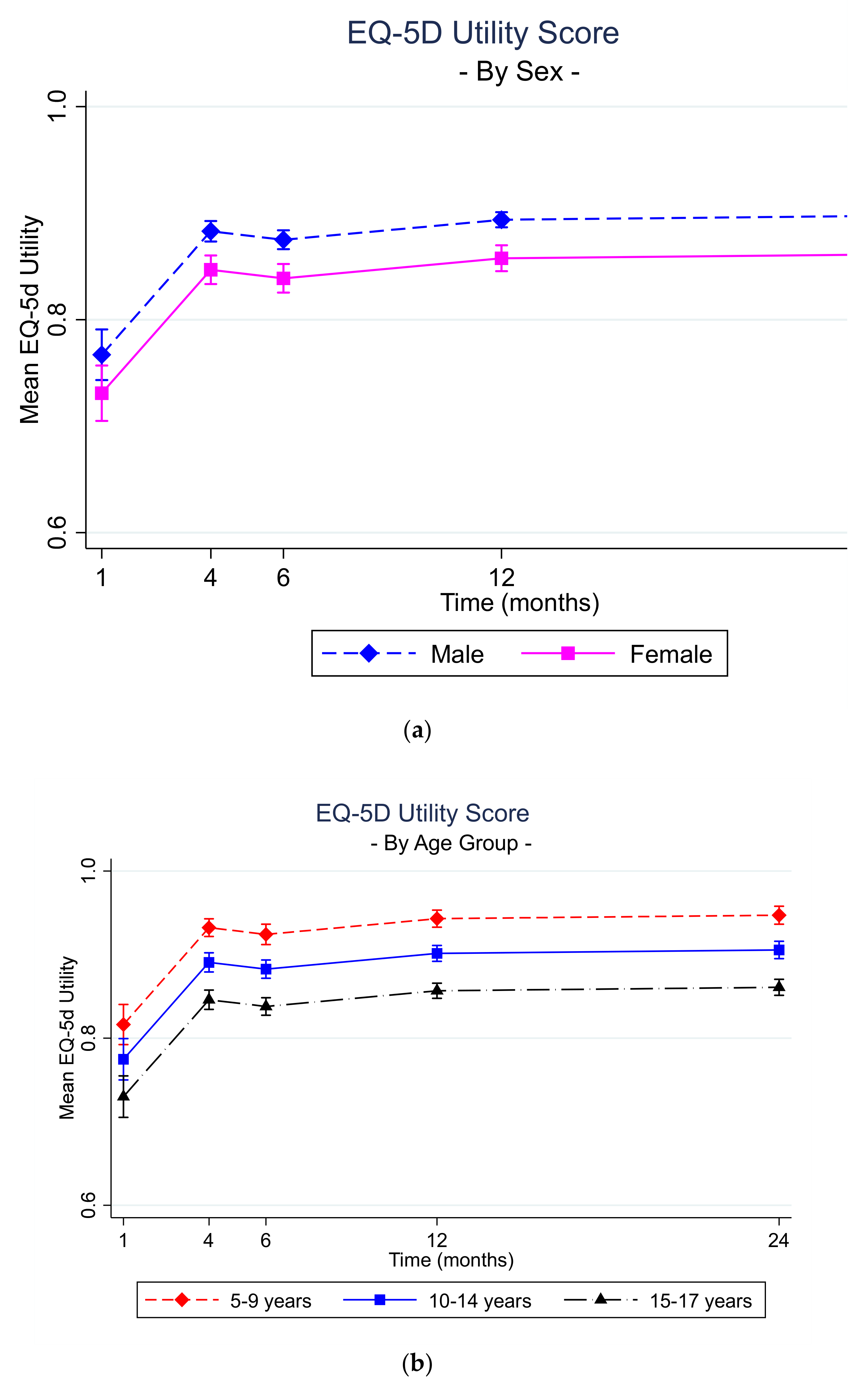
4.3. EQ-5D Utility Score Model
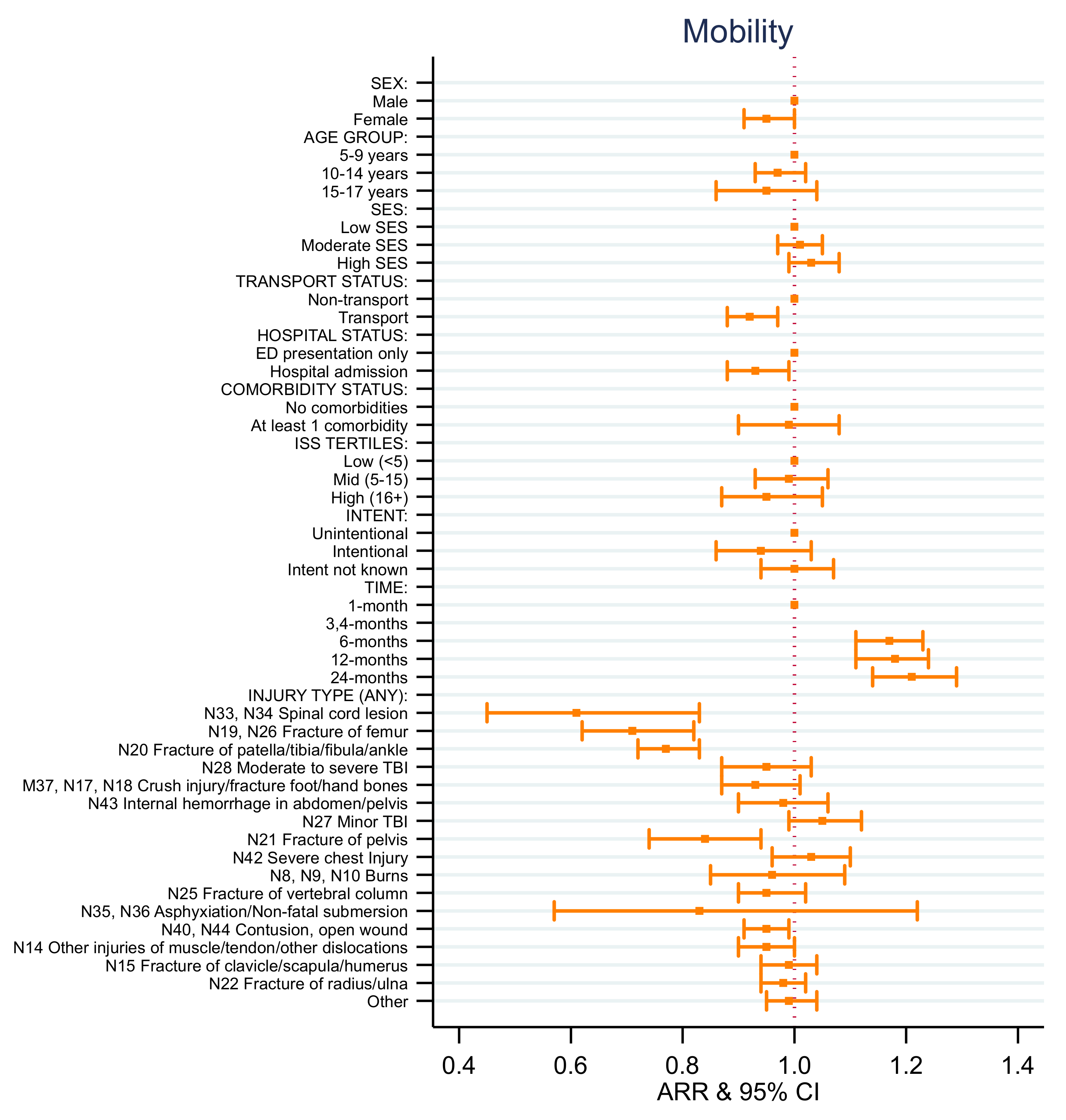
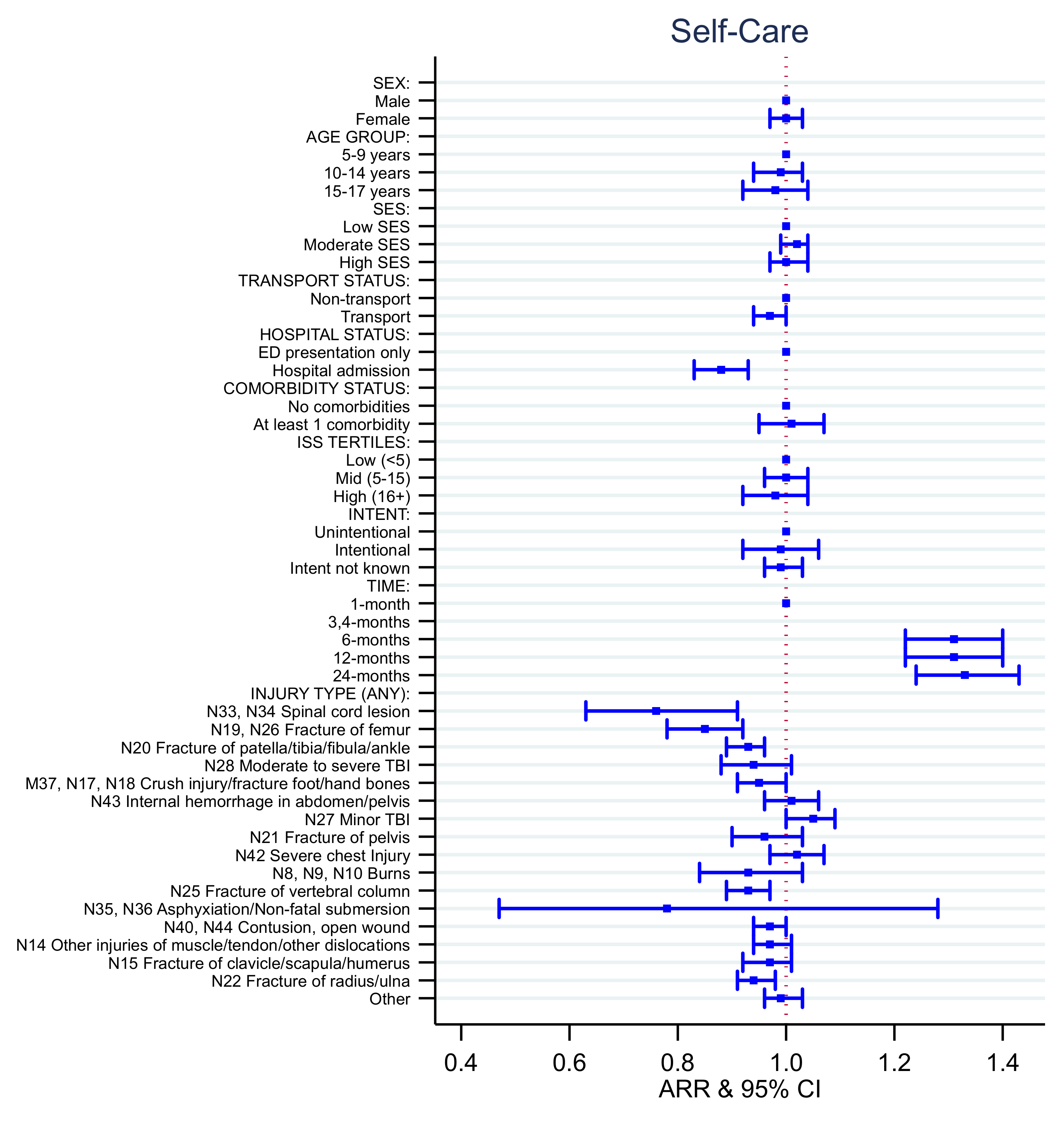
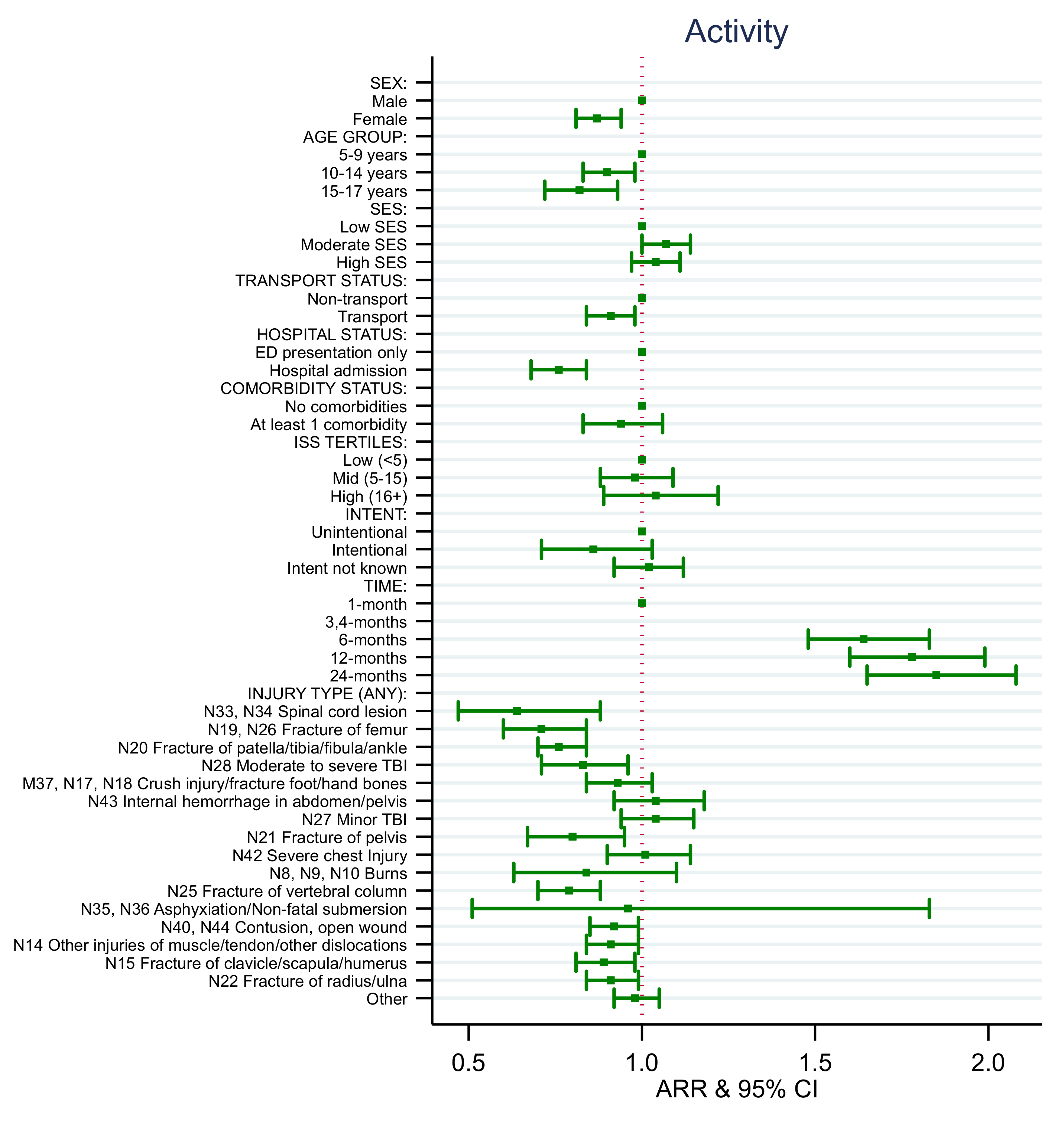
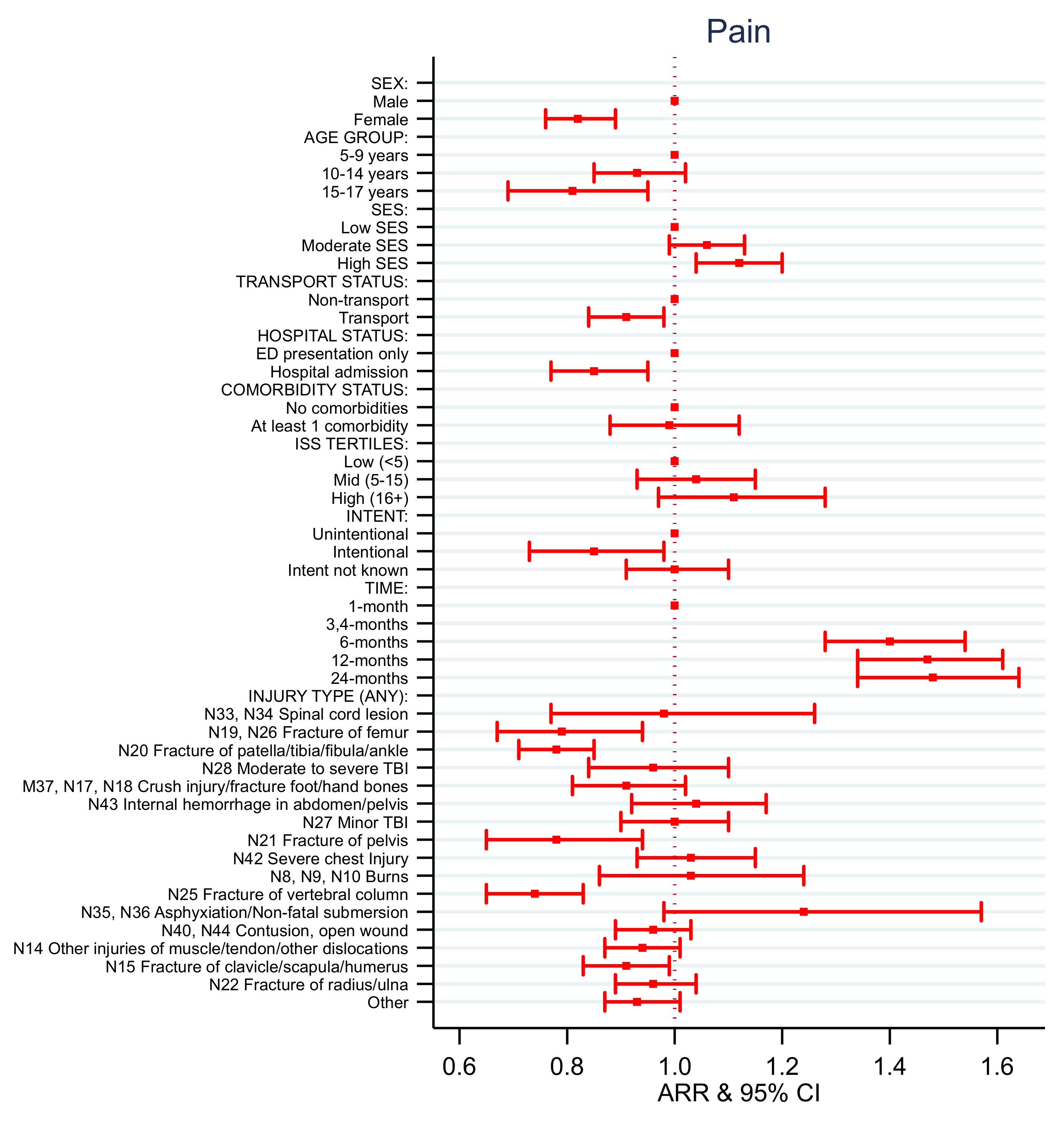
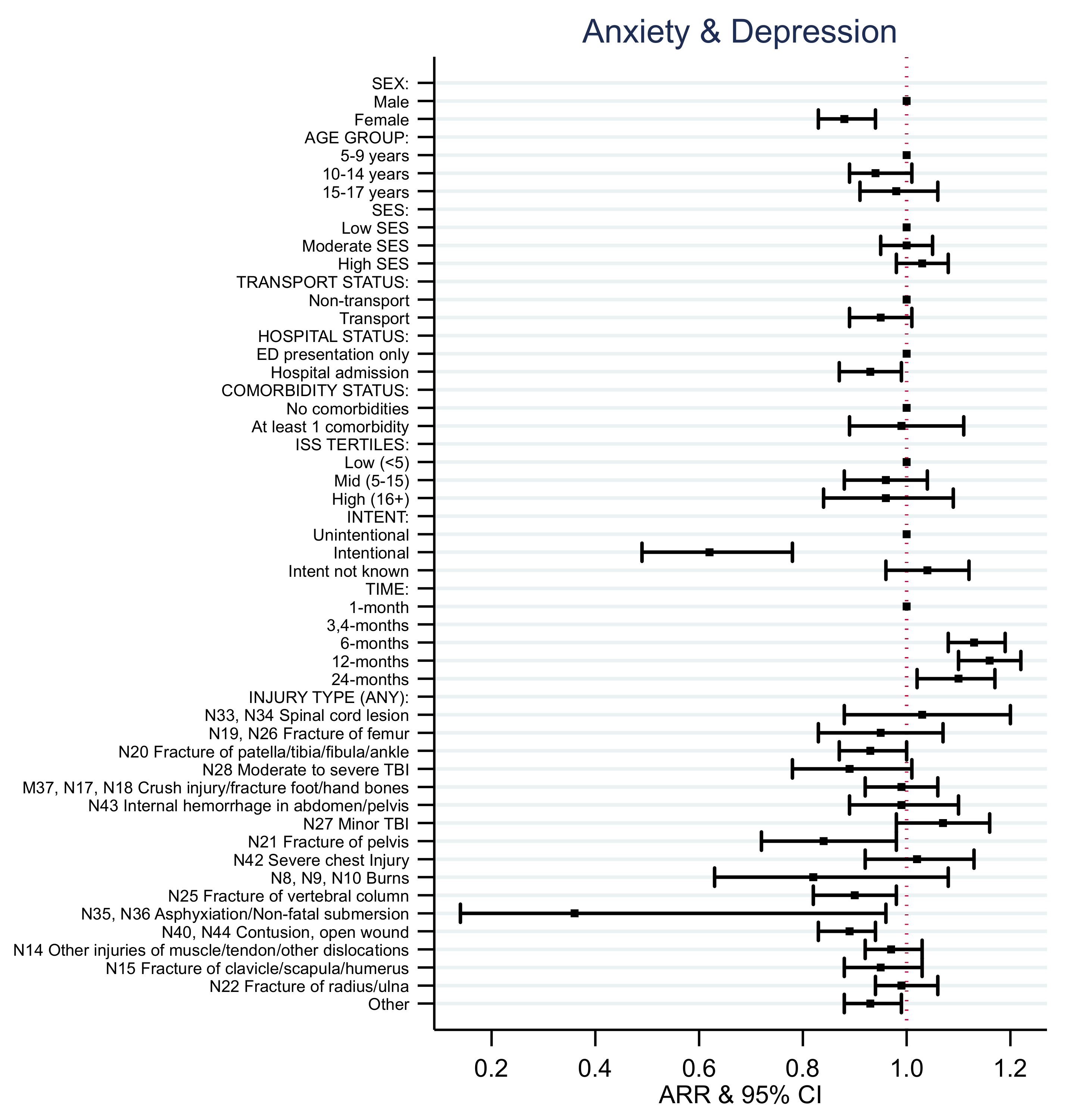
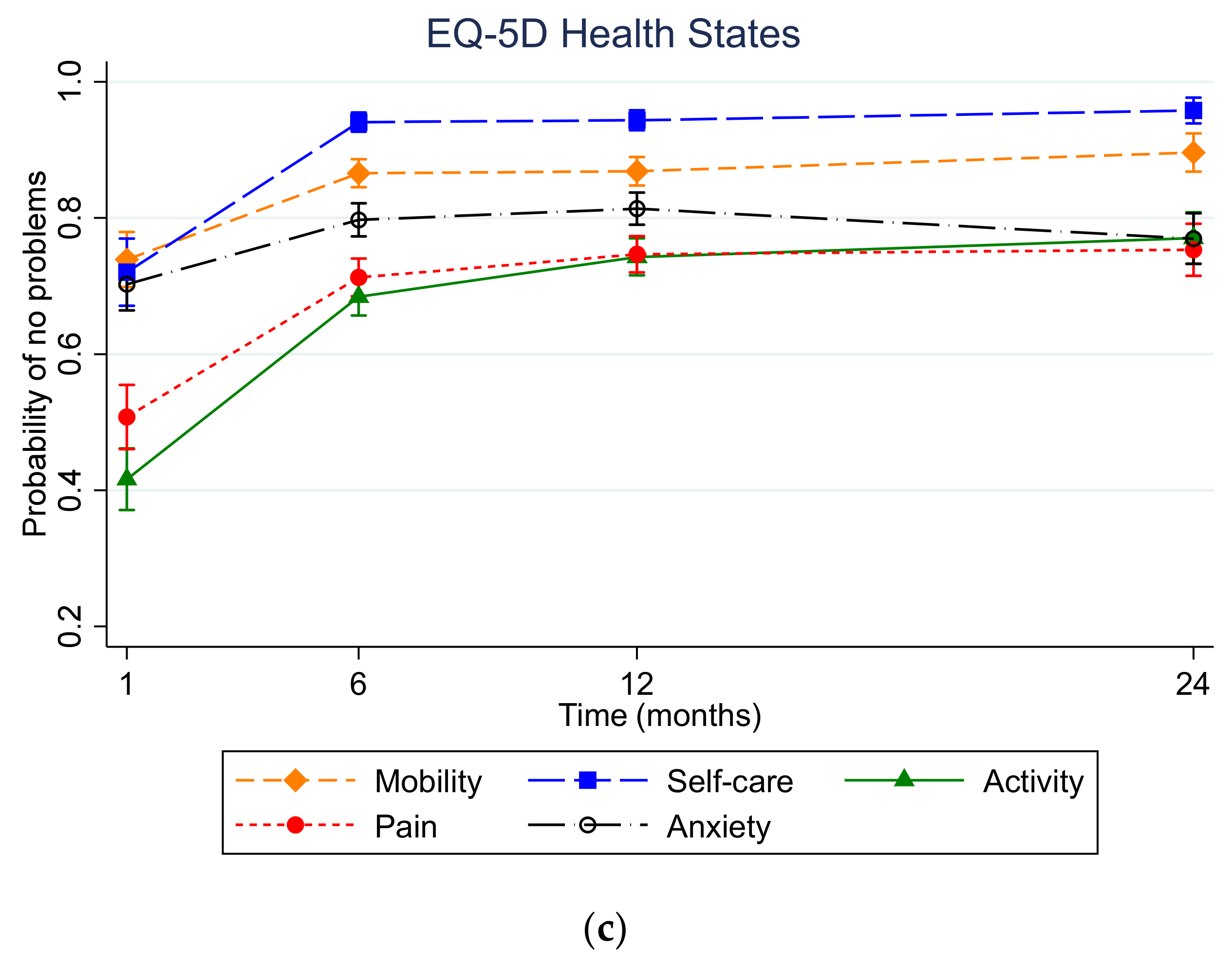
4.4. EQ-5D Health State Models
4.5. HRQoL Trajectories
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Harvey, A.; Towner, E.; Peden, M.; Soori, H.; Bartolomeos, K. Injury prevention and the attainment of child and adolescent health. Bull. World Health Organ. 2009, 87, 390–394. [Google Scholar] [CrossRef]
- Peden, M.; Oyegbite, K.; Ozanne-Smith, J.; Hyder, A.A.; Branche, C.; Rahman, A.; Rivara, F.; Bartolomeos, K. World Report on Child Injury Prevention; World Health Organization: Geneva, Switzerland, 2009; Volume 2008. [Google Scholar]
- Rabin, R.; Charro, F.D. EQ-SD: A measure of health status from the EuroQol Group. Ann. Med. 2001, 33, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Gabbe, B.J.; Simpson, P.M.; Cameron, P.A.; Ponsford, J.; Lyons, R.A.; Collie, A.; Fitzgerald, M.; Judson, R.; Teague, W.J.; Braaf, S. Long-term health status and trajectories of seriously injured patients: A population-based longitudinal study. PLoS Med. 2017, 14, e1002322. [Google Scholar] [CrossRef] [PubMed]
- Chevalier, Z.; Kennedy, P.; Sherlock, O. Spinal cord injury, coping and psychological adjustment: A literature review. Spinal Cord 2009, 47, 778–782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devlin, N.; Parkin, D.; Janssen, B. An Introduction to EQ-5D Instruments and Their Applications. In Methods for Analysing and Reporting EQ-5D Data; Springer: Berlin/Heidelberg, Germany, 2020; pp. 1–22. [Google Scholar]
- Brussoni, M.; Kruse, S.; Walker, K. Validity and reliability of the EQ-5D-3L™ among a paediatric injury population. Health Qual. Life Outcomes 2013, 11, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabbe, B.J.; Dipnall, J.F.; Lynch, J.W.; Rivara, F.P.; Lyons, R.A.; Ameratunga, S.; Brussoni, M.; Lecky, F.E.; Bradley, C.; Simpson, P.M. Validating injury burden estimates using population birth cohorts and longitudinal cohort studies of injury outcomes: The VIBES-Junior study protocol. BMJ Open 2018, 8, e024755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cameron, P.A.; Finch, C.F.; Gabbe, B.J.; Collins, L.J.; Smith, K.L.; McNeil, J.J. Developing Australia’s first statewide trauma registry: What are the lessons? ANZ J. Surg. 2004, 74, 424–428. [Google Scholar] [CrossRef] [PubMed]
- Edwards, E.; Graves, S.; McNeil, J.; Williamson, O.; Urquhart, D.; Cicuttini, F.; Victorian Orthopaedic Trauma Outcomes Registry Project (V.O.T.O.R.P.) Group. Orthopaedic Trauma: Establishment of an Outcomes Registry to Evaluate and Monitor Treatment Effectiveness; Elsevier: Amsterdam, The Netherlands, 2006. [Google Scholar]
- Koepsell, T.D.; Rivara, F.P.; Vavilala, M.S.; Wang, J.; Temkin, N.; Jaffe, K.M.; Durbin, D.R. Incidence and descriptive epidemiologic features of traumatic brain injury in King County, Washington. Pediatrics 2011, 128, 946–954. [Google Scholar] [CrossRef]
- Lyons, R.A.; Kendrick, D.; Towner, E.; Christie, N.; Phillips, C.; Coupland, C.; Hayes, M.; Macey, S.; Brophy, S.; Carter, B. The UK burden of injuries study (UKBOI). Inj. Prev. 2010, 16, A242–A243. [Google Scholar] [CrossRef]
- Schneeberg, A.; Ishikawa, T.; Kruse, S.; Zallen, E.; Mitton, C.; Bettinger, J.A.; Brussoni, M. A longitudinal study on quality of life after injury in children. Health Qual. Life Outcomes 2016, 14, 120. [Google Scholar] [CrossRef] [Green Version]
- Dipnall, J.F.; Berk, M.; Jacka, F.N.; Williams, L.J.; Dodd, S.; Pasco, J.A. Data Integration Protocol in Ten-steps (DIPIT): A new standard for medical researchers. Methods 2014, 69, 237–246. [Google Scholar] [CrossRef]
- Palmer, C. Major trauma and the injury severity score-where should we set the bar? In Proceedings of the Annual Proceedings/Association for the Advancement of Automotive Medicine, Melbourne, Australia, 15–17 October 2007; pp. 13–29. [Google Scholar]
- Huang, Y.-T.; Huang, Y.-H.; Hsieh, C.-H.; Li, C.-J.; Chiu, I.-M. Comparison of Injury Severity Score, Glasgow Coma Scale, and Revised Trauma Score in predicting the mortality and prolonged ICU stay of traumatic young children: A cross-sectional retrospective study. Emerg. Med. Int. 2019, 2019, 5453624. [Google Scholar] [CrossRef] [Green Version]
- Mitchell, R.J.; Curtis, K.; Braithwaite, J. Health outcomes and costs for injured young people hospitalised with and without chronic health conditions. Injury 2017, 48, 1776–1783. [Google Scholar] [CrossRef]
- Khan, K.A.; Petrou, S.; Rivero-Arias, O.; Walters, S.J.; Boyle, S.E. Mapping EQ-5D utility scores from the PedsQL™ generic core scales. Pharmacoeconomics 2014, 32, 693–706. [Google Scholar] [CrossRef]
- Janssen, M.; Szende, A.; Cabases, J.; Ramos-Goñi, J.M.; Vilagut, G.; König, H.-H. Population norms for the EQ-5D-3L: A cross-country analysis of population surveys for 20 countries. Eur. J. Health Econ. 2019, 20, 205–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Devlin, N.; Parkin, D.; Janssen, B. Methods for Analysing and Reporting EQ-5D Data; Springer Nature: Basingstoke, UK, 2020. [Google Scholar]
- Zamora, B.; Parkin, D.; Feng, Y.; Bateman, A.; Herdman, M.; Devlin, N. New Methods for Analysing the Distribution of EQ-5D Observations, OHE Research Paper. March 2018. Available online: www.ohe.org/publications/new-methods-analysing-distribution-eq-5d-observations, (accessed on 23 June 2021).
- Twisk, J.W. Applied Mixed Model Analysis: A Practical Guide; Cambridge University Press: Cambridge, UK, 2019. [Google Scholar]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics, 6th ed.; Pearson: Boston, MA, USA, 2013. [Google Scholar]
- Newman, D.A. Missing data: Five practical guidelines. Organ. Res. Methods 2014, 17, 372–411. [Google Scholar] [CrossRef]
- Twisk, J.; de Boer, M.; de Vente, W.; Heymans, M. Multiple imputation of missing values was not necessary before performing a longitudinal mixed-model analysis. J. Clin. Epidemiol. 2013, 66, 1022–1028. [Google Scholar] [CrossRef] [PubMed]
- Zou, G. A modified poisson regression approach to prospective studies with binary data. Am. J. Epidemiol. 2004, 159, 702–706. [Google Scholar] [CrossRef] [PubMed]
- NHMRC. National Statement on Ethical Conduct in Human Research (2007)—Updated 2018; Canberra NHMRC: Canberra, Australia, 2018.
- Ryder, C.; Mackean, T.; Hunter, K.; Williams, H.; Clapham, K.; Holland, A.J.; Ivers, R. Equity in functional and health related quality of life outcomes following injury in children—A systematic review. Crit. Public Health 2020, 30, 352–366. [Google Scholar] [CrossRef] [Green Version]
- Ameratunga, S.; Ramke, J.; Jackson, N.; Tin Tin, S.; Gabbe, B. Disparities in non-fatal health outcomes in pediatric general trauma studies. Int. J. Environ. Res. Public Health 2018, 15, 43. [Google Scholar] [CrossRef] [Green Version]
- Weyers, S.; Dragano, N.; Möbus, S.; Beck, E.-M.; Stang, A.; Möhlenkamp, S.; Jöckel, K.H.; Erbel, R.; Siegrist, J. Poor social relations and adverse health behaviour: Stronger associations in low socioeconomic groups? Int. J. Public Health 2010, 55, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Senn, T.E.; Walsh, J.L.; Carey, M.P. The mediating roles of perceived stress and health behaviors in the relation between objective, subjective, and neighborhood socioeconomic status and perceived health. Ann. Behav. Med. 2014, 48, 215–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newacheck, P.W.; Hung, Y.Y.; Jane Park, M.; Brindis, C.D.; Irwin, C.E., Jr. Disparities in adolescent health and health care: Does socioeconomic status matter? Health Serv. Res. 2003, 38, 1235–1252. [Google Scholar] [CrossRef] [Green Version]
- Blackwell, D.L.; Martinez, M.E.; Gentleman, J.F.; Sanmartin, C.; Berthelot, J.-M. Socioeconomic status and utilization of health care services in Canada and the United States: Findings from a binational health survey. Med. Care 2009, 47, 1136–1146. [Google Scholar] [CrossRef] [PubMed]
- Zwingmann, J.; Lefering, R.; Maier, D.; Hohloch, L.; Eberbach, H.; Neumann, M.; Strohm, P.C.; Südkamp, N.P.; Hammer, T. Pelvic fractures in severely injured children: Results from the TraumaRegister DGU. Medicine 2018, 97, e11955. [Google Scholar] [CrossRef]
- Vogel, L.C.; Hickey, K.J.; Klaas, S.J.; Anderson, C.J. Unique issues in pediatric spinal cord injury. Orthop. Nurs. 2004, 23, 300–308. [Google Scholar] [CrossRef] [PubMed]
- Albert, P.R. Why is depression more prevalent in women? J. Psychiatry Neurosci. JPN 2015, 40, 219. [Google Scholar] [CrossRef]
- O’Donnell, M.L.; Creamer, M.; Pattison, P.; Atkin, C. Psychiatric morbidity following injury. Am. J. Psychiatry 2004, 161, 507–514. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study & Setting | Month/Year & Participants | Inclusion Criteria & Injury Diagnosis Coding | Post-Injury Follow-Up Time Point EQ-5D Measures & Mode of Interview |
|---|---|---|---|
| VSTR Australia | 03/2009 to 03/2017 n = 824, 5–16 years | In hospital death, ISS > 12, ICU admission or urgent surgery, met burns criteria 20–29% full/partial thickness. ICD-10-AM | EQ-5D total score and items at 6, 12 and 24 months. Telephone |
| VOTOR Australia | 03/2009 to 03/2017 n = 502, 16–17 years | 16+ years of age, orthopedic injury admission >24 h or death ICD-10-AM | EQ-5D total score and items at 6, 12 and 24 months. Telephone |
| CHAI United States of America | 03/2007 to 09/2008 n = 635, 5–17 years | Presentation to ED or hospital admission for either a TBI or an upper extremity injury ICD-9 mapped to ICD-10 | PedsQL scores mapped to EQ-5D total score at 3, 12, and 24 months. Online, telephone and postal |
| UKBOI United Kingdom | 09/2005 to 04/2007 n = 174, 5–17 years | Presentation to ED or hospital admission. ICD-10 | EQ-5D total score and items at 1, 6 and 12 months. Postal |
| BCCH-LIO Canada | 02/2011 to 12/2013 n = 199, 5–16 years | Presentation to ED or hospital admission. ICD-10 | EQ-5D total score and items at 1, 4, and 12 months. Postal and online |
| Lost to Follow Up (n = 400) | Included (n = 2334) | Total (n = 2734) | p-Value † | |
|---|---|---|---|---|
| Sex | 0.162 | |||
| Male | 279 (69.8%) | 1710 (73.3%) | 1989 (72.8%) | |
| Female | 121 (30.2%) | 624 (26.7%) | 745 (27.2%) | |
| Age Group | <0.001 | |||
| 5–9 years | 190 (47.5%) | 371 (15.9%) | 561 (20.5%) | |
| 10–14 years | 82 (20.5%) | 728 (31.2%) | 810 (29.6%) | |
| 15–17 years | 128 (32.0%) | 1235 (52.9%) | 1363 (49.9%) | |
| Age (years) (mean, SD) | 10.8 (4.4) | 13.6 (3.5) | 13.1 (3.8) | |
| Socio Economic Status (SES) Tertile | 0.608 | |||
| Low SES | 155 (39.9%) | 842 (37.8%) | 997 (38.1%) | |
| Moderate SES | 151 (38.9%) | 926 (41.5%) | 1077 (41.2%) | |
| High SES | 82 (21.1%) | 461 (20.7%) | 543 (20.7%) | |
| Cohort | <0.001 | |||
| VSTR | 270 (67.5%) | 824 (35.3%) | 1094 (40.0%) | |
| VOTOR | 49 (12.2%) | 502 (21.5%) | 551 (20.2%) | |
| CHAI | 12 (3.0%) | 635 (27.2%) | 647 (23.7%) | |
| UKBOI | 7 (1.8%) | 174 (7.5%) | 181 (6.6%) | |
| BCCH-LIO | 62 (15.5%) | 199 (8.5%) | 261 (9.5%) | |
| Transport Status | 0.136 | |||
| Non-transport | 226 (58.9%) | 1438 (63.0%) | 1664 (62.4%) | |
| Transport | 158 (41.1%) | 845 (37.0%) | 1003 (37.6%) | |
| Hospital Status | <0.001 | |||
| ED only | 50 (12.5%) | 641 (27.5%) | 691 (25.3%) | |
| Hospital admission | 350 (87.5%) | 1691 (72.5%) | 2041 (74.7%) | |
| Comorbidity status | <0.001 | |||
| No comorbidities | 340 (85.0%) | 2140 (91.7%) | 2480 (90.7%) | |
| At least 1 comorbidity | 60 (15.0%) | 194 (8.3%) | 254 (9.3%) | |
| ISS Tertile | <0.001 | |||
| Low (<5) | 92 (23.4%) | 1035 (45.4%) | 1127 (42.1%) | |
| Mid (5–15) | 119 (30.2%) | 620 (27.2%) | 739 (27.6%) | |
| High (16+) | 183 (46.4%) | 625 (27.4%) | 808 (30.2%) | |
| Intent | 0.032 | |||
| Unintentional | 332 (83.0%) | 1855 (79.5%) | 2187 (80.0%) | |
| Intentional | 24 (6.0%) | 110 (4.7%) | 134 (4.9%) | |
| Intent not known | 44 (11.0%) | 369 (15.8%) | 413 (15.1%) | |
| Injury Type (any) ^ | ||||
| N33, N34 spinal cord lesion | 8 (2.0%) | 45 (1.9%) | 53 (1.9%) | 1.000 |
| N19, N26 fracture of femur | 30 (7.5%) | 121 (5.2%) | 151 (5.5%) | 0.079 |
| N20 fracture of patella, tibia, fibula, or ankle | 30 (7.5%) | 274 (11.7%) | 304 (11.1%) | 0.016 |
| N28 moderate to severe traumatic brain injury | 122 (30.5%) | 424 (18.2%) | 546 (20.0%) | <0.001 |
| N37, N17, N18 crush injury, fracture foot/hand bones | 16 (4.0%) | 150 (6.4%) | 166 (6.1%) | 0.078 |
| N43 internal hemorrhage in abdomen or pelvis | 85 (21.2%) | 323 (13.8%) | 408 (14.9%) | <0.001 |
| N27 minor traumatic brain injury | 64 (16.0%) | 614 (26.3%) | 678 (24.8%) | <0.001 |
| N21 fracture of pelvis | 34 (8.5%) | 159 (6.8%) | 193 (7.1%) | 0.266 |
| N42 severe chest Injury | 60 (15.0%) | 272 (11.7%) | 332 (12.1%) | 0.070 |
| N8, N9, N10 burns (including lower airways) | 20 (5.0%) | 35 (1.5%) | 55 (2.0%) | <0.001 |
| N25 fracture of vertebral column | 45 (11.2%) | 268 (11.5%) | 313 (11.4%) | 0.960 |
| N35, N36 asphyxiation, Non-fatal submersion | <10 | <10 | 12 (0.4%) | 0.542 |
| N40, N44 contusion, open wound | 117 (29.2%) | 537 (23.0%) | 654 (23.9%) | 0.008 |
| N14 other injuries of muscle & tendon and other dislocations | 63 (15.8%) | 297 (12.7%) | 360 (13.2%) | 0.116 |
| N15 fracture of clavicle, scapula, or humerus | 36 (9.0%) | 255 (10.9%) | 291 (10.6%) | 0.286 |
| N22 fracture of radius or ulna | 35 (8.8%) | 325 (13.9%) | 360 (13.2%) | 0.006 |
| Other | 228 (57.0%) | 1003 (43.0%) | 1231 (45.0%) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dipnall, J.F.; Rivara, F.P.; Lyons, R.A.; Ameratunga, S.; Brussoni, M.; Lecky, F.E.; Bradley, C.; Beck, B.; Lyons, J.; Schneeberg, A.; et al. Health-Related Quality of Life (HRQoL) Outcomes Following Injury in Childhood and Adolescence Using EuroQol (EQ-5D) Responses with Pooled Longitudinal Data. Int. J. Environ. Res. Public Health 2021, 18, 10156. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910156
Dipnall JF, Rivara FP, Lyons RA, Ameratunga S, Brussoni M, Lecky FE, Bradley C, Beck B, Lyons J, Schneeberg A, et al. Health-Related Quality of Life (HRQoL) Outcomes Following Injury in Childhood and Adolescence Using EuroQol (EQ-5D) Responses with Pooled Longitudinal Data. International Journal of Environmental Research and Public Health. 2021; 18(19):10156. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910156
Chicago/Turabian StyleDipnall, Joanna F., Frederick P. Rivara, Ronan A. Lyons, Shanthi Ameratunga, Mariana Brussoni, Fiona E. Lecky, Clare Bradley, Ben Beck, Jane Lyons, Amy Schneeberg, and et al. 2021. "Health-Related Quality of Life (HRQoL) Outcomes Following Injury in Childhood and Adolescence Using EuroQol (EQ-5D) Responses with Pooled Longitudinal Data" International Journal of Environmental Research and Public Health 18, no. 19: 10156. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910156